

Photodynamic Therapy in Non-Surgical Treatment of Periodontitis: A Systematic Review and Meta-Analysis
 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Question
- -
- In patients with untreated periodontitis, does the application of photodynamic therapy (aPDT) provide additional effects to traditional treatment with manual and mechanical instruments when comparing the patient’s clinical parameters?
- -
- In patients with untreated periodontitis, does the application of photodynamic therapy (aPDT) provide additional effects to traditional treatment with manual and mechanical instruments when comparing the patient’s microbiological parameters?
2.2. Search Strategy
3. Results
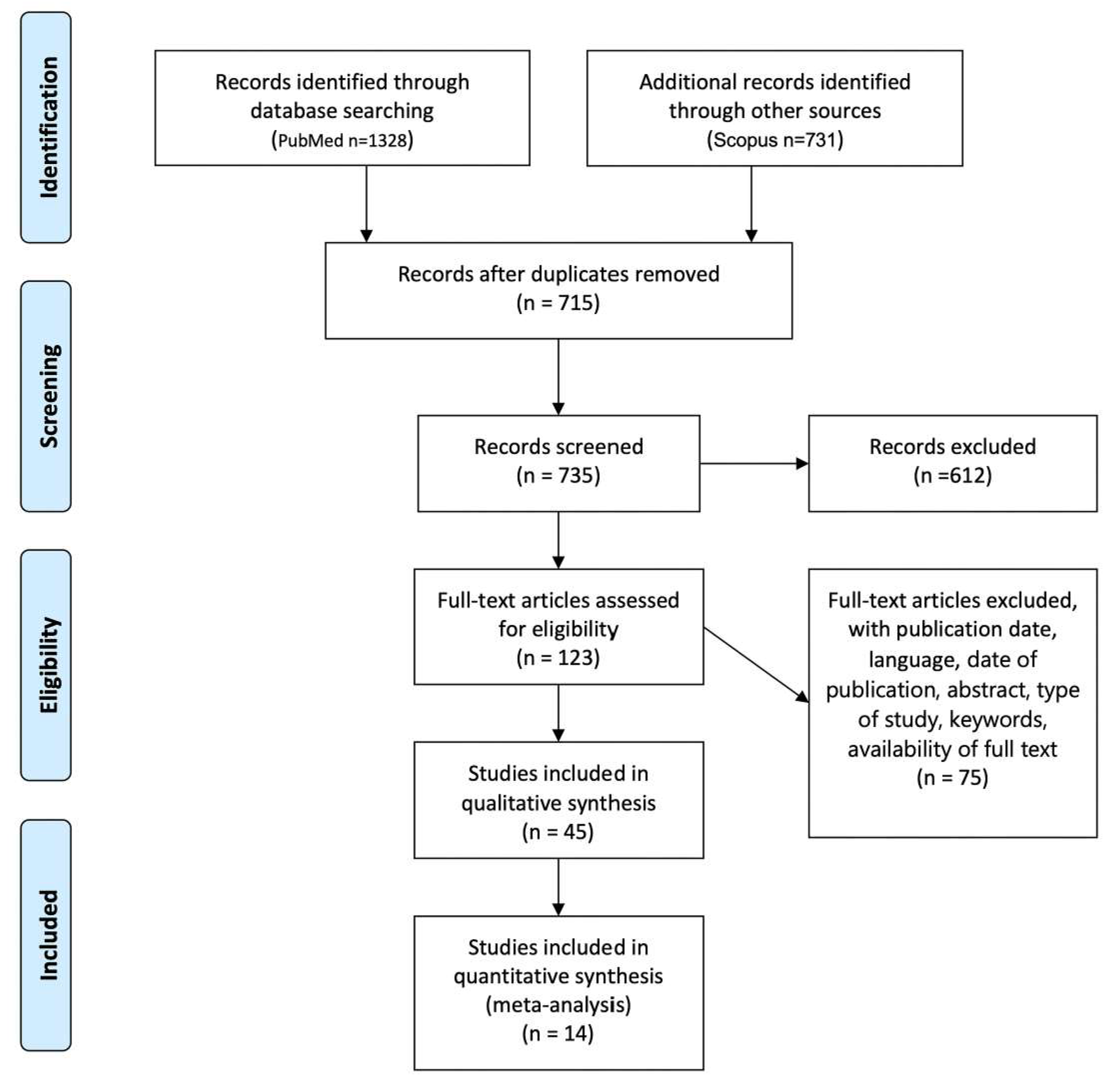
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Main Outcome of the Study
3.4. Microbiological Outcome of the Study
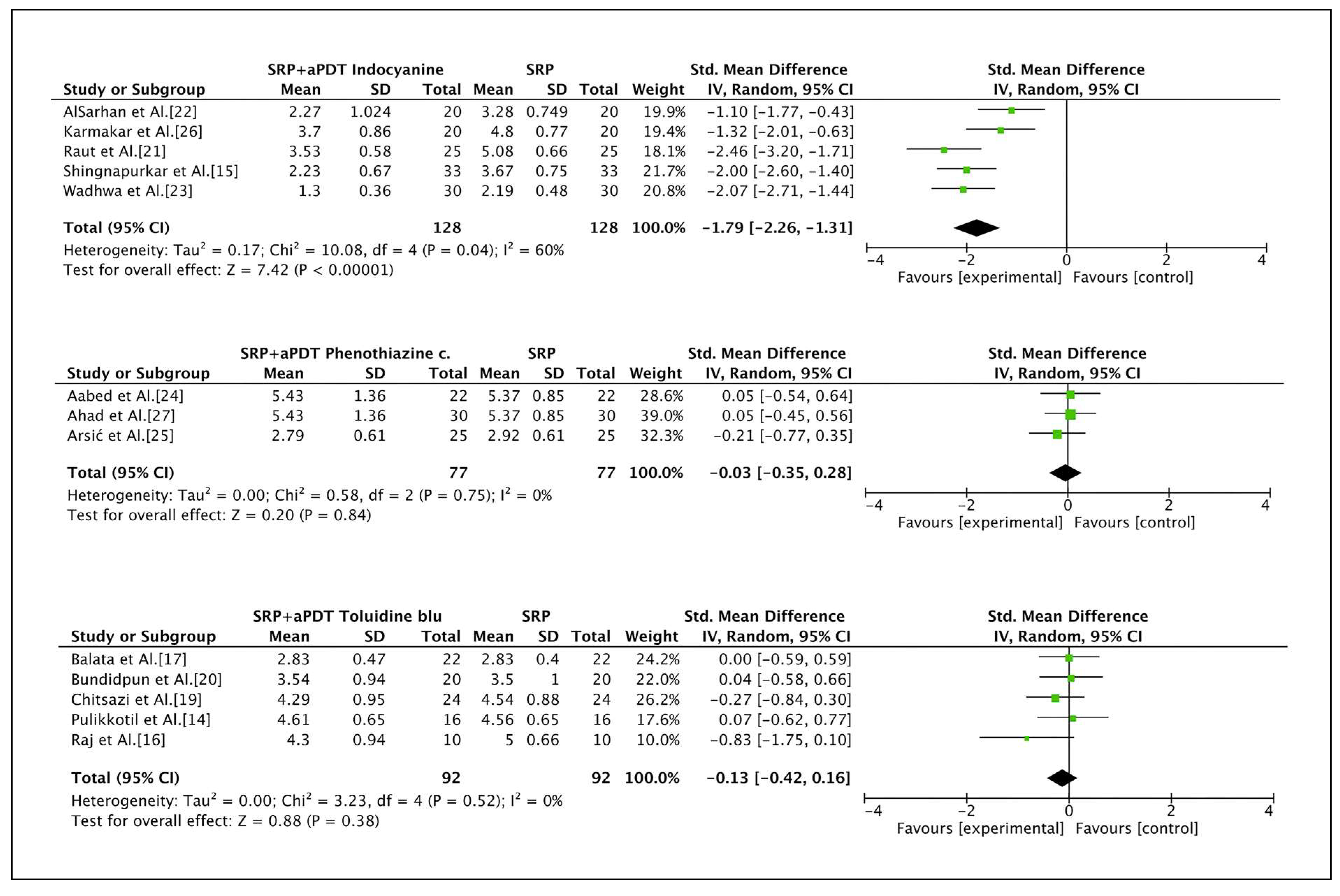
3.5. Meta-Analysis
4. Discussion
5. Conclusions
- -
- The first question that this systematic review aims to answer is whether there is sufficient evidence to justify the use of photodynamic therapy as an adjunct to conventional nonsurgical periodontal therapy using manual or mechanical instruments. A PDT emerged as a beneficial treatment option for periodontitis. The results of many studies indicated that aPDT combined with SRP has a slight advantage in the treatment of periodontitis. Despite a wide range of heterogeneity, all the included studies indicate that aPDT has the potential to be an effective adjuvant in the treatment of periodontitis. Scaling and root planing (SRP) remains essential for the promotion of a healthy subgingival environment.
- -
- The second question was whether photodynamic therapy (aPDT) provides additional effects to traditional treatment with manual and mechanical instruments when comparing the patient’s clinical parameters. The analysis of the studies suggests a short-term benefit of PDT in addition to SRP in terms of clinical outcome variables; however, the evidence regarding its long-term efficacy is still insufficient, and no significant effect was confirmed in terms of CAL gain at 3 months.
- -
- The third question concerned was whether in patients with untreated periodontitis the application of photodynamic therapy (aPDT) provides additional effects to the traditional treatment with manual and mechanical instruments when comparing the microbiological parameters of the patient. The bactericidal effect of aPDT as an adjunctive treatment to SRP against periodontopathogens in periodontal disorders remains questionable.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van der Weijden, G.A.; Timmerman, M.F. A systematic review on the clinical efficacy of subgingival debridement in the treat- ment of chronic periodontitis. J. Clin. Periodontol. 2002, 29, 55e71. [Google Scholar] [CrossRef] [PubMed]
- Heitz-Mayfield, L.J.; Trombelli, L.; Heitz, F.; Needleman, I.; Moles, D. A systematic review of the effect of surgical debridement vs non-surgical debridement for the treatment of chronic peri- odontitis. J. Clin. Periodontol. 2002, 29, 92e102. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.J.; Lozdan, J.; Boyde, A. Tooth surfaces treated in situ with periodontal instruments. Scanning electron microscopic studies. Dent. J. 1972, 132, 57. [Google Scholar] [CrossRef] [PubMed]
- Jones, W.; O’Leary, T.J. The effectiveness of in vivo root planing in removing bacterial endotoxin from the roots of periodontally involved teeth. J. Periodontol. 1978, 49, 337. [Google Scholar] [CrossRef]
- Waerhaug, J. Healing of the dento-epithelial junction following subgingival plaque control. II. As observed on extracted teeth. J. Periodontol. 1978, 49, 119. [Google Scholar] [CrossRef]
- Graziani, F.; Karapetsa, D.; Alonso, B.; Herrera, D. Nonsurgical and surgical treatment of periodontitis: How many options for one disease? Periodontol 2000 2017, 75, 152–188. [Google Scholar] [CrossRef]
- Sigusch, B.W.; Pfitzner, A.; Albrecht, V.; Glockmann, E. Efficacy of photodynamic therapy on inflammatory signs and two selected periodontopathogenic species in a beagle dog model. J. Periodontol. 2005, 76, 1100e5. [Google Scholar] [CrossRef]
- Nagarakanti, S.; Gunupati, S.; Chava, V.K.; Reddy, B.V. Effectiveness of Subgingival Irrigation as an Adjunct to Scaling and Root Planing in the Treatment of Chronic Periodontitis: A Systematic Review. J. Clin. Diagn. Res. 2015, 9, ZE06-9. [Google Scholar] [CrossRef]
- Mizutani, K.; Aoki, A.; Coluzzi, D.; Yukna, R.; Wang, C.Y.; Pavlic, V.; Izumi, Y. Lasers in minimally invasive periodontal and peri-implant therapy. Periodontology 2000 2016, 71, 185–212. [Google Scholar] [CrossRef]
- Schwarz, F.; Aoki, A.; Becker, J.; Sculean, A. Laser application in non-surgical periodontal therapy: A systematic review. J. Clin. Periodontol. 2008, 35 (Suppl. S8), 29–44. [Google Scholar] [CrossRef]
- Castano, A.P.; Demidova, T.N.; Hamblin, M.R. Mechanisms in photodynamic therapy: Part one—Photosensitizers, photochemistry, and cellular localization. Photodiagnosis Photodyn. Ther. 2004, 1, 279–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamblin, M.R.; Hasan, T. Photodynamic therapy: A new antimicrobial approach to infectious disease? Photochem. Photobiol. Sci. 2004, 3, 436–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulikkotil, S.J.; Toh, C.G.; Mohandas, K.; Leong, K. Effect of photodynamic therapy adjunct to scaling and root planing in periodontitis patients: A randomized clinical trial. Aust. Dent. J. 2016, 61, 440–445. [Google Scholar] [CrossRef] [Green Version]
- Shingnapurkar, S.H.; Mitra, D.K.; Kadav, M.S.; Shah, R.A.; Rodrigues, S.V.; Prithyani, S.S. The effect of indocyanine green-mediated photodynamic therapy as an adjunct to scaling and root planing in the treatment of chronic periodontitis: A comparative split-mouth randomized clinical trial. Indian J. Dent. Res. 2016, 27, 609–617. [Google Scholar] [CrossRef]
- Raj, K.R.; Musalaiah SV, V.S.; Nagasri, M.; Kumar, P.A.; Reddy, P.I.; Greeshma, M. Evaluation of efficacy of photodynamic therapy as an adjunct to nonsurgical periodontal therapy in treatment of chronic periodontitis patients: A clinico-microbiological study. Indian J. Dent. Res. 2016, 27, 483–487. [Google Scholar] [CrossRef]
- Balata, M.L.; Andrade, L.P.; Santos, D.B.; Cavalcanti, A.N.; Tunes Uda, R.; Ribeiro Édel, P.; Bittencourt, S. Photodynamic therapy associated with full-mouth ultrasonic debridement in the treatment of severe chronic periodontitis: A randomized-controlled clinical trial. J. Appl. Oral Sci. 2013, 21, 208–214. [Google Scholar] [CrossRef]
- Berakdar, M.; Callaway, A.; Fakhr Eddin, M.; Roß, A.; Willershausen, B. Comparison between scaling-root-planing (SRP) and SRP/photodynamic therapy: Six-month study. Head Face Med. 2012, 8, 12. [Google Scholar] [CrossRef] [Green Version]
- Chitsazi, M.T.; Shirmohammadi, A.; Pourabbas, R.; Abolfazli, N.; Farhoudi, I.; Azar, B.D.; Farhadi, F. Clinical and Microbiological Effects of Photodynamic Therapy Associated with Non-surgical Treatment in Aggressive Periodontitis. J. Dent. Res. Dent. Clin. Dent. Prospects 2014, 8, 153–159. [Google Scholar]
- Bundidpun, P.; Srisuwantha, R.; Laosrisin, N. Clinical effects of photodynamic therapy as an adjunct to full-mouth ultrasonic scaling and root planing in treatment of chronic periodontitis. Laser Ther. 2018, 27, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Raut, C.P.; Sethi, K.S.; Kohale, B.R.; Mamajiwala, A.; Warang, A. Indocyanine green-mediated photothermal therapy in treatment of chronic periodontitis: A clinico-microbiological study. J. Indian Soc. Periodontol. 2018, 22, 221–227. [Google Scholar] [CrossRef] [PubMed]
- AlSarhan, M.A.; Altammami, M.A.; Alaqeely, R.S.; AlEbdi, A.; Jasser, R.A.; Otaibi, D.A.; Oraini, S.A.; Habib, S.R.; Alqahtani, L.; Alduhaymi, I.S.; et al. Short-term improvement of clinical parameters and microbial diversity in periodontitis patients following Indocyanine green-based antimicrobial photodynamic therapy: A randomized single-blind split-mouth cohort. Photodiagnosis Photodyn. Ther. 2021, 35, 102349. [Google Scholar] [CrossRef] [PubMed]
- Wadhwa, A.; Mallapragada, S.; Sharma, P. Novel indocyanine green mediated antimicrobial photodynamic therapy in the management of chronic periodontitis-A randomized controlled clinico-microbiological pilot study. J. Oral Biol. Craniofac. Res. 2021, 11, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Aabed, K.; Moubayed, N.; BinShabaib, M.S.; ALHarthi, S.S. Is a single session of antimicrobial photodynamic therapy as an adjuvant to non-surgical scaling and root planing effective in reducing periodontal inflammation and subgingival presence of Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans in patients with periodontitis? Photodiagnosis Photodyn. Ther. 2022, 38, 102847. [Google Scholar]
- Arsić, Z.; Jovanović, R.; Djordjević, A.; Šehalić, M.; Marjanović, D.; Mikić, M.; Vlahović, Z.; Mladenović, R. Clinical and microbiological effects of photodynamic therapy applied in non-surgical treatment of periodontitis. Vojnosanit. Pregl. 2020, 79, 17–24. [Google Scholar] [CrossRef]
- Karmakar, S.; Prakash, S.; Jagadeson, M.; Namachivayam, A.; Das, D.; Sarkar, S. Clinico-microbiological Efficacy of Indocyanine Green as a Novel Photosensitizer for Photodynamic Therapy among Patients with Chronic Periodontitis: A Split-mouth Randomized Controlled Clinical Trial. J. Pharm. Bioallied Sci. 2021, 13 (Suppl. S1), S143–S148. [Google Scholar] [CrossRef]
- Ahad, A.; Lamba, A.K.; Faraz, F.; Tandon, S.; Chawla, K.; Yadav, N. Effect of Antimicrobial Photodynamic Therapy as an Adjunct to Nonsurgical Treatment of Deep Periodontal Pockets: A Clinical Study. J. Lasers Med. Sci. 2016, 7, 220–226. [Google Scholar] [CrossRef] [Green Version]
- Butera, A.; Maiorani, C.; Gallo, S.; Pascadopoli, M.; Venugopal, A.; Marya, A.; Scribante, A. Evaluation of Adjuvant Systems in Non-Surgical Peri-Implant Treatment: A Literature Review. Healthcare 2022, 10, 886. [Google Scholar] [CrossRef]
- Gallo, S.; Scribante, A. Ozone therapy in dentistry: From traditional applications towards innovativeones. A review of the literature. IOP Conf. Ser. Earth Environ. Sci. 2021, 707, 012001. [Google Scholar] [CrossRef]
- Colombo, M.; Gallo, S.; Garofoli, A.; Poggio, C.; Arciola, C.R.; Scribante, A. Ozone Gel in Chronic Periodontal Disease: A Randomized Clinical Trial on the Anti-Inflammatory Effects of Ozone Application. Biology 2021, 10, 625. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Luraghi, G.; Scribante, A. Ozonized Water Administrationin Peri- Implant Mucositis Sites: A Randomized Clinical Trial. Appl. Sci. 2021, 11, 7812. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2020, 9, 69. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Maiorani, C.; Preda, C.; Chiesa, A.; Esposito, F.; Pascadopoli, M.; Scribante, A. Management of Gingival Bleeding in Periodontal Patients with Domiciliary Use of Toothpastes Containing Hyaluronic Acid, Lactoferrin, or Paraprobiotics: A Randomized Controlled Clinical Trial. Appl. Sci. 2021, 11, 8586. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Maiorani, C.; Milone, A.; Alovisi, M.; Scribante, A. Paraprobiotics in Non- Surgical Periodontal Therapy: Clinical and Microbiological Aspects in a 6-Month Follow-Up Domiciliary Protocol for Oral Hygiene. Microorganisms 2022, 10, 337. [Google Scholar] [CrossRef]
- Butera, A.; Pascadopoli, M.; Gallo, S.; Alovisi, M.; Lovati, E.; Mutti, E.; Scribante, A. Domiciliary Management of Periodontal Indexes and Glycosylated Hemoglobin (HbA1c) in Type 1 Diabetic Patients with Paraprobiotic-Based Toothpaste and Mousse: Randomized Clinical Trial. Appl. Sci. 2022, 12, 8610. [Google Scholar] [CrossRef]
- Butera, A.; Gallo, S.; Pascadopoli, M.; Taccardi, D.; Scribante, A. Home Oral Care of Periodontal Patients Using Antimicrobial Gel with Postbiotics, Lactoferrin, and Aloe Barbadensis Leaf Juice Powder vs. Conventional Chlorhexidine Gel: A Split-Mouth Randomized Clinical Trial. Antibiotics 2022, 11, 118. [Google Scholar] [CrossRef]
- Butera, A.; Pascadopoli, M.; Pellegrini, M.; Gallo, S.; Zampetti, P.; Cuggia, G.; Scribante, A. Domiciliary Use of Chlorhexidine vs. Postbiotic Gels in Patients with Peri-Implant Mucositis: A Split-Mouth Randomized Clinical Trial. Appl. Sci. 2022, 12, 2800. [Google Scholar] [CrossRef]
- Scribante, A.; Gallo, S.; Pascadopoli, M.; Soleo, R.; Di Fonso, F.; Politi, L.; Venugopal, A.; Marya, A.; Butera, A. Management of Periodontal Disease with Adjunctive Therapy with Ozone and Photobiomodulation (PBM): A Randomized Clinical Trial. Photonics 2022, 9, 138. [Google Scholar] [CrossRef]
- Azaripour, A.; Dittrich, S.; Van Noorden, C.J.F.; Willershausen, B. Efficacy of photodynamic therapy as adjunct treatment of chronic periodontitis: A systematic review and meta-analysis. Lasers Med. Sci. 2018, 33, 407–423. [Google Scholar] [CrossRef]
- Akram, Z. How effective is adjunctive antimicrobial photodynamic therapy in treating deep periodontal pockets in periodontal disease? A systematic review. J. Investig. Clin. Dent. 2018, 9, e12345. [Google Scholar] [CrossRef]
- Atieh, M.A. Photodynamic therapy as an adjunctive treatment for chronic periodontitis: A meta-analysis. Lasers Med. Sci. 2010, 25, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Topaloglu, N.; Gulsoy, M.; Yuksel, S. Antimicrobial photodynamic therapy of resistant bacterial strains by indocyanine green and 809-nm diode laser. Photomed. Laser Surg. 2013, 31, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Sukumar, K.; Tadepalli, A.; Parthasarathy, H.; Ponnaiyan, D. Evaluation of combined efficacy of photodynamic therapy using indocyanine green photosensitizer and non-surgical periodontal therapy on clinical and microbial parameters in the management of chronic periodontitis subjects: A randomized split-mouth design. Photodiagnosis Photodyn. Ther. 2020, 31, 101949. [Google Scholar] [CrossRef] [PubMed]
- Marconcini, S.; Giammarinaro, E.; Cosola, S.; Oldoini, G.; Genovesi, A.; Covani, U. Effects of Non-Surgical Periodontal Treatment on Reactive Oxygen Metabolites and Glycemic Control in Diabetic Patients with Chronic Periodontitis. Antioxidants 2021, 10, 1056. [Google Scholar] [CrossRef] [PubMed]
- Aoyama, N.; Suzuki, J.I.; Kobayashi, N.; Hanatani, T.; Ashigaki, N.; Yoshida, A.; Shiheido, Y.; Sato, H.; Kumagai, H.; Ikeda, Y.; et al. Periodontitis deteriorates peripheral arterial disease in Japanese population via enhanced systemic inflammation. Heart Vessels. 2017, 32, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Carrizales-Sepúlveda, E.F.; Ordaz-Farías, A.; Vera-Pineda, R.; Flores-Ramírez, R. Periodontal Disease, Systemic Inflammation and the Risk of Cardiovascular Disease. Heart Lung Circ. 2018, 27, 1327–1334. [Google Scholar] [CrossRef]
- Lira-Junior, R.; Figueredo, C.M. Periodontal and inflammatory bowel diseases: Is there evidence of complex pathogenic interactions? World J. Gastroenterol. 2016, 22, 7963–7972. [Google Scholar] [CrossRef]
- Ricci, E.; Ciccarelli, S.; Agnese Mauri, P.; Gerli, S.; Favilli, A.; Cipriani, S.; Fedele, F.; Roncella, E.; Esposito, G.; Parazzini, F.; et al. Periodontitis, female fertility and conception (Review). Biomed. Rep. 2022, 17, 86. [Google Scholar] [CrossRef]
- Hyun, H.; Park, Y.W.; Kwon, Y.C.; Cho, B.K.; Lee, J.H. Relationship Between Chronic Periodontitis and Lower Urinary Tract Symptoms/Benign Prostatic Hyperplasia. Int. Neurourol. J. 2021, 25, 77–83. [Google Scholar] [CrossRef]
- Gomes-Filho, I.S.; Cruz, S.S.D.; Trindade, S.C.; Passos-Soares, J.S.; Carvalho-Filho, P.C.; Figueiredo, A.C.M.G.; Lyrio, A.O.; Hintz, A.M.; Pereira, M.G.; Scannapieco, F. Periodontitis and respiratory diseases: A systematic review with meta-analysis. Oral Dis. 2020, 26, 439–446. [Google Scholar] [CrossRef]
- Moghadam, S.A.; Shirzaiy, M.; Risbaf, S. The Associations between Periodontitis and Respiratory Disease. J. Nepal. Health Res. Counc. 2017, 15, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.C.; Fu, E.; Li, C.H.; Huang, R.Y.; Chiu, H.C.; Cheng, W.C.; Chen, W.L. Association between periodontitis and pulmonary function based on the Third National Health and Nutrition Examination Survey (NHANES III). J. Clin. Periodontol. 2020, 47, 788–795. [Google Scholar] [CrossRef] [PubMed]
- She, Y.Y.; Kong, X.B.; Ge, Y.P.; Liu, Z.Y.; Chen, J.Y.; Jiang, J.W.; Jiang, H.B.; Fang, S.L. Periodontitis and inflammatory bowel disease: A meta-analysis. BMC Oral Health 2020, 20, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, E.M.; Reis, C.; Manzanares-Céspedes, M.C. Chronic periodontitis, inflammatory cytokines, and interrelationship with other chronic diseases. Postgrad. Med. 2018, 130, 98–104. [Google Scholar] [CrossRef]
- Sczepanik, F.S.C.; Grossi, M.L.; Casati, M.; Goldberg, M.; Glogauer, M.; Fine, N.; Tenenbaum, H.C. Periodontitis is an inflammatory disease of oxidative stress: We should treat it that way. Periodontol 2000 2020, 84, 45–68. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Investigators | Study Design | Lasers and Fotosensitizing | Patients | Parameters Involved | Follow up (Weeks) |
|---|---|---|---|---|---|
| Pulikkotil SJ et al. [14] | RCT-split mouth | Methylene blue; wavelength 628 nm; Diode laser | 16 patients; CP; average age 39 ± 21 years | CAL; PPD; BOP A. actinomycetemcomitans | Up to 12 |
| Shingnapurkar et al. [15] | RCT-split mouth | Indocyaine green (IGC); wavelength 810 nm; Diode laser | 33 patients; chronic periodontitis; average age 40 ± 15 years | PPD; PI; GI; RAL | Up to 12 |
| Raj et al. [16] | RCT-Full mouth | Toluidine blue, wavelength of 635 nm; PAD [Lit 600], Apoza, Taiwan | 20 patients; chronic periodontitis; average age 42.5 ± 7.5 years | CAL; PPD P. gingivalis, T. forsythia, T. denticola | Up to 12 |
| Balata et al. [17] | RCT-split mouth | Methylene blue, wavelength 660 nm; AsGaAl diode laser | 22 patients; CP; average age 46.5 ± 15.5 years | CAL; PPD; BOP | Up to 24 |
| Berakdar et al. [18] | RCT-split mouth | Methylene blue, wavelength of 670 nm; Diode laser Periowave | 22 patients; CP; average age 56 ± 18 years | PPD: BOP | Up to 24 |
| Chitsazi et al. [19] | RCT-split mouth | Blu-toluidine; wavelength of 670–690 nm; Diode laser | 24 patients; AgP; average age 29 years | CAL; PPD BOP; GI; REC A. actinomycetecommitans | Up to 12 |
| Bundidpun et al. [20] | RCT-split mouth | Phenothiazine chloride (HELBO Blue); wavelength of 660 nm; Diode laser | 20 patients; CP; average age 52.5 ± 17.5 years | CAL; PPD; BOP; PI; GI | Up to 24 |
| Raut et al. [21] | RCT Full mouth | Indocyain green (IGC), wavelength of 810 nm; AsGaA Diode laser | 50 patients; CP; NA | CAL; PPD; BOP; PI | Up to 24 |
| AlSarhan et al. [22] | RCT-split mouth | Indocyanine green; wavelength of 808 nm +/− 10 nm. Diode laser Elexxion Claros peak; Elexxion AG | 20 patients; CP, average age 54 years | CAL; PPD; BOP; PI; REC | Up to 12 |
| Wadhwa et al. [23] | RCT Split Mouth | Indocyanine green; wavelength 810 nm. AsGaA Diode laser | 30 patients; CP; average age 46 ± 10 years | PPD; BOP; PI; GI; | Up to 24 |
| Aabed et al. [24] | RCT Full mouth | Methylene blue (MB) (0.005%), wavelength 660 nm and 150 mW, Diode laser | 44 patients; CP; NA | CAL; PPD; PI; GI A. actinomycetemcomitans, P. gingivalis | Up to 12 |
| Arsic Z et al. [25] | RCT Split Mouth | Phenothiazine chloride (HELBO Blue); wavelength of 660 nm; Diode laser, HELBO | 25 patients; CP; average age 50 ± 20 years | CAL; PPD; BOP; PI A. actinomycetemcomitans, P. gingivalis, T. denticola | Up to 12 |
| Karmakar et al. [26] | RCT Split Mouth | Indocyanine green (IGC); wavelength of 810 nm. Diode laser Picasso, AMD | 20 patients; CP; average age 45 ± 10 years | CAL; PPD P. gingivalis, T. forsythia | Up to 12 |
| Ahad et al. [27] | RCT Split Mouth | Phenothiazine chloride (HELBO Blue); wavelength of 660 nm; Helbo diode laser | 30 patients; CP; average age 38.67 ± 10.52 years | CAL; PPD; BOP; PI | Up to 12 |
| Investigators | Changes in PPD (mm) Comparing Test and Control Groups | |
|---|---|---|
| Pulikkotil SJ et al. [14] | aPDT + SRP (≥5 mm) T0: 4.66 ± 0.39 Follow-up:3.56 ± 0.69 * | SRP (≥5 mm) T0: 4.95 ± 0.95 Follow-up: 3.93 ± 0.23 * |
| Shingnapurkar SH et al. [15] | aPDT + SRP (≥5 mm) T0: 5.13 ± 0.34 Follow-up:2.23 ± 0.67 * | SRP (≥5 mm) T0: 5.27 ± 0.069 Follow-up: 3.67 ± 0.75 * |
| Raj KR et al. [16] | aPDT + SRP (≥5 mm) T0: 6 ± 1.1 Follow-up: 3.5 ± 0.8 | SRP (≥5 mm) T0: 5.9 ± 0.99 Follow-up: 3.5 ± 0.6 |
| Berakdar M et al. [18] | aPDT + SRP (≥5 mm) T0: 6.0 ± 1.1 Follow-up: 4.3 ± 0.94 * | SRP (≥5 mm) T0: 5.9 ± 0.99 Follow-up: 5 ± 0.66 * |
| Chitsazi MT et al. [19] | aPDT + SRP (≥4 mm) T0: 5.79 ± 1.06 Follow-up: 4.29 ± 0.95 | SRP (≥4 mm) T0: 5.45 ± 0.77 Follow-up: 4.54 ± 0.88 |
| Bundidpun P, et al. [20] | aPDT + SRP (≥6 mm) T0: 4.96 ± 1.11 Follow-up: 3.54 ± 0.94 | SRP (≥6 mm) T0: 4.91 ± 1.02 Follow-up: 3.5 ± 1 |
| Balata ML et al. [17] | aPDT + SRP (≥5 mm) T0: 5.11 ± 0.56 Follow-up: 2.83 ± 0.47 * | SRP (≥5 mm) T0: 5.15 ± 0.46 Follow-up: 2.83 ± 0.4 * |
| Raut CP et al. [21] | aPDT + SRP (≥5 mm) T0: 6.04 ± 0.82 Follow-up: 3.53 ± 0.58 * | SRP (≥5 mm) T0: 6.08 ± 0.73 Follow-up: 5.08 ± 0.66 * |
| AlSarhan MA et al. [22] | aPDT + SRP (≥5 mm) T0: 4.71 ± 0.863 Follow-up: 2.27 ± 1.024 * | SRP (≥5 mm) T0: 5.22 ± 0.924 Follow-up: 3.28 ± 0.749 * |
| Wadhwa A et al. [23] | aPDT + SRP (≥5 mm) T0: 3.37 ± 0.47 Follow-up:1.3 ± 0.36 * | SRP (≥5 mm) T0: 3.37 ± 0.46 Follow-up: 2.19 ± 0.48 * |
| Arsić, Z., et al. [25] | aPDT + SRP (≥5 mm) T0: 3.75 ± 0.7 Follow-up: 2.79 ± 0.61 * | SRP (≥5 mm) T0: 3.78 ± 0.75 Follow up: 2.92 ± 0.61 * |
| Karmakar S., et al. [26] | aPDT + SRP (≥5 mm) T0: 6.5 ± 0.61 Follow-up: 3.7 ± 0.86 | SRP (≥5 mm) T0: 6.4 ± 0.75 Follow-up: 4.8 ± 0.77 |
| Ahad, A., et al. [27] | aPDT + SRP (≥5 mm) T0: 7.9 ± 1.71 Follow-up: 5.43 ± 1.36 | SRP (≥5 mm) T0: 7.53 ± 1.31 Follow-up: 5.37 ± 0.85 |
| Aabed K et al. [24] | aPDT + SRP (≥5 mm) T0: 4.7 ± 0.2 Follow-up: 1.3 ± 0.2 | SRP (≥5 mm) T0: 4.5 ± 0.07 Follow-up: 1.5 ± 0.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pardo, A.; Butera, A.; Giordano, A.; Gallo, S.; Pascadopoli, M.; Scribante, A.; Albanese, M. Photodynamic Therapy in Non-Surgical Treatment of Periodontitis: A Systematic Review and Meta-Analysis. Appl. Sci. 2023, 13, 1086. https://doi.org/10.3390/app13021086
Pardo A, Butera A, Giordano A, Gallo S, Pascadopoli M, Scribante A, Albanese M. Photodynamic Therapy in Non-Surgical Treatment of Periodontitis: A Systematic Review and Meta-Analysis. Applied Sciences. 2023; 13(2):1086. https://doi.org/10.3390/app13021086
Chicago/Turabian StylePardo, Alessia, Andrea Butera, Angela Giordano, Simone Gallo, Maurizio Pascadopoli, Andrea Scribante, and Massimo Albanese. 2023. "Photodynamic Therapy in Non-Surgical Treatment of Periodontitis: A Systematic Review and Meta-Analysis" Applied Sciences 13, no. 2: 1086. https://doi.org/10.3390/app13021086