
An Update of Carbazole Treatment Strategies for COVID-19 Infection
 ,
, 
 and
and
Abstract
:1. Introduction
2. Viral Features
3. Different COVID-19 Treatments
- (A)
- Agents that target the virus proteins: S protein and viral proteases or virus RNA which are the main viral targets.
- (B)
- Agents that target host proteins that allow the virus to enter the cell, such as the enzyme ACE-2, TMPRSS2 (transmembrane protease serine 2), furin, and cathepsin-L, the proteins which can promote the attachment of viral cells such as HSPG (heparin sulfate proteoglycans), eukaryotic translation proteins such as S1R (endoplasmic reticulum chaperone protein), and transcriptional system proteins such as inosine monophosphate dehydrogenase and dihydroorotate dehydrogenase [22,23].
- (1)
- Inhibitors that block the virus from entering the human cell:
- a.
- S Protein inhibitors: plasma from convalescing infected persons, miniproteins, monoclonal antibodies, nanocods, soluble human ACE-2 protein;
- b.
- Fusion entry inhibitors;
- c.
- inhibitors of TMPRSS2, such as nitazoxanid, camostat, nafamostat, gabexat, dutasteride, bromhexine, niclosamide, and proxalutamide;
- d.
- Endosomal entry inhibitors: NIP1 inhibitors (EG00229), niclosamide, hydroxychloroquine, umifenovir, nitazoxanide; furin inhibitors (dec-RVKR-cmk); cathepsin L inhibitors (teicoplanin, SSAA09E1, K1777);
- e.
- Inhibitors of HSPG (lactoferrin).
- (2)
- Viral proteases inhibitors: inhibitors of Mpro, the main protease of the virus (lopinavir/ritonavir, PF-07321332, PF-07304814, GC376, carprofen (1, Figure 1)); viral papain-like protease inhibitors (PLpro).
- (3)
- Viral RNA inhibitors, RNA-dependent RNA polymerase (RdRp) inhibitors (AT-527, remdesivir, molnupiravir, favipiravir), host protein inhibitors that support the synthesis of viral RNA (dihydroorarate dehydrogenase inhibitor (PTC299), inosine monophosphate dehydrogenase inhibitor (merimepodib).
- (4)
- Host protein inhibitors that support the synthesis of viral protein: S1R agonists (fluvoxamine); inhibitors eEF1A (plitidepsin).
- (5)
- Viral immunomodulation inhibitors: host α/β importin inhibitors (ivermectin).
- (6)
- Agents that support natural host immunity: interferons [23].
4. Carbazoles Treatment
4.1. SARS-CoV-2 M-Pro Inhibitors
4.2. Viral-Entry Inhibitors Targeting Human ACE2
4.3. NPC1 Inhibitor
4.4. Antiviral against PLpro
4.5. Immunotherapy Treatment
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, J. Pathogenicity and Transmissibility of 2019-NcoV-A Quick Overview and Comparison with Other Emerging Viruses. Microbes Infect. 2020, 22, 69–71. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, I.; Muhammad, I.; Muhammad Waseem, M.; Basra, R.; Asim, M. Molecular Docking and Computational Exploration of Isolated Drugs from Daphne Species Against COVID-19. Iran. J. Chem. Chem. Eng. 2021, 40, 2019–2027. [Google Scholar]
- Iacopetta, D.; Ceramella, J.; Catalano, A.; Saturnino, C.; Pellegrino, M.; Mariconda, A.; Longo, P.; Sinicropi, M.S.; Aquaro, S. COVID-19 at a glance: An up-to-date overview on variants, drug design and therapies. Viruses 2022, 14, 573. [Google Scholar] [CrossRef] [PubMed]
- Dhama, K.; Khan, S.; Tiwari, R.; Sircar, S.; Bhat, S.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W.; Bonilla-Aldana, D.K.; Rodriguez Morales, A.J. Coronavirus Disease 2019–COVID-19. Clin. Microbiol. Rev. 2020, 33, e00028-20. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Halim, H.; Hajar, M.; Hasouneh, L.; Abdelmalek, S.M.A. Identification of Drug Combination Therapies for SARS-CoV-2: A Molecular Dynamics Simulations Approach. Drug Des. Dev. Ther. 2022, 16, 2995–3013. [Google Scholar] [CrossRef] [PubMed]
- WHO Virtual Press Conference on COVID-19—11 March 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/transcripts/who-audio-emergencies-coronavirus-press-conference-full-and-final-11mar2020.pdf?sfvrsn=cb432bb3_2 (accessed on 8 September 2022).
- Catalano, A.; Iacopetta, D.; Ceramella, J.; Maio, A.C.D.; Basile, G.; Giuzio, F.; Bonomo, M.G.; Aquaro, S.; Walsh, T.J.; Sinicropi, M.S.; et al. Are Nutraceuticals Effective in COVID-19 and Post-COVID Prevention and Treatment? Foods 2022, 11, 2884. [Google Scholar] [CrossRef] [PubMed]
- Al-kuraishy, H.M.; Al-Gareeb, A.I.; Alblihed, M. COVID-19 and risk of acute ischemic stroke and acute lung injury in patients with type II diabetes mellitus: The anti-infammatory role of metformin. Front. Med. 2021, 8, 644295. [Google Scholar] [CrossRef]
- Onohuean, H.; Al Kuraishy, H.M.; Al Gareeb, A.I.; Qusti, S.; Alshammari, E.M.; El Saber Batiha, G. Covid 19 and development of heart failure: Mystery and truth. Naunyn Schmiedebergs Arch. Pharmacol. 2021, 394, 2013–2021. [Google Scholar] [CrossRef]
- Velavan, T.P.; Meyer, C.G. The COVID-19 epidemic. Trop. Med. Int. Health 2020, 25, 278–280. [Google Scholar] [CrossRef] [Green Version]
- Salamanna, F.; Veronesi, F.; Martini, L.; Landini, M.P.; Fini, M. Post-COVID-19 syndrome: The persistent symptoms at the post-viral stage of the disease. A systematic review of the current data. Front. Med. 2021, 8, 653516. [Google Scholar] [CrossRef]
- Maltezou, H.; Pavli, A.; Tsakris, A. Post-COVID syndrome: An insight on its pathogenesis. Post-COVID Syndrome: An Insight on Its Pathogenesis. Vaccines 2021, 9, 497. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-de-Las-Penas, C.; Palacios-Cena, D.; Gomez-Mayordomo, V.; Cuadrado, M.L.; Florencio, L.L. Defining post-COVID symptoms (post-acute COVID, long COVID, persistent post-COVID): An integrative classification. Int. J. Environ. Res. Public Health 2021, 18, 2621. [Google Scholar] [CrossRef]
- Yang, H.; Yang, M.; Ding, Y. The crystal structures of severe acute respiratory syndrome virus main protease and its complex with an inhibitor. Proc. Natl. Acad. Sci USA 2003, 100, 13190–13195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziebuhr, J. The coronavirus replicase. Curr. Top. Microbiol. Immunol. 2005, 287, 57–94. [Google Scholar]
- Fehr, A.R.; Perlman, S. Coronaviruses: An overview of their replication and pathogenesis. In Coronaviruses: Methods and Protocols; Maier, H.J., Bickerton, E., Britton, P., Eds.; Springer: New York, NY, USA, 2015; pp. 1–23. [Google Scholar]
- Wu, C.; Liu, Y.; Yang, Y.; Zhang, P.; Zhong, W.; Wang, Y.; Wang, Q.; Xu, Y.; Li, M.; Li, X. Analysis of Therapeutic Targets for Sars-Cov-2 and Discovery of Potential Drugs by Computational Methods. Acta Pharm. Sin. B 2020, 10, 766–788. [Google Scholar] [CrossRef] [PubMed]
- Alattar, R.; Ibrahim, T.B.H.; Shaar, S.H. Abdalla, S.; Shukri, K.; Daghfal, J.N.; Khatib, M.Y.; Aboukamar, M.; Abukhattab, M.; Alsoub, H.A.; Almaslamani, M.A.; Omrani, A.S. Tocilizumab for the treatment of severe coronavirus disease 2019. J. Med. Virol. 2020, 92, 2042–2049. [Google Scholar] [CrossRef]
- Deng, L.; Li, C.; Zeng, Q. Arbidol combined with LPV/r versus LPV/r alone against Corona Virus Disease 2019: A retrospective cohort study. J. Infect. 2020, e1–e5. [Google Scholar] [CrossRef]
- Singh, A.K.; Singh, A.; Shaikh, A.; Singh, R.; Misra, A. Chloroquine and hydroxychloroquine in the treatment of COVID-19 with or without diabetes: A systematic search and a narrative review with a special reference to India and other developing countries. Diabetes Metab. Syndr. 2020, 14, 241–246. [Google Scholar] [CrossRef]
- Gavriatopoulou, M.; Ntanasis Stathopoulos, I.; Korompoki, E.; Fotiou, D.; Migkou, M.; Tzanninis, I.G.; Psaltopoulou, T.; Kastritis, E.; Terpos, E.; Dimopoulos, M.A. Emerging treatment strategies for COVID 19 infection. Clin. Experim. Med. 2021, 21, 167–179. [Google Scholar] [CrossRef]
- Dolgin. E. The race for antiviral drugs to beat COVID—And the next pandemic. Nature 2021, 592, 340–343. [Google Scholar] [CrossRef]
- Yavuz Şimşek, S.; Komşuoğlu Çelikyurt, İ. An update of anti-viral treatment of COVID-19. Turk. J. Med. Sci. 2021, 51, 3372–3390. [Google Scholar] [CrossRef] [PubMed]
- Aronskyy, I.; Masoudi-Sobhanzadeh, Y.; Cappuccio, A.; Zaslavsky, E. Advances in the computational landscape for repurposed drugs against COVID-19. Drug Discov. Today 2021, 26, 2800–2815. [Google Scholar] [CrossRef] [PubMed]
- Pushpakom, S.; Iorio, F.; Eyers, P.A. Drug repurposing: Progress, challenges and recommendations. Nat. Rev. Drug Discov. 2019, 18, 41–58. [Google Scholar] [CrossRef] [PubMed]
- Jang, W.D.; Jeon, S.; Kim, S.; Lee, S.Y. Drugs repurposed for COVID-19 by virtual screening of 6218 drugs and cell-based assay. Proc. Nat. Acad. Sci. USA 2021, 118, e2024302118. [Google Scholar] [CrossRef]
- Kumar, A.; Sharanya, C.; Abhithaj, J.; Sadasivan, C. Drug repurposing to identify therapeutics against COVID 19 with SARS-Cov-2 spike glycoprotein and main protease as targets: An in silico study. ChemRxiv 2020. [Google Scholar] [CrossRef]
- Lazniewski, M.; Dermawan, D.; Hidayat, S.; Muchtaridi, M.; Dawson, W.K.; Plewczynski, D. Drug repurposing for identification of potential spike inhibitors for SARS-CoV-2 using molecular docking and molecular dynamics simulations. Methods 2022, 203, 498–510. [Google Scholar] [CrossRef]
- Cao, B.; Wang, Y.; Wen, D. A trial of lopinavir–ritonavir in adults hospitalized with severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef]
- Tong, S.; Su, Y.; Yu, Y. Ribavirin therapy for severe COVID-19: A retrospective cohort study. Int. J. Antimicrob. Agents 2020, 56, 106114. [Google Scholar] [CrossRef]
- Farne, H.; Kumar, K.; Ritchie, A.I.; Finney, L.J.; Johnston, S.L.; Singanayagam, A. Repurposing existing drugs for the treatment of COVID-19. Ann. Am. Thorac. Soc. 2020, 17, 1186–1194. [Google Scholar] [CrossRef] [PubMed]
- Shen, Q.; Li, J.; Zhang, Z.; Guo, S.; Wang, Q.; An, X.; Chang, H. COVID-19: Systemic pathology and its implications for therapy. Int. J. Biol. Sci 2022, 18, 386–408. [Google Scholar] [CrossRef]
- Beran, A.; Mhanna, M.; Srour, O.; Ayesh, H.; Stewart, J.M.; Hjouj, M.; Khokher, W.; Mhanna, A.S.; Ghazaleh, D.; Khader, Y.; et al. Clinical significance of micronutrient supplements in patients with coronavirus disease 2019: A comprehensive systematic review and meta-analysis. Clin. Nutr. ESPEN 2022, 48, 167–177. [Google Scholar] [CrossRef]
- Anand, A.V.; Balamuralikrishnan, B.; Kaviya, M.; Bharathi, K.; Parithathvi, A.; Arun, M.; Senthilkumar, N.; Velayuthaprabhu, S.; Saradhadevi, M.; Al-Dhabi, N.A. Medicinal plants, phytochemicals, and herbs to combat viral pathogens including SARS-CoV-2. Molecules 2021, 26, 1775. [Google Scholar] [CrossRef]
- Domi, E.; Hoxha, M.; Kolovani, E.; Tricarico, D.; Zappacosta, B. The importance of nutraceuticals in COVID-19: What’s the role of resveratrol? Molecules 2022, 27, 2376. [Google Scholar] [CrossRef]
- Balboni, E.; Zagnoli, F.; Filippini, T.; Fairweather-Tait, S.J.; Vinceti, M. Zinc and selenium supplementation in COVID-19 prevention and treatment: A systematic review of the experimental studies. J. Trace Elem. Med. Biol. 2022, 71, 126956. [Google Scholar] [CrossRef]
- Jackson, C.B.; Farzan, M.; Chen, B.; Choe, H. Mechanisms of SARS-CoV-2 entry into cells. Nat. Rev. Mol. Cell Biol. 2022, 23, 3–20. [Google Scholar] [CrossRef]
- Lan, J.; He, X.; Ren, Y.; Wang, Z.; Zhou, H.; Fan, S.; Zhu, C.; Liu, D.; Shao, B.; Liu, T.-Y.; et al. Structural insights into the SARS-CoV-2 Omicron RBD-ACE2 interaction. Cell Res. 2022, 32, 593–595. [Google Scholar] [CrossRef]
- Motti, M.L.; Tafuri, D.; Donini, L.; Masucci, M.T.; De Falco, V.; Mazzeo, F. The role of nutrients in prevention, treatment and Post-Coronavirus Disease-2019 (COVID-19). Nutrients 2022, 14, 1000. [Google Scholar] [CrossRef]
- Derosa, G.; Maffioli, P.; D’Angelo, A.; Di Pierro, F. Nutraceutical approach to preventing Coronavirus Disease 2019 and related complications. Front. Immunol. 2021, 12, 582556. [Google Scholar] [CrossRef]
- Cámara, M.; Sánchez-Mata, M.; Fernández-Ruiz, V.; Cámara, R.; Cebadera, E.; Domínguez, L. A Review of the Role of Micronutrients and Bioactive Compounds on Immune System Supporting to Fight against the COVID-19 Disease. Foods 2021, 10, 1088. [Google Scholar] [CrossRef]
- Gasmi, A.; Tippairote, T.; Mujawdiya, P.K.; Peana, M.; Menzel, A.; Dadar, M.; Benahmed, A.G.; Bjørklund, G. The microbiotamediated dietary and nutritional interventions for COVID-19. Clin. Immunol. 2021, 226, 108725. [Google Scholar] [CrossRef] [PubMed]
- Shakoor, H.; Feehan, J.; Al Dhaheri, A.S.; Ali, H.I.; Platat, C.; Ismail, L.C.; Apostolopoulos, V.; Stojanovska, L. Immune-boosting role of vitamins D, C, E, zinc, selenium and omega-3 fatty acids: Could they help against COVID-19? Maturitas 2021, 143, 1–9. [Google Scholar] [CrossRef]
- Emergency Use Authorization. U.S. Food & Drug Administration. Available online: https://www.fda.gov/emergency-preparedness-and-response/mcm-legal-regulatory-and-policy-framework/emergency-use-authorization#coviddrugs (accessed on 5 December 2022).
- Gimeno, A.; Mestres-Truyol, J.; Ojeda-Montes, M.J.; Macip, G.; Saldivar-Espinoza, B.; Cereto-Massagué, A.; Pujadas, G.; Garcia-Vallvé, S. Prediction of Novel Inhibitors of the Main Protease (M-pro) of SARS-CoV-2 through Consensus Docking and Drug Reposition. Int. J. Mol. Sci. 2020, 21, 3793. [Google Scholar] [CrossRef]
- Vasanthakumar, N. Beta-Adrenergic Blockers as a Potential Treatment for COVID-19 Patients. BioEssays 2020, 42, 2000094–2000102. [Google Scholar] [CrossRef]
- Najmeddin, F.; Solhjoo, M.; Ashraf, H.; Salehi, M.; Rasooli, F.; Ghoghaei, M.; Soleimani, A.; Bahreini, M. Effects of Renin-Angiotensin-Aldosterone Inhibitors on Early Outcomes of Hypertensive COVID-19 Patients: A Randomized Triple-Blind Clinical Trial. Am. J. Hypertens. 2021, 34, 1217–1226. [Google Scholar] [CrossRef]
- Zhang, P.; Zhu, L.; Cai, J.; Lei, F.; Qin, J.J.; Xie, J.; Liu, Y.M.; Zhao, Y.C.; Huang, X.; Lin, L.; et al. Association of inpatient use of angiotensin converting enzyme inhibitors and angiotensin II receptor blockers with mortality among patients with hypertension hospitalized with COVID-19. Circ. Res. 2020, 126, 1671–1681. [Google Scholar] [CrossRef] [Green Version]
- Skayem, C.; Ayoub, N. Carvedilol and COVID-19: A potential role in reducing infectivity and infection severity of SARS-CoV-2. Am. J. Med. Sci. 2020, 360, 300. [Google Scholar] [CrossRef] [PubMed]
- Congly, S.E.; Sadler, M.D.; Abraldes, J.G.; Tandon, P.; Lee, S.S.; Burak, K.W. Practical management of esophageal varices in the context of SARS-CoV-2 (COVID19): The Alberta protocol. Can. Liver J. 2020, 3, 300–303. [Google Scholar] [CrossRef]
- Jadhav, K.P.; Jariwala, P.V. Ivabradine versus carvedilol in the management of palpitation with sinus tachycardia among recovered COVID-19 patients. J. Cardiol. Cardiovasc. Med. 2020, 1, 10–14. [Google Scholar]
- Servato, M.L.; Valente, F.X.; García-Moreno, L.G.; Casas, G.; Galera, R.F.; Burcet, G.; Teixidó-Tura, G.; Calabria, H.C.; González, I.F.; Rodríguez-Palomares, J.F. Intraventricular conundrum in a SARS-CoV-2–positive patient with elevated biomarkers of myocardial injury. JACC Case Rep. 2021, 3, 566–572. [Google Scholar] [CrossRef]
- Wadanambi, P.M.; Jayathilaka, N.; Seneviratne, K.N. A Computational Study of Carbazole Alkaloids from Murraya koenigii as Potential SARS CoV 2 Main Protease Inhibitors. Appl. Biochem. Biotechnol. 2022, 195, 573–596. [Google Scholar] [CrossRef]
- Teralı, K.; Baddal, B.; Gülcan, H.O. Prioritizing potential ACE2 inhibitors in the COVID-19 pandemic: Insights from a molecular mechanics-assisted structure-based virtual screening experiment. J. Mol. Graph. Model. 2020, 100, 107697–107706. [Google Scholar] [CrossRef] [PubMed]
- Scialo, F.; Daniele, A.; Amato, F.; Pastore, L.; Matera, M.G.; Cazzola, M.; Castaldo, G.; Bianco, A. ACE2: Te major cell entry receptor for SARS-CoV-2. Lung 2020, 198, 867–877. [Google Scholar] [CrossRef]
- Serra, A.; Fratello, M.; Federico, A.; Ojha, R.; Provenzani, R.; Tasnadi, E.; Cattelani, L.; del Giudice, G.; Kinaret, P.A.S.; Saarimäki, L.A.; et al. Computationally prioritized drugs inhibit SARS-CoV-2 infection and syncytia formation. Brief. Bioinform. 2022, 23, bbab507. [Google Scholar] [CrossRef] [PubMed]
- Cheshenko, N.; Bonanno, J.B.; Hoffmann, H.H.; Jangra, R.K.; Chandran, K.; Rice, C.M.; Almo, S.C.; Herold, B.C. Cell-impermeable staurosporine analog targets extracellular kinases to inhibit HSV and SARS-CoV-2. Commun. Biol. 2022, 5, 1096–1110. [Google Scholar] [CrossRef] [PubMed]
- Tanimoto, K.; Hirota, K.; Fukazawa, T.; Matsuo, Y.; Nomura, T.; Tanuza, N.; Hirohashi, N.; Bono, H.; Sakaguchi, T. Inhibiting SARS CoV 2 infection in vitro by suppressing its receptor, angiotensin converting enzyme 2, via aryl hydrocarbon receptor signal. Sci. Rep. 2021, 11, 16629–16640. [Google Scholar] [CrossRef] [PubMed]
- García-Dorival, I.; Cuesta-Geijo, M.A.; Barrado-Gil, L.; Galindo, I.; Garaigorta, U.; Urquiza, J.; del Puerto, A.; Campillo, N.E.; Martínez, A.; Gastaminza, P.; et al. Identification of Niemann-Pick C1 protein as a potential novel SARS-CoV-2 intracellular target. Antivir. Res. 2021, 194, 105167–105176. [Google Scholar] [CrossRef]
- Elkaeed, E.B.; Metwaly, A.M.; Alesawy, M.S.; Saleh, A.M.; Alsfouk, A.A.; Eissa, I.H. Discovery of Potential SARS-CoV-2 Papain-like Protease Natural Inhibitors Employing a Multi-Phase In Silico Approach. Life 2022, 12, 1407. [Google Scholar] [CrossRef]
- Chiang, K.C.; Rizk, J.G.; Nelson, D.J.; Krishnamurti, L.; Subbian, S.; Imig, J.D.; Khan, I.; Reddy, S.T.; Gupta, A. Ramatroban for chemoprophylaxis and treatment of COVID-19: David takes on Goliath. Expert Opin. Ther. Targ. 2022, 26, 13–28. [Google Scholar] [CrossRef]
- Ogletree, M.L.; Kulshreshta, R.; Agarwal, A.; Agarwal, A.; Gupta, A. Treatment of COVID-19 Pneumonia and Acute Respiratory Distress with Ramatroban, a Thromboxane A2 and Prostaglandin D2 Receptor Antagonist: A Four-Patient Case Series Report. Front Pharmacol. 2022, 13, 904020–904037. [Google Scholar] [CrossRef]
- Caruso, A.; Lancelot, J.C.; El-Kashef, H.; Sinicropi, M.S.; Legay, R.; Lesnard, A.; Rault, S. A Rapid and Versatile Synthesis of Novel Pyrimido[5,4-b]carbazoles. Tetrahedron 2009, 65, 10400–10405. [Google Scholar] [CrossRef]
- Iacopetta, D.; Rosano, C.; Puoci, F.; Parisi, O.I.; Saturnino, C.; Caruso, A.; Longo, P.; Ceramella, J.; Malzert-Fréon, A.; Dallemagne, P.; et al. Multifaceted Properties of 1,4-Dimethylcarbazoles: Focus on Trimethoxybenzamide and Trimethoxyphenylurea Derivatives as Novel Human Topoisomerase II Inhibitors. Eur. J. Pharm. Sci. 2017, 96, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Caruso, A.; Chimento, A.; El-Kashef, H.; Lancelot, J.C.; Panno, A.; Pezzi, V.; Saturnino, C.; Sinicropi, M.S.; Sirianni, R.; Rault, S. Antiproliferative Activity of Some 1,4-Dimethylcarbazoles on Cells That Express Estrogen Receptors: Part, I. J. Enzym. Inhib. Med. Chem. 2012, 27, 609–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caruso, A.; Voisin-Chiret, A.S.; Lancelot, J.C.; Sinicropi, M.S.; Garofalo, A.; Rault, S. Efficient and Simple Synthesis of 6-Aryl-1,4-Dimethyl-9H-Carbazoles. Molecules 2008, 13, 1312–1320. [Google Scholar] [CrossRef] [PubMed]
- Sinicropi, M.S.; Iacopetta, D.; Rosano, C.; Randino, R.; Caruso, A.; Saturnino, C.; Muià., N.; Ceramella, J.; Puoci, F.; Rodriquez, M.; et al. N-thioalkylcarbazoles derivatives as new anti-proliferative agents: Synthesis, characterisation and molecular mechanism evaluation. J. Enzym. Inhib. Med. Chem. 2018, 33, 434–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caruso, A.; Barbarossa, A.; Carocci, A.; Salzano, G.; Sinicropi, M.S.; Saturnino, C. Carbazole derivatives as STAT inhibitors: An overview. Appl. Sci. 2021, 11, 6192. [Google Scholar] [CrossRef]
- Saturnino, C.; Iacopetta, D.; Sinicropi, M.S.; Rosano, C.; Caruso, A.; Caporale, A.; Marra, N.; Marengo, B.; Pronzato, M.A.; Parisi, O.I.; et al. N-alkyl carbazole derivatives as new tools for Alzheimer’s disease: Preliminary studies. Molecules 2014, 19, 9307–9317. [Google Scholar] [CrossRef]
- Gupta, A.; Chiang, K.C. Prostaglandin D2 as a mediator of lymphopenia and a therapeutic target in COVID-19 disease. Med. Hypotheses 2020, 143, 110122–110124. [Google Scholar] [CrossRef]
- Gimeno, A.; Ojeda-Montes, M.; Tomás-Hernández, S.; Cereto-Massagué, A.; Beltrán-Debón, R.; Mulero, M.; Pujadas, G.; Garcia-Vallvé, S. The Light and Dark Sides of Virtual Screening: What Is There to Know? Int. J. Mol. Sci. 2019, 20, 1375. [Google Scholar] [CrossRef] [Green Version]
- Mody, V.; Ho, J.; Wills, S.; Mawri, A.; Lawson, L.; Ebert, M.C.; Fortin, G.M.; Rayalam, S.; Taval, S. Identifcation of 3-chymotrypsin like protease (3CLPro) inhibitors as potential anti-SARSCoV-2 agents. Commun. Biol. 2021, 4, 93. [Google Scholar] [CrossRef]
- Shin, D.; Mukherjee, R.; Grewe, D.; Bojkova, D.; Baek, K.; Bhattacharya, A.; Schulz, L.; Widera, M.; Mehdipour, A.R.; Tascher, G.; et al. Papain-like protease regulates SARS-CoV-2 viral spread and innate immunity. Nature 2020, 587, 657–662. [Google Scholar] [CrossRef]
- Báez-Santos, Y.M.; John, S.E.S.; Mesecar, A.D. The SARS-coronavirus papain-like protease: Structure, function and inhibition by designed antiviral compounds. Antivir. Res. 2015, 115, 21–38. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Lin, D.; Sun, X.; Curth, U.; Drosten, C.; Sauerhering, L.; Becker, S.; Rox, K.; Hilgenfeld, R. Crystal structure of SARS-CoV-2 main protease provides a basis for design of improved α-ketoamide inhibitors. Science 2020, 368, 409–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, R.; Yang, G.; Xue, R.; Liu, M.; Wang, F.; Hu, J.; Guo, X.; Chang, S. COVID-19 Docking Server: A meta server for docking small molecules, peptides and antibodies against potential targets of COVID-19. Bioinformatics 2020, 36, 5109–5111. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.; He, F.; Liu, D.; He, F.; Wu, T.; Fang, M.; Niu, Z.; Wu, Z.; Xu, D. AI-aided design of novel targeted covalent inhibitors against SARS-CoV-2. Biomolecules 2022, 12, 746. [Google Scholar] [CrossRef]
- Zhou, Y.; Hou, Y.; Shen, J.; Huang, Y.; Martin, W.; Cheng, F. Network-based drug repurposing for novel coronavirus 2019-nCoV/SARS-CoV-2. Cell Discov. 2020, 6, 14. [Google Scholar] [CrossRef] [Green Version]
- Amirshahrokhi, K.; Khalili, A.R. Carvedilol attenuates paraquatinduced lung injury by inhibition of proinfammatory cytokines, chemokine MCP-1, NF-κB activation and oxidative stress mediators. Cytokine 2016, 88, 144–153. [Google Scholar] [CrossRef]
- Owen, L.; Laird, K.; Shivkumar, M. Antiviral plant-derived natural products to combat RNA viruses: Targets throughout the viral life cycle. Lett. Appl. Microbiol. 2021, 75, 476–499. [Google Scholar] [CrossRef]
- Balakrishnan, R.; Vijayraja, D.; Jo, S.H.; Ganesan, P.; Su-Kim, I.; Choi, D.K. Medicinal profle, phytochemistry, and pharmacological activities of Murraya koenigii and its primary bioactive compounds. Antioxidants 2020, 9, 101. [Google Scholar] [CrossRef] [Green Version]
- Caruso, A.; Ceramella, J.; Iacopetta, D.; Saturnino, C.; Mauro, M.V.; Bruno, R.; Aquaro, S.; Sinicropi, M.S. Carbazole Derivatives as Antiviral Agents: An Overview. Molecules 2019, 24, 1912. [Google Scholar] [CrossRef] [Green Version]
- Schultes, S.; De Graaf, C.; Haaksma, E.E.; De Esch, I.J.; Leurs, R.; Krämer, O. Ligand efciency as a guide in fragment hit selection and optimization. Drug Discov. Today Technol. 2010, 7, e157–e162. [Google Scholar] [CrossRef] [Green Version]
- Guo, Z. The modifcation of natural products for medical use. Acta Pharm. Sin. B. 2017, 7, 119–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sampath, D.; Cortes, J.; Estrov, Z.; Du, M.; Shi, Z.; Andreeff, M.; Gandhi, V.; Plunkett, W. Pharmacodynamics of cytarabine alone and in combination with 7- hydroxystaurosporine (UCN-01) in AML blasts in vitro and during a clinical trial. Blood 2006, 107, 2517–2524. [Google Scholar] [CrossRef] [Green Version]
- Santos, F.P.S.; Kantarjian, H.; Cortes, J.; Quintas-Cardama, A. Bafetinib, a dual BcrAbl/Lyn tyrosine kinase inhibitor for the potential treatment of leukemia. Curr. Opin. Investig. Drugs 2010, 11, 1450–1465. [Google Scholar] [PubMed]
- Matsuyama, S.; Nao, N.; Shirato, K.; Kawase, M.; Saito, S.; Takayama, I.; Nagata, N.; Sekizuka, T.; Katoh, H.; Kato, F.; et al. Enhanced isolation of SARS-CoV-2 by TMPRSS2-expressing cells. Proc. Natl. Acad. Sci. USA 2020, 117, 7001–7003. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compound | Name | Reference |
|---|---|---|
| SARS-CoV-2 M-pro inhibitors | ||
| 1 | Carprofen 2-(6-Chloro-9H-carbazol-2yl)propanoic acid | [45] |
| 2 | Carvedilol 1-(9H-Carbazol-4-yloxy)-3-[2-(2-methoxyphenoxy) ethylamino]propan-2-ol | [5,9,17,46,47,48,49,50,51,52] |
| 3 | Koenigicine 8-Methoxy-3,3,5-trimethyl-11H-pyrano[3,2-a]carbazol-9-ol | [53] |
| 4 | Mukonicine 9,11-Dimethoxy-3,3,5-trimethyl-11H-pyrano[3,2-a]carbazole | [53] |
| 5 | O-methylmurrayamine A 9-Methoxy-3,3,5-trimethyl-11H-pyrano[3,2-a]carbazole | [53] |
| 6 | Koenine 3,3,5-Trimethyl-11H-pyrano[3,2-a]carbazol-8-ol | [53] |
| 7 | Girinimbine 3,11-Dihydro-3,3,5-trimethyl-pyrano[3,2-a]carbazole | [53] |
| Viral-entry inhibitors targeting human ACE2 | ||
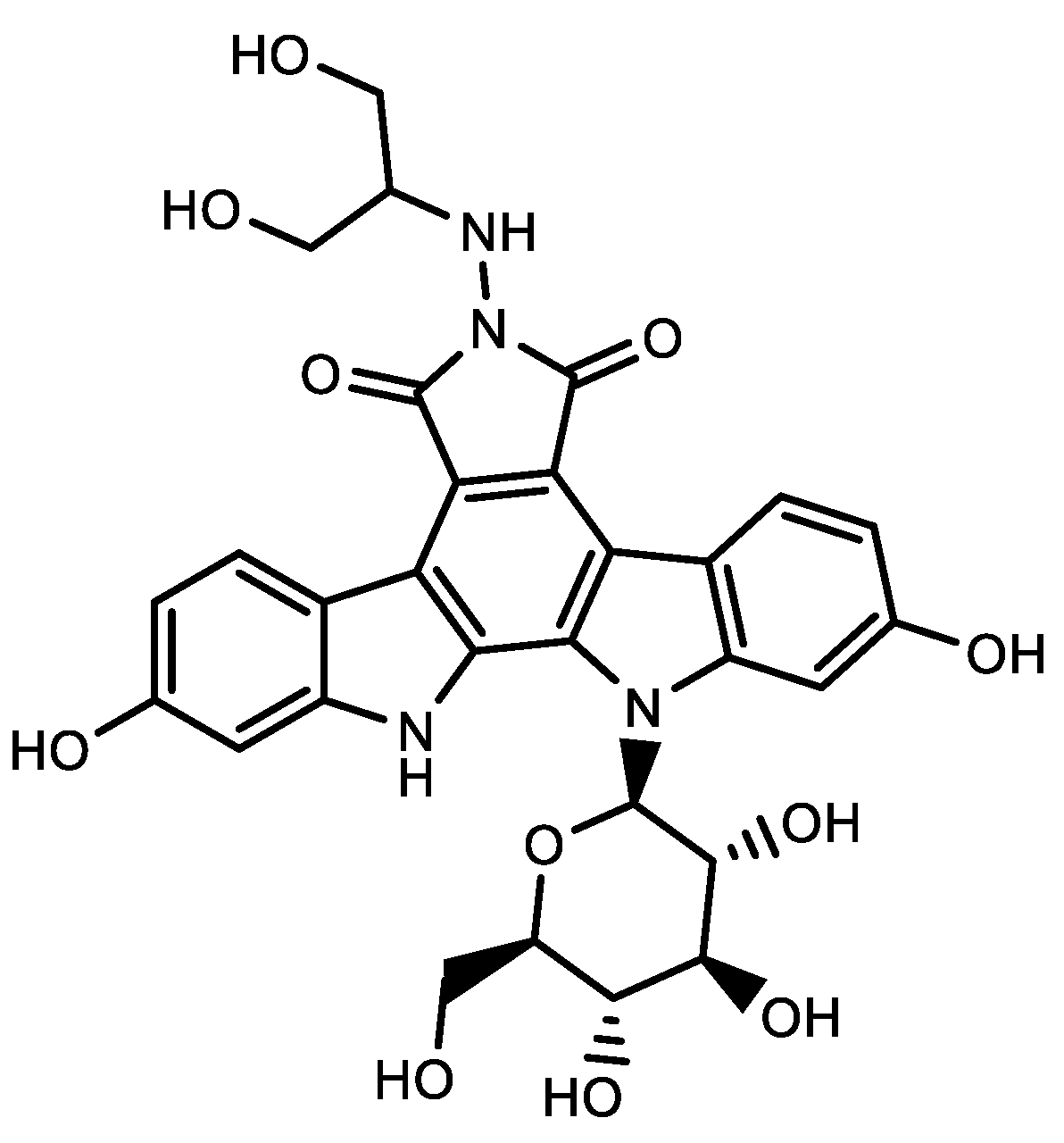
| 8 | Edotecarin 6-((1,3-Dihydroxypropan-2-yl)amino)-2,10-dihydroxy-12-((2R,3R,4S,5S,6R)-3,4,5-trihydroxy-6-(hydroxymethyl)tetrahydro-2H-pyran-2-yl)-12,13-dihydro-5H-indolo[2,3-a]pyrrolo[3,4-c]carbazole-5,7(6H)-dione | [54,55] |
| 9 | 7-Hydroxystaurosporine (5S,6R,7R,9R,16R)-16-hydroxy-6-methoxy-5-methyl-7-(methylamino)-6,7,8,9,15,16-hexahydro-17-oxa-4b,9a,15-triaza-5,9-methanodibenzo[b,h]cyclonona[jkl]cyclopenta[e]-as-indacen-14(5H)-one | [56] |
| 10 | CIMSSNa sodium 3-(4-(((S)-5-((5S,7S,8R,9S)-8-methoxy-9-methyl-16-oxo-6,7,8,9,15,16-hexahydro-5H,14H-4b,9a,15-triaza-5,9-methanodibenzo[b,h]cyclonona[jkl]cyclopenta[e]-as-indacen-7-yl)-4-oxohexanamido)methyl)-1H-1,2,3-triazol-1-yl)propane-1-sulfonate | [57] |
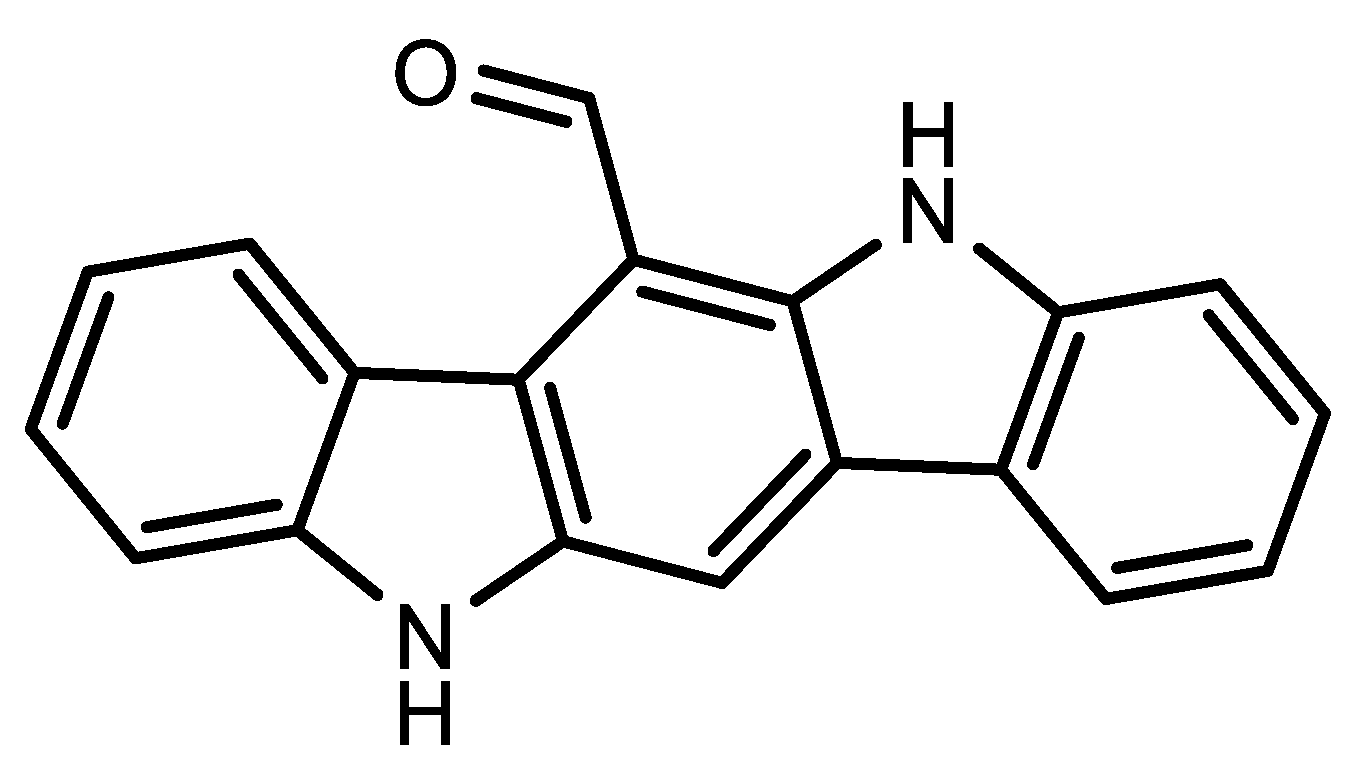
| 11 | 6-Formylindolo(3,2-b)carbazole | [58] |
| NPC1 inhibitor | ||
| 12 | 2-((2-(1-Benzylpiperidin-4-yl)ethyl)amino)-N-(9H-carbazol-9-yl)acetamide | [59] |
| Antiviral against PLpro | ||
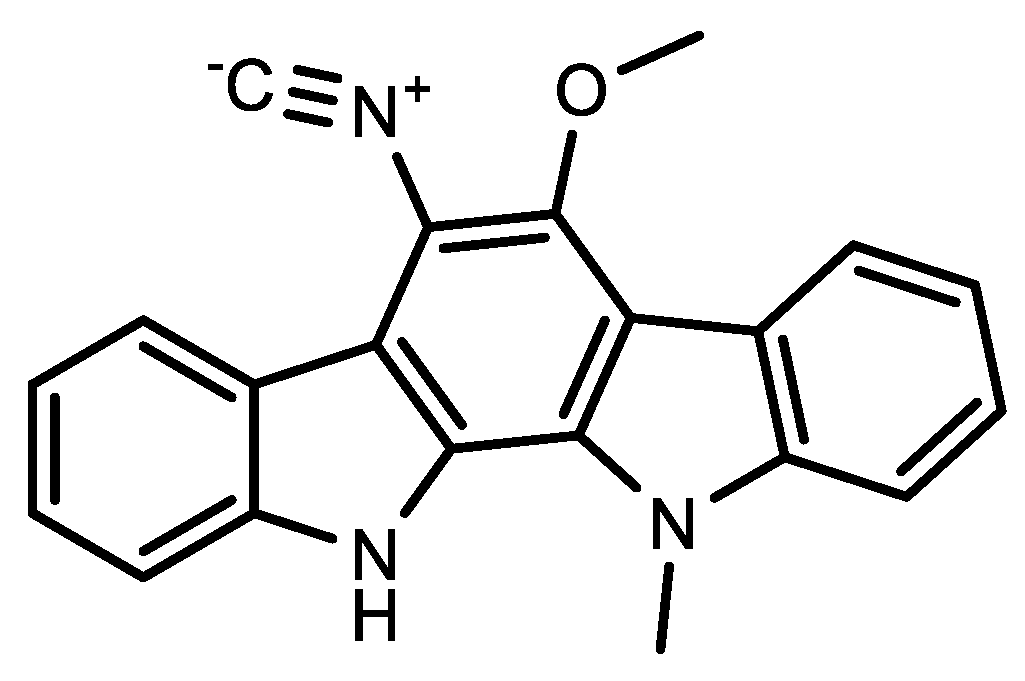
| 13 | 6-Cyano-5-methoxy-12-methylindolo [2, 3A] carbazole | [60] |
| Immunotherapy treatment | ||
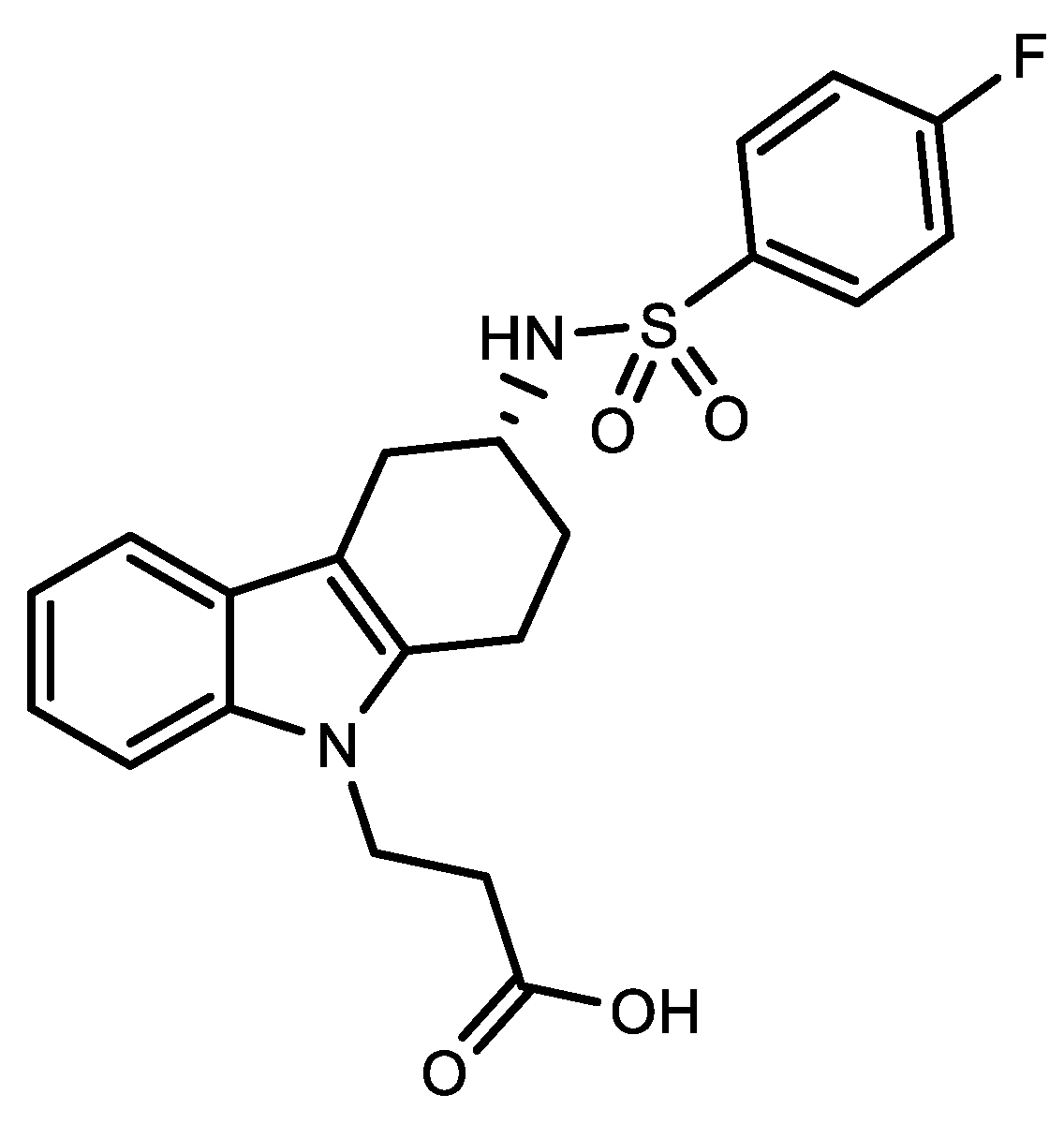
| 14 | Ramatroban 3-[(3R)-3-[(4-fluorophenyl)sulfonylamino]-1,2,3,4-tetrahydrocarbazol-9-yl]propanoic acid | [53,61,62] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonomo, M.G.; Caruso, A.; El-Kashef, H.; Salzano, G.; Sinicropi, M.S.; Saturnino, C. An Update of Carbazole Treatment Strategies for COVID-19 Infection. Appl. Sci. 2023, 13, 1522. https://doi.org/10.3390/app13031522
Bonomo MG, Caruso A, El-Kashef H, Salzano G, Sinicropi MS, Saturnino C. An Update of Carbazole Treatment Strategies for COVID-19 Infection. Applied Sciences. 2023; 13(3):1522. https://doi.org/10.3390/app13031522
Chicago/Turabian StyleBonomo, Maria Grazia, Anna Caruso, Hussein El-Kashef, Giovanni Salzano, Maria Stefania Sinicropi, and Carmela Saturnino. 2023. "An Update of Carbazole Treatment Strategies for COVID-19 Infection" Applied Sciences 13, no. 3: 1522. https://doi.org/10.3390/app13031522