
Carbazoles: Role and Functions in Fighting Diabetes

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Carbazole Derivatives in the Pathogenesis of Diabetes
2.1. Carvedilol
2.2. 1,2,4-Triazine-Carbazoles
2.3. Sulfonamide Carbazole and Carbazole-Containing Cyclic Urea
2.4. Carbazole Triazoles
2.5. Tetrahydrocarbazole Derivatives
2.6. Carbazole Alkaloids
2.7. Carbazole-Ethoxy-Phenyl Propionic Acid Derivative
2.8. Chiglitazar
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kitabchi, A.E.; Umpierrez, G.E.; Miles, J.M.; Fisher, J.N. Hyperglycemic Crises in Adult Patients with Diabetes. Diabetes Care 2009, 32, 1335–1343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baron, A.D. Postprandial Hyperglycaemia and Alpha-Glucosidase Inhibitors. Diabetes Res Clin Pract. 1998, 40, S51–S55. [Google Scholar] [CrossRef] [PubMed]
- Lebovitz, H.E. Effect of the Postprandial State on Nontraditional Risk Factors. Am. J. Cardiol. 2001, 88, 5H–20H. [Google Scholar] [CrossRef]
- Deshpande, A.D.; Harris-Hayes, M.; Schootman, M. Epidemiology of Diabetes and Diabetes-Related Complications. Phys. Ther. 2008, 88, 1254–1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Candales, A. Metabolic Syndrome X: A Comprehensive Review of the Pathophysiology and Recommended Therapy. J. Med. 2001, 32, 283–300. [Google Scholar]
- Wang, G.; Wang, J.; He, D.; Li, X.; Li, J.; Peng, Z. Synthesis and Biological Evaluation of Novel 1,2,4-Triazine Derivatives Bearing Carbazole Moiety as Potent α-Glucosidase Inhibitors. Bioorg. Med. Chem. Lett. 2016, 26, 2806–2809. [Google Scholar] [CrossRef] [PubMed]
- Farahani-Zangaraki, M.; Taheri, A.; Etebari, M. Niosome-Carvedilol Protects DNA Damage of Supraphysiologic Concentrations of Insulin Using Comet Assay: An in Vitro Study. Hum. Exp. Toxicol. 2021, 40, S150–S157. [Google Scholar] [CrossRef]
- Singh, K.; Maity, P.; Krug, L.; Meyer, P.; Treiber, N.; Lucas, T.; Basu, A.; Kochanek, S.; Wlaschek, M.; Geiger, H.; et al. Superoxide Anion Radicals Induce IGF-1 Resistance through Concomitant Activation of PTP 1 B and PTEN. EMBO Mol. Med. 2015, 7, 59–77. [Google Scholar] [CrossRef]
- Rostoker, R.; Bitton-Worms, K.; Caspi, A.; Shen-Orr, Z.; LeRoith, D. Investigating New Therapeutic Strategies Targeting Hyperinsulinemia’s Mitogenic Effects in a Female Mouse Breast Cancer Model. Endocrinology 2013, 154, 1701–1710. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.J.; Yi, Y.W.; Kim, H.J.; Hong, Y.B.; Seong, Y.S.; Bae, I. BRCA1 Negatively Regulates IGF-1 Expression through an Estrogen-Responsive Element-like Site. Cell Death Dis. 2012, 3, e336. [Google Scholar] [CrossRef] [Green Version]
- Babiker, A.; Dubayee, M. Anti-Diabetic Medications: How to Make a Choice? Sudan J. Paediatr. 2017, 17, 11–20. [Google Scholar] [CrossRef]
- Saturnino, C.; Grande, F.; Aquaro, S.; Caruso, A.; Iacopetta, D.; Bonomo, M.G.; Longo, P.; Schols, D.; Sinicropi, M.S. Chloro-1,4-Dimethyl-9H-Carbazole Derivatives Displaying Anti-HIV Activity. Molecules 2018, 23, 286. [Google Scholar] [CrossRef] [Green Version]
- Ceramella, J.; Iacopetta, D.; Barbarossa, A.; Caruso, A.; Grande, F.; Bonomo, M.G.; Mariconda, A.; Longo, P.; Carmela, S.; Sinicropi, M.S. Carbazole Derivatives as Kinase-Targeting Inhibitors for Cancer Treatment. Mini Rev. Med. Chem. 2020, 20, 444–465. [Google Scholar] [CrossRef]
- Grande, F.; de Bartolo, A.; Occhiuzzi, M.A.; Caruso, A.; Rocca, C.; Pasqua, T.; Carocci, A.; Rago, V.; Angelone, T.; Sinicropi, M.S. Carbazole and Simplified Derivatives: Novel Tools toward β-Adrenergic Receptors Targeting. Appl. Sci. 2021, 11, 5486. [Google Scholar] [CrossRef]
- Caruso, A.; Voisin-Chiret, A.S.; Lancelot, J.C.; Sinicropi, M.S.; Garofalo, A.; Rault, S. Efficient and Simple Synthesis of 6-Aryl-1,4-Dimethyl-9H-Carbazoles. Molecules 2008, 13, 1312–1320. [Google Scholar] [CrossRef]
- Chakraborty, D.P. Chapter 4 Chemistry and Biology of Carbazole Alkaloids. Alkaloids Chem. Pharmacol. 1993, 44, 257–364. [Google Scholar] [CrossRef]
- Sinicropi, M.S.; Iacopetta, D.; Rosano, C.; Randino, R.; Caruso, A.; Saturnino, C.; Muià, N.; Ceramella, J.; Puoci, F.; Rodriquez, M.; et al. N-Thioalkylcarbazoles Derivatives as New Anti-Proliferative Agents: Synthesis, Characterisation and Molecular Mechanism Evaluation. J. Enzym. Inhib. Med. Chem. 2018, 33, 434–444. [Google Scholar] [CrossRef] [Green Version]
- Bashir, M.; Bano, A.; Ijaz, A.S.; Chaudhary, B.A. Recent Developments and Biological Activities of N-Substituted Carbazole Derivatives: A Review. Molecules 2015, 20, 13496–13517. [Google Scholar] [CrossRef] [Green Version]
- Caruso, A.; Chimento, A.; El-Kashef, H.; Lancelot, J.C.; Panno, A.; Pezzi, V.; Saturnino, C.; Sinicropi, M.S.; Sirianni, R.; Rault, S. Antiproliferative Activity of Some 1,4-Dimethylcarbazoles on Cells That Express Estrogen Receptors: Part, I.J. Enzym. Inhib. Med. Chem. 2012, 27, 609–613. [Google Scholar] [CrossRef] [Green Version]
- Caruso, A.; Sinicropi, M.S.; Lancelot, J.C.; El-Kashef, H.; Saturnino, C.; Aubert, G.; Ballandonne, C.; Lesnard, A.; Cresteil, T.; Dallemagne, P.; et al. Synthesis and Evaluation of Cytotoxic Activities of New Guanidines Derived from Carbazoles. Bioorg. Med. Chem. Lett. 2014, 24, 467–472. [Google Scholar] [CrossRef]
- Panno, A.; Sinicropi, M.S.; Caruso, A.; El-Kashef, H.; Lancelot, J.C.; Aubert, G.; Lesnard, A.; Cresteil, T.; Rault, S. New Trimethoxybenzamides and Trimethoxyphenylureas Derived from Dimethylcarbazole as Cytotoxic Agents. Part, I.J. Heterocycl. Chem. 2014, 51, E294–E302. [Google Scholar] [CrossRef]
- Humphries, P.S.; Bersot, R.; Kincaid, J.; Mabery, E.; McCluskie, K.; Park, T.; Renner, T.; Riegler, E.; Steinfeld, T.; Turtle, E.D.; et al. Carbazole-Containing Amides and Ureas: Discovery of Cryptochrome Modulators as Antihyperglycemic Agents. Bioorg. Med. Chem. Lett. 2018, 28, 293–297. [Google Scholar] [CrossRef]
- Sinicropi, M.; Lappano, R.; Caruso, A.; Santolla, M.; Pisano, A.; Rosano, C.; Capasso, A.; Panno, A.; Lancelot, J.; Rault, S.; et al. (6-Bromo-1,4-Dimethyl-9H-Carbazol-3-Yl-Methylene)-Hydrazine (Carbhydraz) Acts as a GPER Agonist in Breast Cancer Cells. Curr. Top. Med. Chem. 2015, 15, 1035–1042. [Google Scholar] [CrossRef] [PubMed]
- Saturnino, C.; Caruso, A.; Iacopetta, D.; Rosano, C.; Ceramella, J.; Muià, N.; Mariconda, A.; Bonomo, M.G.; Ponassi, M.; Rosace, G.; et al. Inhibition of Human Topoisomerase II by N,N,N-Trimethylethanammonium Iodide Alkylcarbazole Derivatives. ChemMedChem 2018, 13, 2635–2643. [Google Scholar] [CrossRef] [PubMed]
- Saturnino, C.; Sinicropi, M.S.; Iacopettab, D.; Ceramella, J.; Caruso, A.; Muià, N.; Longo, P.; Rosace, G.; Galletta, M.; Ielo, I.; et al. N-Thiocarbazole-Based Gold Nanoparticles: Synthesis, Characterization and Anti-Proliferative Activity Evaluation. IOP Conf. Ser. Mater. Sci. Eng. 2018, 459, 012023. [Google Scholar] [CrossRef]
- Caruso, A.; Ceramella, J.; Iacopetta, D.; Saturnino, C.; Mauro, M.V.; Bruno, R.; Aquaro, S.; Sinicropi, M.S. Carbazole Derivatives as Antiviral Agents: An Overview. Molecules 2019, 24, 1912. [Google Scholar] [CrossRef] [Green Version]
- Nodari, S.; Metra, M.; Dei Cas, A.; Dei Cas, L. Efficacy and Tolerability of the Long-Term Administration of Carvedilol in Patients with Chronic Heart Failure with and without Concomitant Diabetes Mellitus. Eur. J. Heart Fail. 2003, 5, 803–809. [Google Scholar] [CrossRef] [Green Version]
- Kveiborg, B.; Hermann, T.S.; Major-Pedersen, A.; Christiansen, B.; Rask-Madsen, C.; Raunsø, J.; Køber, L.; Torp-Pedersen, C.; Dominguez, H. Metoprolol Compared to Carvedilol Deteriorates Insulin-Stimulated Endothelial Function in Patients with Type 2 Diabetes—A Randomized Study. Cardiovasc Diabetol 2010, 9, 21. [Google Scholar] [CrossRef] [Green Version]
- Vardeny, O.; Nicholas, G.; Andrei, A.; Buhr, K.A.; Hermanson, M.P.; Moran, J.J.; Detry, M.A.; Stein, J.H. β-AR Polymorphisms and Glycemic and Lipid Parameters in Hypertensive Individuals Receiving Carvedilol or Metoprolol. Am. J. Hypertens. 2012, 25, 920–926. [Google Scholar] [CrossRef] [Green Version]
- Nardotto, G.H.B.; Coelho, E.B.; Paiva, C.E.; Lanchote, V.L. Effects of Type 2 Diabetes Mellitus in Patients on Treatment with Glibenclamide and Metformin on Carvedilol Enantiomers Metabolism. J. Clin. Pharm. 2017, 57, 760–769. [Google Scholar] [CrossRef]
- Nardotto, G.H.B.; Lanchote, V.L.; Coelho, E.B.; della Pasqua, O. Population Pharmacokinetics of Carvedilol Enantiomers and Their Metabolites in Healthy Subjects and Type-2 Diabetes Patients. Eur. J. Pharm. Sci. 2017, 109, S108–S115. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.V.; Ta, Q.V.; Dang, T.B.; Nguyen, P.H.; Nguyen, T.; Pham, T.V.H.; Nguyen, T.H.T.; Baker, S.; le Tran, T.; Yang, D.J.; et al. Carvedilol Improves Glucose Tolerance and Insulin Sensitivity in Treatment of Adrenergic Overdrive in High Fat Diet-Induced Obesity in Mice. PLoS ONE 2019, 14, e0224674. [Google Scholar] [CrossRef]
- Amirshahrokhi, K.; Zohouri, A. Carvedilol Prevents Pancreatic β-Cell Damage and the Development of Type 1 Diabetes in Mice by the Inhibition of Proinflammatory Cytokines, NF-ΚB, COX-2, INOS and Oxidative Stress. Cytokine 2021, 138, 155394. [Google Scholar] [CrossRef] [PubMed]
- Rahim, F.; Ullah, H.; Javid, M.T.; Wadood, A.; Taha, M.; Ashraf, M.; Shaukat, A.; Junaid, M.; Hussain, S.; Rehman, W.; et al. Synthesis, in vitro evaluation and molecular docking studies of thiazole derivatives as new inhibitors of α-glucosidase. Bioorg. Chem. 2015, 62, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Humphries, P.S.; Bersot, R.; Kincaid, J.; Mabery, E.; McCluskie, K.; Park, T.; Renner, T.; Riegler, E.; Steinfeld, T.; Turtle, E.D.; et al. Carbazole-Containing Sulfonamides and Sulfamides: Discovery of Cryptochrome Modulators as Antidiabetic Agents. Bioorg. Med. Chem. Lett. 2016, 26, 757–760. [Google Scholar] [CrossRef]
- Iqbal, S.; Khan, M.A.; Javaid, K.; Sadiq, R.; Fazal-ur-Rehman, S.; Choudhary, M.I.; Basha, F.Z. New Carbazole Linked 1,2,3-Triazoles as Highly Potent Non-Sugar α-Glucosidase Inhibitors. Bioorg. Chem. 2017, 74, 72–81. [Google Scholar] [CrossRef]
- Zhang, J.Q.; Li, S.M.; Ma, X.; Zhong, G.; Chen, R.; Li, X.S.; Zhu, G.F.; Zhou, B.; Guo, B.; Wu, H.S.; et al. Discovery of Tetrahydrocarbazoles with Potent Hypoglycemic and Hypolipemic Activities. Eur. J. Med. Chem. 2018, 150, 102–112. [Google Scholar] [CrossRef]
- Wang, L.L.; Du, Y.; Li, S.M.; Cheng, F.; Zhang, N.N.; Chen, R.; Cui, X.; Yang, S.G.; Fan, L.L.; Wang, J.T.; et al. Design, Synthesis and Evaluation of Tetrahydrocarbazole Derivatives as Potential Hypoglycemic Agents. Bioorg. Chem. 2021, 115, 105172. [Google Scholar] [CrossRef]
- Biswas, A.; Bhattacharya, S.; Dasgupta, S.; Kundu, R.; Roy, S.S.; Pal, B.C.; Bhattacharya, S. Insulin Resistance Due to Lipid-Induced Signaling Defects Could Be Prevented by Mahanine. Mol. Cell Biochem. 2010, 336, 97–107. [Google Scholar] [CrossRef]
- Uvarani, C.; Jaivel, N.; Sankaran, M.; Chandraprakash, K.; Ata, A.; Mohan, P.S. Axially Chiral Biscarbazoles and Biological Evaluation of the Constituents from Murraya Koenigii. Fitoterapia 2014, 94, 10–20. [Google Scholar] [CrossRef]
- Nooron, N.; Athipornchai, A.; Suksamrarn, A.; Chiabchalard, A. Mahanine Enhances the Glucose-Lowering Mechanisms in Skeletal Muscle and Adipocyte Cells. Biochem. Biophys. Res. Commun. 2017, 494, 101–106. [Google Scholar] [CrossRef]
- Patel, O.P.S.; Mishra, A.; Maurya, R.; Saini, D.; Pandey, J.; Taneja, I.; Raju, K.S.R.; Kanojiya, S.; Shukla, S.K.; Srivastava, M.N.; et al. Naturally Occurring Carbazole Alkaloids from Murraya Koenigii as Potential Antidiabetic Agents. J. Nat. Prod. 2016, 79, 1276–1284. [Google Scholar] [CrossRef]
- Sauerberg, P.; Pettersson, I.; Jeppesen, L.; Bury, P.S.; Mogensen, J.P.; Wassermann, K.; Brand, C.L.; Sturis, J.; Wöldike, H.F.; Fleckner, J.; et al. Novel Tricyclic-Alpha-Alkyloxyphenylpropionic Acids: Dual PPARalpha/Gamma Agonists with Hypolipidemic and Antidiabetic Activity. J. Med. Chem. 2002, 45, 789–804. [Google Scholar] [CrossRef]
- Deeks, E.D. Chiglitazar: First Approval. Drugs 2022, 82, 87–92. [Google Scholar] [CrossRef]
- Ji, L.; Song, W.; Fang, H.; Li, W.; Geng, J.; Wang, Y.; Guo, L.; Cai, H.; Yang, T.; Li, H.; et al. Efficacy and Safety of Chiglitazar, a Novel Peroxisome Proliferator-Activated Receptor Pan-Agonist, in Patients with Type 2 Diabetes: A Randomized, Double-Blind, Placebo-Controlled, Phase 3 Trial (CMAP). Sci. Bull. Beijing 2021, 66, 1571–1580. [Google Scholar] [CrossRef]
- Li, X.; Yu, J.; Wu, M.; Li, Q.; Liu, J.; Zhang, H.; Zhu, X.; Li, C.; Zhang, J.; Ning, Z.; et al. Pharmacokinetics and Safety of Chiglitazar, a Peroxisome Proliferator-Activated Receptor Pan-Agonist, in Patients. Clin. Pharm. Drug Dev. 2021, 10, 789–796. [Google Scholar] [CrossRef]
- Hercek, R.; Skoda, A.; Proksa, B. Process for Preparation of Carvedilol. U.S. Patent 2006/0167077A1, 19 May 2009. [Google Scholar]
- Berridge, M.S.; Nelson, A.D.; Zheng, L.; Leisure, G.P.; Miraldi, F. Specific Beta-Adrenergic Receptor Binding of Carazolol Measured with PET. J. Nucl. Med. 1994, 35, 1665–1676. [Google Scholar]
- Fonarow, G.C. Role of Carvedilol Controlled-Release in Cardiovascular Disease. Expert. Rev. Cardiovasc. Ther. 2009, 7, 483–498. [Google Scholar] [CrossRef]
- Ahmad, A. Carvedilol Can Replace Insulin in the Treatment of Type 2 Diabetes Mellitus. J. Diabetes Metab. 2017, 8, 2. [Google Scholar] [CrossRef]
- Bakris, G.L.; Fonseca, V.; Katholi, R.E.; McGill, J.B.; Messerli, F.H.; Phillips, R.A.; Raskin, P.; Wright, J.T.; Oakes, R.; Lukas, M.A.; et al. Metabolic Effects of Carvedilol vs Metoprolol in Patients with Type 2 Diabetes Mellitus and Hypertension: A Randomized Controlled Trial. JAMA 2004, 292, 2227–2236. [Google Scholar] [CrossRef] [Green Version]
- Seferović, P.M.; Petrie, M.C.; Filippatos, G.S.; Anker, S.D.; Rosano, G.; Bauersachs, J.; Paulus, W.J.; Komajda, M.; Cosentino, F.; de Boer, R.A.; et al. Type 2 Diabetes Mellitus and Heart Failure: A Position Statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2018, 20, 853–872. [Google Scholar] [CrossRef] [Green Version]
- Dézsi, C.A.; Szentes, V. The Real Role of B-Blockers in Daily Cardiovascular Therapy. Am. J. Cardiovasc. Drugs 2017, 17, 361–373. [Google Scholar] [CrossRef]
- Jacob, S.; Rett, K.; Wicklmayr, M.; Agrawal, B.; Augustin, H.J.; Dietze, G.J. Differential Effect of Chronic Treatment with Two Beta-Blocking Agents on Insulin Sensitivity: The Carvedilol-Metoprolol Study. J. Hypertens. 1996, 14, 489–494. [Google Scholar] [CrossRef]
- Refsgaard, J.; Thomsen, C.; Andreasen, F.; Gøtzsche, O. Carvedilol Does Not Alter the Insulin Sensitivity in Patients with Congestive Heart Failure. Eur. J. Heart Fail. 2002, 4, 445–453. [Google Scholar] [CrossRef]
- Yue, T.L.; Cheng, H.Y.; Lysko, P.G.; McKenna, P.J.; Feuerstein, R.; Gu, J.L.; Lysko, K.A.; Davis, L.L.; Feuerstein, G. Carvedilol, a New Vasodilator and Beta Adrenoceptor Antagonist, Is an Antioxidant and Free Radical Scavenger. J. Pharm. Exp. Ther. 1992, 263, 92–98. [Google Scholar]
- Afonso, R.A.; Patarrao, R.S.; Macedo, M.P.; Carmo, M.M. Carvedilol Action Is Dependent on Endogenous Production of Nitric Oxide. Am. J. Hypertens. 2006, 19, 419–425. [Google Scholar] [CrossRef] [Green Version]
- Ehrenborg, E.; Skogsberg, J.; Ruotolo, G.; Large, V.; Eriksson, P.; Arner, P.; Hamsten, A. The Q/E27 Polymorphism in the Beta2-Adrenoceptor Gene Is Associated with Increased Body Weight and Dyslipoproteinaemia Involving Triglyceride-Rich Lipoproteins. J. Intern. Med. 2000, 247, 651–656. [Google Scholar] [CrossRef] [Green Version]
- González Sánchez, J.L.; Proenza, A.M.; Martínez Larrad, M.T.; Ramis, J.M.; Fernández Pérez, C.; Palou, A.; Serrano Ríos, M. The Glutamine 27 Glutamic Acid Polymorphism of the Beta2-Adrenoceptor Gene Is Associated with Abdominal Obesity and Greater Risk of Impaired Glucose Tolerance in Men but Not in Women: A Population-Based Study in Spain. Clin. Endocrinol. Oxf. 2003, 59, 476–481. [Google Scholar] [CrossRef]
- Suresha, R.N.; Ashwini, V.; Pragathi, B.; Kalabharathi, H.L.; Satish, A.M.; Pushpa, V.H.; Jayanthi, M.K.; Snehalatha, P. The Effect of Carvedilol on Blood Glucose Levels in Normal Albino Rats. J. Clin. Diagn. Res. 2013, 7, 1900–1903. [Google Scholar] [CrossRef]
- Farhat, R.; Su, G.; Sejling, A.S.; Knight, N.; Fisher, S.J.; Chan, O. Carvedilol Prevents Counterregulatory Failure and Impaired Hypoglycaemia Awareness in Non-Diabetic Recurrently Hypoglycaemic Rats. Diabetologia 2019, 62, 676–686. [Google Scholar] [CrossRef] [Green Version]
- Mishra, J.; Löbmann, K.; Grohganz, H.; Rades, T. Influence of Preparation Technique on Co-Amorphization of Carvedilol with Acidic Amino Acids. Int. J. Pharm. 2018, 552, 407–413. [Google Scholar] [CrossRef]
- Ross, S.A.; Gulve, E.A.; Wang, M. Chemistry and Biochemistry of Type 2 Diabetes. Chem. Rev. 2004, 104, 1255–1282. [Google Scholar] [CrossRef]
- Bass, J. Circadian Topology of Metabolism. Nature 2012, 491, 348–356. [Google Scholar] [CrossRef]
- Marcheva, B.; Ramsey, K.M.; Peek, C.B.; Affinati, A.; Maury, E.; Bass, J. Circadian Clocks and Metabolism. Handb. Exp. Pharm. 2013, 217, 127–155. [Google Scholar] [CrossRef] [Green Version]
- Renström, F.; Koivula, R.W.; Varga, T.V.; Hallmans, G.; Mulder, H.; Florez, J.C.; Hu, F.B.; Franks, P.W. Season-Dependent Associations of Circadian Rhythm-Regulating Loci (CRY1, CRY2 and MTNR1B) and Glucose Homeostasis: The GLACIER Study. Diabetologia 2015, 58, 997–1005. [Google Scholar] [CrossRef] [Green Version]
- Machicao, F.; Peter, A.; Machann, J.; Konigsrainer, I.; Bohm, A.; Lutz, S.Z.; Heni, M.; Fritsche, A.; Schick, F.; Konigsrainer, A.; et al. Glucose-Raising Polymorphisms in the Human Clock Gene Cryptochrome 2 (CRY2) Affect Hepatic Lipid Content. PLoS ONE 2016, 11, e0145563. [Google Scholar] [CrossRef]
- Kelly, M.A.; Rees, S.D.; Hydriem, Z.L.; Shera, A.S.; Bellary, S.; O’Hare, J.P.; Kumar, S.; Taheri, S.; Basit, A.; Barnett, A.H. Circadian Gene Variants and Susceptibility to Type 2 Diabetes: A Pilot Study. PLoS ONE 2012, 7, e32670. [Google Scholar] [CrossRef] [Green Version]
- Dashti, H.S.; Smith, C.E.; Lee, Y.C.; Parnell, L.D.; Lai, C.Q.; Arnett, D.K.; Ordovás, J.M.; Garaulet, M. CRY1 Circadian Gene Variant Interacts with Carbohydrate Intake for Insulin Resistance in Two Independent Populations: Mediterranean and North American. Chronobiol. Int. 2014, 31, 660–667. [Google Scholar] [CrossRef] [Green Version]
- Hardie, D.G. AMP-Activated Protein Kinase: Maintaining Energy Homeostasis at the Cellular and Whole-Body Levels. Annu. Rev. Nutr. 2014, 34, 31–55. [Google Scholar] [CrossRef] [Green Version]
- Herzig, S.; Shaw, R.J. AMPK: Guardian of Metabolism and Mitochondrial Homeostasis. Nat. Rev. Mol. Cell Biol. 2018, 19, 121–135. [Google Scholar] [CrossRef] [Green Version]
- Caruso, A.; Barbarossa, A.; Carocci, A.; Salzano, G.; Sinicropi, M.S.; Saturnino, C. Carbazole Derivatives as STAT Inhibitors: An Overview. Appl. Sci. 2021, 11, 6192. [Google Scholar] [CrossRef]
- Caruso, A.; Iacopetta, D.; Puoci, F.; Rita Cappello, A.; Saturnino, C.; Stefania Sinicropi, M. Carbazole Derivatives: A Promising Scenario for Breast Cancer Treatment. Mini-Rev. Med. Chem. 2016, 16, 630–643. [Google Scholar] [CrossRef] [PubMed]
- Santomauro, A.T.M.G.; Boden, G.; Silva, M.E.R.; Rocha, D.M.; Santos, R.F.; Ursich, M.J.M.; Strassmann, P.G.; Wajchenberg, B.L. Overnight Lowering of Free Fatty Acids with Acipimox Improves Insulin Resistance and Glucose Tolerance in Obese Diabetic and Nondiabetic Subjects. Diabetes 1999, 48, 1836–1841. [Google Scholar] [CrossRef] [PubMed]
- Willson, T.M.; Cobb, J.E.; Cowan, D.J.; Wiethe, R.W.; Correa, I.D.; Prakash, S.R.; Beck, K.D.; Moore, L.B.; Kliewer, S.A.; Lehmann, J.M. The Structure-Activity Relationship between Peroxisome Proliferator-Activated Receptor Gamma Agonism and the Antihyperglycemic Activity of Thiazolidinediones. J. Med. Chem. 1996, 39, 665–668. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.J.; Winegar, D.A.; Plunket, K.D.; Moore, L.B.; Lewis, M.C.; Wilson, J.G.; Sundseth, S.S.; Koble, C.S.; Wu, Z.; Chapman, J.M.; et al. A Ureido-Thioisobutyric Acid (GW9578) Is a Subtype-Selective PPARalpha Agonist with Potent Lipid-Lowering Activity. J. Med. Chem. 1999, 42, 3785–3788. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.L.; Blanchard, S.G.; Boswell, G.E.; Charifson, P.S.; Cobb, J.E.; Henke, B.R.; Hull-Ryde, E.A.; Kazmierski, W.M.; Lake, D.H.; Leesnitzer, L.M.; et al. N-(2-Benzoylphenyl)-L-Tyrosine PPARgamma Agonists. 2. Structure-Activity Relationship and Optimization of the Phenyl Alkyl Ether Moiety. J. Med. Chem. 1998, 41, 5037–5054. [Google Scholar] [CrossRef] [PubMed]
- Henke, B.R.; Blanchard, S.G.; Brackeen, M.F.; Brown, K.K.; Cobb, J.E.; Collins, J.L.; Harrington, W.W.; Hashim, M.A.; Hull-Ryde, E.A.; Kaldor, I.; et al. N-(2-Benzoylphenyl)-L-Tyrosine PPARgamma Agonists. 1. Discovery of a Novel Series of Potent Antihyperglycemic and Antihyperlipidemic Agents. J. Med. Chem. 1998, 41, 5020–5036. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DRUG CLASS | MECHANISM OF ACTION | MORE COMMON SIDE EFFECTS AND DISADVANTAGES |
|---|---|---|
| BIGUANIDES: Metformin | AMP-Kinase activation; Decrease in hepatic glucose production. | Gastrointestinal side effects (diarrhea, abdominal cramping); Lactic acidosis risk; Vit B12 deficiency; Hypoxia; Dehydration. |
| SULPHONYLUREAS: Glibenclamide Gliclazide Glipizide Glimepiride | Closure of KATP channels on β cell plasma membranes; Increase in insulin secretion. | Hypoglycemia; Weight gain. |
| GLINIDES (MEGLITINIDES): Repaglinide Nateglinide | Closure of KATP channels on β cell plasma membranes; Increase in insulin secretion. | Hypoglycemia; Weight gain. |
| α-GLUCOSIDASE INHIBITORS: Acarbose Miglitol | Inhibition of intestinal α-glucosidase; Intestinal carbohydrate digestion and absorption reduction. | Generally modest HbA1c efficacy; Gastrointestinal side effects (flatulence, diarrhea). |
| THIAZOLIDINEDIONES (TZDs): Pioglitazone Rosiglitazone Lobeglitazone | Nuclear transcription factor PPAR-γ activation; Increase in insulin sensitivity. | Weight gain; Edema; Heart failure; Bone fractures. |
| DPP4 INHIBITORS (GLIPTINS): Sitagliptin Vildagliptin Saxagliptin Alogliptin Alogliptin Linagliptin | DPP-4 inhibition; Increase in postprandial active incretin (GLP-1, GIP) concentrations; Increase in glucose-dependent insulin secretion; Decrease in glucose-dependent glucagon secretion. | Generally modest HbA1c efficacy; Urticaria; Angioedema. |
| GLP-1 AGONISTS: Exenatide Liraglutide Lixisenatide Dulaglutide | GLP-1 receptors activation; Increase in glucose-dependent insulin secretion; Decrease in glucose-dependent glucagon secretion.; Slowing of gastric emptying; Satiety increase. | Gastrointestinal side effects (nausea/vomiting); Pancreatitis; C-cell hyperplasia. |
| SGLT2 INHIBITORS: Dapagliflozin Empagliflozin Canagliflozin | Block of sodium/glucose cotransporter 2 (SGLT2) in renal tubules Reduction of glucose reabsorption in the kidney; Decrease in serum blood glucose level. | Renal failure; Increased risk of genital and urinary trac fungal infection; Increased risk of euglycemic diabetic ketoacidosis. |
| AMYLIN ANALOGUES Pramlintide | Amylin receptors activation; Glucagon secretion reduction; Slowing of gastric emptying; Satiety increase. | Generally modest HbA1c efficacy; Gastrointestinal side effects Hypoglycemia. |
| Compound | Name | Biological Activity | References |
|---|---|---|---|
| 1 (Synthetic compound) | Carvedilol (1-(9H-carbazol-4-yloxy)-3-[2-(2-methoxyphenoxy)ethylamino]propan-2-ol) | Reduction of insulin resistance by sensitizing insulin receptors and inhibiting the sympathetic nervous system Beneficial effects on left ventricular function, resting and exercise hemodynamics and clinical conditions Stimulation of endothelial NO production Beneficial effects on endothelial dysfunction caused by oxidative stress Long-term benefits on glucose metabolism Blockade of adrenergic hyperactivation Prevention of pancreatic β-cell damage Inhibition of inflammatory and oxidative mediators | [7,27,28,29,30,31,32,33] |
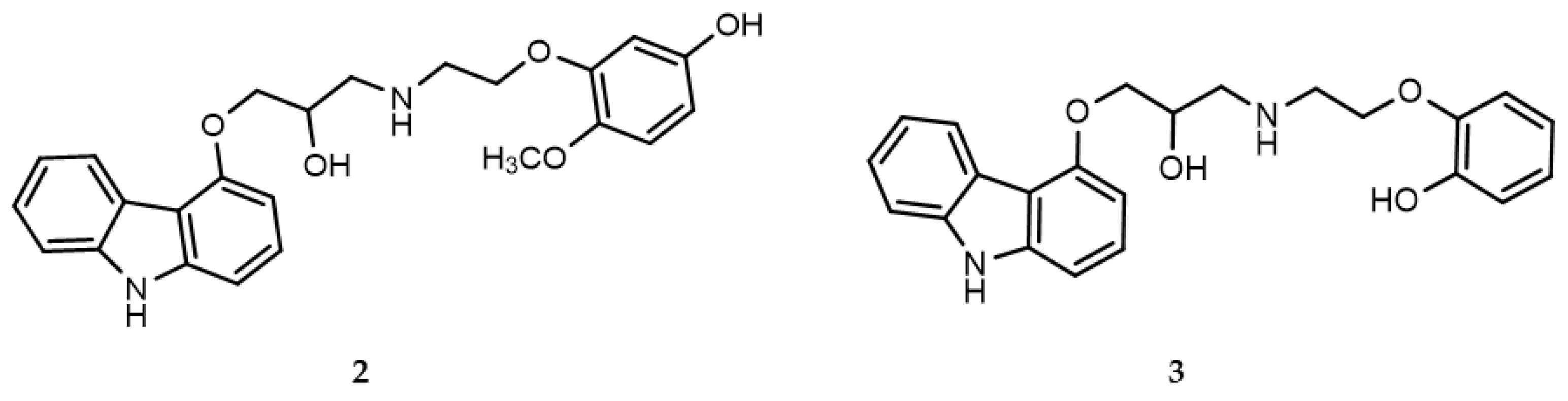
| 2 | Hydroxyphenyl-carvedilol (OHC) 4-[2-[[3-(9H-Carbaz-ol-4-yloxy)-2-hydroxypro-pyl]amino]ethoxy]-3-methoxyphenol | Metabolite of carvedilol | [30] |
| 3 | O-Desmethylcarvedilol (DMC) 2-[2-[[3-(9H-Carbaz-ol-4-yloxy)-2-hydroxypro-pyl]amino]ethoxy]phenol | Metabolite of carvedilol | [30] |
| 4 (Synthetic compound) | 1-((5,6-Di(furan-2-yl)-1,2,4-triazin-3-yl)thio)-3-(3,6-dibromo-9H-carbazol-9-yl)propan-2-ol | α-Glucosidase inhibition (IC50 = 4.27 ± 0.07 µM) | [6,34] |
| 5 (Synthetic compound) | 2-(3-(9H-Carbazol-9-yl)-2-hydroxypropyl)isothiazoline-1,1-dioxide | Cryptochrome modulator | [35] |
| 6 (Synthetic compound) | 1-(3-(3,6-Difluoro-9H-carbazol-9-yl)-2-hydroxypropyl)imidazolidin-2-one | Cryptochrome modulator | [22] |
| 7 (Synthetic compound) | 2-(4-((9H-Carbazol-9-yl)methyl)-1H-1,2,3-triazol-1-yl)-1-(3-bromo-4-hydroxyphenyl) ethanone | α-Glucosidase inhibition (IC50 = 1.0 ± 0.057 µM) | [36] |
| 8 (Synthetic compound) | 9-((1-(Pyridin-3-yl-methyl)-1H-1,2,3-triazol-4-yl) methyl)-9H-carbazole | α-Glucosidase inhibition (IC50 = 0.8 ± 0.01 µM) | [36] |
| 9 (Synthetic compound) | 6-(Benzyloxy)-9-(4-chlorobenzoyl)-2,3,4,9-tetrahydro-1H-carbazole-3-carboxylic acid | Hypoglycemic effect via the AMPK pathway | [37] |
| 10 (Synthetic compound) | Ethyl 8-(benzyloxy)-5-(4-chlorobenzoyl)-7-fluoro-3,4-dihydro-1H-pyrido[4,3-b]indole-2(5H)-carboxylate | Hypoglycemic effect via the AMPK pathway | [38] |
| 11 (Naturalcompound) | Mahanine 3,5-Dimethyl-3-(4-methylpent-3-enyl)-11H-pyrano[3,2-a]carbazol-9-ol | Prevention of insulin resistance due to lipid induced signaling defects α-Glucosidase inhibition (IC50 = 21.4 ± 0.4 μM) Antioxidant properties Increase in the translocation of GLUT4 protein from intracellular vesicles into the plasma fraction and glucose uptake through the activation of phosphorylation of Akt | [39,40,41] |
| 12 (Naturalcompound) | Bisgerayafoline D 3,3′-Bis((E)-3,7-dimethylocta-2,6-dien-1-yl)-9′-methoxy-3,3′,5,5′-tetramethyl-3,3′,11,11′-tetrahydro-[9,10′-bipyrano[3,2-a]carbazol]-10-ol | Antioxidant and α-glucosidase properties | [40] |
| 13 (Naturalcompound) | Bismahanimbinol 3,3′,5,5′-Tetramethyl-3,3′-bis(4-methylpent-3-en-1-yl)-3,3′,11,11′-tetrahydro-[9,10′-bipyrano[3,2-a]carbazol]-8-ol | Antioxidant and α-glucosidase properties | [40] |
| 14 (Naturalcompound) | Bispyrayafoline 3,3′,5,5′-Tetramethyl-3,3′-bis(4-methylpent-3-en-1-yl)-3,3′,11,11′-tetrahydro-[10,10′-bipyrano [3,2-a]carbazole]-9,9′-diol | Antioxidant and α-glucosidase properties | [40] |
| 15 (Naturalcompound) | O-Methyl mahanine 9-Methoxy-3,5-dimethyl-3-(4-methylpent-3-en-1-yl)-3,11-dihydropyrano[3,2-a]carbazole | Antioxidant and α-glucosidase properties | [40] |
| 16 (Naturalcompound) | O-Methyl mukonal Koenimbine 8-Methoxy-3,3,5-trimethyl-11H-pyrano[3,2-a]carbazole | Antioxidant and α-glucosidase properties Antidiabetic activity in L6-GLUT4 myc myotubes | [40,42] |
| 17 (Naturalcompound) | O-Methylmurrayamine A 9-Methoxy-3,3,5-trimethyl-11H-pyrano[3,2-a]carbazole | Antidiabetic activity in L6-GLUT4 myc myotubes Decrease in blood glucose profile | [42] |
| 18 (Naturalcompound) | Koenidine 8,9-Dimethoxy-3,3,5-trimethyl-11H-pyrano [3,2-a]carbazole | Antidiabetic activity in L6-GLUT4myc myotubes Increase in insulin sensitivity and progressive reduction of blood glucose level | [42] |
| 19 (Naturalcompound) | Mahanimbine 3,5-Dimethyl-3-(4-methylpent-3-enyl)-11H-pyrano[3,2-a]carbazole | Antidiabetic activity in L6-GLUT4myc myotubes | [42] |
| 20 (Naturalcompound) | Murrayazoline (14R,17S,19S)-3,13,13,17-Tetramethyl-21-oxa-12-azahexacyclo[10.7.1.12,17.05,20.06,11.014,19]henicosa-1,3,5(20),6,8,10-hexaene | Antidiabetic activity in L6-GLUT4myc myotubes | [42] |
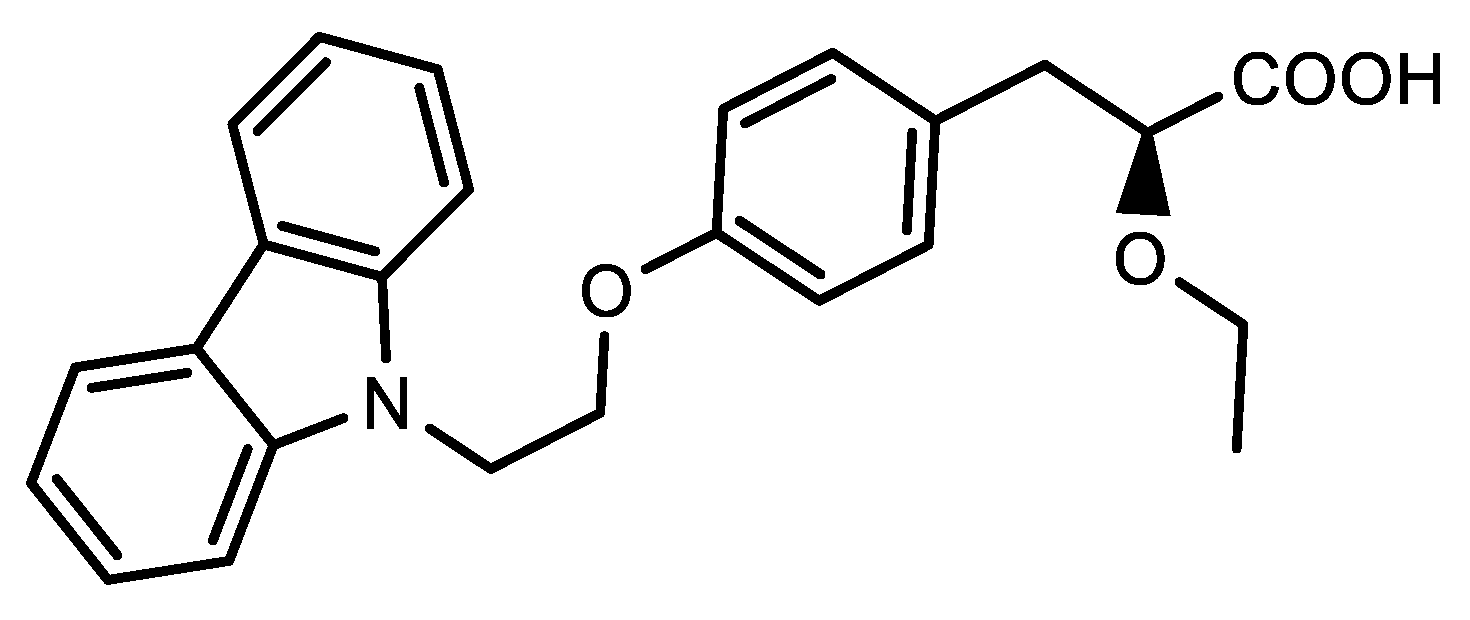
| 21 (Synthetic compound) | (S)-3-(4-(2-(9H-Carbazol-9-yl)ethoxy)phenyl)-2-ethoxypropanoic acid | Improve of the insulin sensitivity Activity on PPARR and PPARγ | [43] |
| 22 (Synthetic compound) | Chiglitazar (2S)-3-[4-(2-Carbazol-9-ylethoxy)phenyl]-2-[2-(4-fluorobenzoyl)anilino]propanoic acid | Reduction of glycosylated hemoglobin A1c (HbA1c) Hypoglycemic effect Increase in insulin sensitivity Reduction of triglycerides | [44,45,46] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grande, F.; Ioele, G.; Caruso, A.; Occhiuzzi, M.A.; El-Kashef, H.; Saturnino, C.; Sinicropi, M.S. Carbazoles: Role and Functions in Fighting Diabetes. Appl. Sci. 2023, 13, 349. https://doi.org/10.3390/app13010349
Grande F, Ioele G, Caruso A, Occhiuzzi MA, El-Kashef H, Saturnino C, Sinicropi MS. Carbazoles: Role and Functions in Fighting Diabetes. Applied Sciences. 2023; 13(1):349. https://doi.org/10.3390/app13010349
Chicago/Turabian StyleGrande, Fedora, Giuseppina Ioele, Anna Caruso, Maria Antonietta Occhiuzzi, Hussein El-Kashef, Carmela Saturnino, and Maria Stefania Sinicropi. 2023. "Carbazoles: Role and Functions in Fighting Diabetes" Applied Sciences 13, no. 1: 349. https://doi.org/10.3390/app13010349