
Feasibility of Shoulder Kinematics Assessment Using Magnetic Inertial Measurement Units in Hemiplegic Patients after Stroke: A Pilot Study
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Evaluation of Function
- The hand from the contralateral knee to the ipsilateral ear;
- Shoulder flexion at 180° (with the elbow at 0° and pronation–supination at 0°);
- Shoulder abduction at 180° (elbow at 0° and forearm pronated);
- The hand from the ipsilateral ear to the contralateral knee;
- The hand to the lumbar spine from the hand on the lap.
2.3. Scapular Kinematics
2.4. Data Analysis
3. Results
3.1. Demographic Characteristics
3.2. Glenohumeral Kinematics and Scapular Movements at Maximum Flexion and Extension
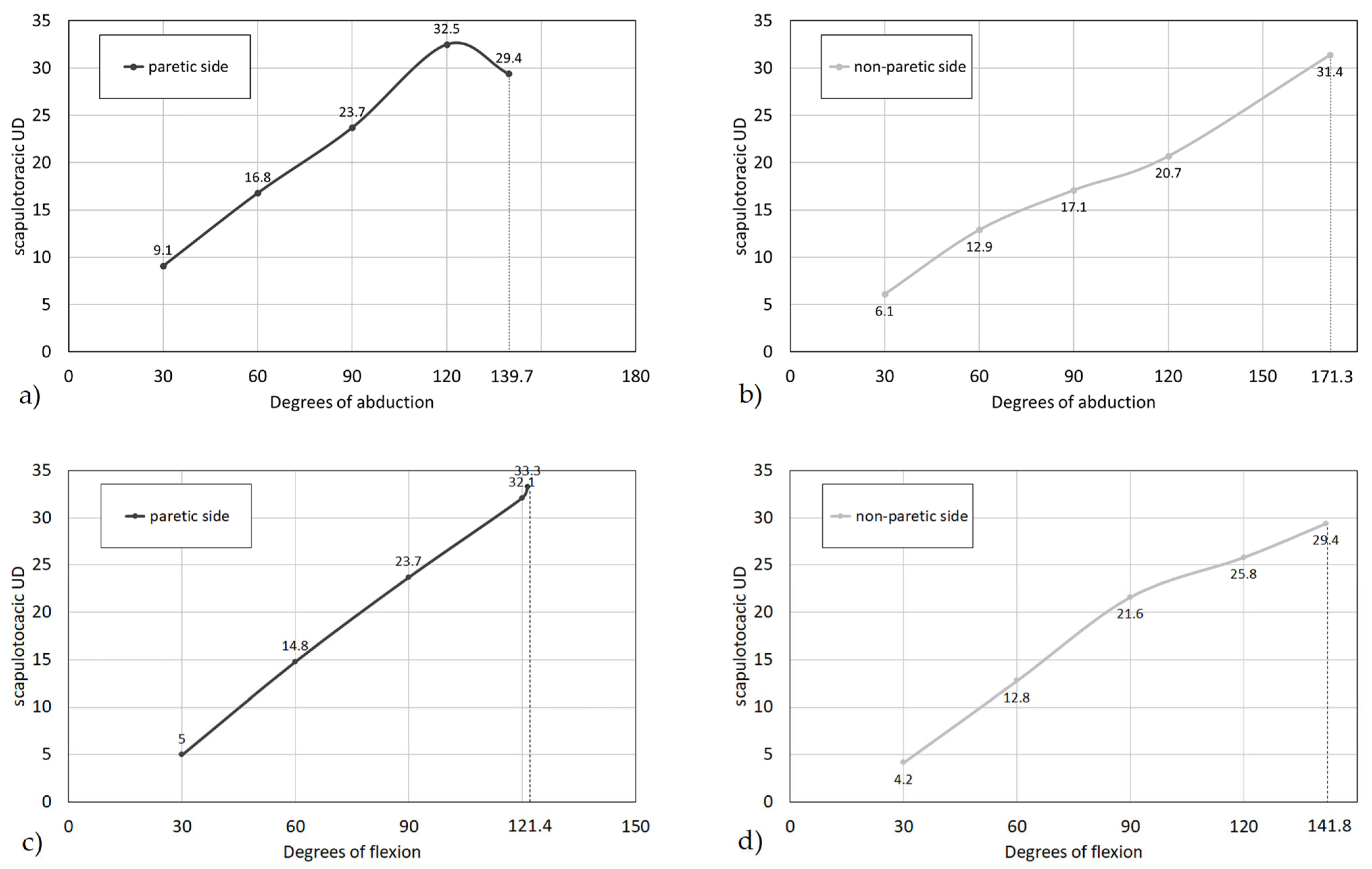
3.3. Scapular Angles during Different Angles of Shoulder Flexion and Abduction
3.4. Correlation between Glenohumeral and Scapular Kinematics and FMA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schwarz, A.; Kanzler, C.M.; Lambercy, O.; Luft, A.R.; Veerbeek, J.M. Systematic Review on Kinematic Assessments of Upper Limb Movements After Stroke. Stroke 2019, 50, 718–727. [Google Scholar] [CrossRef] [PubMed]
- van der Vliet, R.; Selles, R.W.; Andrinopoulou, E.R.; Nijland, R.; Ribbers, G.M.; Frens, M.A.; Meskers, C.; Kwakkel, G. Predicting Upper Limb Motor Impairment Recovery after Stroke: A Mixture Model. Ann. Neurol. 2020, 87, 383–393. [Google Scholar] [PubMed]
- De Baets, L.; Jaspers, E.; Desloovere, K.; Van Deun, S. A systematic review of 3D scapular kinematics and muscle activity during elevation in stroke subjects and controls. J. Electromyogr. Kinesiol. 2013, 23, 3–13. [Google Scholar] [PubMed]
- Avila, M.A.; Romaguera, F.; Oliveira, A.B.; Camargo, P.R.; Salvini, T.F. Bilateral impairments of shoulder abduction in chronic hemiparesis: Electromyographic patterns and isokinetic muscle performance. J. Electromyogr. Kinesiol. 2013, 23, 712–720. [Google Scholar] [PubMed]
- Rundquist, P.J.; Obrecht, C.; Woodruff, L. Three-dimensional shoulder kinematics? To complete activities of daily living. Am. J. Phys. Med. Rehabil. 2009, 88, 623–629. [Google Scholar] [CrossRef]
- Carnevale, A.; Longo, U.G.; Schena, E.; Massaroni, C.; Lo Presti, D.; Berton, A.; Candela, V.; Denaro, V. Wearable systems for shoulder kinematics assessment: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 546. [Google Scholar]
- Del Din, S.; Patel, S.; Cobelli, C.; Bonato, P. Estimating Fugl-Meyer clinical scores in stroke survivors using wearable sensors. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 5839–5842. [Google Scholar]
- De Baets, L.; Van Deun, S.; Desloovere, K.; Jaspers, E. Dynamic scapular movement analysis: Is it feasible and reliable in stroke patients during arm elevation? PLoS ONE 2013, 8, e79046. [Google Scholar]
- De Baets, L.; Van Deun, S.; Monari, D.; Jaspers, E. Three-dimensional kinematics of the scapula and trunk. and associated scapular muscle timing in individuals with stroke. Hum. Mov. Sci. 2016, 48, 82–90. [Google Scholar] [CrossRef]
- Rundquist, P.J.; Dumit, M.; Hartley, J.; Schultz, K.; Finley, M.A. Three-dimensional shoulder complex kinematics in individuals with upper extremity impairment from chronic stroke. Disabil. Rehabil. 2012, 34, 402–407. [Google Scholar]
- Meskers, C.G.M.; Koppe, P.A.; Konijnenbelt, H.; Veeger, H.E.J.; Janssen, T.W.J. Kinematic Alterations in the Ipsilateral Shoulder of Patients with Hemiplegia Due to Stroke. Am. J. Phys. Med. Rehabil. 2005, 84, 97–105. [Google Scholar]
- Lixandrão, M.C.; Camargo, P.R.; Scarpa, C.E.N.; Prado-Medeiros, C.L.; Salvini, T.F. Bilateral changes in 3-D scapular kinematics in individuals with chronic stroke. ClinBiomech 2017, 47, 79–86. [Google Scholar] [CrossRef]
- Niessen, M.; Janssen, T.; Meskers, C.; Koppe, P.; Konijnenbelt, M.; Veeger, D.J. Kinematics of the contralateral and ipsilateral shoulder: A possible relationship with post-stroke shoulder pain. J. Rehabil. Med. 2008, 40, 482–486. [Google Scholar] [CrossRef]
- Błaszczyszyn, M.; Szczęsna, A.; Konieczny, M.; Pakosz, P.; Balko, S.; Borysiuk, Z. Quantitative Assessment of Upper Limb Movement in Post-Stroke Adults for Identification of Sensitive Measures in Reaching and Lifting Activities. J. Clin. Med. 2023, 12, 3333. [Google Scholar] [CrossRef]
- Eftekhar, P.; Li, M.H.; Semple, M.J.; Richardson, D.; Brooks, D.; Mochizuki, G.; Dutta, T. Investigation of the Kinematic Upper-Limb Movement Assessment (KUMA): A Pilot Study. Physiother. Can. 2022, 74, 316–323. [Google Scholar] [CrossRef]
- Wang, Q.; Markopoulos, P.; Yu, B.; Chen, W.; Timmermans, A. Interactive wearable systems for upper body rehabilitation: A systematic review. J. Neuroeng. Rehabil. 2017, 14, 20. [Google Scholar] [CrossRef]
- Patel, S.; Hughes, R.; Hester, T.; Stein, J.; Akay, M.; Dy, J.; Bonato, P. Tracking motor recovery in stroke survivors undergoing rehabilitation using wearable technology. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 6858–6861. [Google Scholar]
- Patel, S.; Park, H.; Bonato, P.; Chan, L.; Rodgers, M. A review of wearable sensors and systems with application in rehabilitation. J. Neuroeng. Rehabil. 2012, 9, 21. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Pepper, M.G.; Yan, Y.; Spurgeon, S.K.; Sakel, M.; Phillips, M. Quantitative assessment of upper limb motion in neurorehabilitation utilizing inertial sensors. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 232–243. [Google Scholar] [CrossRef]
- Tedim Cruz, V.; Bento, V.F.; Ribeiro, D.D.; Araújo, I.; Branco, C.A.; Coutinho, P. A novel system for automatic classification of upper limb motor function after stroke: An exploratory study. Med. Eng. Phys. 2014, 36, 1704–1710. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Xiong, D.; Guo, L.; Wang, J. A remote quantitative Fugl-Meyer assessment framework for stroke patients based on wearable sensor networks. Comput. Methods Programs Biomed. 2016, 128, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.F.; Lin, Y.J.; Lin, Z.H.; Chuang, L.Y.; Hsu, W.C.; Lin, Y.H. Feasibility and efficacy of wearable devices for upper limb rehabilitation in patients with chronic stroke: A randomized controlled pilot study. Eur. J. Phys. Rehabil. Med. 2018, 54, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Cutti, A.G.; Parel, I.; Pellegrini, A.; Paladini, P.; Sacchetti, R.; Porcellini, G.; Merolla, G. The Constant score and the assessment of scapula dyskinesis: Proposal and assessment of an integrated outcome measure. J. Electromyogr. Kinesiol. 2016, 29, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Vanmechelen, I.; Haberfehlner, H.; De Vleeschhauwer, J.; Van Wonterghem, E.; Feys, H.; Desloovere, K.; Aerts, J.M.; Monbaliu, E. Assessment of movement disorders using wearable sensors during upper limb tasks: A scoping review. Front. Robot. AI 2023, 9, 1068413. [Google Scholar] [CrossRef] [PubMed]
- de-la-Fuente-Robles, Y.M.; Ricoy-Cano, A.J.; Albín-Rodríguez, A.P.; López-Ruiz, J.L.; Espinilla-Estévez, M. Past. Present and Future of Research on Wearable Technologies for Healthcare: A Bibliometric Analysis Using Scopus. Sensors 2022, 22, 8599. [Google Scholar] [CrossRef] [PubMed]
- Walmsley, C.P.; Williams, S.A.; Grisbrook, T.; Elliott, C.; Imms, C.; Campbell, A. Measurement of Upper Limb Range of Motion Using Wearable Sensors: A Systematic Review. Sports Med. Open 2018, 4, 53. [Google Scholar] [PubMed]
- Singer, B.; Garcia-Vega, J. The Fugl-Meyer Upper Extremity Scale. J. Physiother. 2017, 63, 53. [Google Scholar] [CrossRef] [PubMed]
- Cutti, A.G.; Giovanardi, A.; Rocchi, L.; Davalli, A.; Sacchetti, R. Ambulatory measurement of shoulder and elbow kinematics through inertial and magnetic sensors. Med. Biol. Eng. Comput. 2008, 46, 169–178. [Google Scholar] [CrossRef]
- Ruiz Ibán, M.A.; Paniagua Gonzalez, A.; Muraccini, M.; AsenjoGismero, C.; Varini, A.; Berardi, A.; Mantovani, M. Evaluation of a novel portable three-dimensional scapular kinematics assessment system with inter and intraobserver reproducibility and normative data for healthy adults. J. Exp. Orthop. 2020, 7, 31. [Google Scholar] [CrossRef]
- Roldán-Jiménez, C.; Cuadros-Romero, M.; Bennett, P.; Cuesta-Vargas, A.I. Differences in Tridimensional Shoulder Kinematics between Asymptomatic Subjects and Subjects Suffering from Rotator Cuff Tears by Means of Inertial Sensors: A Cross-Sectional Study. Sensors 2023, 16, 231012. [Google Scholar] [CrossRef]
- Lempereur, M.; Brochard, S.; Leboeuf, F.; Rémy-Néris, O. Validity and reliability of 3D marker based scapular motion analysis: A systematic review. J. Biomech. 2014, 47, 2219–2230. [Google Scholar] [CrossRef]
- Umehara, J.; Yagi, M.; Hirono, T.; Komamura, T.; Nishishita, S.; Ichihashi, N. Relationship between scapular initial position and scapular movement during dynamic motions. PLoS ONE 2019, 14, e0227313. [Google Scholar]
- Kazi, E.N.; Ganvir, S.S. Scapular Malalignment in Patients with Stroke: A Narrative. Int. J. Physiother. Res. 2021, 9, 4051–4057. [Google Scholar] [CrossRef]
- Price, C.I.; Franklin, P.; Rodgers, H.; Curless, R.H.; Johnson, G.R. Non-invasive evaluation of shoulder problems after stroke. Lancet 1999, 353, 298. [Google Scholar] [CrossRef] [PubMed]
- McQuade, K.J.; Smidt, G.L. Dynamic scapulohumeral rhythm: The effects of external resistance during elevation of the arm in the scapular plane. J. Orthop. Sports Phys. Ther. 1998, 27, 125–133. [Google Scholar] [CrossRef]
- Mahmoud, L.S.E.D.; Aly, S.M. The effect of scapular dyskinesia on the scapular balance angle and upper extremity sensorimotor function in stroke patients with spasticity. Bull. Fac. Phys. Ther. 2020, 25, 8. [Google Scholar] [CrossRef]
- Phadke, V.; Camargo, P.R.; Ludewig, P.M. Scapular and rotator cuff muscle activity during arm elevation: A review of normal function and alterations with shoulder impingement. Rev. Bras. Fisioter. 2009, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Molina Rueda, F.; Rivas Montero, F.M.; Pérez de Heredia Torres, M.; Alguacil Diego, I.M.; Molero Sánchez, A.; Miangolarra Page, J.C. Movement analysis of upper extremity hemiparesis in patients with cerebrovascular disease: A pilot study. Neurologija 2012, 27, 343–347. [Google Scholar] [CrossRef]
- Zadafiya, H.; Shah, D. An Effect of Scapular Position on Upper Limb Mobility among Stroke Patients in Tertiary Care Hospital: A Cross Sectional Study. Int. J. Sci. Res. 2020, 9, 272–275. [Google Scholar]
- Hou, S.; Ivanhoe, C.; Sheng, L. Botulinum toxin injection for spastic scapular dyscinesia after stroke: Case series. Medicine 2015, 94, e1300. [Google Scholar] [CrossRef]
- Meskers, C.G.; Van der Helm, F.C.; Rozing, P.M. The size of the supraspinatus outlet during elevation of the arm in the frontal and sagittal plane: A 3-D model study. Clin. Biomech. 2002, 17, 257–266. [Google Scholar] [CrossRef]
- Li, Y.; Yang, S.; Cui, L.; Bao, Y.; Gu, L.; Pan, H.; Wang, J.; Xie, Q. Prevalence, risk factor and outcome in middle-aged and elderly population affected by hemiplegic shoulder pain: An observational study. Front. Neurol. 2023, 13, 1041263. [Google Scholar]



{kind=link}
{kind=link}
| Pts | Age (Year) | Follow-Up (Months) | Paretic Side | FMA (0–15) | MAS | VAS |
|---|---|---|---|---|---|---|
| 1 | 47 | 1.5 | Left | 15 | 0 | 0 |
| 2 | 57 | 12.5 | Right | 12 | 0 | 0 |
| 3 | 58 | 36.4 | Right | 11 | 0 | 0 |
| 4 | 27 | 28.4 | Left | 10 | 1 | 0 |
| 5 | 74 | 61.8 | Right | 8 | 0 | 0 |
| 6 | 55 | 32.7 | Right | 10 | 0 | 3 |
| 7 | 58 | 13.8 | Left | 9 | 0 | 0 |
| Paretic Side | Non-Paretic Side | Ruiz Ibán et al., 2020 [29] | |
|---|---|---|---|
| RoM MaxFlex * | 121.4 (18.7) | 141.8 (17.9) | 137.6 (9.2) |
| RoM MaxAbd | 139.7 (33.6) | 171.3 (14.2) | 170.3 (13.4) |
| Scapular PR MaxFlex | 19.5 (7) | 17.8 (9.4) | |
| Scapular TI MaxFlex * | 17.0 (7.4) | 25.6 (4.7) | |
| Scapular UD MaxFlex | 33.3 (8.6) | 29.4 (8.7) | |
| Scapular PR MaxAbd | 15.5 (8.1) | 16.5 (6.8) | |
| Scapular TI MaxAbd | 17.1 (9.2) | 19.1 (8.9) | |
| Scapular UD MaxAbd | 29.4 (11.5) | 31.4 (9.7) |
| Paretic Side | Non-Paretic Side | Ruiz Ibán et al., 2020 [29] | |
|---|---|---|---|
| 30° flexion | |||
| PR | 2.3 (2.6) | 0.5 (1.6) | 1.4 (1.7) |
| UD | 5.0 (2) | 4.2 (2.2) | 2.6 (1.7) |
| TI | 2.4 (2.1) | 2.8 (3.2) | 2.5 (2.7) |
| 60° flexion | |||
| PR | 1.5 (5.3) | 0.9 (3.7) | 2.3 (2.8) |
| UD | 14.8 (4.8) | 12.8 (4.8) | 9.6 (3.1) |
| TI | 5.3 (6.2) | 6.1 (3.4) | 4.5 (4.2) |
| 90° flexion | |||
| PR | −3.3 (11.1) | −1.9 (5.3) | 1 (3.9) |
| UD | 23.7 (6.5) | 21.6 (6.5) | 18.6 (4.3) |
| TI | 10.0 (10.1) | 11.6 (3.5) | 8 (5.7) |
| 120° flexion | |||
| PR | −8.5 (8.5) | −7.3 (8.4) | −4.6 (5.2) |
| UD | 32.1 (3.1) | 25.8 (7.6) | 25.2 (5.4) |
| TI | 11.1 (13.7) | 18.9 (3.4) | 12.9 (6.6) |
| 30° abduction | |||
| PR | 1.7 (3.9) | −2.0 (5.1) | −1.7 (2.7) |
| UD | 9.1 (8.7) | 6.1 (5.8) | 3.7 (2.3) |
| TI | 2.3 (5.5) | 6.7 (3.6) | 1.9 (2.3) |
| 60° abduction | |||
| PR | 2.7 (6.8) | −2.9 (8.2) | −3.1 (3.9) |
| UD | 16.8 (10.4) | 12.9 (8.6) | 10.7 (3.4) |
| TI * | 3.5 (7.4) | 10.7 (4.9) | 4.1 (4) |
| 90° abduction | |||
| PR | 1.8 (10.4) | −3.3 (10.7) | −4 (4.8) |
| UD | 23.7 (8.8) | 17.1 (9.8) | 18.1 (4.1) |
| TI ** | 5.5 (10.5) | 14.0 (5.8) | 7.3 (5.3) |
| 120° abduction | |||
| PR | −6.3 (12.2) | −3.5 (11.5) | −3.5 (5.7) |
| UD | 32.5 (6.5) | 20.7 (10.8) | 24 (5.3) |
| TI | 7.6 (12.2) | 16.4 (6.4) | 10.3 (6.0) |
| SHR Paretic Side | SHR Non-Paretic Side | |
|---|---|---|
| 30° abduction | 3.3 | 4.9 |
| 60° abduction | 3.6 | 4.7 |
| 90° abduction | 3.8 | 5.3 |
| 120° abduction | 3.7 | 5.8 |
| Max. abduction # | 4.7 | 5.4 |
| 30° flexion | 6.0 | 7.2 |
| 60° flexion | 4.1 | 4.7 |
| 90° flexion | 3.8 | 4.2 |
| 120° flexion | 3.7 | 4.6 |
| Max. flexion § | 3.6 | 4.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longhi, M.; Donati, D.; Mantovani, M.; Casarotti, S.; Calbucci, L.; Puglisi, G.; Platano, D.; Benedetti, M.G. Feasibility of Shoulder Kinematics Assessment Using Magnetic Inertial Measurement Units in Hemiplegic Patients after Stroke: A Pilot Study. Appl. Sci. 2023, 13, 11900. https://doi.org/10.3390/app132111900
Longhi M, Donati D, Mantovani M, Casarotti S, Calbucci L, Puglisi G, Platano D, Benedetti MG. Feasibility of Shoulder Kinematics Assessment Using Magnetic Inertial Measurement Units in Hemiplegic Patients after Stroke: A Pilot Study. Applied Sciences. 2023; 13(21):11900. https://doi.org/10.3390/app132111900
Chicago/Turabian StyleLonghi, Maria, Danilo Donati, Monica Mantovani, Silvia Casarotti, Lucia Calbucci, Giulia Puglisi, Daniela Platano, and Maria Grazia Benedetti. 2023. "Feasibility of Shoulder Kinematics Assessment Using Magnetic Inertial Measurement Units in Hemiplegic Patients after Stroke: A Pilot Study" Applied Sciences 13, no. 21: 11900. https://doi.org/10.3390/app132111900