
3D Printing of Tooth Impressions Based on Multi-Detector Computed Tomography Images Combined with Beam Hardening Artifact Reduction in Metal Structures

Abstract
:1. Introduction
2. Materials and Methods
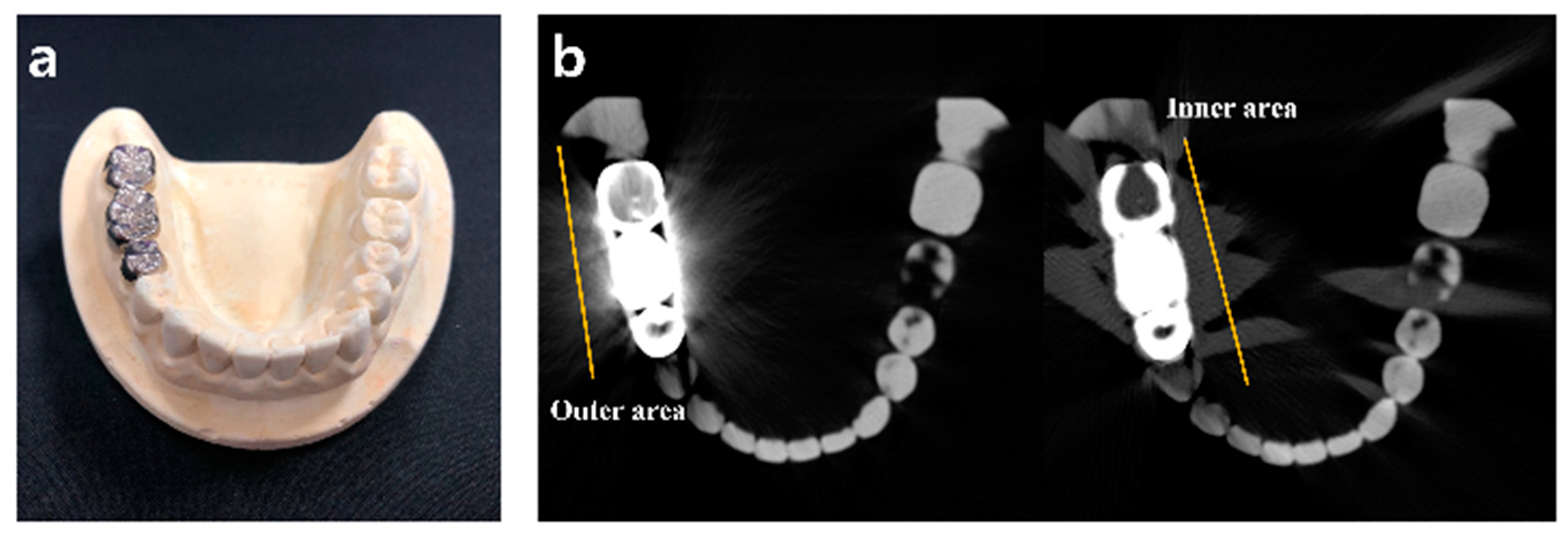
2.1. CT Data Optimized for Metal Artifact Reduction and Phantom Composition
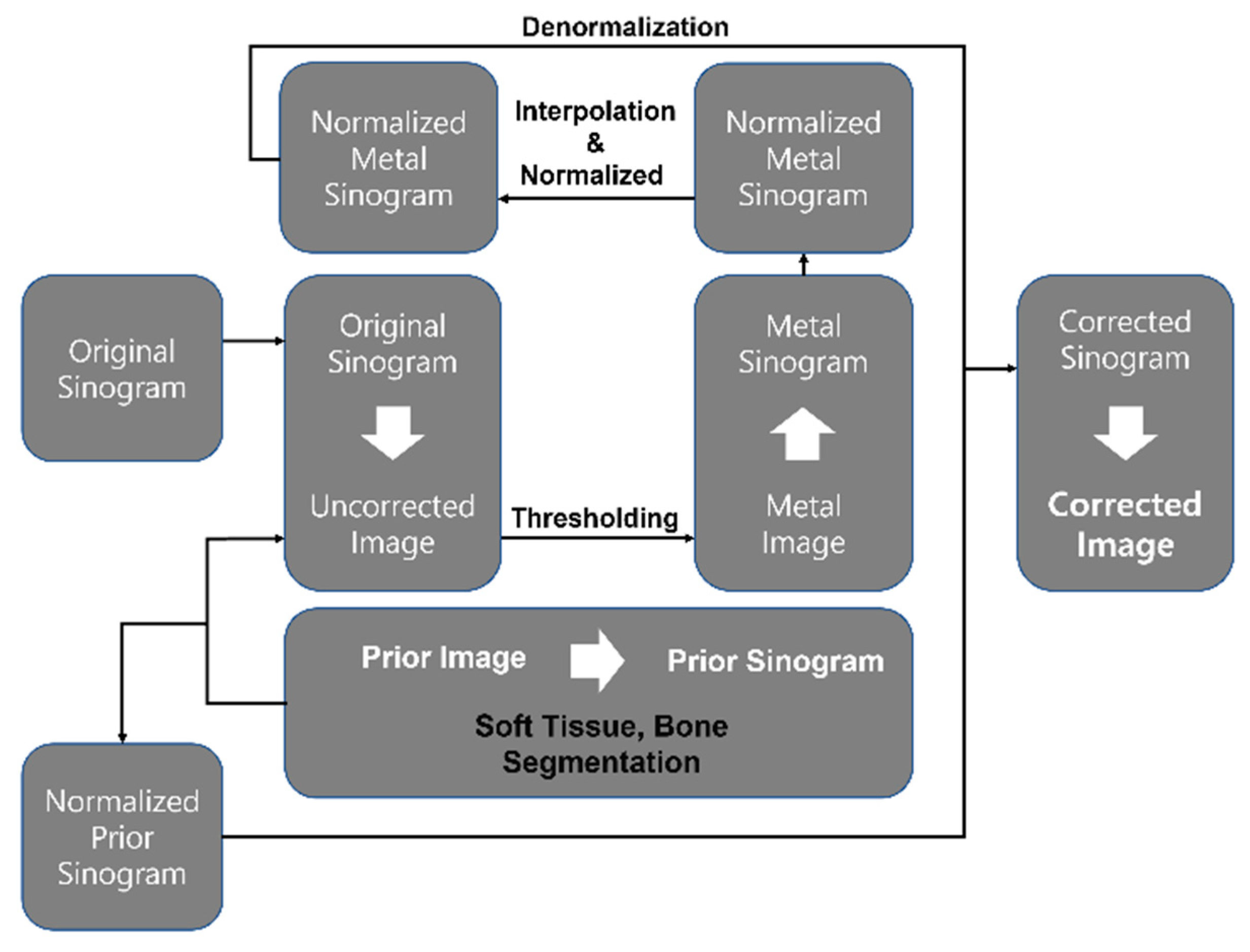
2.2. Application of iMAR Algorithm
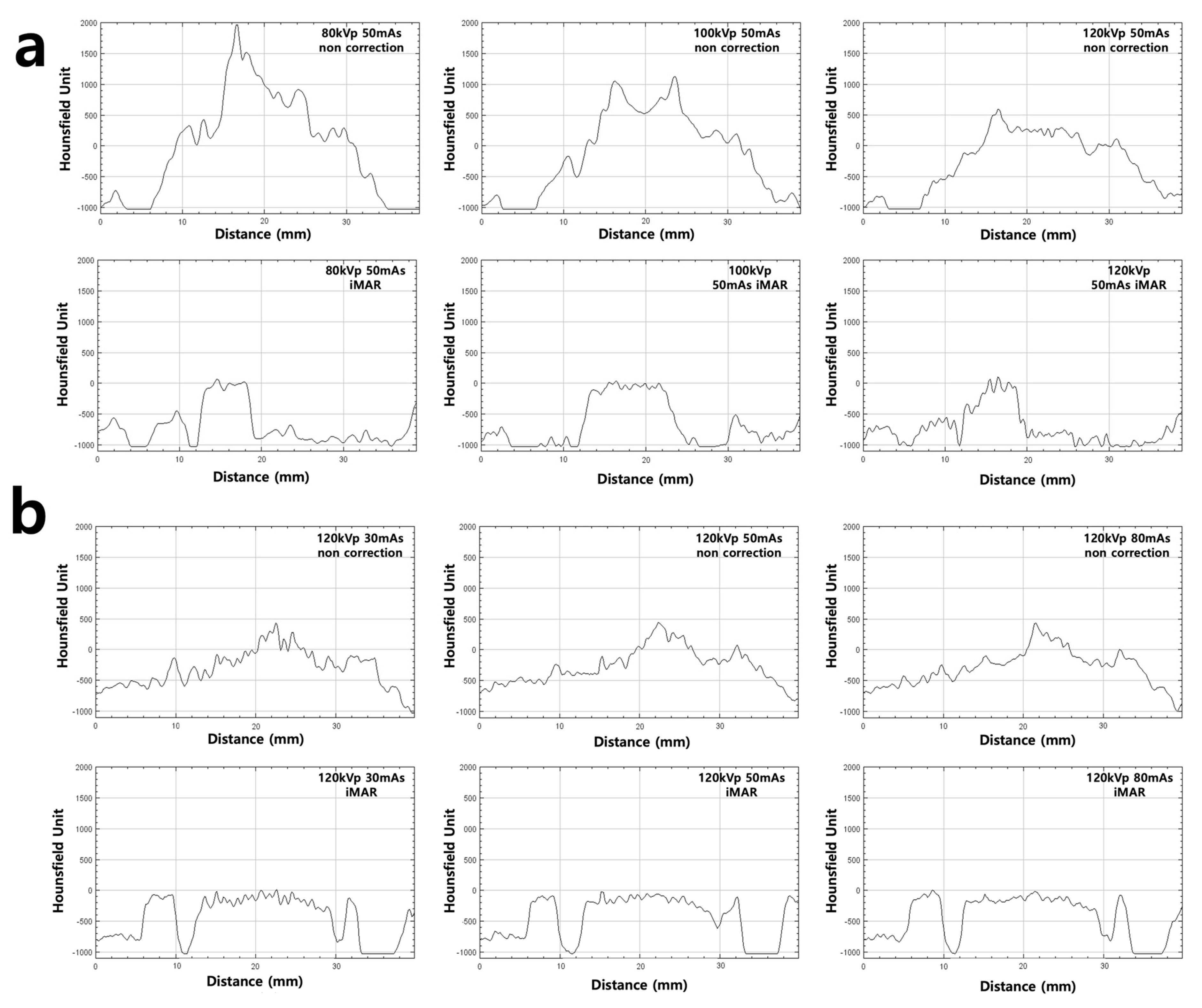
2.3. Measurement of Metal Artifact
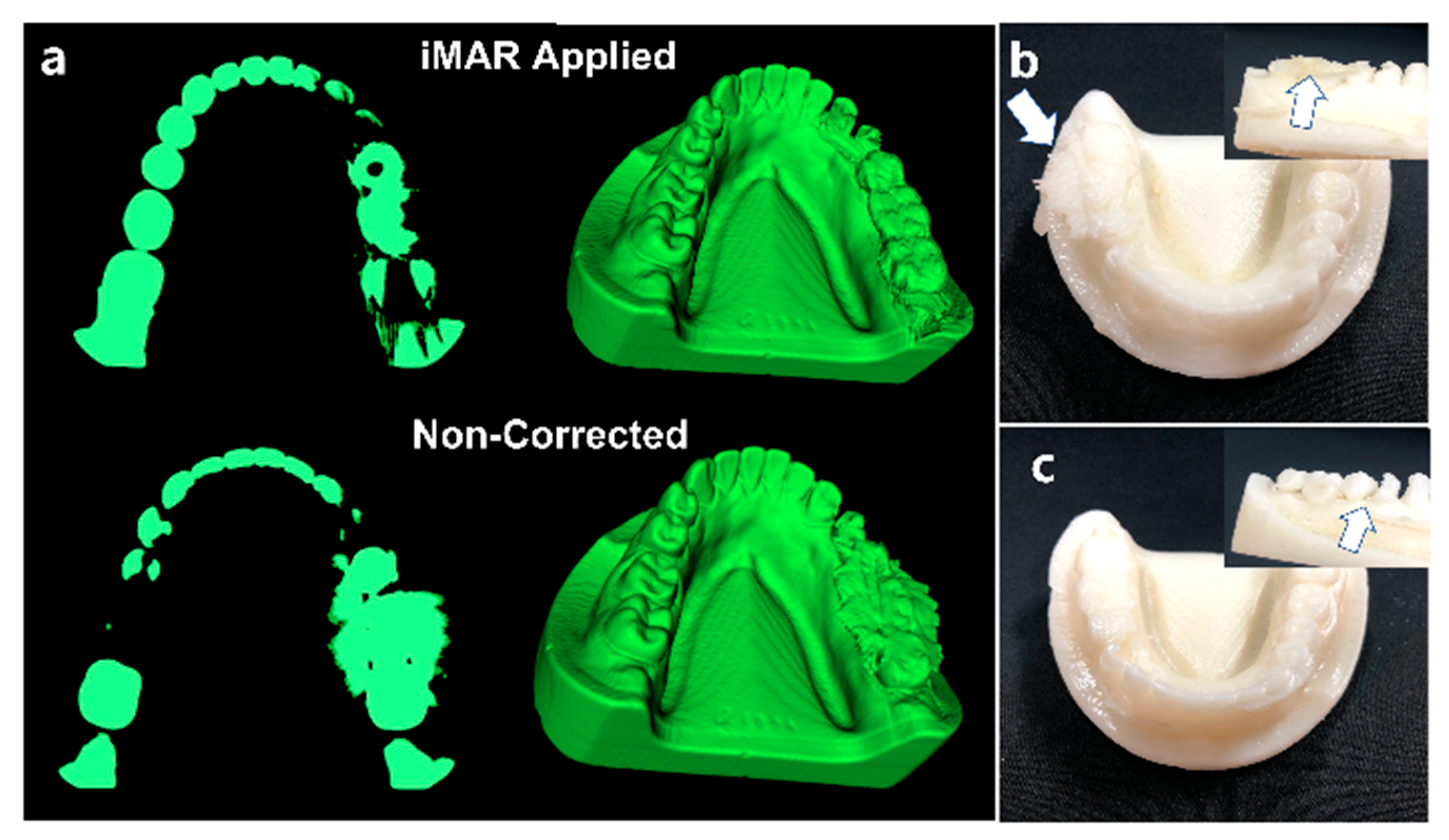
2.4. 3D Printing Processing
3. Results
3.1. CT Image Metal Artifact Evaluation
3.2. 3D Printing Product
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Giordano, R., 2nd. Impression materials: Basic properties. Gen. Dent. 2000, 48, 510–512. [Google Scholar] [PubMed]
- Miyasaka, S. Department on latex impression materials; on basic properties of impression materials by use of blende latex as a base. J. Jpn. Res. Soc. Dent. Mater. Appl. 1973, 30, 7–21. [Google Scholar]
- Ender, A.; Mehl, A. In-vitro evaluation of the accuracy of conventional and digital methods of obtaining full-arch dental impressions. Quintessence Int. 2015, 46, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Renne, W.; Ludlow, M.; Fryml, J.; Schurch, Z.; Mennito, A.; Kessler, R.; Lauer, A. Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons. J. Prosthet. Dent. 2017, 118, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Soto-Alvarez, C.; Fonseca, G.M.; Viciano, J.; Aleman, I.; Rojas-Torres, J.; Zuniga, M.H.; Lopez-Lazaro, S. Reliability, reproducibility and validity of the conventional buccolingual and mesiodistal measurements on 3D dental digital models obtained from intra-oral 3D scanner. Arch. Oral. Biol. 2020, 109, 104575. [Google Scholar] [CrossRef] [PubMed]
- Rajshekar, M.; Julian, R.; Williams, A.-M.; Tennant, M.; Forrest, A.; Walsh, L.J.; Wilson, G.; Blizzard, L. The reliability and validity of measurements of human dental casts made by an intra-oral 3D scanner, with conventional hand-held digital callipers as the comparison measure. Forensic Sci. Int. 2017, 278, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Durán Muñoz-Cruzado, V.; Calero Castro, F.J.; Padillo Eguía, A.; Tallón Aguilar, L.; Tinoco González, J.; Puyana, J.C.; Pareja Ciuró, F.; Padillo-Ruiz, J. Using a bio-scanner and 3D printing to create an innovative custom made approach for the management of complex entero-atmospheric fistulas. Sci. Rep. 2020, 10, 19862. [Google Scholar] [CrossRef]
- Waldecker, M.; Leckel, M.; Rammelsberg, P.; Bömicke, W. Fully digital fabrication of an occlusal device using an intraoral scanner and 3D printing: A dental technique. J. Prosthet. Dent. 2019, 121, 576–580. [Google Scholar] [CrossRef] [PubMed]
- Shujaat, S.; Bornstein, M.M.; Price, J.B.; Jacobs, R. Integration of imaging modalities in digital dental workflows—Possibilities, limitations, and potential future developments. Dentomaxillofacial Radiol. 2021, 50, 20210268. [Google Scholar] [CrossRef]
- Khalil, W.; Ezeldeen, M.; Van De Casteele, E.; Shaheen, E.; Sun, Y.; Shahbazian, M.; Olszewski, R.; Politis, C.; Jacobs, R. Validation of cone beam computed tomography-based tooth printing using different three-dimensional printing technologies. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, 307–315. [Google Scholar] [CrossRef]
- Zhang, H.-R.; Yin, L.-F.; Liu, Y.-L.; Yan, L.-Y.; Wang, N.; Liu, G.; An, X.-L.; Liu, B. Fabrication and accuracy research on 3D printing dental model based on cone beam computed tomography digital modeling. West China J. Stomatol. 2018, 36, 156–161. [Google Scholar] [CrossRef]
- Holberg, C.; Steinhäuser, S.; Geis, P.; Rudzki-Janson, I. Cone-Beam Computed Tomography in Orthodontics: Benefits and Limitations. J. Orofac. Orthop. Fortschr. Der Kieferorthopädie 2005, 66, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Bal, M.; Spies, L. Metal artifact reduction in CT using tissue-class modeling and adaptive prefiltering. Med Phys. 2006, 33, 2852–2859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, J.; Molthen, R.C.; Dawson, C.A.; Johnson, R.H. An iterative approach to the beam hardening correction in cone beam CT. Med. Phys. 2000, 27, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verburg, J.M.; Seco, J. CT metal artifact reduction method correcting for beam hardening and missing projections. Phys. Med. Biol. 2012, 57, 2803–2818. [Google Scholar] [CrossRef] [PubMed]
- Yan, C.H.; Whalen, R.; Beaupre, G.; Yen, S.; Napel, S. Reconstruction algorithm for polychromatic CT imaging: Application to beam hardening correction. IEEE Trans. Med Imaging 2000, 19, 1–11. [Google Scholar] [CrossRef]
- Sugawara, H.; Takayanagi, T.; Ishikawa, T.; Katada, Y.; Fukui, R.; Yamamoto, Y.; Suzuki, S. New Fast kVp Switching Dual-Energy CT: Reduced Severity of Beam Hardening Artifacts and Improved Image Quality in Reduced-Iodine Virtual Monochromatic Imaging. Acad. Radiol. 2019, 27, 1586–1593. [Google Scholar] [CrossRef]
- Katsura, M.; Sato, J.; Akahane, M.; Kunimatsu, A.; Abe, O. Current and Novel Techniques for Metal Artifact Reduction at CT: Practical Guide for Radiologists. RadioGraphics 2018, 38, 450–461. [Google Scholar] [CrossRef] [Green Version]
- Barbin, T.; Veloso, D.V.; Del Rio Silva, L.; Borges, G.A.; Presotto, A.G.C.; Barao, V.A.R.; Mesquita, M.F. 3D metal printing in dentistry: An in vitro biomechanical comparative study of two additive manufacturing technologies for full-arch implant-supported prostheses. J. Mech. Behav. Biomed. Mater. 2020, 108, 103821. [Google Scholar] [CrossRef]
- Keßler, A.; Dosch, M.; Reymus, M.; Folwaczny, M. Influence of 3D- printing method, resin material, and sterilization on the accuracy of virtually designed surgical implant guides. J. Prosthet. Dent. 2021, in press. [Google Scholar] [CrossRef]
- Okolie, O.; Stachurek, I.; Kandasubramanian, B.; Njuguna, J. 3D Printing for Hip Implant Applications: A Review. Polymers 2020, 12, 2682. [Google Scholar] [CrossRef] [PubMed]
- Kjellberg, M.; Al-Amiry, B.; Englund, E.; Sjödén, G.O.; Sayed-Noor, A.S. Measurement of leg length discrepancy after total hip arthroplasty. The reliability of a plain radiographic method compared to CT-scanogram. Skelet. Radiol. 2012, 41, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Lee, F.C.C.; Noar, J.H.; Evans, R.D. Evaluation of the CT scanogram for assessment of craniofacial morphology. Angle Orthod. 2011, 81, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.C.; Jones, A.; Kambhampati, S.; Gilotra, M.N.; Liacouras, P.C.; Stuelke, S.; Shiu, B.; Leong, N.; Hasan, S.A.; Siegel, E.L. CT-Based 3D Printing of the Glenoid Prior to Shoulder Arthroplasty: Bony Morphology and Model Evaluation. J. Digit. Imaging 2019, 32, 816–826. [Google Scholar] [CrossRef]
- Obasare, E.; Mainigi, S.K.; Morris, D.L.; Slipczuk, L.; Goykhman, I.; Friend, E.; Ziccardi, M.R.; Pressman, G.S. CT based 3D printing is superior to transesophageal echocardiography for pre-procedure planning in left atrial appendage device closure. Int. J. Cardiovasc. Imaging 2018, 34, 821–831. [Google Scholar] [CrossRef]
- Ripley, B.; Kelil, T.; Cheezum, M.K.; Gonçalves, A.; Di Carli, M.F.; Rybicki, F.J.; Steigner, M.; Mitsouras, D.; Blankstein, R. 3D printing based on cardiac CT assists anatomic visualization prior to transcatheter aortic valve replacement. J. Cardiovasc. Comput. Tomogr. 2015, 10, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Weidenmaier, W.; Christ, G. The effect of beam hardening on CT values. Rofo 1985, 143, 697–701. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 80 kVp 50 mAs | 100 kVp 50 mAs | 120 kVp 50 mAs | ||||
|---|---|---|---|---|---|---|
| Inner Area | Outer Area | Inner Area | Outer Area | Inner Area | Outer Area | |
| iMAR | −501.20 ± 369.24 | −720.80 ± 631.69 | −434.11 ± 432.70 | −704.18 ± 318.15 | −438.65 ± 344.62 | −575.63 ± 425.25 |
| non iMAR | −76.92 ± 631.69 | −5.099 ± 829.2 | −98.083 ± 457.227 | −120.738 ± 669.435 | −298.416 ± 288.370 | −278.274 ± 461.582 |
| 120 kVp 30 mAs | 120 kVp 50 mAs | 120 kVp 80 mAs | ||||
|---|---|---|---|---|---|---|
| Inner Area | Outer Area | Inner Area | Outer Area | Inner Area | Outer Area | |
| iMAR | −448.98 ± 347.59 | −597.77 ± 411.40 | −438.65 ± 344.62 | −575.63± 425.25 | −438.66 ± 344.70 | −668.73± 374.19 |
| non iMAR | −310.52 ± 298.20 | −271.21 ± 514.26 | −298.42± 288.37 | −278.27 ± 461.58 | −266.78 ± 288.31 | −280.73± 487.60 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, Y.; Yu, S.-M. 3D Printing of Tooth Impressions Based on Multi-Detector Computed Tomography Images Combined with Beam Hardening Artifact Reduction in Metal Structures. Appl. Sci. 2022, 12, 3339. https://doi.org/10.3390/app12073339
Park Y, Yu S-M. 3D Printing of Tooth Impressions Based on Multi-Detector Computed Tomography Images Combined with Beam Hardening Artifact Reduction in Metal Structures. Applied Sciences. 2022; 12(7):3339. https://doi.org/10.3390/app12073339
Chicago/Turabian StylePark, Yeon, and Seung-Man Yu. 2022. "3D Printing of Tooth Impressions Based on Multi-Detector Computed Tomography Images Combined with Beam Hardening Artifact Reduction in Metal Structures" Applied Sciences 12, no. 7: 3339. https://doi.org/10.3390/app12073339