
Novel Methods of AI-Based Gait Analysis in Post-Stroke Patients

Abstract
:Featured Application
Abstract
1. Introduction
1.1. Clinical Gait Analysis
- the large amount of acquired data, which areoften redundant or even useless;
- the need to match tools to observed clinical problems, conditions, and deficits;
- the needs and expectations of clinicians regarding the way in which the results of clinical gait analysis are examined, presented, and interpreted (e.g., it should be fast, accurate, efficient, and based on an individual patient model);
1.2. Specificity of Post-Stroke Gait Analysis
- disorders occurring in both motor (including motor control) and sensory areas, often associated with other conditions and secondary lesions (including in long-term rehabilitation);
- disorders of both gait and balance functions;
- varying areas and degrees of damage and deficits which require a personalized approach to patient improvement;
- the return of lower limb function is an important goal for patients and their families as it significantly increases independence and motivation for further work;
- the risk of repeat strokes and an associated continuing need for prevention;
- the lengthy duration and multistage nature of post-stroke rehabilitation;
- the search for more effective methods of stroke rehabilitation than those currently in use is ongoing because it is not always possible to return a patient to full function, but only to the maximum performance level achievable for them, whereas improved methods of gait analysis may enable better comparative assessments and the selection of rehabilitation methods better suited to the particular condition [27].
- weakness of muscle strength;
- disturbances in the regulation of muscle tone;
- disorders of superficial sensation;
- disorders of deep sensation.
1.3. Former Approaches to Post-Stroke Gait Analysis
1.4. AI-Based Approaches to Gait Analysis
1.4.1. Previous Gait Studies Using Artificial Neural Networks
1.4.2. Previous Gait Studies Using Fractal Parameters
1.4.3. Previous Gait Studies Using Fuzzy Numbers
1.4.4. Previous Gait Studies Using Other Methods, Techniques, and Tools
- an investigation of the possibility of using an independent component analysis (ICA) together with a fractal dimension analysis in the study of the sEMG of small movements and the recognition of movement patterns (useful for the control of robots and other rehabilitation devices);
- an investigation of the spectrum of analysis possibilities using non-linear methods;
- a study of neuromuscular disorders using a wavelet analysis;
- a number of book studies published in the field of practical biomedical signal analysis which discuss clinical gait analysis.
1.4.5. Our Own Studies on AI-Based Post-Stroke Gait Analysis
1.5. Aim of the Study
2. Materials and Methods
2.1. Materials
- The Bobath method was used in the study group;
- The traditional rehabilitation approach was used in the reference group.
2.2. Methods
- AT − BP > 0: improvement
- AT − BP = 0: no change
- AT − BP < 0: deterioration
- AT − BP > 0: deterioration
- AT − BP = 0: no change
- AT − BP < 0: improvement
3. Results
4. Discussion
4.1. Comparison with Results of Current Research
4.2. Limitations of Current Studies
- static examination;
- measurement of joint mobility;
- gait analysis.
- there are no universal methods;
- simple and quick methods are not very accurate;
- accurate, reliable, and reproducible methods are time-consuming, costly, and require complex procedures;
- some methods require organizational changes for their successful implementation.
- the measurement of kinematic parameters (the analysis of human movements without analyzing the forces causing these movements), i.e., ranges of movement in the joints measured during gait as a trajectory of selected points on the body,
- the measurement of kinetic parameters, i.e.,the measurement of forces and moments of forces causing human movement, orthe measurement of muscle activity during gait using electromyography (EMG).
4.3. Directions for Further Research
- where data are difficult to acquire and must be obtainedfrom the patient during their normal activity (e.g., in children when they are uncooperative or unable to understand commands);
- where there are no data audit or the data are duplicated, incomplete, or subject to errors (including errors of unknown origin);
- where data do not permit the construction of a mathematical model and have to be analyzed by other means;
- where data must be obtained quickly, cheaply, and from a large sample.
- investigating the long-term effects of different treatment programs;
- investigating the impact of individual characteristics (e.g., obesity);
- investigating the impact of medical conditions (e.g., diabetes);
- investigating the impact of orthopedic supplies;
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | artificial intelligence |
| AT | after therapy |
| BT | before therapy |
| COTS | commercial off-the-shelf |
| ECG | electrocardiogram |
| EMG | electromyography |
| FD | fractal dimension |
| GDI | Gait Deviation Index |
| GRF | ground reaction force |
| HRQoL | health-related quality of life |
| ICA | independent component analysis |
| KFN | Kosińki’s fuzzy number |
| MLP | multilayer perceptron |
| OFN | ordered fuzzy number |
| PCA | principal component analysis |
| Q1 | lower quartile |
| Q3 | upper quartile |
| SD | standard deviation |
| sEMG | surface electromyography |
| SVM | support vector machine |
| VR | virtual reality |
References
- Lai, D.T.H.; Begg, R.K.; Palaniswami, M. Computational Intelligence in Gait Research: A Perspective on Current Applications and Future Challenges. IEEE Trans. Inf. Technol. Biomed. 2009, 13, 687–702. [Google Scholar] [CrossRef]
- Hodgins, D. The importance of measuring human gait. Med. Device Technol. 2008, 19, 44–47. [Google Scholar]
- Beauchet, O.; Berrut, G. Gait and dual-task: Definition, interest, and perspectives in the elderly. Psychol Neuropsychiatr Vieil. 2006, 4, 215–225. [Google Scholar] [PubMed]
- Mehrholz, J.; Thomas, S.; Werner, C.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2017, 5, CD006185. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Lees, J.; Simpkins, C.; Butler, A. Interventions for preventing falls in people post-stroke: A meta-analysis of randomized controlled trials. Gait Posture 2021, 84, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Bonini-Rocha, A.C.; De Andrade, A.L.S.; Moraes, A.M.; Matheus, L.B.G.; Diniz, L.R.; Martins, W. Effectiveness of Circuit-Based Exercises on Gait Speed, Balance, and Functional Mobility in People Affected by Stroke: A Meta-Analysis. PM&R 2017, 10, 398–409. [Google Scholar] [CrossRef]
- Veerbeek, J.M.; van Wegen, E.; van Peppen, R.; van der Wees, P.J.; Hendriks, E.; Rietberg, M.; Kwakkel, G. What is the evidence for physical therapy poststroke? A systematicreview and meta-analysis. PLoS ONE 2014, 9, e87987. [Google Scholar] [CrossRef]
- Balaban, B.; Tok, F. Gait Disturbances in Patients with Stroke. PM&R 2014, 6, 635–642. [Google Scholar] [CrossRef]
- Abi Hayla, M.; Ghoussayni, S.; Edvins, D.; Khalil, M. An automated method for analysis of gait data to aid clinical interpretation. In Proceedings of the 1st Middle East Conference on Biomedical Engineering (MECBME), Sharjah, United Arab Emirates, 21–24 February 2011; pp. 119–121. [Google Scholar]
- Mittlmeier, T.; Rosenbaum, D. Clinical gait analysis. Unfallchirurg 2005, 108, 614–629. [Google Scholar] [CrossRef] [PubMed]
- Chester, V.L.; Biden, E.N.; Tingley, M. Gait analysis. Biomed. Instrum. Technol. 2005, 39, 64–74. [Google Scholar]
- Simon, S.R. Quantification of human motion: Gait analysis—Benefits and limitations to its application to clinical problems. J. Biomech. 2004, 37, 1869–1880. [Google Scholar] [CrossRef] [PubMed]
- Sweeting, K.; Mock, M. Gait and posture—Assessment in general practice. Aust. Fam. Physician 2007, 36, 398–401, 404–405. [Google Scholar] [PubMed]
- Duhamel, A.; Bourriez, J.; Devos, P.; Krystkowiak, P.; Destée, A.; Derambure, P.; Defebvre, L. Statistical tools for clinical gait analysis. Gait Posture 2004, 20, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Vogt, L.; Brettmann, K.; Pfeifer, K.; Banzer, W. Gait disorders—Assessment and rehabilitation supported by movement analysis. Z Orthop Ihre Grenzgeb. 2002, 140, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Portscher, M.; Vogt, L.; Pfeifer, K.; Banzer, W. Reproducibility of lumbar spine kinematics in clinical gait analysis. Sport. Sportschaden 2000, 14, 50–54. [Google Scholar] [CrossRef]
- Banta, J.V. The evolution of gait analysis: A treatment decision-making tool. Connect. Med. 2001, 65, 323–331. [Google Scholar]
- Boudarham, J.; Roche, N.; Pradon, D.; Bonnyaud, C.; Bensmail, D.; Zory, R. Variations in kinematics in stroke patients. PLoS ONE 2013, 8, e66421. [Google Scholar] [CrossRef] [PubMed]
- Bonnefoy-Mazure, A.; Turcot, K.; Kaelin, A.; De Coulon, G.; Armand, S. Full body gait analysis may improve diagnostic discrimination between hereditary spastic paraplegia and spastic diplegia: A preliminary study. Res. Dev. Disabil. 2013, 34, 495–504. [Google Scholar] [CrossRef]
- Zverev, Y.; Adeloye, A.; Chisi, J. Quantitative analysis of gait pattern in hemiparetic patients. East Afr. Med. J. 2002, 79, 420–422. [Google Scholar] [CrossRef]
- Watelain, E.; Froger, J.; Barbier, F.; Lensel, G.; Rousseaux, M.; Lepoutre, F.-X.; Thevenon, A. Comparison of clinical gait analysis strategies by french neurologists, physiatrists and physiotherapists. J. Rehabil. Med. 2003, 35, 8–14. [Google Scholar] [CrossRef]
- Watelain, E.; Froger, J.; Rousseaux, M.; Lensel, G.; Barbier, F.; Lepoutre, F.-X.; Thevenon, A. Variability of video-based clinical gait analysis in hemiplegia as performed by practitioners in diverse specialties. J. Rehabil. Med. 2005, 37, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Thrift, A.G.; Thayabaranathan, T.; Howard, G.; Howard, V.J.; Rothwell, P.M.; Feigin, V.L.; Norrving, B.; Donnan, G.A.; Cadilhac, D.A. Global stroke statistics. Int. J. Stroke 2017, 12, 13–32. [Google Scholar] [CrossRef]
- Arnao, V.; Acciarresi, M.; Cittadini, E.; Caso, V. Stroke incidence, prevalence and mortality in women worldwide. Int. J. Stroke 2016, 11, 287–301. [Google Scholar] [CrossRef]
- Barker-Collo, S.; Bennett, D.A.; Krishnamurthi, R.V.; Parmar, P.; Feigin, V.L.; Naghavi, M.; Forouzanfar, M.H.; Johnson, C.O.; Nguyen, G.; Mensah, G.A.; et al. Sex Differences in StrokeIncidence, Prevalence, Mortality and Disability-Adjusted Life Years: Results from the Global Burden of Disease Study 2013. Neuroepidemiology 2015, 45, 203–214. [Google Scholar] [CrossRef]
- Sajjad, A.; Chowdhury, R.; Felix, J.F.; Ikram, M.A.; Mendis, S.; Tiemeier, H.; Mant, J.; Franco, O.H. A systematic evaluation of stroke surveillance studies in low- and middle-income countries. Neurology 2013, 80, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Yavuzer, M.G. Walking after Stroke: Interventions to Restore Normal Gait Pattern; Pelikan Publications: Ankara, Turkey, 2006. [Google Scholar]
- Mulroy, S.; Gronley, J.; Weiss, W.; Newsam, C.; Perry, J. Use of cluster analysis for gait pattern classification of patients in the early and late recovery phases following stroke. Gait Posture 2003, 18, 114–125. [Google Scholar] [CrossRef]
- Mohan, D.M.; Khandoker, A.H.; Wasti, S.A.; Alali, S.I.I.I.; Jelinek, H.F.; Khalaf, K. Assessment Methods of Post-stroke Gait: A Scoping Review of Technology-Driven Approaches to Gait Characterization and Analysis. Front. Neurol. 2021, 12, 650024. [Google Scholar] [CrossRef] [PubMed]
- Wikström, J.; Georgoulas, G.; Moutsopoulos, T.; Seferiadis, A. Intelligent data analysis of instrumented gait data in stroke patients—A systematic review. Comput. Biol. Med. 2014, 51, 61–72. [Google Scholar] [CrossRef]
- Derlatka, M.; Kotowski, A. Autocorrelation function for human gait analysis. J. Vibroengineering 2009, 11, 712–716. [Google Scholar]
- Derlatka, M.; Pauk, J. Data Mining in Analysis of Biomechanical Signals. Solid State Phenom. 2009, 147–149, 588–593. [Google Scholar] [CrossRef]
- Derlatka, M.; Pauk, J.; Długosz, R.; Kolasa, M. Human gait analysis and clasification based on neural networks and fuzzy logic. Solid State Phenom. 2009, 147–149, 600–605. [Google Scholar]
- Gioftsos, G.; Grieve, D. The use of neural networks to recognize patterns of human movement: Gait patterns. Clin. Biomech. 1995, 10, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Lapham, A.; Bartlett, R. The use of artificial intelligence in the analysis of sports performance: A review of applications in human gait analysis and future directions for sports biomechanics. J. Sports Sci. 1995, 13, 229–237. [Google Scholar] [CrossRef]
- Kaijima, M.; Foutz, T.L.; McClendon, R.W.; Budsberg, S.C. Diagnosis of lameness in dogs by use of artificial neural networks and ground reaction forces obtained during gait analysis. Am. J. VeterRes. 2012, 73, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Begg, R.; Kamruzzaman, J. Neural networks for detection and classification of walking pattern changes due to ageing. Australas Phys. Eng. Sci. Med. 2006, 29, 188–195. [Google Scholar] [CrossRef]
- Azulay, J.P.; Vacherot, F.; Vaugoyeau, M. Gait disorders: Mechanisms and classification. Rev. Neurol. 2010, 166, 142–148. [Google Scholar] [CrossRef]
- Luu, T.P.; Low, K.; Qu, X.; Lim, H.; Hoon, K. An individual-specific gait pattern prediction model based on generalized regression neural networks. Gait Posture 2014, 39, 443–448. [Google Scholar] [CrossRef]
- Oh, S.E.; Choi, A.; Mun, J.H. Prediction of ground reaction forces during gait based on kinematics and a neural network model. J. Biomech. 2013, 46, 2372–2380. [Google Scholar] [CrossRef]
- Ripoli, A.; Belardinelli, A.; Palagi, G.; Franchi, D.; Bedini, R. An effective algorithm for quick fractal analysis of movement biosignals. J. Med. Eng. Technol. 1999, 23, 216–221. [Google Scholar] [CrossRef]
- Sekine, M.; Tamura, T.; Akay, M.; Fujimoto, T.; Togawa, T.; Fukui, Y. Discrimination of walking patterns using wavelet-based fractal analysis. IEEE Trans. Neural Syst. Rehabil. Eng. 2002, 10, 188–196. [Google Scholar] [CrossRef]
- Wang, J.-S.; Lin, C.-W.; Yang, Y.-T.C.; Ho, Y.-J. Walking Pattern Classification and Walking Distance Estimation Algorithms Using Gait Phase Information. IEEE Trans. Biomed. Eng. 2012, 59, 2884–2892. [Google Scholar] [CrossRef]
- Phinyomark, A.; Larracy, R.; Scheme, E. Fractal Analysis of Human Gait Variability via Stride Interval Time Series. Front. Physiol. 2020, 11, 333. [Google Scholar] [CrossRef] [PubMed]
- Si, W.; Yang, G.; Chen, X.; Jia, J. Gait identification using fractal analysis and support vector machine. Soft Comput. 2019, 23, 9287–9297. [Google Scholar] [CrossRef]
- Arjunan, S.P.; Kumar, D.K. Fractal Based Modelling and Analysis of Electromyography (EMG) To Identify Subtle Actions. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2007, 2007, 1961–1964. [Google Scholar] [CrossRef]
- Sagawa, Y., Jr.; Watelain, E.; De Coulon, G.; Kaelin, A.; Gorce, P.; Armand, S. Are clinical measurements linked to the gait deviation index in cerebral palsy patients? Gait Posture 2013, 38, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Senanayake, C.M.; Senanayake, S.M.N.A. Computational Intelligent Gait-Phase Detection System to Identify Pathological Gait. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 1173–1179. [Google Scholar] [CrossRef]
- Armand, S.; Sangeux, M.; Baker, R. Optimal markers’ placement on the thorax for clinical gait analysis. Gait Posture 2014, 39, 147–153. [Google Scholar] [CrossRef]
- Keegan, K.G.; Arafat, S.; Skubic, M.; Wilson, D.A.; Krämer, J.; Messer, N.M.; Johnson, P.J.; O’Brien, D.P.; Johnson, G. Detection of spinal ataxia in horses using fuzzy clustering of body position uncertainty. Equine Veter. J. 2010, 36, 712–717. [Google Scholar] [CrossRef]
- Muniz, A.; Nadal, J. Application of principal component analysis in vertical ground reaction force to discriminate normal and abnormal gait. Gait Posture 2009, 29, 31–35. [Google Scholar] [CrossRef]
- Lozano-Ortiz, C.A.; Muniz, A.M.S.; Nadal, J. Human gait classification after lower limb fracture using Artificial Neural Networks and principal component analysis. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September2010; pp. 1413–1416. [Google Scholar] [CrossRef]
- Mikołajewska, E.; Prokopowicz, P.; Mikolajewski, D. Computational gait analysis using fuzzy logic for everyday clinical purposes—Preliminary findings. Bio-Algorithms Med-Systeams 2017, 13, 37–42. [Google Scholar] [CrossRef]
- Prokopowicz, P.; Mikołajewski, D.; Tyburek, K.; Mikołajewska, E. Computational gait analysis for post-stroke rehabilitation purposes using fuzzy numbers, fractal dimension and neural networks. Bull. Pol. Acad. Sci. 2020, 68, 191–198. [Google Scholar]
- Prokopowicz, P.; Mikołajewska, E.; Mikołajewski, D.; Kotlarz, P. Traditional vs. OFN-based Analysis of Temporo-spatial Gait. In Ordered Fuzzy Numbers: Theory and Applications; Parameters, W., Prokopowicz, P., Czerniak, J., Mikołajewski, D., Apiecionek, Ł., Ślęzak, D., Eds.; A tribute to Professor Witold Kosiński; Spinger: New York, NY, USA; Berlin/Heidelberg, Germany, 2017; pp. 287–297. [Google Scholar]
- Cicirelli, G.; Impedovo, D.; Dentamaro, V.; Marani, R.; Pirlo, G.; D’Orazio, T.R. Human Gait Analysis in Neurodegenerative Diseases: A Review. IEEE J. Biomed. Health Inform. 2021, 26, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Xu, T.; Qi, S.; Cao, X.; Yeung, E.H.K.; Hu, Y. Non-age-related gait kinematics and kinetics in the elderly. BMC Musculoskelet. Disord. 2022, 23, 623. [Google Scholar] [CrossRef]
- Das, R.; Paul, S.; Mourya, G.K.; Kumar, N.; Hussain, M. Recent Trends and Practices Toward Assessment and Rehabilitation of Neurodegenerative Disorders: Insights From Human Gait. Front. Neurosci. 2022, 16, 859298. [Google Scholar] [CrossRef]
- Mikołajewska, E. Associations between results of post-stroke NDT-Bobath rehabilitation in gait parameters, ADL and hand functions. Adv. Clin. Exp. Med. 2013, 22, 731–738. [Google Scholar] [PubMed]
- Prokopowicz, P.; Mikołajewski, D.; Mikołajewska, E.; Kotlarz, P. Fuzzy system as an assessment tool for analysis of the health-related quality of life for the people after stroke. In Proceedings of the Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics). In Proceedings of the 16th International Conference, ICAISC, Zakopane, Poland, 11–15 June 2017; 10245 LNAI; pp. 710–721. [Google Scholar] [CrossRef]
- Eltoukhy, M.; Oh, J.; Kuenze, C.; Signorile, J. Improved kinect-based spatiotemporal and kinematic treadmill gait assessment. Gait Posture 2017, 51, 77–83. [Google Scholar] [CrossRef]
- Auvinet, E.; Multon, F.; Manning, V.; Meunier, J.; Cobb, J. Validity and sensitivity of the longitudinal asymmetry index to detect gait asymmetry using Microsoft Kinect data. Gait Posture 2017, 51, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Ferber, R.; Osis, S.T.; Hicks, J.L.; Delp, S.L. Gait biomechanics in the era of data science. J. Biomech. 2016, 49, 3759–3761. [Google Scholar] [CrossRef]
- Fong, D.T.-P.; Chan, Y.-Y. The Use of Wearable Inertial Motion Sensors in Human Lower Limb Biomechanics Studies: A Systematic Review. Sensors 2010, 10, 11556–11565. [Google Scholar] [CrossRef]
- Shu, L.; Hua, T.; Wang, Y.; Li, Q.; Feng, D.D.; Tao, X. In-Shoe Plantar Pressure Measurement and Analysis System Based on Fabric Pressure Sensing Array. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 767–775. [Google Scholar] [CrossRef]
- Luvizutto, G.J.; Silva, G.F.; Nascimento, M.R.; Santos, K.C.S.; Appelt, P.A.; Neto, E.D.M.; de Souza, J.T.; Wincker, F.C.; Miranda, L.A.; Filho, P.T.H.; et al. Use of artificial intelligence as an instrument of evaluation after stroke: A scoping review based on international classification of functioning, disability and health concept. Top. Stroke Rehabil. 2021, 29, 331–346. [Google Scholar] [CrossRef]
- Iosa, M.; Capodaglio, E.; Pelà, S.; Persechino, B.; Morone, G.; Antonucci, G.; Paolucci, S.; Panigazzi, M. Artificial Neural Network Analyzing Wearable Device Gait Data for Identifying Patients With Stroke Unable to Return to Work. Front. Neurol. 2021, 12, 650542. [Google Scholar] [CrossRef]
- Iosa, M.; Benedetti, M.G.; Antonucci, G.; Paolucci, S.; Morone, G. Artificial Neural Network Detects Hip Muscle Forces as Determinant for Harmonic Walking in People after Stroke. Sensors 2022, 22, 1374. [Google Scholar] [CrossRef]
- Romijnders, R.; Warmerdam, E.; Hansen, C.; Schmidt, G.; Maetzler, W. A Deep Learning Approach for Gait Event Detection from a Single Shank-Worn IMU: Validation in Healthy and Neurological Cohorts. Sensors 2022, 22, 3859. [Google Scholar] [CrossRef] [PubMed]
- Ghaderzadeh, M. Clinical Decision SupportSystem for Early Detection of Prostate Cancer from Benign Hyperplasia of Prostate. Stud. Health Technol. Inform. 2013, 192, 928. [Google Scholar] [CrossRef] [PubMed]
- Gheisari, M.; Ebrahimzadeh, F.; Rahimi, M.; Moazzamigodarzi, M.; Liu, Y.; Pramanik, P.K.D.; Heravi, M.A.; Mehbodniya, A.; Ghaderzadeh, M.; Feylizadeh, M.R.; et al. Deep learning: Applications, architectures, models, tools, and frameworks: A comprehensive survey. CAAI Trans. Intell. Technol. 2023, 1–26. [Google Scholar] [CrossRef]
- Ghaderzadeh, M.; Asadi, F.; Hosseini, A.; Bashash, D.; Abolghasemi, H.; Roshanpour, A. Machine Learning in Detection and Classification of Leukemia Using Smear Blood Images: A Systematic Review. Sci. Program. 2021, 2021, 9933481. [Google Scholar] [CrossRef]
- Garavand, A.; Salehnasab, C.; Behmanesh, A.; Aslani, N.; Zadeh, A.H.; Ghaderzadeh, M. Efficient Model for Coronary Artery Disease Diagnosis: A Comparative Study of Several Machine Learning Algorithms. J. Health Eng. 2022, 2022, 5359540. [Google Scholar] [CrossRef] [PubMed]
- Sadoughi, F.; Ghaderzadeh, M. A Hybrid Particle Swarm and Neural Network Approach for Detection of Prostate Cancer from Benign Hyperplasia of Prostate. Stud. Health Technol. Inform. 2014, 205, 481–485. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Study Group n = 46 (100%) | Reference Group n = 46 (100%) |
|---|---|---|
| Age (years): | ||
| mean | 64.70 | 66.67 |
| SD (standard deviation) | 9.99 | 10.75 |
| min | 41 | 43 |
| Q1 (lower quartile) | 58 | 57 |
| median | 66 | 68 |
| Q3 (upper quartile) | 72 | 74 |
| max | 81 | 83 |
| Gender: | ||
| female (F) | 23 (50.00%) | 22 (47.82%) |
| male (M) | 23 (50.00%) | 24 (52.18%) |
| Side affected: | ||
| left (L) | 21(45.65%) | 23 (50%) |
| right (P) | 25(54.34%) | 23 (50%) |
| Time after cerebrovascular accident (weeks): | ||
| mean | 63.22 | 64.17 |
| SD (standard deviation) | 15.87 | 15.21 |
| min | 6 | 6 |
| Q1 (lower quartile) | 24 | 19 |
| median | 61 | 62 |
| Q3 (upper quartile) | 103 | 107 |
| max | 151 | 155 |
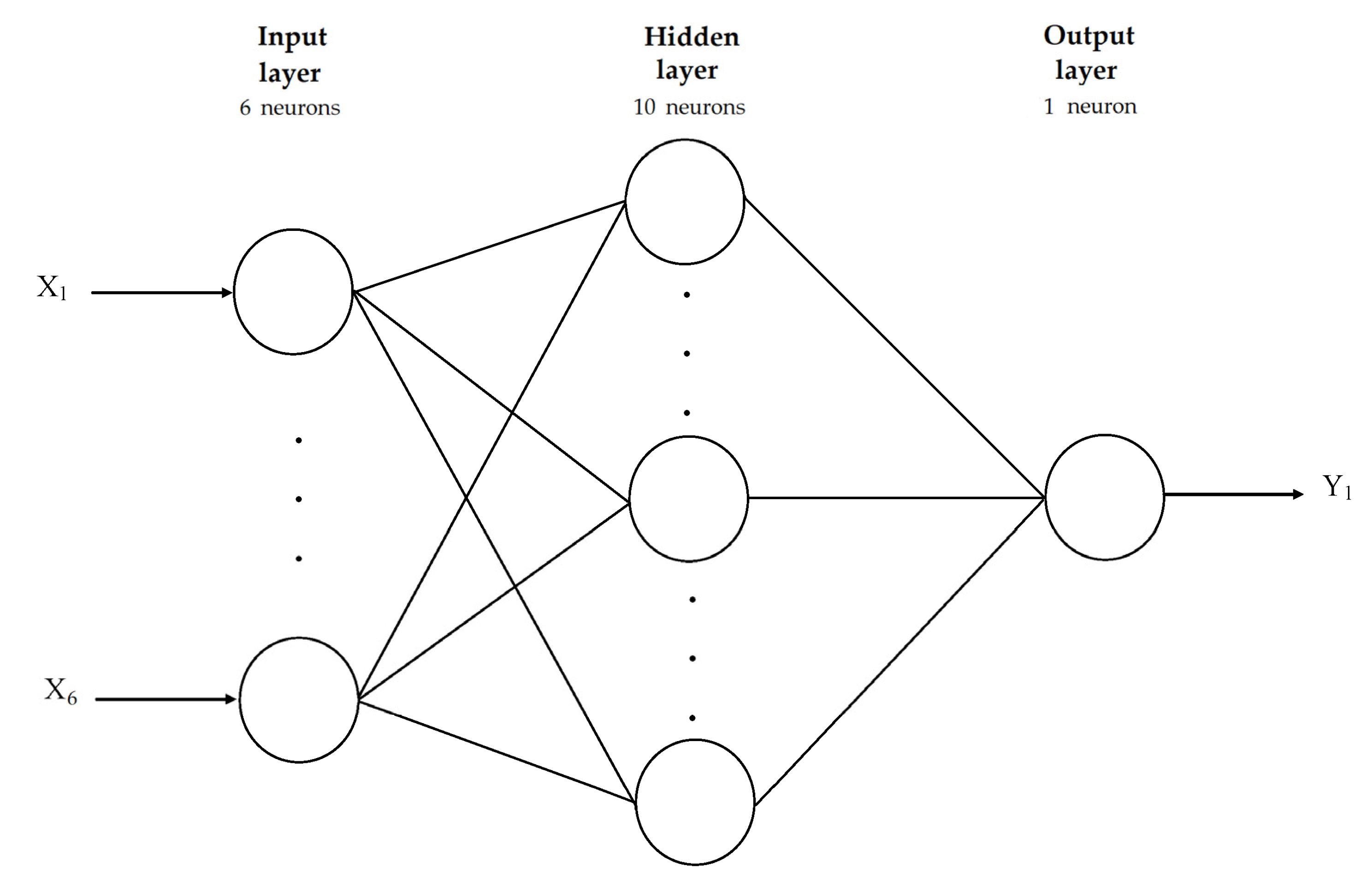
| Network Structure | Accuracy (Learning) (%) | Quality (Testing) (%) |
|---|---|---|
| MLP 6-8-1 | 89.02 | 89.68 |
| MLP 6-9-1 | 91.41 | 92.31 |
| MLP 6-10-1 | 92.81 | 93.13 |
| MLP 6-12-1 | 91.16 | 92.37 |
| MLP 6-14-1 | 88.46 | 88.74 |
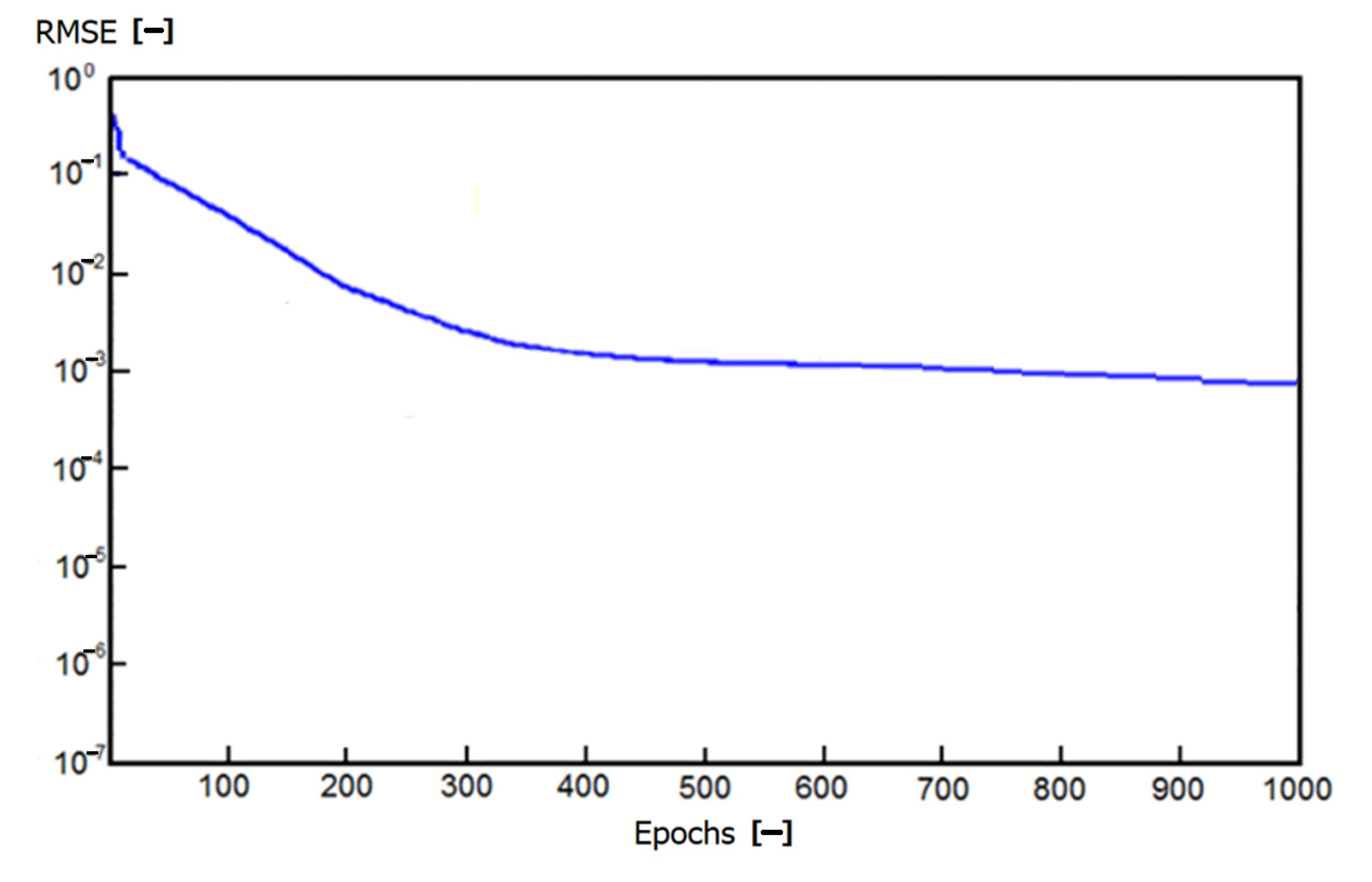
| Network Structure | RMSE (Learning) Value (–) |
|---|---|
| MLP 6-8-1 | 0.02 |
| MLP 6-9-1 | 0.01 |
| MLP 6-10-1 | 0.001 |
| MLP 6-12-1 | 0.01 |
| MLP 6-14-1 | 0.02 |
| Change in study group | Mean | 0.08 |
| SD | 0.02 | |
| Min | 0.02 | |
| Q1 | 0.04 | |
| Median | 0.07 | |
| Q3 | 0.08 | |
| Max | 0.09 | |
| Changein reference group | Mean | 0.07 |
| SD | 0.02 | |
| Min | 0.03 | |
| Q1 | 0.08 | |
| Median | 0.07 | |
| Q3 | 0.08 | |
| Max | 0.09 | |
| Distribution | Not normal | |
| p | 0.042 | |
| Change in study group | Mean | 0.07 |
| SD | 0.01 | |
| Min | 0.01 | |
| Q1 | 0.05 | |
| Median | 0.07 | |
| Q3 | 0.13 | |
| Max | 0.29 | |
| Change in reference group | Mean | 0.05 |
| SD | 0.01 | |
| Min | 0.01 | |
| Q1 | 0.03 | |
| Median | 0.05 | |
| Q3 | 0.09 | |
| Max | 0.40 | |
| Distribution | Not normal | |
| p | 0.021 | |
| Velocity | Cadence | Stride Length | Normalized Velocity | Normalized Cadence | Normalized Stride Length | Fractal Dimension | Fuzzy Parameter | |
|---|---|---|---|---|---|---|---|---|
| Velocity | − | 0.656 p = 0.001 | 0.672 p = 0.003 | 0.942 p = 0.012 | 0.746 p = 0.014 | 0.659 p = 0.015 | −0.476 0.012 | 0.423 0.015 |
| Cadence | − | 0.634 p = 0.005 | 0.816 p = 0.007 | 0.945 p = 0.041 | n.s. | −0.561 p = 0.001 | 0.645 p = 0.012 | |
| Stride length | − | 0.689 p = 0.006 | 0.366 p = 0.022 | 0.412 p = 0.011 | −0.614 p = 0.003 | 0.613 p = 0.011 | ||
| Normalized velocity | − | 0.734 p = 0.004 | 0.618 p = 0.017 | −0.338 p = 0.002 | 0.367 p = 0.008 | |||
| Normalized cadence | − | 0.523 p = 0.034 | −0.452 p = 0.001 | 0.399 p = 0.005 | ||||
| Normalized stride length | − | −0.491 p = 0.007 | 0.423 p = 0.001 | |||||
| Fractal dimension | − | −0.478 p = 0.004 | ||||||
| Fuzzy parameter | − |
| Velocity | Cadence | Stride Length | Normalized Velocity | Normalized Cadence | Normalized Stride Length | Fractal Dimension | Fuzzy Parameter | |
|---|---|---|---|---|---|---|---|---|
| Velocity | − | 0.597 p = 0.001 | 0.629 p = 0.000 | 0.912 p = 0.002 | 0.624 p = 0.003 | 0.489 p = 0.007 | −0.467 0.005 | 0.412 0.021 |
| Cadence | − | 0.520 p = 0.003 | 0.518 p = 0.004 | 0.756 p = 0.000 | n.s. | −0.576 p = 0.002 | 0.642 p = 0.004 | |
| Stride length | − | 0.523 p = 0.003 | 0.491 p = 0.011 | 0.771 p = 0.001 | −0.629 p = 0.032 | 0.657 p = 0.022 | ||
| Normalized velocity | − | 0.634 p = 0.001 | 0.351 p = 0.013 | −0.387 p = 0.004 | 0.387 p = 0.016 | |||
| Normalized cadence | − | n.s. | −0.487 p = 0.012 | 0.432 p = 0.005 | ||||
| Normalized stride length | − | −0.423 p = 0.006 | 0.412 p = 0.005 | |||||
| Fractal dimension | − | −0.489 p = 0.001 | ||||||
| Fuzzy parameter | − |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojek, I.; Prokopowicz, P.; Dorożyński, J.; Mikołajewski, D. Novel Methods of AI-Based Gait Analysis in Post-Stroke Patients. Appl. Sci. 2023, 13, 6258. https://doi.org/10.3390/app13106258
Rojek I, Prokopowicz P, Dorożyński J, Mikołajewski D. Novel Methods of AI-Based Gait Analysis in Post-Stroke Patients. Applied Sciences. 2023; 13(10):6258. https://doi.org/10.3390/app13106258
Chicago/Turabian StyleRojek, Izabela, Piotr Prokopowicz, Janusz Dorożyński, and Dariusz Mikołajewski. 2023. "Novel Methods of AI-Based Gait Analysis in Post-Stroke Patients" Applied Sciences 13, no. 10: 6258. https://doi.org/10.3390/app13106258