1. Introduction
Polymethyl methacrylate (PMMA) is the most common material for making removable dentures bases [
1]. This material has good mechanical, physical and aesthetic properties, as well as its simplicity to be repaired and hardened [
2]. However, PMMA did not provide all the requirements for ideal removable dentures bases [
1,
2]. The increase in the occlusal vertical dimension of the complete acrylic denture during the laboratory stages is an important clinical consideration and is attributed to the properties of the materials and techniques used [
3]. PMMA is subjected to deformation during the curing process, which is one of its major obstacles [
4]. Moreover, this material is also subjected to expansion when heated and contraction during hardening and cooling [
5], which results in the release of internal stress during removal from the crucible, which leads to undesirable changes in dimensions [
6,
7]. Therefore, the vertical occlusal dimension must be adjusted when delivering the dentures, and this procedure requires a long time to accomplish, resulting in a loss of the anatomical shape of the artificial teeth [
8,
9].
Polymethyl methacrylate treatment and polymerization methods were developed over the years to improve its physical and mechanical properties. Several methods have been used, such as heat, light, chemicals, microwave energy and curing by pressure and heat device (autoclave) [
10]. The water bath technique was used as a traditional method for curing thermosetting acryl due to its simplicity and low cost. However, this technique suffered from a major drawback which is the long time required for the curing process [
11]. A pressurized steam device was used to harden acrylic bases for removable dentures for the first time by Muley in 1976 [
12]. This method of curing with a pressure device (autoclave) depends on raising the pressure and water temperature above 100 °C in a vacuum chamber. This method showed better results with its fast and slow cycles in terms of mechanical properties [
13].
The physical and mechanical properties of the acryl used in the fabrication of dentures were studied by Ming et al. [
14]. They showed no difference in hardness between the prepared materials using the traditional method compared to an automatic pressure cooker. In contrast, they reported longer time for the traditional method than that of the automatic pressure cooker. Several studies have also been conducted on the autoclave curing technique, and Durkan et al. [
15] reported that curing by using an autoclave ameliorates the mechanical properties of the curing acryl denture bases compared to the water bath curing technique. Abdulwahhab et al. [
16] mentioned that the use of an autoclave could change the porosity of thermosetting acryl. Khalaf [
17] did not find a difference between slow (121 °C, 2.1 KPa for 30 min) and rapid (121 °C, 2.1 KPa for 15 min) autoclave curing methods on surface hardness, water absorption, mechanical resistance, and solubility. Considering the rapid and continuous developments in the field of prosthetic devices, new materials and techniques were introduced in the dental market. These techniques were used by relying on modern polymerizing methods such as injection, microwave, and autoclave, replacing the traditional method of polymerizing with a water bath in order to save time and effort as well as to preserve the anatomical shape of the artificial teeth. In addition, the change in the vertical occlusion dimension of a complete acrylic denture cured with an autoclave was rarely studied in the literature.
Therefore, the aim of the present in vitro study was to evaluate the vertical occlusal dimension changes of complete acrylic dentures following four different polymerization methods. The null hypothesis was that there is no difference between the tested methods on the vertical occlusal dimension changes of complete acrylic dentures.
2. Materials and Methods
2.1. Samples
Forty complete upper and lower identical acrylic dentures were used in the present in vitro study. The samples were divided into four equal groups (n = 10) according to the method of curing.
2.2. Cast Wax Preparation
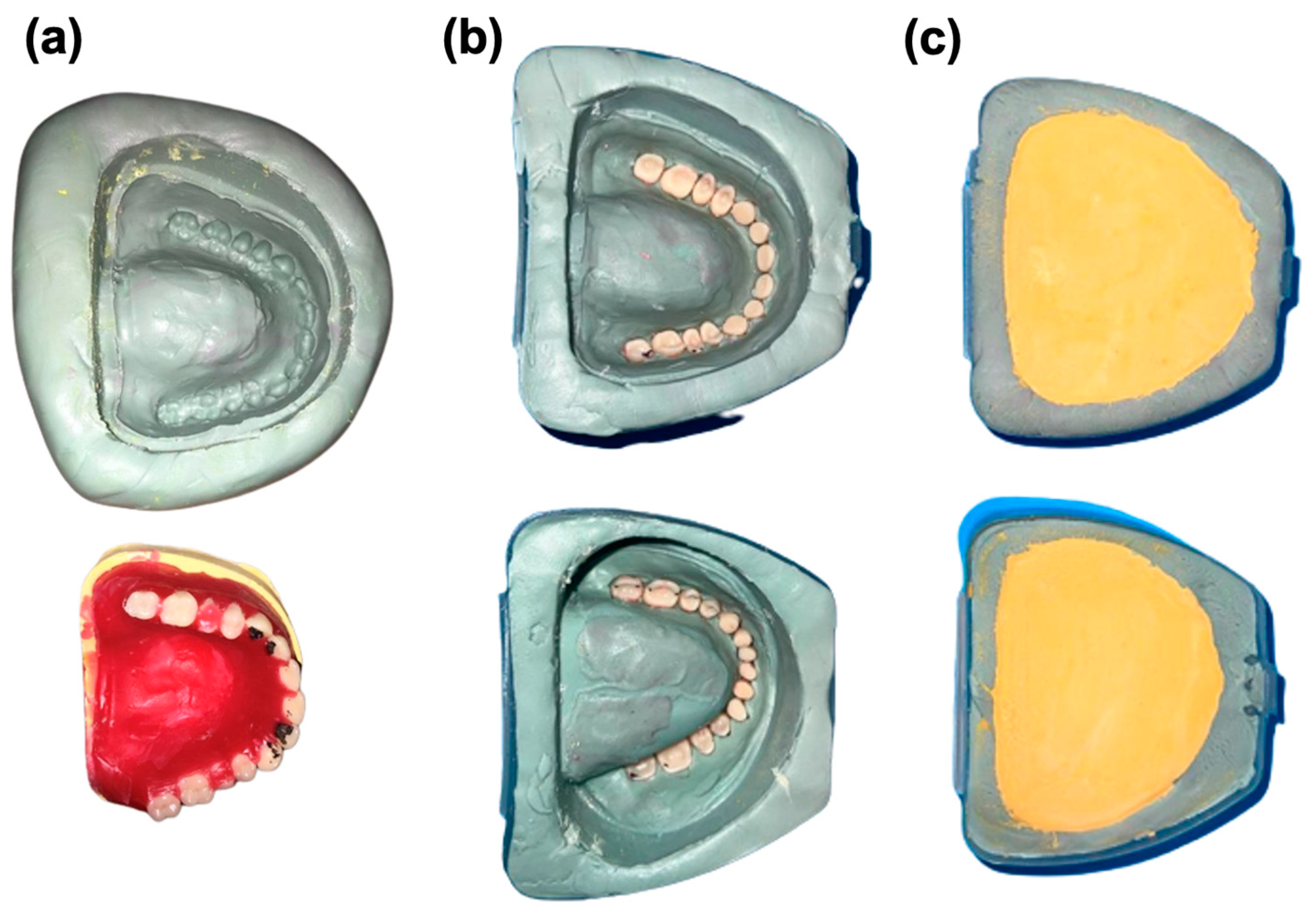
Forty similar upper and lower edentulous casts were prepared using Type III stone gypsum (Durguix hard natural stone, Prothecno, Gerona, Spain). Three grooves were engraved on all casts in order to be reinstalled on the articulator and numbered from 1 to 40. Base plates and wax elevations were made on all upper and lower casts. Wax elevations were made using wax (Modeling wax, metro wax, metrodent, Huddersfield HD3 4EP, UK) with 10 mm of height and 7 mm of width for the anterior upper and lower regions and 10 mm of height and 7 mm of width for the posterior upper region. The lower posterior region is contiguous with the retromolar pad; thus, the tops of the upper and lower wax elevations were touched surface to surface. The master upper and lower casts were placed on a semi-adjustable articulator (Dentatus ARL Articulator, ABdentatus, Hagersten, Sweden). The BENT angle was 15°, and the condyloid guide angle was set at 30° before configuring the artificial teeth. Artificial teeth (Mejor dent classic, Major dental, Moncalieri, Italy) were used. Anterior teeth from 1 to 3 and then from 4 to 7 were arranged according to the principle of balanced occlusion (Class 1). All exterior surfaces of the master upper and lower dentures were waxed and appropriately finished. The lower cast was dismantled, and the upper cast was left in place. The reinstallation guide was made on the lower arm of the articulator using plaster, where only the tips of the artificial teeth cusps were immersed in plaster. In addition, to have similar models, the waxed casts were copied using additional silicone rubber, where it was affirmed that the upper edge of the silicone mold exactly parallels the edge of the cast base. After the arrangement of all teeth, the red wax was melted and poured into the silicone mold, and then the cast was applied and pressed (
Figure 1). The process was repeated 40 times.
2.3. Initial Installation on the Articulator
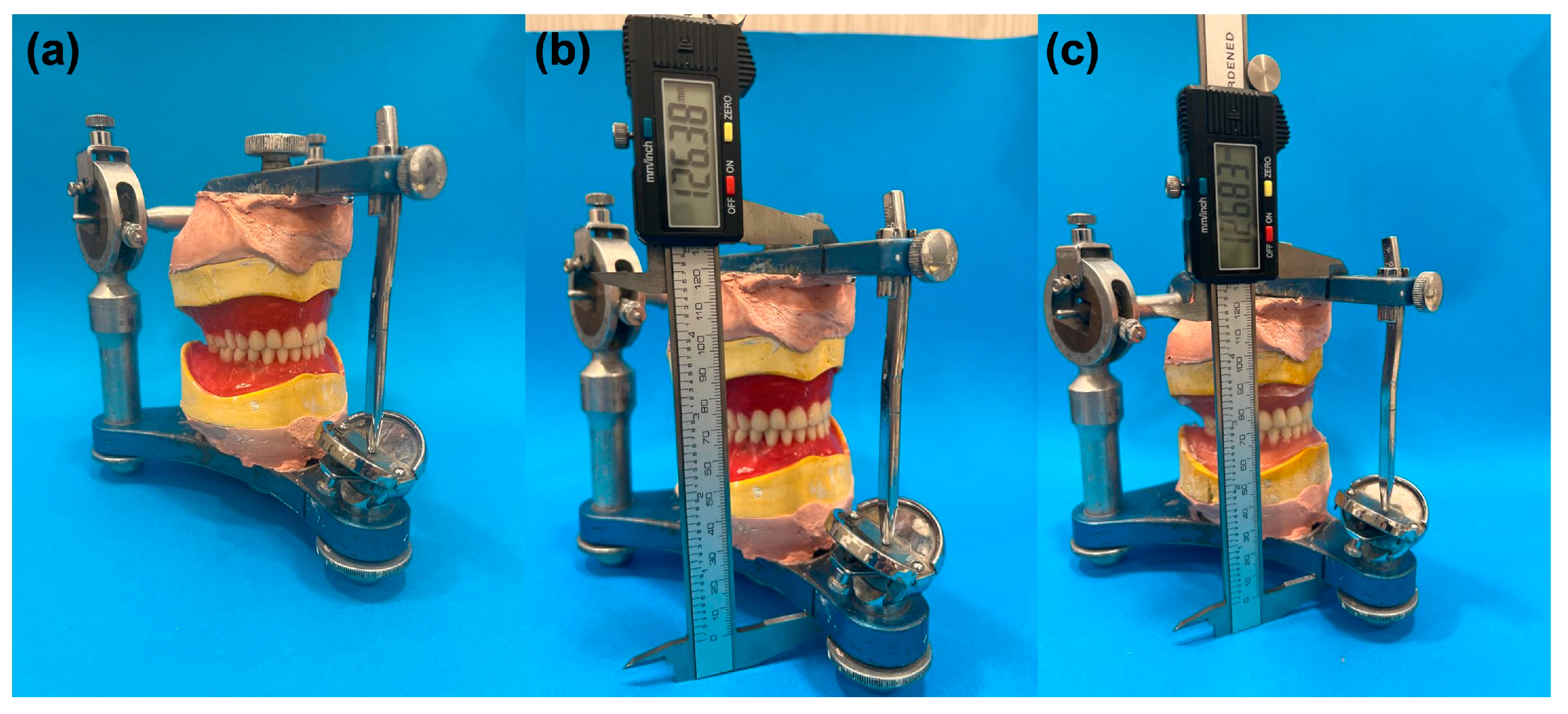
A semi-adjusted articulator was used, whereby two parallel reference lines were drawn on each of the upper and lower arms. The guide pin was fixed on the number zero. The ring of the articulator was installed on the upper arm, and the upper cast was positioned according to the reinstallation guide. After that, the upper cast was fixed using gypsum on the ring attached to the articulator. The two arms were tied with a rubber ring to ensure that they did not separate, and the plaster was left until it was completely hardened. After that, the reinstallation guide was removed, and the lower cast was fixed in its place in order to ensure that the teeth of the upper and lower experimental dentures were firmly crossed. Finally, the initial vertical dimension (before polymerized) (
Figure 2a) was measured between the two reference points (
Figure 2b) three times using a digital caliper scale (Mitutoyo Corporation, Kanagawa Japan), and the average of those measurements was taken to be the approved initial vertical occlusal dimension.
2.4. Cladding and Preparation for Polymerization of the Waxed Casts
Type II white plaster (Lap plaster, modern materials, Heraeus, Yardley, PA, USA) was placed within the lower half of the crucible. The gypsum wax model was isolated using silicate insulator (Divosep, vertex dental, Soesterberg, The Netherlands). Then, the cast was immersed in the white plaster until the edge of the lower part of the crucible. After that, the surface of the white plaster was isolated using silicate insulator (Divosep, vertex dental, The Netherlands) after hardening, and the upper half of the crucible was also isolated and applied onto the lower half. Type III yellow plaster was then applied until the incisal borders and cusps of the artificial teeth. After plaster hardening, the yellow plaster surface was isolated, and white plaster was poured until the crucible was full. After that, the crucible was immersed in boiling water for 5 min, the crucible was opened, and the melted wax was removed using a supplementary amount of boiling water. The surface of the gypsum mold was isolated by silicate insulator (Divosep, vertex dental, The Netherlands) using a brush. The artificial teeth were not isolated during this step. Then, the thermosetting acrylic resin (Vertex Regular, Vertex Dental, The Netherlands) was used according to the manufacturer’s instructions. After reaching the pasty phase, a sufficient amount of acrylic was applied to the upper half of the crucible. A sheet of polyethylene was placed on top of the acrylic paste, and the crucible was closed and slowly pressed by a hydraulic press at a pressure of 1500 psi, allowing the excess amount of acrylic resin to flow out. These acrylic excesses were removed with a spatula. This step (experimental closing process) was repeated 3 times. Finally, the polyethylene sheet was removed, and the crucible was finally closed at 3500 psi pressed by the hydraulic press, and it was tied with a manual clamp.
2.5. Dentures Polymerization Steps
The curing was performed by the following:
Group 1 (G1, control group): It was polymerized by the traditional water bath method within the Hanau device (Hanau Engineering, Buffalo, NY, USA), and the crucible was taken to the curing unit that was previously set according to the manufacturer’s instructions and was placed in water at a temperature of 74 °C for 90 min. Then, the temperature was raised to 100 °C, and the crucible was left at this temperature for 30 min.
Group 2 (G2): The autoclave was operated on a specific program so that the temperature and pressure gradually increased to reach (134 °C/2.1 bar) for 10 min, then cooled and gradually decreased the pressure for 11 min; then, the crucible was taken out and left to cool to room temperature.
Group 3 (G3): The autoclave was operated on a specific program in which the temperature and pressure gradually increased to reach (121 °C/1.1 bar) for 20 min, then cooled and gradually reduced pressure for 11 min; then, the crucible was taken out and left to cool to room temperature.
Group 4 (G4): The autoclave was operated on a specific program in which the temperature and pressure gradually increased to reach (121 °C/1.1 bar) for 5 min, then cooled and gradually reduced pressure for 8 min; then, the crucible was taken out and left to cool in room temperature.
2.6. Final Mounting on the Articulator and Measurement of the Vertical Occlusal Dimension
After the polymerization step, no finishing or polishing preparations were performed for the dentures, and only the remnants of plaster were cleaned. Upper and lower polymerized dentures were re-mounted on the semi-adjusted articulator using a gypsum base. After the verification of the complete entering of the cusps of the artificial teeth in their respective excavations, the distance between the two reference points located on the upper and lower arms of the articulator was measured three times (
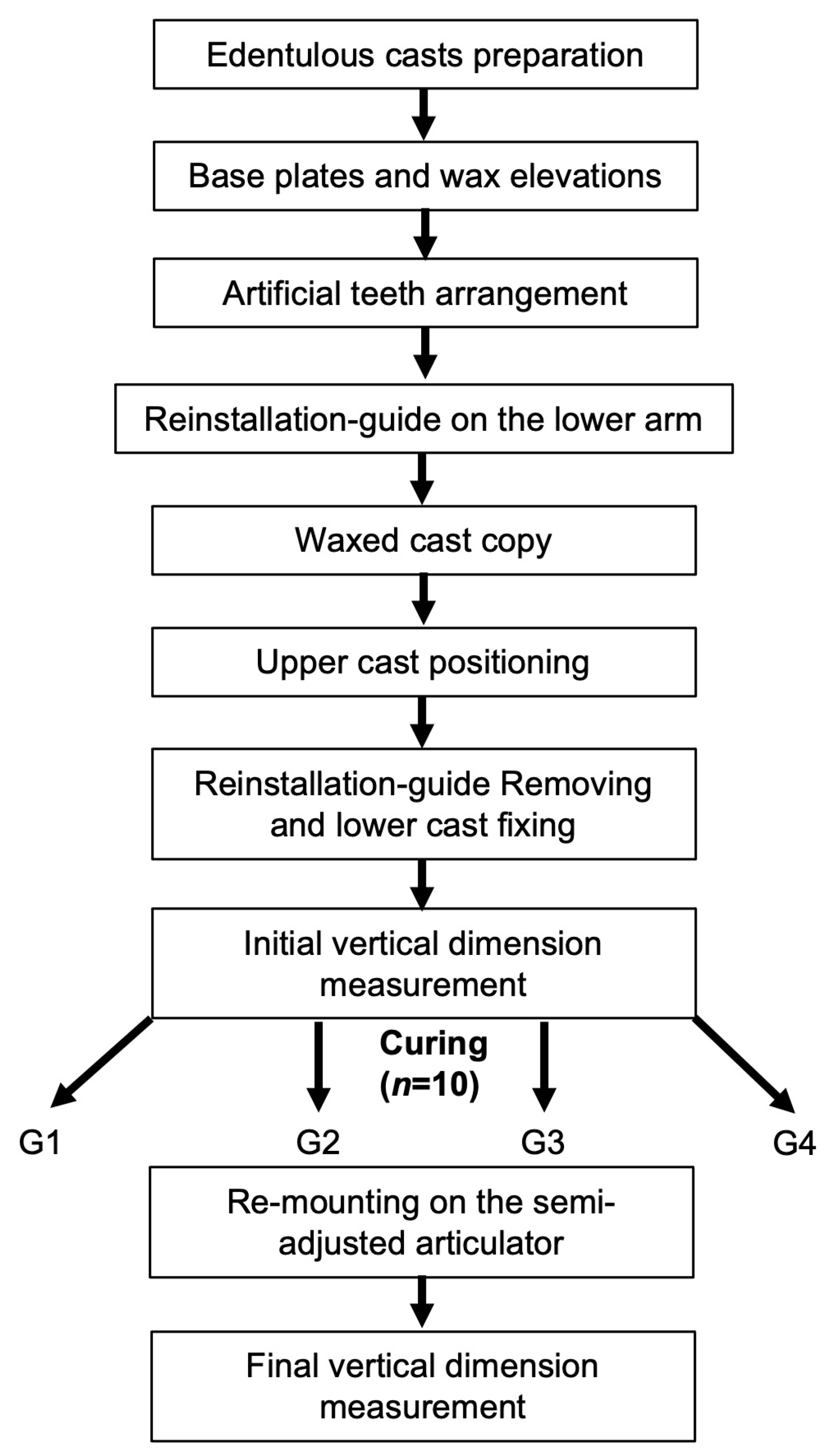
Figure 2c). The average of the recorded measurements was compared to the average of the initial measurements (before polymerization). The difference between the first measurement (before polymerization) and the second (after polymerization) was the change in the vertical occlusal dimension. All the methodological steps are summarized in
Figure 3.
2.7. Statistical Analysis
Statistical analysis was performed using SPSS software version (version 17, SPSS, Chicago, IL, USA). The Kolmogorov–Smirnov test was used to verify the normality of the data within all groups; thus, it revealed a normal distribution of the data. Therefore, paired t-test was used to determine whether significant differences existed between the initial and final vertical occlusal dimensions for each group. A one-way ANOVA test along with a multiple comparison procedure (Tukey’s test) was used to determine whether significant differences existed in the vertical occlusal dimension changes between the different curing techniques. In all tests, a statistical significance level of α = 0.05 was adopted.
3. Results
All groups showed a statistically significant increase in the vertical occlusal dimension after the polymerization step compared to the initial situation (p < 0.05).
The lowest change between the initial dimension and the change after polymerization step was observed in G1 (0.703 ± 0.078 mm).
The greatest change between the initial dimension and the change after polymerization step was observed in G4 (1.263 ± 0.063 mm).
Moreover, G2 (0.844 ± 0.061 mm) and G3 (0.88 ± 0.059 mm) demonstrated a statistically significant increase in the vertical dimension between the initial measurement (before polymerization) and the final measurement (after polymerization) (p < 0.05).
Statistically significant lower vertical dimension changes were detected in G1 compared to the other groups “G2, G3, G4” (p < 0.05).
Statistically significant higher changes were detected in G4 compared to the other groups ‘’G1, G2, G3” (p < 0.05).
No statistically significant differences were found between G2 (0.844 ± 0.061 mm) and G3 (0.88 ± 0.059 mm) (
p > 0.05) (
Table 1).
G1, G2 and G3 demonstrated vertical occlusal dimension changes of complete acrylic dentures lower than 1 mm after the different curing techniques, whilst G4 demonstrated dimension changes more than 1 mm after the polymerization step “(121 °C/1.1 bar) for 5 min”.
The change in the occlusal vertical dimension of the complete dentures was studied previously for different curing techniques such as compression method [
18], injection modeling [
19] and microwave processing [
20,
21]. Barbosa et al. [
20] determined the influence of different curing cycles in a microwave oven on changes in the occlusal vertical dimension of complete dentures. They reported that microwaves could change the vertical occlusal dimension (<0.5 mm). Moreover, Nelson et al. [
21] also studied the influence of curing in a microwave on the occlusal vertical dimension of complete dentures. They showed that the use of microwaves could increase the vertical occlusal dimension (0.628 ± 0.128 mm). Keenan et al. [
19] demonstrated that the injection method with different parameters could influence the vertical occlusal dimension of complete dentures between 0.52 and 0.75 mm. Strohaver [
18] compared the changes in vertical dimension after injection or compression procedure. The study showed that the injection method had lower changes (0.02 mm) compared to the compression procedure (0.66 mm).
4. Discussion
The traditional water bath method (short polymerization cycle) was used for the control group due to the common use of this method among labs and its simplicity. This method was used by many previous researchers and considered as a control method in the polymerization of the acrylic dentures [
15,
16,
17,
18,
20,
21,
22,
23,
24,
25,
26]. The polymerization using the autoclave technique was used previously by several researchers [
15,
16,
17,
22]. Despite this, no study addressed the changes in vertical occlusal dimension after the polymerization of acrylic dentures by using an autoclave with different parameters.
The present study suggested polymerization of a complete acrylic prosthesis with autoclave using three different parameters at a pressure of 2.1 bar/temperature of 134 °C for 10 min, at a pressure of 1.1 bar/temperature of 121 °C for 20 min, and at a pressure of 1.1 bar/121 °C of time 5 min, compared to the traditional method of polymerization acrylic prosthesis in a water bath. The traditional method was used in the present study as a control group in order to compare it to the other suggested automated methods. The parameters (temperatures and pressures) used in the autoclave groups (G2, G3 and G4) were chosen following the autoclave manufacturer’s instructions. The parameters used in G4 are similar to G3 but with less time to investigate the possibility of saving time without changing the other parameters (temperature and pressure). Higher temperature and pressure with less time were chosen for G2 compared to G3 in order to investigate their effects on the vertical dimension changes.
In the present study, both methods of polymerization (traditional and autoclave) increased the vertical occlusal dimension. This increase can be attributed to the type of gypsum used in making the main cast, the type of cladding material used, and the amount of free water, which change the amount of polymerization expansion of these materials [
26,
27]. In addition, statistically significant lower vertical dimension changes were detected for the traditional group compared to the other groups (
p < 0.05), whilst statistically greater changes were detected for the autoclave group with a pressure of 1.1 bar/121 °C of time 5 min (
p < 0.05). Therefore, the null hypothesis must be rejected.
The change in the vertical occlusal dimension in the control group was statistically lower compared to the other autoclave groups as well as lower than 1 mm, which is considered clinically acceptable [
21]. This result can be explained by various factors associated with the curing stage and the cooling stage, which resulted in a slight increase in the occlusal vertical dimension. In addition, the exposure of the crucibles directly for two hours in water in the traditional method (knowing that the water diffusion coefficient in acryl is 0.11 × 6
−10 cm
2/s [
27,
28]) makes slightly volumetric exposure in acrylic resin following the equation: each 1% increase in acryl weight resulting in 0.23% increase of volumetric expansion of the acrylic resin [
27]. The entry of water molecules into the resin mass results in two important effects, the slight expansion of the polymer mass and the interference of water molecules with the crosslinked polymer chains [
27,
29].
The higher increase of vertical occlusal dimension in both Groups 2 and 3 compared to the control group (G1) can be explained by the fact that the curing time in both groups was less than that for the control group, as this may cause of higher percentages of non-ionotropic monomers, and thus the polymer chains will move away from each other [
29].
The clinically acceptable results (<1 mm) of Groups 2 and 3 compared to Group 4 can be explained by the following: (1) The increase in the pressure inside the autoclave chamber in addition to the closure of the crucibles at a pressure of 241.32 bar, which can bring the polymer chains closer together. (2) Raising the pressure on the resin to the value of 11.65 bar raises the boiling/evaporating/monomer temperature to 193 °C, as well as raising the pressure on the resin to the value of 22.79 bar, which raises the boiling/evaporation/monomer temperature to 228 °C so that no porosity occurs within the acrylic resin, meaning that sufficient pressure led to an increase in the monomer’s boiling temperature and prevented it from evaporating [
30]. (3) The cycle of coagulation or solidification (which is the temperature used to control coagulation at a specific time) is completely and automatically controlled by the autoclave device in the transition between the stages of vacuum, pressure raising and the introduction of high-temperature steam into the pressure chamber. Therefore, the cured acryl is not exposed to any effect of a random rise in temperature that leads to the boiling of the monomer and porosity at the base of the device [
27]. (4) Studies have shown that it is possible to obtain satisfactory and convergent results between curing in a traditional water bath and other methods to provide the necessary heat to stimulate the fumigation reaction “steam–dry air ovens–infrared rays…” provided that the temperature and pressure applied to the crucibles are well controlled and non-random [
29].
The close result in Groups 2 and 3, where no statistically significant differences appeared between them in terms of increase in the occlusal vertical dimension after curing, can be explained by the fact that despite Group 3 exposure to lower pressure and temperature than Group 2, the decrease in these conditions was increased by doubling the time from 10 min to 20 min in Group 3, resulting in two similar groups that were both clinically acceptable (<1 mm).
Group 4 had statistically higher vertical occlusal dimension change compared to the other groups (p < 0.05). This may be explained by the fact that different parameters could play an important role in the change of the vertical occlusal dimensions, such as the pressure, temperature and curing time. The time of curing in G4 was 5 min which is half of the curing time in G2, as well as the pressure was 1.1 bar compared to 2.1 bar in G2, which demonstrated clinically accepted results. Therefore, time and pressure could be considered important parameters on the changes of the occlusal vertical dimension when using autoclave systems to harden the acrylic devices.
The outcomes of the present study showed that two groups among the three autoclave curing groups (G2 and G3) are clinically acceptable for curing the bases of dentures. Therefore, these two methods (G2 and G3) could be used in dental practice to improve the physical and chemical properties of complete dentures as well as save time; and easier methods (fully automated) compared to the traditional method (G1).
Within the limitations of an in vitro study, these results are relevant to confirm the complexity of the change in vertical occlusion dimension in the complete dentures. From a clinical standpoint, the difference observed in the vertical occlusal dimension after the different curing methods could indicate to the dental laboratories which use the autoclave technique to avoid the low pressure and the short time, which could influence the vertical occlusal dimension. One of the limitations of the present study was that the remounting of the models on the articulator is a very sensitive step and should be carefully performed. Moreover, the arrangement of artificial teeth should be carried out by an expert in order to validate the correct occlusion. Further studies are necessary to investigate denture-processing methods that can yield minimal vertical occlusal dimension change. Moreover, future studies should be performed to investigate the effect of autoclave curing on various resins, as well as the influences contributed by the different used times and temperatures of autoclave curing in the studies on different resins.








{kind=link}
{kind=link}
{kind=link}