
The Impact of Apical Periodontitis and Endodontic Treatment on Salivary Inflammatory Biomarkers: A Longitudinal Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Sample Size Calculation
2.3. Patient Recruitment
2.4. Clinical Examination
2.5. Radiographic Outcome Analysis
2.6. Saliva Sample Collection
2.7. Saliva Samples Processing
2.8. Statistical Analysis
3. Results
3.1. Treatment Outcome
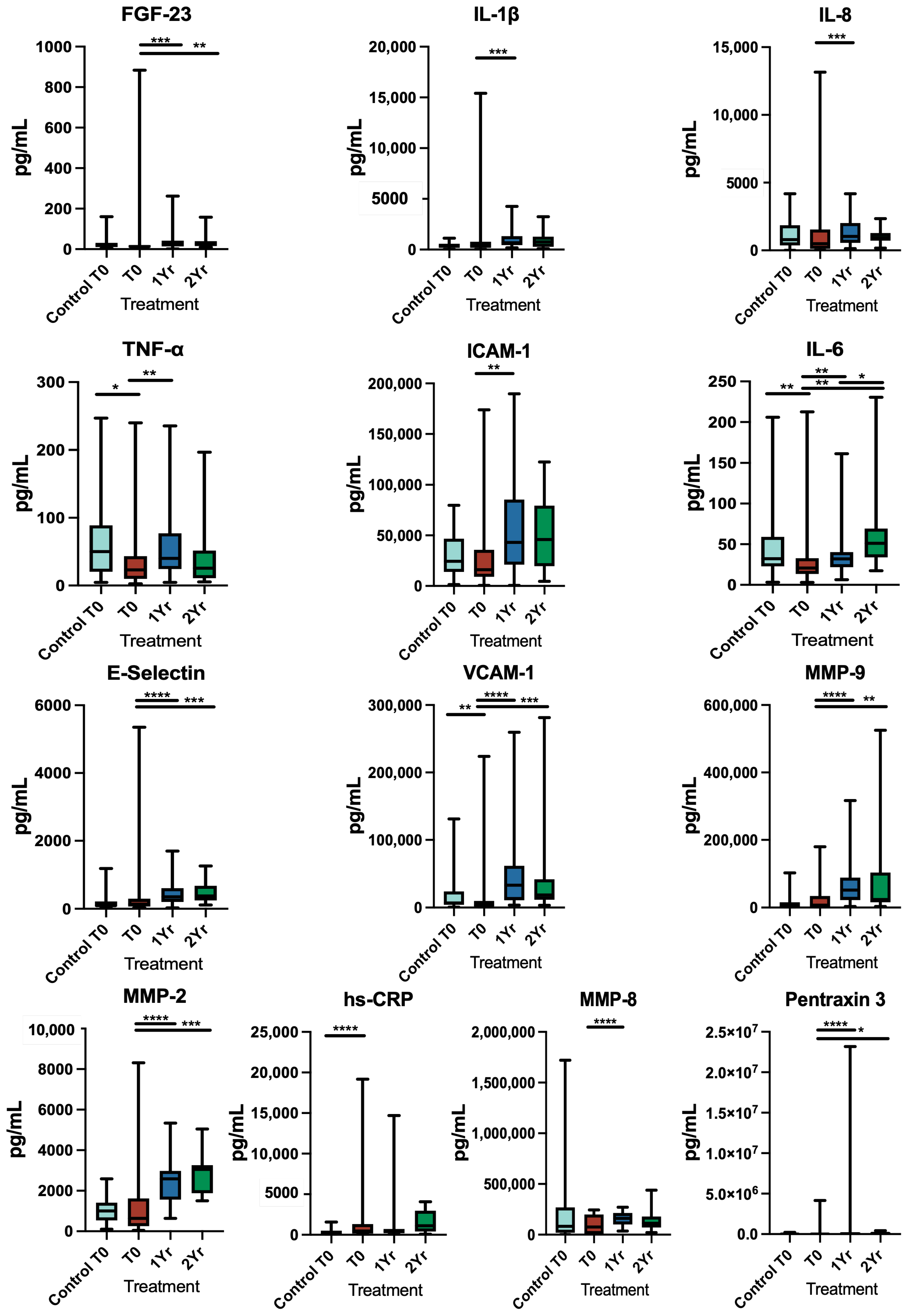
3.2. Inflammatory Markers
3.2.1. Pre-Operative Levels
3.2.2. One-Year Post-Treatment Follow-Up
3.2.3. Two-Year Post-Treatment Follow-Up
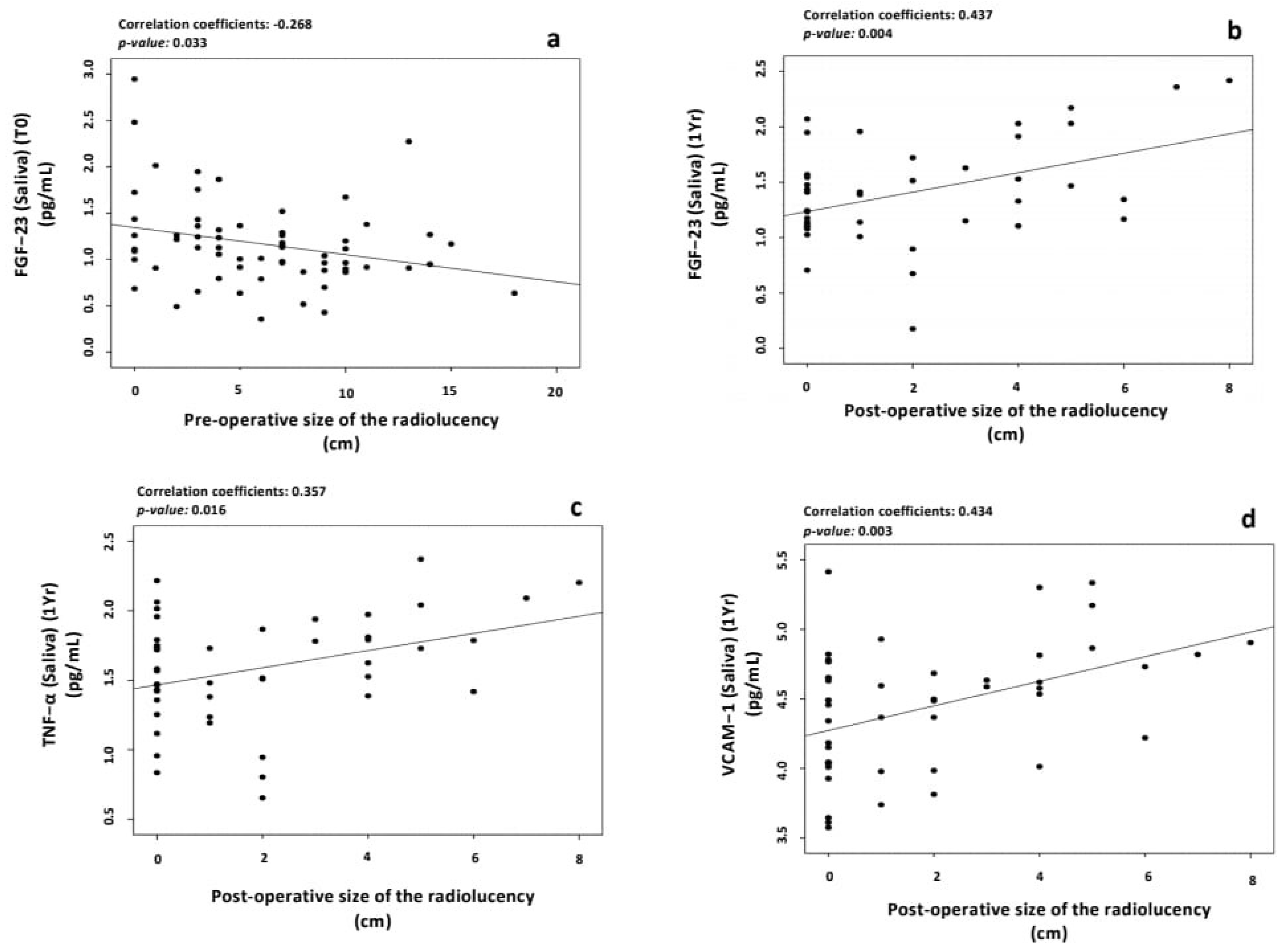
3.3. Effect of the Size of Radiolucency on the Levels of Inflammatory Markers
3.4. Correlation between the Outcome of Treatment and the Levels of Salivary Inflammatory Markers
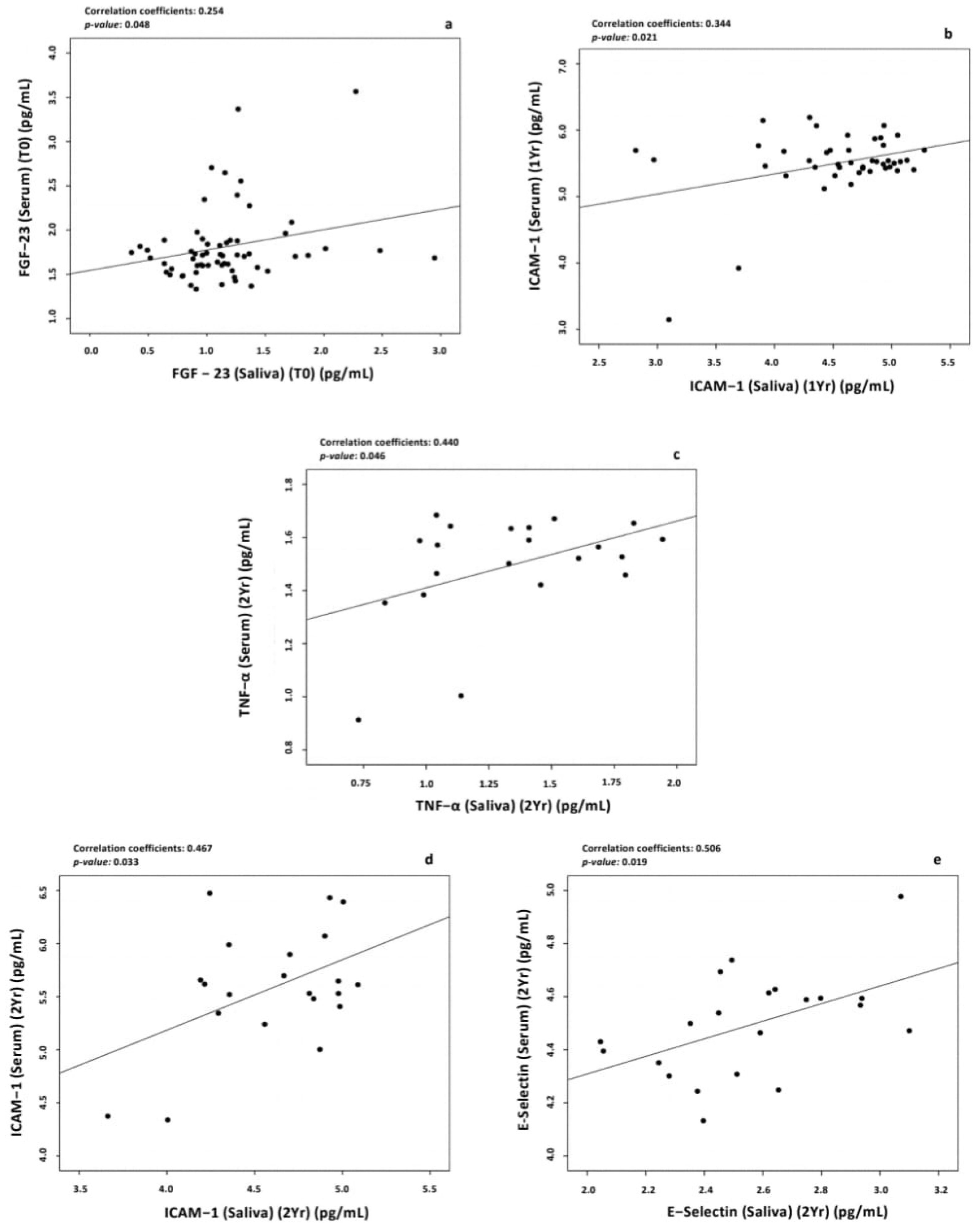
3.5. Correlation between Salivary and Serum Levels of Biomarkers
3.5.1. Baseline Levels
3.5.2. One-Year Post-Treatment Follow-Up
3.5.3. Two-Year Post-Treatment Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Figdor, D. Apical periodontitis: A very prevalent problem. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2002, 94, 651–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tibúrcio-Machado, C.S.; Michelon, C.; Zanatta, F.B.; Gomes, M.S.; Marin, J.A.; Bier, C.A. The global prevalence of apical periodontitis: A systematic review and meta-analysis. Int. Endod. J. 2021, 54, 712–735. [Google Scholar] [CrossRef] [PubMed]
- Georgiou, A.C.; Crielaard, W.; Armenis, I.; de Vries, R.; van der Waal, S.V. Apical Periodontitis Is Associated with Elevated Concentrations of Inflammatory Mediators in Peripheral Blood: A Systematic Review and Meta-analysis. J. Endod. 2019, 45, 1279–1295. [Google Scholar] [CrossRef] [PubMed]
- Rathnayake, N.; Akerman, S.; Klinge, B.; Lundegren, N.; Jansson, H.; Tryselius, Y.; Sorsa, T.; Gustafsson, A. Salivary biomarkers for detection of systemic diseases. PLoS ONE 2013, 8, e61356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorsa, T.; Mäntylä, P.; Rönkä, H.; Kallio, P.; Kallis, G.B.; Lundqvist, C.; Kinane, D.F.; Salo, T.; Golub, L.M.; Teronen, O. Scientific basis of a matrix metalloproteinase-8 specific chair-side test for monitoring periodontal and peri-implant health and disease. Ann. N. Y. Acad. Sci. 1999, 878, 130–140. [Google Scholar] [CrossRef]
- Miller, C.S.; King Jr, C.P.; Langub, M.C.; Kryscio, R.J.; Thomas, M.V. Salivary biomarkers of existing periodontal disease: A cross-sectional study. J. Am. Dent. Assoc. 2006, 137, 322–329. [Google Scholar] [CrossRef]
- Lee, A.; Ghaname, C.B.; Braun, T.M.; Sugai, J.V.; Teles, R.P.; Loesche, W.J.; Kornman, K.S.; Giannobile, W.V.; Kinney, J.S. Bacterial and salivary biomarkers predict the gingival inflammatory profile. J. Periodontol. 2012, 83, 79–89. [Google Scholar] [CrossRef]
- Baldini, C.; Giusti, L.; Ciregia, F.; Da Valle, Y.; Giacomelli, C.; Donadio, E.; Sernissi, F.; Bazzichi, L.; Giannaccini, G.; Bombardieri, S.; et al. Proteomic analysis of saliva: A unique tool to distinguish primary Sjögren’s syndrome from secondary Sjögren’s syndrome and other sicca syndromes. Arthritis Res. 2011, 13, R194. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, A.C.; Marson, F.A.d.L.; Mendonça, R.M.d.H.; Ribeiro, J.D.; Ribeiro, A.F.; Paschoal, I.A.; Levy, C.E. Saliva as a potential tool for cystic fibrosis diagnosis. Diagn. Pathol. 2013, 8, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Out, D.; Hall, R.J.; Granger, D.A.; Page, G.G.; Woods, S.J. Assessing salivary C-reactive protein: Longitudinal associations with systemic inflammation and cardiovascular disease risk in women exposed to intimate partner violence. Brain Behav. Immun. 2012, 26, 543–551. [Google Scholar] [CrossRef] [Green Version]
- Sugiyama, A.; Uehara, A.; Iki, K.; Matsushita, K.; Nakamura, R.; Ogawa, T.; Sugawara, S.; Takada, H. Activation of human gingival epithelial cells by cell-surface components of black-pigmented bacteria: Augmentation of production of interleukin-8, granulocyte colony-stimulating factor and granulocyte-macrophage colony-stimulating factor and expression of intercellular adhesion molecule 1. J. Med. Microbiol. 2002, 51, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Huang, G.J.; Haake, S.K.; Kim, J.W.; Park, N.H. Differential expression of interleukin-8 and intercellular adhesion molecule-1 by human gingival epithelial cells in response to Actinobacillus actinomycetemcomitans or Porphyromonas gingivalis infection. Oral Microbiol. Immunol. 1998, 13, 301–309. [Google Scholar] [CrossRef]
- Berlin-Broner, Y.; Febbraio, M.; Levin, L. Apical periodontitis and atherosclerosis: Is there a link? Review of the literature and potential mechanism of linkage. Quintessence Int. 2017, 48, 527–534. [Google Scholar] [CrossRef]
- Jimenez-Sanchez, M.C.; Cabanillas-Balsera, D.; Areal-Quecuty, V.; Velasco-Ortega, E.; Martin-Gonzalez, J.; Segura-Egea, J.J. Cardiovascular diseases and apical periodontitis: Association not always implies causality. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e652–e659. [Google Scholar] [CrossRef]
- Perez-Losada, F.L.; Estrugo-Devesa, A.; Castellanos-Cosano, L.; Segura-Egea, J.J.; Lopez-Lopez, J.; Velasco-Ortega, E. Apical periodontitis and diabetes mellitus type 2: A systematic review and meta-analysis. J. Clin. Med. 2020, 9, 540. [Google Scholar] [CrossRef] [Green Version]
- Bakhsh, A.; Moyes, D.; Proctor, G.; Mannocci, F.; Niazi, S.A. The Impact of Apical Periodontitis, Non-surgical Root Canal Retreatment and Periapical Surgery on Serum Inflammatory Biomarkers. Int. Endod. J. 2022, 55, 923–937. [Google Scholar] [CrossRef]
- Cotti, E.; Zedda, A.; Deidda, M.; Piras, A.; Flore, G.; Ideo, F.; Madeddu, C.; Pau, V.M.; Mercuro, G. Endodontic infection and endothelial dysfunction are associated with different mechanisms in men and women. J. Endod. 2015, 41, 594–600. [Google Scholar] [CrossRef]
- Patel, S.; Wilson, R.; Dawood, A.; Foschi, F.; Mannocci, F. The detection of periapical pathosis using digital periapical radiography and cone beam computed tomography—Part 2: A 1-year post-treatment follow-up. Int. Endod. J. 2012, 45, 711–723. [Google Scholar] [CrossRef]
- Granger, D.A.; Kivlighan, K.T.; Fortunato, C.; Harmon, A.G.; Hibel, L.C.; Schwartz, E.B.; Whembolua, G.L. Integration of salivary biomarkers into developmental and behaviorally-oriented research: Problems and solutions for collecting specimens. Physiol. Behav. 2007, 92, 583–590. [Google Scholar] [CrossRef]
- Pfaffe, T.; Cooper-White, J.; Beyerlein, P.; Kostner, K.; Punyadeera, C. Diagnostic potential of saliva: Current state and future applications. Clin. Chem. 2011, 57, 675–687. [Google Scholar] [CrossRef] [Green Version]
- Paiva, K.B.S.; Granjeiro, J.M. Matrix Metalloproteinases in Bone Resorption, Remodeling, and Repair. Prog. Mol. Biol. Transl. Sci. 2017, 148, 203–303. [Google Scholar] [CrossRef] [PubMed]
- Rai, B.; Kaur, J.; Jain, R.; Anand, S.C. Levels of gingival crevicular metalloproteinases-8 and -9 in periodontitis. Saudi Dent. J. 2010, 22, 129–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaushik, R.; Yeltiwar, R.K.; Pushpanshu, K. Salivary interleukin-1β levels in patients with chronic periodontitis before and after periodontal phase I therapy and healthy controls: A case-control study. J. Periodontol. 2011, 82, 1353–1359. [Google Scholar] [CrossRef] [PubMed]
- Cole, W.; NHS Dental Patients in England Have Missed 19 MILLION Appointments This Year Alone—As Lockdown Triggers ‘Ticking Time Bomb’ for Nation’s Oral Health. Daily Mail 2020. Available online: https://www.dailymail.co.uk/news/article-8953103/NHS-dental-patients-England-missed-19-MILLION-appointments-year.html (accessed on 17 March 2023).
- Patel, S.; Wilson, R.; Dawood, A.; Mannocci, F. The detection of periapical pathosis using periapical radiography and cone beam computed tomography—Part 1: Pre-operative status. Int. Endod. J. 2012, 45, 702–710. [Google Scholar] [CrossRef]
- Zahran, S.; Patel, S.; Koller, G.; Mannocci, F. The impact of an enhanced infection control protocol on molar root canal treatment outcome—A randomized clinical trial. Int. Endod. J. 2021, 54, 1993–2005. [Google Scholar] [CrossRef]
- European Society of Endodontology. Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [Google Scholar] [CrossRef]
- Kindt, T.; Goldsby, R.; Osborne, B. Kuby Immunology, 6th ed.; Aufl. W. H. Freeman: New York, NY, USA, 2006. [Google Scholar]
- Du Clos, T.W. Function of C-reactive protein. Ann. Med. 2000, 32, 274–278. [Google Scholar] [CrossRef]
- Ebersole, J.L.; Kryscio, R.J.; Campbell, C.; Kinane, D.; McDevitt, J.; Christodoulides, N.; Floriano, P.; Miller, C.S. Salivary and serum adiponectin and C-reactive protein levels in acute myocardial infarction related to body mass index and oral health. J. Periodontal Res. 2017, 52, 419–427. [Google Scholar] [CrossRef]
- Pay, J.B.; Shaw, A.M. Towards salivary C-reactive protein as a viable biomarker of systemic inflammation. Clin. Biochem. 2019, 68, 1–8. [Google Scholar] [CrossRef]
- Megson, E.; Fitzsimmons, T.; Dharmapatni, K.; Mark Bartold, P. C-reactive protein in gingival crevicular fluid may be indicative of systemic inflammation. J. Clin. Periodontol. 2010, 37, 797–804. [Google Scholar] [CrossRef]
- Kopanczyk, R.; Opris, D.C.; Lickliter, J.; Bridges, E.G.; Nazar, A.M.; Bridges, K.G. C-reactive protein levels in blood and saliva show no correlation in young, healthy adults. FASEB J. 2010, 24, lb409. [Google Scholar] [CrossRef]
- Mirzaii-Dizgah, I.; Riahi, E. Salivary high-sensitivity cardiac troponin T levels in patients with acute myocardial infarction. Oral Dis. 2013, 19, 180–184. [Google Scholar] [CrossRef]
- Byrne, M.L.; O’Brien-Simpson, N.M.; Reynolds, E.C.; Walsh, K.A.; Laughton, K.; Waloszek, J.M.; Woods, M.J.; Trinder, J.; Allen, N.B. Acute phase protein and cytokine levels in serum and saliva: A comparison of detectable levels and correlations in a depressed and healthy adolescent sample. Brain Behav. Immun. 2013, 34, 164–175. [Google Scholar] [CrossRef]
- Cullen, T.; Thomas, A.; Webb, R.; Hughes, M.G. The relationship between interleukin-6 in saliva, venous and capillary plasma, at rest and in response to exercise. Cytokine 2015, 71, 397–400. [Google Scholar] [CrossRef]
- Liu, S.; Guo, R.; Simpson, L.G.; Xiao, Z.S.; Burnham, C.E.; Quarles, L.D. Regulation of fibroblastic growth factor 23 expression but not degradation by PHEX. J. Biol. Chem. 2003, 278, 37419–37426. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, J.; Liu, S.; Quarles, L.D. Role of fibroblast growth factor 23 in phosphate homeostasis and pathogenesis of disordered mineral metabolism in chronic kidney disease. Semin Dial. 2007, 20, 302–308. [Google Scholar] [CrossRef]
- Batra, J.; Buttar, R.S.; Kaur, P.; Kreimerman, J.; Melamed, M.L. FGF-23 and cardiovascular disease: Review of literature. Curr. Opin. Endocrinol. Diabetes Obes. 2016, 23, 423–429. [Google Scholar] [CrossRef]
- Vázquez-Sánchez, S.; Poveda, J.; Navarro-García, J.A.; González-Lafuente, L.; Rodríguez-Sánchez, E.; Ruilope, L.M.; Ruiz-Hurtado, G. An Overview of FGF-23 as a Novel Candidate Biomarker of Cardiovascular Risk. Front. Physiol. 2021, 12, 632260. [Google Scholar] [CrossRef]
- Martin, A.; David, V.; Quarles, L.D. Regulation and function of the FGF23/klotho endocrine pathways. Physiol. Rev. 2012, 92, 131–155. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Yoshiko, Y.; Yamamoto, R.; Minamizaki, T.; Kozai, K.; Tanne, K.; Aubin, J.E.; Maeda, N. Overexpression of fibroblast growth factor 23 suppresses osteoblast differentiation and matrix mineralization in vitro. J. Bone Miner. Res. 2008, 23, 939–948. [Google Scholar] [CrossRef]
- Cybulsky, M.I.; Iiyama, K.; Li, H.; Zhu, S.; Chen, M.; Iiyama, M.; Davis, V.; Gutierrez-Ramos, J.C.; Connelly, P.W.; Milstone, D.S. A major role for VCAM-1, but not ICAM-1, in early atherosclerosis. J. Clin. Investig. 2001, 107, 1255–1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook-Mills, J.M.; Marchese, M.E.; Abdala-Valencia, H. Vascular cell adhesion molecule-1 expression and signaling during disease: Regulation by reactive oxygen species and antioxidants. Antioxid. Redox Signal. 2011, 15, 1607–1638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yılmaz Şaştım, Ç.; Gürsoy, M.; Könönen, E.; Kasurinen, A.; Norvio, S.; Gürsoy, U.K.; Doğan, B. Salivary and serum markers of angiogenesis in periodontitis in relation to smoking. Clin. Oral Investig. 2021, 25, 1117–1126. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Inclusion | Exclusion |
|---|---|
| >18 years old | Smokers |
| Pregnant women | |
| Teeth with periodontal pockets >4 mm/endodontic—periodontal lesion, gingivitis, periodontitis | |
| Root canal retreatment cases | Patients with chronic inflammatory condition (Asthma, Inflammatory bowel diseases, Irritable bowel syndrome, Chronic peptic ulcer, Rheumatoid arthritis, Ulcerative colitis, Liver diseases, Crohn’s disease, Sinusitis, Active hepatitis, Autoimmune diseases, Tuberculosis, Renal diseases or Cancer). |
| Periapical surgery cases | Patients on medication altering bone metabolism |
| Unrestorable teeth | |
| Antibiotics in last 3 months | |
| Surgical procedure in last 6 months |
| Control | Treatment | p-Value | |
|---|---|---|---|
| Median (IQR) | Median (IQR) | ||
| FGF-23 | 20.44 (10.71–31.26) | 13.23 (8.09–20.17) | 0.089 |
| IL-1β | 354.14 (181.2–577.2) | 398.01 (178.3–772.1) | 0.257 |
| IL-8 | 797.57 (370.2–1860) | 511.09 (117.3–1547) | 0.172 |
| Pentraxin 3 | 4217.6 (2131–8020) | 2093 (1286–29,057) | 0.143 |
| TNF-α | 40.15 (20.28–88.88) | 22.96 (9.79–43.46) | 0.029 * |
| ICAM-1 | 25,883.02 (13,974–46,718) | 15,975.95 (9041–35,671) | 0.144 |
| IL-6 | 31.17 (22.74–59.01) | 20.68 (13.44–32.85) | 0.005 ** |
| MMP-8 | 82,732.46 (18,560–269,023) | 84,431.78 (5458–199,330) | 0.136 |
| E-selectin | 95.22 (65.03–217.3) | 138.86 (68.16–291.4) | 0.182 |
| VCAM-1 | 6412.39 (4205–23,601) | 3059.68 (1557–9886) | 0.005 ** |
| hs-CRP | 192.04 (100.9–502.2) | 372.35 (166.6–1324) | <0.001 *** |
| MMP-2 | 974.52 (537.9–1413) | 638.66 (251.3–1617) | 0.127 |
| MMP-9 | 4446.12 (921.1–15,776) | 8100.99 (2157–33,650) | 0.057 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakhsh, A.; Al-Abdulla, N.; Mannocci, F.; Allihaibi, M.; Moyes, D.; Proctor, G.; Niazi, S.A. The Impact of Apical Periodontitis and Endodontic Treatment on Salivary Inflammatory Biomarkers: A Longitudinal Study. Appl. Sci. 2023, 13, 3952. https://doi.org/10.3390/app13063952
Bakhsh A, Al-Abdulla N, Mannocci F, Allihaibi M, Moyes D, Proctor G, Niazi SA. The Impact of Apical Periodontitis and Endodontic Treatment on Salivary Inflammatory Biomarkers: A Longitudinal Study. Applied Sciences. 2023; 13(6):3952. https://doi.org/10.3390/app13063952
Chicago/Turabian StyleBakhsh, Abdulaziz, Noor Al-Abdulla, Francesco Mannocci, Marwa Allihaibi, David Moyes, Gordon Proctor, and Sadia Ambreen Niazi. 2023. "The Impact of Apical Periodontitis and Endodontic Treatment on Salivary Inflammatory Biomarkers: A Longitudinal Study" Applied Sciences 13, no. 6: 3952. https://doi.org/10.3390/app13063952