
EMG Signs of Motor Units’ Enlargement in Stroke Survivors
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Motor Function Evaluation and Dominance Evaluation
2.3. Experimental Protocol
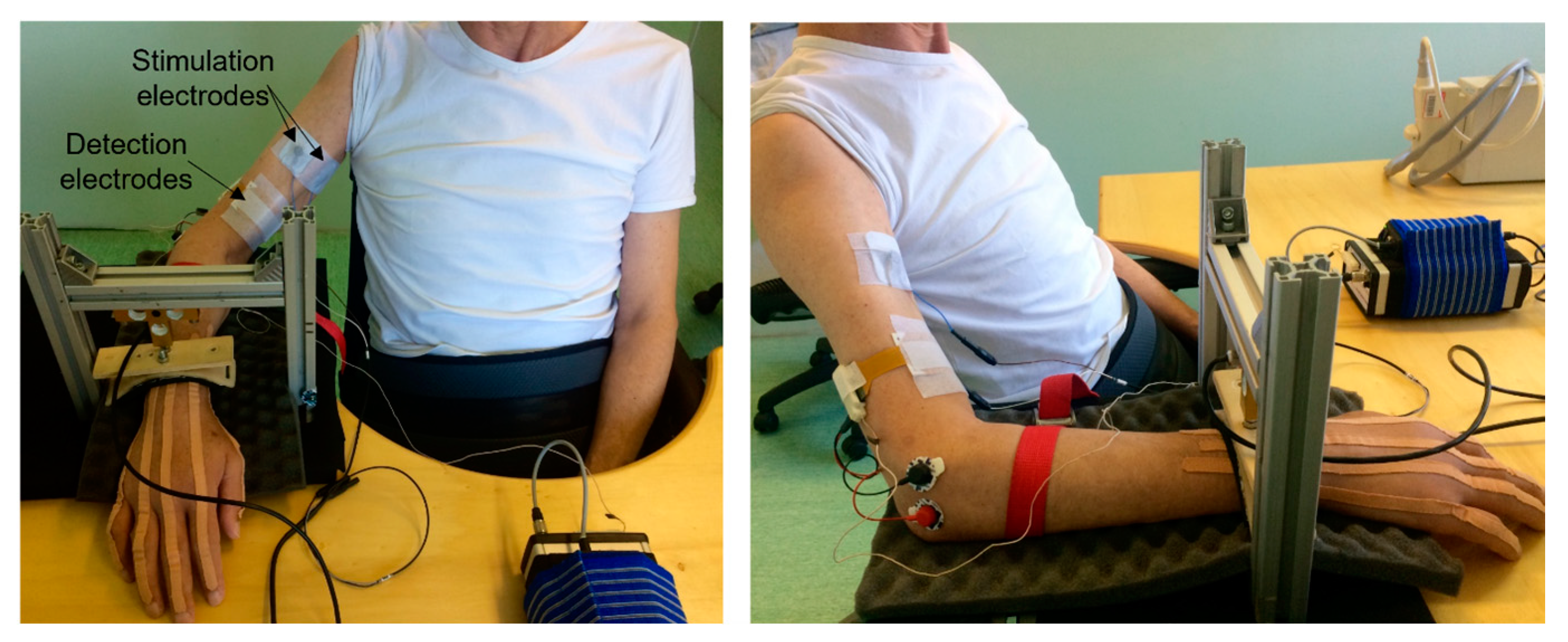
2.4. Stimulation Electrode Positioning
2.5. EMG Recordings
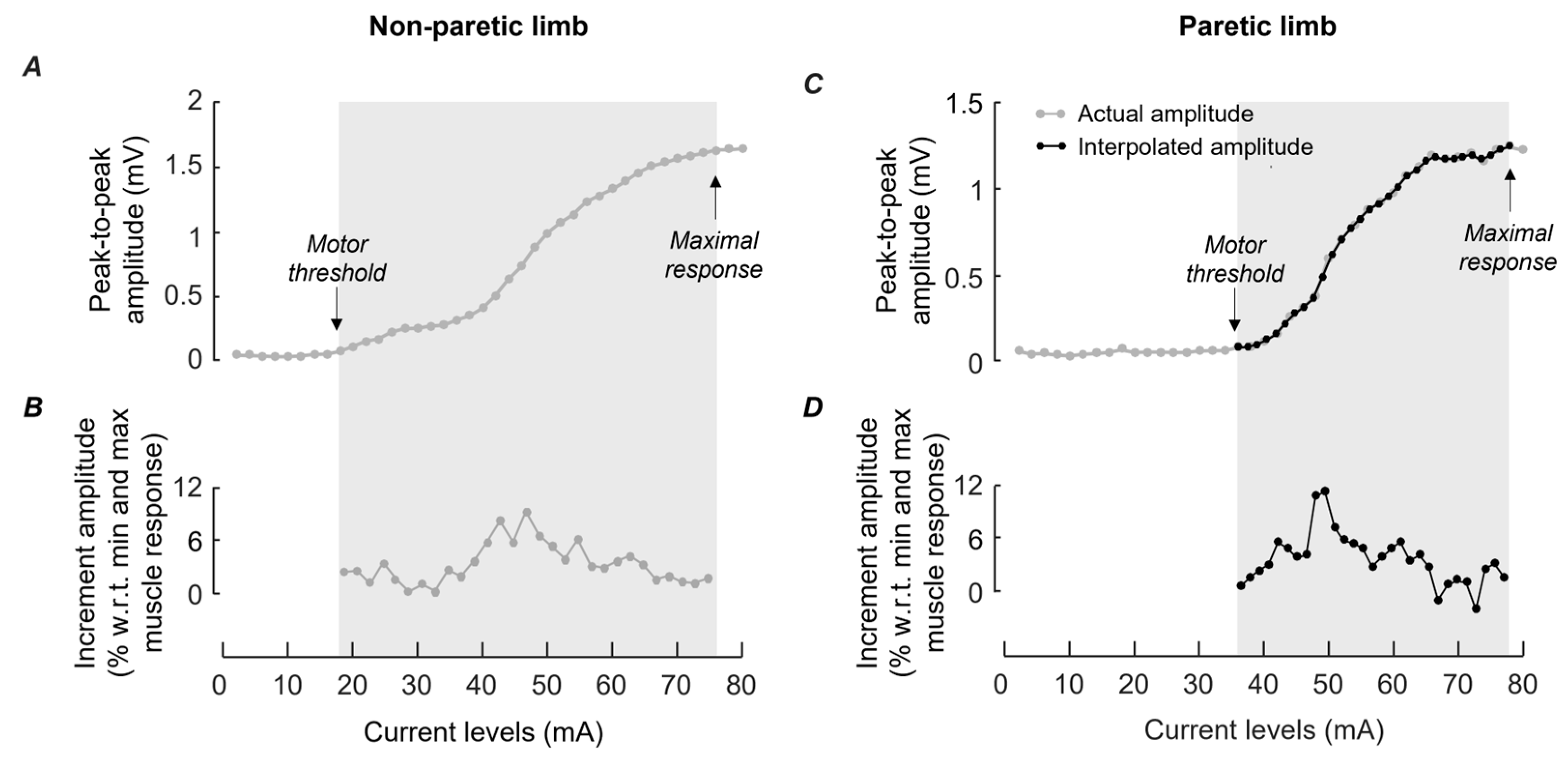
2.6. Assessment of Muscle Responses in Paretic and Non-Paretic Limbs
2.7. Statistics
3. Results
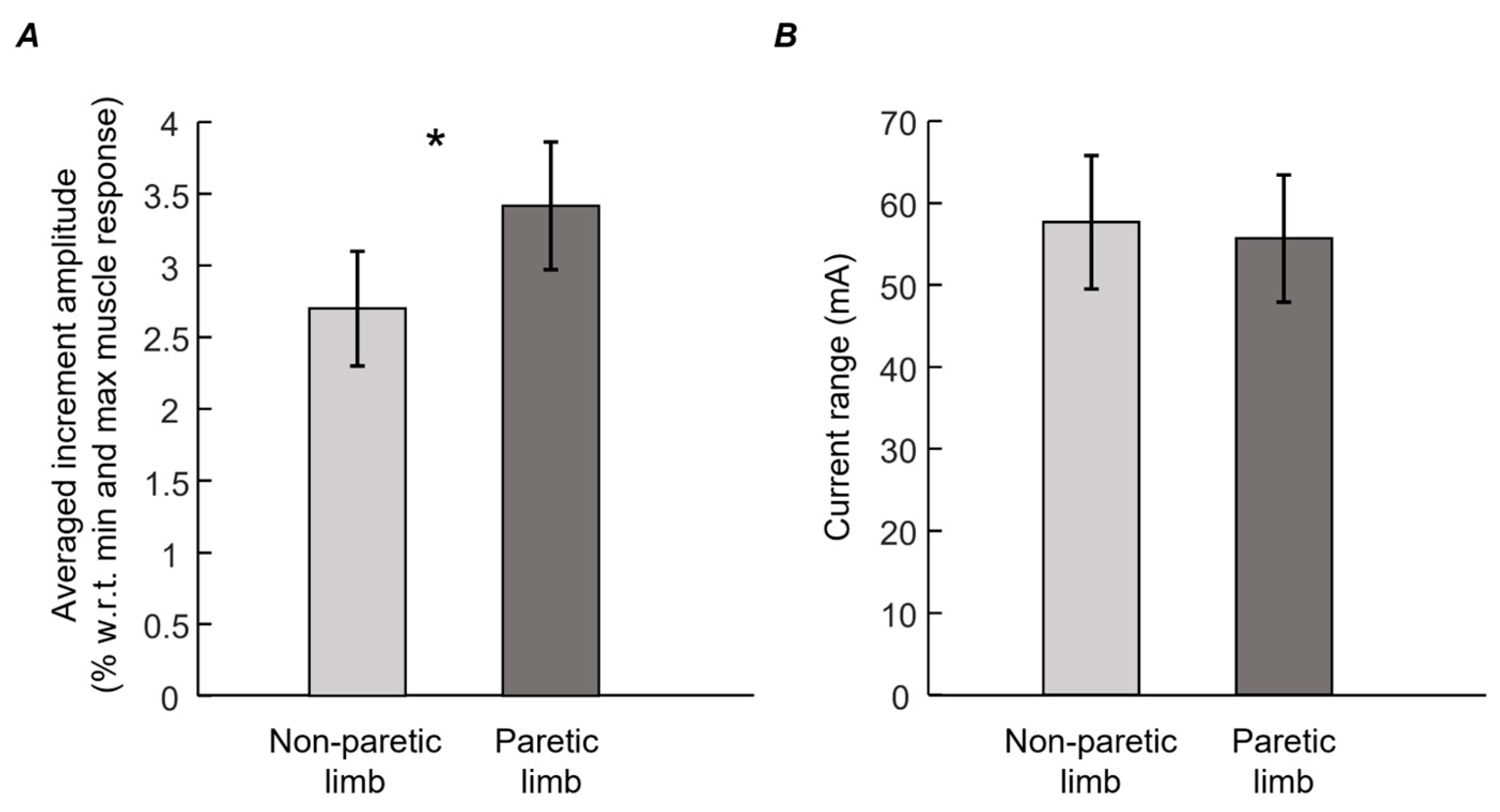
Differences between Muscle Responses in Paretic and Non-Paretic Limbs
4. Discussion
4.1. Preliminary Considerations
4.2. Variations in M-Wave Amplitude Differed between Biceps Brachii of Paretic and Non-Paretic Limbs
4.3. Physiological Implications
4.4. Study Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McComas, A.J.; Sica, R.E.; Upton, A.R.; Aguilera, N. Functional Changes in Motoneurones of Hemiparetic Patients. J. Neurol. Neurosurg. Psychiatry 1973, 36, 183–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hara, Y.; Masakado, Y.; Chino, N. The Physiological Functional Loss of Single Thenar Motor Units in the Stroke Patients: When Does It Occur? Does It Progress? Clin. Neurophysiol. 2004, 115, 97–103. [Google Scholar] [CrossRef]
- Cowan, W.M. Anterograde and Retrograde Transneuronal Degeneration in the Central and Peripheral Nervous System. In Contemporary Research Methods in Neuroanatomy; Springer: Berlin/Heidelberg, Germany, 1970; pp. 217–251. [Google Scholar]
- Kouzi, I.; Trachani, E.; Anagnostou, E.; Rapidi, C.-A.; Ellul, J.; Sakellaropoulos, G.C.; Chroni, E. Motor Unit Number Estimation and Quantitative Needle Electromyography in Stroke Patients. J. Electromyogr. Kinesiol. 2014, 24, 910–916. [Google Scholar] [CrossRef]
- Li, X.; Wang, Y.-C.; Suresh, N.L.; Rymer, W.Z.; Zhou, P. Motor Unit Number Reductions in Paretic Muscles of Stroke Survivors. IEEE Trans. Inf. Technol. Biomed. 2011, 15, 505–512. [Google Scholar] [CrossRef]
- Li, X.; Liu, J.; Li, S.; Wang, Y.-C.; Zhou, P. Examination of Hand Muscle Activation and Motor Unit Indices Derived from Surface EMG in Chronic Stroke. IEEE Trans. Biomed. Eng. 2014, 61, 2891–2898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez, A.C.; del Campo, F.; Mingo, M.R.; Conde, M.C.P. Altered Motor Unit Architecture in Hemiparetic Patients. A Single Fibre EMG Study. J. Neurol. Neurosurg. Psychiatry 1982, 45, 756–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukács, M.; Vécsei, L.; Beniczky, S. Changes in Muscle Fiber Density Following a Stroke. Clin. Neurophysiol. 2009, 120, 1539–1542. [Google Scholar] [CrossRef] [PubMed]
- Kallenberg, L.A.C.; Hermens, H.J. Motor Unit Properties of Biceps Brachii in Chronic Stroke Patients Assessed with High-Density Surface EMG. Muscle Nerve 2009, 39, 177–185. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Suresh, A.; Zhou, P.; Rymer, W.Z. Alterations in the Peak Amplitude Distribution of the Surface Electromyogram Poststroke. IEEE Trans. Biomed. Eng. 2013, 60, 845–852. [Google Scholar] [CrossRef]
- Yao, B.; Klein, C.S.; Hu, H.; Li, S.; Zhou, P. Motor Unit Properties of the First Dorsal Interosseous in Chronic Stroke Subjects: Concentric Needle and Single Fiber EMG Analysis. Front. Physiol. 2018, 9, 1587. [Google Scholar] [CrossRef] [Green Version]
- Stålberg, E. Use of Single Fiber EMG and Macro EMG in Study of Reinnervation. Muscle Nerve 1990, 13, 804–813. [Google Scholar] [CrossRef] [PubMed]
- Vieira, T.M.; Lemos, T.; Oliveira, L.A.S.; Horsczaruk, C.H.R.; Freitas, G.R.; Tovar-Moll, F.; Rodrigues, E.C. Postural Muscle Unit Plasticity in Stroke Survivors: Altered Distribution of Gastrocnemius’ Action Potentials. Front. Neurol. 2019, 10, 686. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.; Alix, J.J.P.; Neuwirth, C.; Barkhaus, P.E.; Castro, J.; Jenkins, T.M.; McDermott, C.J.; Shaw, P.J.; Carvalho, M.; Nandedkar, S.; et al. Reinnervation as Measured by the Motor Unit Size Index Is Associated with Preservation of Muscle Strength in Amyotrophic Lateral Sclerosis, but Not All Muscles Reinnervate. Muscle Nerve 2022, 65, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Heckman, C.J.; Enoka, R.M. Motor Unit. Compr. Physiol. 2012, 2, 2629–2682. [Google Scholar] [CrossRef]
- Juel, V.C. Single Fiber Electromyography. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2019; pp. 303–310. [Google Scholar]
- National Stroke Association. What Is Stroke? Available online: http://www.stroke.org/understand-stroke/what-stroke (accessed on 1 June 2017).
- McComas, A.J.; Fawcett, P.R.W.; Campbell, M.J.; Sica, R.E.P. Electrophysiological Estimation of the Number of Motor Units within a Human Muscle. J. Neurol. Neurosurg. Psychiatry 1971, 34, 121–131. [Google Scholar] [CrossRef] [Green Version]
- Blok, J.H.; Ruitenberg, A.; Maathuis, E.M.; Visser, G.H. The Electrophysiological Muscle Scan. Muscle Nerve 2007, 36, 436–446. [Google Scholar] [CrossRef]
- McPhedran, A.M.; Wuerker, R.B.; Henneman, E. Properties of Motor Units in a Heterogeneous Pale Muscle (m. Gastrocnemius) of the Cat. J. Neurophysiol. 1965, 28, 85–99. [Google Scholar] [CrossRef]
- McPhedran, A.M.; Wuerker, R.B.; Henneman, E. Properties of Motor Units in a Homogeneous Red Muscle (Soleus) of Cat. J. Neurophysiol. 1965, 28, 71–84. [Google Scholar] [CrossRef]
- Calder, K.M.; Hall, L.A.; Lester, S.M.; Inglis, J.G.; Gabriel, D.A. Reliability of the Biceps Brachii M-Wave. J. Neuroeng. Rehabil. 2005, 2, 33. [Google Scholar] [CrossRef] [Green Version]
- Merletti, R.; Farina, D.; Gazzoni, M. The Linear Electrode Array: A Useful Tool with Many Applications. J. Electromyogr. Kinesiol. 2003, 13, 37–47. [Google Scholar] [CrossRef]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke Rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- Bamford, J.; Sandercock, P.; Dennis, M.; Burn, J.; Warlow, C. Classification and Natural History of Clinically Identifiable Subtypes of Cerebral Infarction. Lancet 1991, 337, 1521–1526. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The Post-Stroke Hemiplegic Patient. 1. a Method for Evaluation of Physical Performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [PubMed]
- Pinto, T.P.; Gazzoni, M.; Botter, A.; Vieira, T.M. Does the Amplitude of Biceps Brachii M Waves Increase Similarly in Both Limbs during Staircase, Electrically Elicited Contractions? Physiol. Meas. 2018, 39, 085005. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, R.C. The Assessment and Analysis of Handedness: The Edinburgh Inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef] [PubMed]
- Barone, U.; Merletti, R. Design of a Portable, Intrinsically Safe Multichannel Acquisition System for High-Resolution, Real-Time Processing HD-SEMG. IEEE Trans. Biomed. Eng. 2013, 60, 2242–2252. [Google Scholar] [CrossRef] [Green Version]
- van Dijk, J.P.; Lowery, M.M.; Lapatki, B.G.; Stegeman, D.F. Evidence of Potential Averaging over the Finite Surface of a Bioelectric Surface Electrode. Ann. Biomed. Eng. 2009, 37, 1141–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botter, A.; Merletti, R. EMG of Electrically Stimulated Muscles. In Surface Electromyography: Physiology, Engineering, and Applications; Merletti, R., Farina, D., Eds.; Wiley Online Library: Hoboken, NJ, USA, 2016; pp. 311–332. [Google Scholar]
- Pacha Vicente, D.; Forcada Calvet, P.; Carrera Burgaya, A.; Llusá Pérez, M. Innervation of Biceps Brachii and Brachialis: Anatomical and Surgical Approach. Clin. Anat. 2005, 18, 186–194. [Google Scholar] [CrossRef]
- Cambon-Binder, A.; Leclercq, C. Anatomical Study of the Musculocutaneous Nerve Branching Pattern: Application for Selective Neurectomy in the Treatment of Elbow Flexors Spasticity. Surg. Radiol. Anat. 2015, 37, 341–348. [Google Scholar] [CrossRef]
- Roeleveld, K.; Stegeman, D.F.; Vingerhoets, H.M.; Van Oosterom, A. The Motor Unit Potential Distribution over the Skin Surface and Its Use in Estimating the Motor Unit Location. Acta Physiol. Scand. 1997, 161, 465–472. [Google Scholar] [CrossRef]
- Rodriguez-Falces, J.; Negro, F.; Gonzalez-Izal, M.; Farina, D. Spatial Distribution of Surface Action Potentials Generated by Individual Motor Units in the Human Biceps Brachii Muscle. J. Electromyogr. Kinesiol. 2013, 23, 766–777. [Google Scholar] [CrossRef] [PubMed]
- Merletti, R.; Knaflitz, M.; DeLuca, C.J. Electrically Evoked Myoelectric Signals. Crit. Rev. Biomed. Eng. 1992, 19, 293–340. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| ID | Sex | Age (yo) | Stroke Type | Paretic Limb | LQ Score (%) | Time since Stroke (Months) | FMA-UE Score | Inc Amp Non-Paretic Limb (%) | Inc Amp Paretic Limb (%) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 48 | hemorrhagic | right | 81.0 | 19 | 5/12 | 3.5 | 4.8 |
| 2 | F | 68 | ischemic | right | 90.5 | 10 | 4/12 | 4.0 | 4.1 |
| 3 | M | 61 | hemorrhagic | left | 90.5 | 39 | 10/12 | 1.4 | 1.6 |
| 4 | F | 71 | ischemic | right | 41.7 | 1 | 3/12 | 3.0 | 3.7 |
| 5 | M | 59 | ischemic | right | 100.0 | 2 | 2/12 | 2.3 | 3.1 |
| 6 | M | 70 | ischemic | left | 100.0 | 43 | 6/12 | 2.0 | 3.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinto, T.P.; Turolla, A.; Gazzoni, M.; Agostini, M.; Vieira, T.M. EMG Signs of Motor Units’ Enlargement in Stroke Survivors. Appl. Sci. 2023, 13, 2680. https://doi.org/10.3390/app13042680
Pinto TP, Turolla A, Gazzoni M, Agostini M, Vieira TM. EMG Signs of Motor Units’ Enlargement in Stroke Survivors. Applied Sciences. 2023; 13(4):2680. https://doi.org/10.3390/app13042680
Chicago/Turabian StylePinto, Talita P., Andrea Turolla, Marco Gazzoni, Michela Agostini, and Taian M. Vieira. 2023. "EMG Signs of Motor Units’ Enlargement in Stroke Survivors" Applied Sciences 13, no. 4: 2680. https://doi.org/10.3390/app13042680