
Augmented Reality and Virtual Reality in Dentistry: Highlights from the Current Research

 ,
,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
- Clinical trials
- Case-control studies
- Observational studies
- Studies where AR and VR have focused on dentistry
- Studies in the English Language
- Review articles
- Short communications
- Letters to Editors
- Studies in languages other than English
3. Outcomes of Literature Search
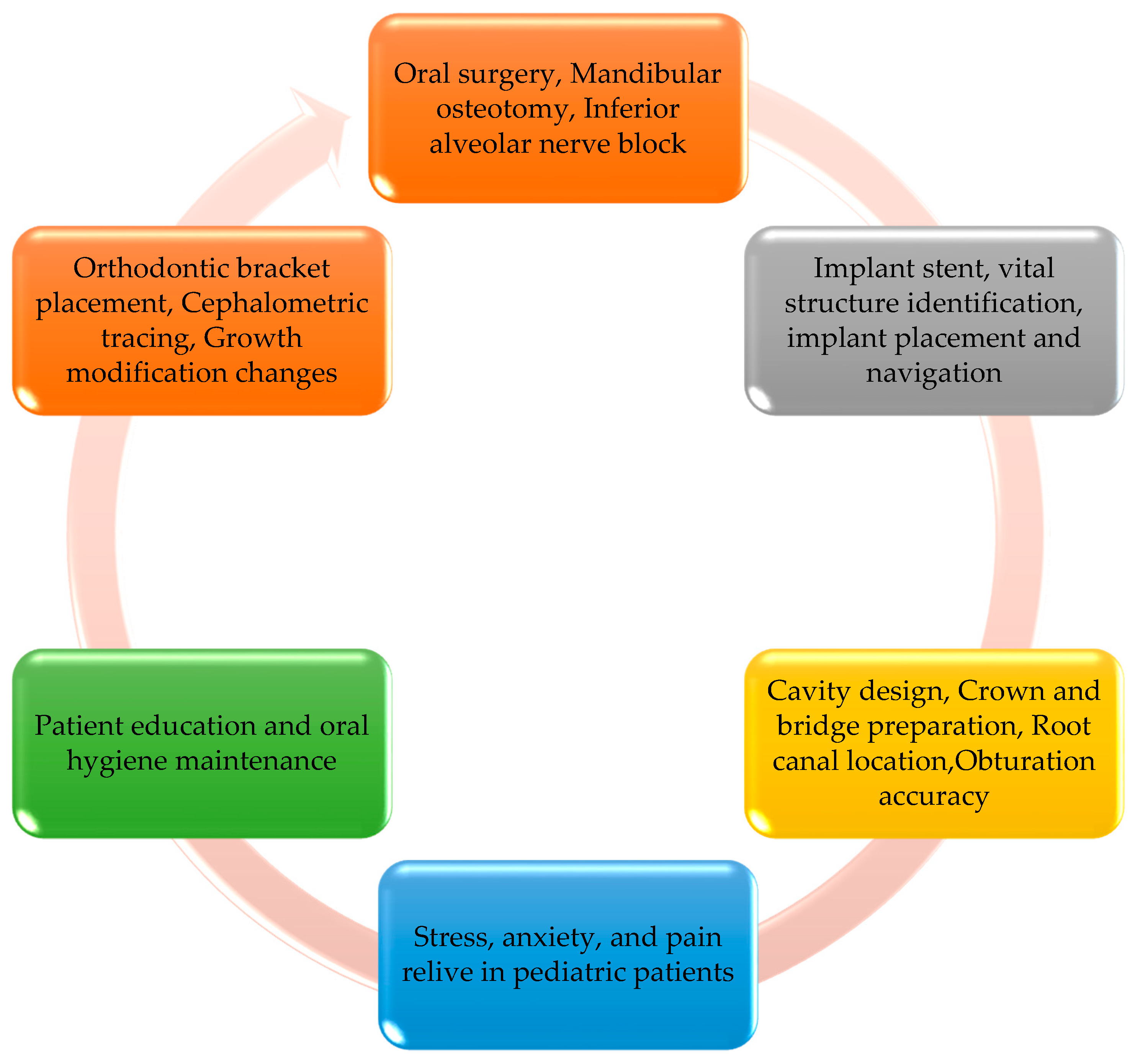
4. Applications of AR and VR in Dentistry
4.1. AR and VR in Dental Specialties
4.2. AR and VR in Dental Education/Training
4.3. AR and VR in Oral and Maxillofacial Surgery
4.4. AR and VR in Paediatric Dentistry
4.5. AR and VR in Dental Implantology
4.6. AR and VR in Restorative Dentistry and Endodontics
5. Clinical Implications of Haptic Feedback in AR/VR
6. Whether to Embrace AR/VR Systems or Not?
7. Future Recommendations
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, T.-K.; Yang, C.-H.; Hsieh, Y.-H.; Wang, J.-C.; Hung, C.-C. Augmented reality (AR) and virtual reality (VR) applied in dentistry. Kaohsiung J. Med. Sci. 2018, 34, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Freina, L.; Ott, M. A literature review on immersive virtual reality in education: State of the art and perspectives. In Proceedings of the International Scientific Conference eLearning and Software for Education (eLSE), Bucharest, Romania, 23–24 April 2015. [Google Scholar] [CrossRef]
- Lambooij, M.; Fortuin, M.; Heynderickx, I.; Ijsselsteijn, W. Visual Discomfort and Visual Fatigue of Stereoscopic Displays: A Review. J. Imaging Sci. Technol. 2009, 53, 30201–30211. [Google Scholar] [CrossRef] [Green Version]
- Kwon, H.-B.; Park, Y.-S.; Han, J.-S. Augmented reality in dentistry: A current perspective. Acta Odontol. Scand. 2018, 76, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kim, H.; Kim, Y.O. Virtual Reality and Augmented Reality in Plastic Surgery: A Review. Arch. Plast. Surg. 2017, 44, 179–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, J.; Tan, G.; Zhan, T.; Wu, S.-T. Breaking the field-of-view limit in augmented reality with a scanning waveguide display. OSA Contin. 2020, 3, 2730–2740. [Google Scholar] [CrossRef]
- Zafar, S.; Zachar, J.J. Evaluation of HoloHuman augmented reality application as a novel educational tool in dentistry. Eur. J. Dent. Educ. 2020, 24, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Green, B.N.; Johnson, C.D.; Adams, A. Writing narrative literature reviews for peer-reviewed journals: Secrets of the trade. J. Chiropr. Med. 2006, 5, 101–117. [Google Scholar] [CrossRef] [Green Version]
- Ran, L.; Zhao, N.; Fan, L.; Zhou, P.; Zhang, C.; Yu, C. Application of virtual reality on non-drug behavioral management of short-term dental procedure in children. Trials 2021, 22, 562. [Google Scholar] [CrossRef]
- Felemban, O.M.; Alshamrani, R.M.; Aljeddawi, D.H.; Bagher, S.M. Effect of virtual reality distraction on pain and anxiety during infiltration anesthesia in pediatric patients: A randomized clinical trial. BMC Oral Health 2021, 21, 321. [Google Scholar] [CrossRef] [PubMed]
- Gujjar, K.R.; van Wijk, A.; Kumar, R.; de Jongh, A. Efficacy of virtual reality exposure therapy for the treatment of dental phobia in adults: A randomized controlled trial. J. Anxiety Disord. 2019, 62, 100–108. [Google Scholar] [CrossRef]
- Jiang, W.; Ma, L.; Zhang, B.; Fan, Y.; Qu, X.; Zhang, X.; Liao, H. Evaluation of the 3D augmented reality–guided intraoperative posit ioning of dental implants in edentulous mandibular models. Int. J. Oral Maxillofac. Implant. 2018, 33, 1219–1228. [Google Scholar] [CrossRef] [PubMed]
- Murugesan, Y.P.; Alsadoon, A.; Manoranjan, P.; Prasad, P. A novel rotational matrix and translation vector algorithm: Geometric accuracy for augmented reality in oral and maxillofacial surgeries. Int. J. Med. Robot. Comput. Assist. Surg. 2018, 14, e1889. [Google Scholar] [CrossRef] [PubMed]
- Pulijala, Y.; Ma, M.; Pears, M.; Peebles, D.; Ayoub, A. Effectiveness of Immersive Virtual Reality in Surgical Training—A Randomized Control Trial. J. Oral Maxillofac. Surg. 2018, 76, 1065–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreurs, R.; Dubois, L.; Becking, A.; Maal, T. Implant-oriented navigation in orbital reconstruction. Part 1: Technique and accuracy study. Int. J. Oral Maxillofac. Surg. 2018, 47, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Llena, C.; Folguera, S.; Forner, L.; Rodríguez-Lozano, F.J. Implementation of augmented reality in operative dentistry learning. Eur. J. Dent. Educ. 2018, 22, e122–e130. [Google Scholar] [CrossRef]
- Won, Y.J.; Kang, S.H. Application of augmented reality for inferior alveolar nerve block anesthesia: A technical note. J. Dent. Anesth. Pain Med. 2017, 17, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, M.; Chai, G.; Zhang, Y.; Ma, X.; Gan, J. Registration Strategy Using Occlusal Splint Based on Augmented Reality for Mandibular Angle Oblique Split Osteotomy. J. Craniofacial Surg. 2011, 22, 1806–1809. [Google Scholar] [CrossRef] [PubMed]
- Bruellmann, D.D.; Tjaden, H.; Schwanecke, U.; Barth, P. An optimized video system for augmented reality in endodontics: A feasibility study. Clin. Oral Investig. 2012, 17, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Aichert, A.; Wein, W.; Ladikos, A.; Reichl, T.; Navab, N. Image-Based Tracking of the Teeth for Orthodontic Augmented Reality. Comput. Vision 2012, 15, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Bogdan, C.M.; Popovici, D.M. Information system analysis of an e-learning system used for dental restorations simulation. Comput. Methods Programs Biomed. 2012, 107, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Gao, Y.; Abdelrehem, A.; Zhang, L.; Chen, X.; Xie, L.; Wang, X. Augmented reality navigation method for recontouring surgery of craniofacial fibrous dysplasia. Sci. Rep. 2021, 11, 10043. [Google Scholar] [CrossRef]
- Lahti, S.; Suominen, A.; Freeman, R.; Lähteenoja, T.; Humphris, G. Virtual Reality Relaxation to Decrease Dental Anxiety: Immediate Effect Randomized Clinical Trial. JDR Clin. Transl. Res. 2020, 5, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Suenaga, H.; Yang, L.; Kobayashi, E.; Sakuma, I. Video see-through augmented reality for oral and maxillofacial surgery. Int. J. Med. Robot. Comput. Assist. Surg. 2017, 13, e1754. [Google Scholar] [CrossRef] [PubMed]
- Qu, M.; Hou, Y.; Xu, Y.; Shen, C.; Zhu, M.; Xie, L.; Wang, H.; Zhang, Y.; Chai, G. Precise positioning of an intraoral distractor using augmented reality in patients with hemifacial microsomia. J. Cranio-Maxillofac. Surg. 2015, 43, 106–112. [Google Scholar] [CrossRef]
- Badiali, G.; Ferrari, V.; Cutolo, F.; Freschi, C.; Caramella, D.; Bianchi, A.; Marchetti, C. Augmented reality as an aid in maxillofacial surgery: Validation of a wearable system allowing maxillary repositioning. J. Cranio-Maxillofac. Surg. 2014, 42, 1970–1976. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-K.; Yau, H.-T.; Wang, I.-C.; Zheng, C.; Chung, K.-H. A Novel Dental Implant Guided Surgery Based on Integration of Surgical Template and Augmented Reality. Clin. Implant Dent. Relat. Res. 2015, 17, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y.-J.; Choi, J.-S.; Kim, J.; Kim, H.-J.; Moon, S.-Y. Virtual Reality (VR) Simulation and Augmented Reality (AR) Navigation in Orthognathic Surgery: A Case Report. Appl. Sci. 2021, 11, 5673. [Google Scholar] [CrossRef]
- Arikatla, V.S.; Tyagi, M.; Enquobahrie, A.; Nguyen, T.; Blakey, G.H.; White, R.; Paniagua, B. High fidelity virtual reality orthognathic surgery simulator. In Medical Imaging 2018: Image-Guided Procedures, Robotic Interventions, and Modeling; International Society for Optics and Photonics: Bellingham, WA, USA, 2018; Volume 10576, p. 1057612. [Google Scholar]
- Abbasi, H.; Saqib, M.; Jouhar, R.; Lal, A.; Ahmed, N.; Ahmed, M.A.; Alam, M.K. The Efficacy of Little Lovely Dentist, Dental Song, and Tell-Show-Do Techniques in Alleviating Dental Anxiety in Paediatric Patients: A Clinical Trial. BioMed Res. Int. 2021, 2021, 1119710. [Google Scholar] [CrossRef] [PubMed]
- Albakri, G.; Bouaziz, R.; Alharthi, W.; Kammoun, S.; Al-Sarem, M.; Saeed, F.; Hadwan, M. Phobia Exposure Therapy Using Virtual and Augmented Reality: A Systematic Review. Appl. Sci. 2022, 12, 1672. [Google Scholar] [CrossRef]
- Raikar, S.; Talukdar, P.; Kumari, S.; Panda, S.K.; Oommen, V.M.; Prasad, A. Factors affecting the survival rate of dental implants: A retrospective study. J. Int. Soc. Prev. Community Dent. 2017, 7, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, S.; Ohtani, T.; Ono, S.; Yamanishi, Y.; Sohmura, T.; Yatani, T.S.A.H. Intuitive Surgical Navigation System for Dental Implantology by Using Retinal Imaging Display. In Implant Dentistry—A Rapidly Evolving Practice; InTech: London, UK, 2011. [Google Scholar]
- Durham, M.; Engel, B.; Ferrill, T.; Halford, J.; Singh, T.P.; Gladwell, M. Digitally Augmented Learning in Implant Dentistry. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 387–398. [Google Scholar] [CrossRef] [PubMed]
- McGleenon, E.L.; Morison, S. Preparing dental students for independent practice: A scoping review of methods and trends in undergraduate clinical skills teaching in the UK and Ireland. Br. Dent. J. 2021, 230, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.L.-S.; Yeung, C.; Chu, S.; Wong, A.W.-Y.; Yu, O.Y.; Chu, C.-H. Use of Computer Simulation in Dental Training with Special Reference to Simodont. Dent. J. 2021, 9, 125. [Google Scholar] [CrossRef]
- Tabassum, S.; Khan, F.R. Failure of endodontic treatment: The usual suspects. Eur. J. Dent. 2016, 10, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, A. The Factors Responsible for Endodontic Treatment Failure in the Permanent Dentitions of the Patients Reported to the College of Dentistry, the University of Aljouf, Kingdom of Saudi Arabia. J. Clin. Diagn. Res. 2016, 10, ZC146–ZC148. [Google Scholar] [CrossRef] [PubMed]
- Peterson, D.C.; Mlynarczyk, G.S. Analysis of traditional versus three-dimensional augmented curriculum on anatomical learning outcome measures. Anat. Sci. Educ. 2016, 9, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Dissabandara, L.O.; Nirthanan, S.N.; Khoo, T.K.; Tedman, R. Role of cadaveric dissections in modern medical curricula: A study on student perceptions. Anat. Cell Biol. 2015, 48, 205–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, E.W.; Slott, P.A.; Terracio, L.; Cunningham, E. An Innovative Method for Teaching Anatomy in the Predoctoral Dental Curriculum. J. Dent. Educ. 2013, 77, 1498–1507. [Google Scholar] [CrossRef] [PubMed]
- Mladenovic, R.; AlQahtani, S.; Mladenovic, K.; Bukumiric, Z.; Zafar, S. Effectiveness of technology-enhanced teaching methods of undergraduate dental skills for local anaesthesia administration during COVID-19 era: Students’ perception. BMC Oral Health 2022, 22, 40. [Google Scholar] [CrossRef]
- Gaviria, L.; Salcido, J.P.; Guda, T.; Ong, J.L. Current trends in dental implants. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 50–60. [Google Scholar] [CrossRef]
- Vieira, A.R.; Silva, M.B.; Souza, K.K.A.; Filho, A.V.A.; Rosenblatt, A.; Modesto, A. A Pragmatic Study Shows Failure of Dental Composite Fillings Is Genetically Determined: A Contribution to the Discussion on Dental Amalgams. Front. Med. 2017, 6, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, D.; Shi, Y.; Liu, S.; Zhang, Y.; Xiao, J. Haptic Simulation of Organ Deformation and Hybrid Contacts in Dental Operations. IEEE Trans. Haptics 2014, 7, 48–60. [Google Scholar] [CrossRef] [PubMed]
- Overtoom, E.M.; Horeman, T.; Jansen, F.-W.; Dankelman, J.; Schreuder, H.W.R. Haptic Feedback, Force Feedback, and Force-Sensing in Simulation Training for Laparoscopy: A Systematic Overview. J. Surg. Educ. 2019, 76, 242–261. [Google Scholar] [CrossRef] [PubMed]
- Dorri, M. Healthcare research: VR and AR. Br. Dent. J. 2017, 222, 224–225. [Google Scholar] [CrossRef]
- Zimmer, A.; Wang, N.; Ibach, M.K.; Fehlmann, B.; Schicktanz, N.S.; Bentz, D.; Michael, T.; Papassotiropoulos, A.; de Quervain, D.J. Effectiveness of a smartphone-based, augmented reality exposure app to reduce fear of spiders in real-life: A randomized controlled trial. J. Anxiety Disord. 2021, 82, 102442. [Google Scholar] [CrossRef] [PubMed]
- Mladenovic, R.; Dakovic, D.; Pereira, L.; Matvijenko, V.; Mladenovic, K. Effect of augmented reality simulation on admin-istration of local anaesthesia in paediatric patients. Eur. J. Dent. Educ. 2020, 24, 507–512. [Google Scholar] [CrossRef]


{kind=link}
| Author ID and Year | Study Design | Sample Size | Outcomes | Field of Dentistry |
|---|---|---|---|---|
| Longkuan et al. [9] 2021 | Clinical Trial | 120 | The use of virtual reality resulted in decreased anxiety and pain in children | Pediatric Dentistry |
| Osama et al. [10] 2021 | Clinical Trial | 50 | Virtual reality is effective in reducing anxiety and pain | Pediatric Dentistry |
| Liu et al. [22] 2021 | Cross-sectional study | 5 | Augmented reality improved the efficiency and safety of craniofacial fibrous dysplasia recontouring | Oral and Maxillofacial Surgery |
| Lahti et al. [23] 2020 | Clinical Trial | 255 | Virtual reality resulted in a decrease in preoperative dental anxiety | Dental Public Health |
| Gujjar et al. [11] 2019 | Clinical Trial | 30 | Virtual reality was found to be effective in dental phobia treatment | Preventive Dentistry |
| Jiang et al. [12] 2018 | Clinical Trial | 12 | Improved accuracy and efficiency of virtual reality | Dental Implantology |
| Murugesan et al. [13] 2018 | Experimental Study | 23 | Expectable accuracy of VR | Oral and Maxillofacial Surgery |
| Pulijala et al. [14] 2018 | Clinical Trial | 98 | VR improves self-confidence and knowledge amongst surgical residents | Oral and Maxillofacial Surgery |
| Schreurs et al. [15] 2018 | Pilot Study | 1 | A novel concept of orbital reconstruction | Oral and Maxillofacial Surgery |
| Llena et al. [16] 2018 | Case-control | 41 | AR resulted in improved knowledge and skills | Operative Dentistry |
| Won YJ et al. [17] 2017 | Descriptive | 1 | Use of VR in inferior alveolar nerve block | Oral and Maxillofacial Surgery |
| Zhu et al. [18] 2017 | Clinical Trial | 20 | AR resulted in improved and effective mandibular angle oblique split osteotomy | Oral and Maxillofacial surgery |
| Bruellmann et al. [19] 2013 | In vitro study | 126 | Real-time detection of root canal orifices | Endodontics |
| Aichert et al. [20] 2012 | Experimental study | 1 | Use of AR in orthodontics procedure | Orthodontics |
| Bogdan et al. [21] 2011 | Descriptive study | Not mentioned | Use of VR for dental education of students | Dental Education |
| Wang et al. [24] 2017 | Clinical Trial | 2 | VR can be integrated into OMFS | Oral and Maxillofacial Surgery |
| Suenaga et al. [6] 2015 | Clinical Trial | 1 | The use of AR improves 3D-CT images with higher accuracy | Oral and Maxillofacial Surgery |
| Qu M et al. [25] 2015 | Clinical Trial | 20 | AR enhances intraoperative distraction osteogenesis | Oral and Maxillofacial Surgery |
| Badiali et al. [26] 2014 | Experimental Study | 1 | AR enhances surgical procedures | Oral and Maxillofacial Surgery |
| Lin et al. [27] 2013 | In vitro study | 40 | AR-enhanced implant placement | Oral Implantology |
| Parameters | Traditional Dentistry | AR-Based Dentistry | VR-Based Dentistry |
|---|---|---|---|
| Alleviation of Dental Anxiety Pre-Operatively | Achieved Verbally OR via Sedation/Psychotherapy (Practiced Commonly Worldwide) | Smartphone/Tablet-Based AR Exposure Apps (restricted to Laboratories and Experiments) | VR Headset soothes patient with a tranquil virtual environment (Integration in Limited number of Dental Offices) |
| Pain Management | Pharmacotherapy/prophylaxis-based pain management | AR simulators enhance pain threshold | Pain intensity is perceived artificially through a virtual simulation |
| Training Opportunity | Not effective for complex cases; poses risk for real patients | Dental Training units featuring AR-based systems; complex cases practiced safely | Dental training units featuring haptic technology: complex cases practiced safely and with precision with haptic feedback |
| Patients’ Accurately Understand Dental Procedures | Not Reliable | Fully Reliable | Fully Reliable |
| Remote Equipment Repairs | Not possible hence procedures are halted until a technician repairs in-person | Unexplored | Possible hence faulty equipment repaired easily with technician’s guidance remotely |
| Patients’ Symptoms Experienced by Dentist First-hand | The dentist cannot relate accurately | Unexplored | The dentist is fully empathetic as one can experience a particular symptom virtually |
| 360-degree View of the Operatory Experienced Remotely | Possible but does not provide a realistic experience | Provides incredibly realistic experience | Provides fully immersive virtual views |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fahim, S.; Maqsood, A.; Das, G.; Ahmed, N.; Saquib, S.; Lal, A.; Khan, A.A.G.; Alam, M.K. Augmented Reality and Virtual Reality in Dentistry: Highlights from the Current Research. Appl. Sci. 2022, 12, 3719. https://doi.org/10.3390/app12083719
Fahim S, Maqsood A, Das G, Ahmed N, Saquib S, Lal A, Khan AAG, Alam MK. Augmented Reality and Virtual Reality in Dentistry: Highlights from the Current Research. Applied Sciences. 2022; 12(8):3719. https://doi.org/10.3390/app12083719
Chicago/Turabian StyleFahim, Sidra, Afsheen Maqsood, Gotam Das, Naseer Ahmed, Shahabe Saquib, Abhishek Lal, Abdul Ahad Ghaffar Khan, and Mohammad Khursheed Alam. 2022. "Augmented Reality and Virtual Reality in Dentistry: Highlights from the Current Research" Applied Sciences 12, no. 8: 3719. https://doi.org/10.3390/app12083719