
Raman Spectroscopy of Individual Cervical Exfoliated Cells in Premalignant and Malignant Lesions

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cervical Sample Collection
2.2. Sample Preparation
2.3. Data Analysis
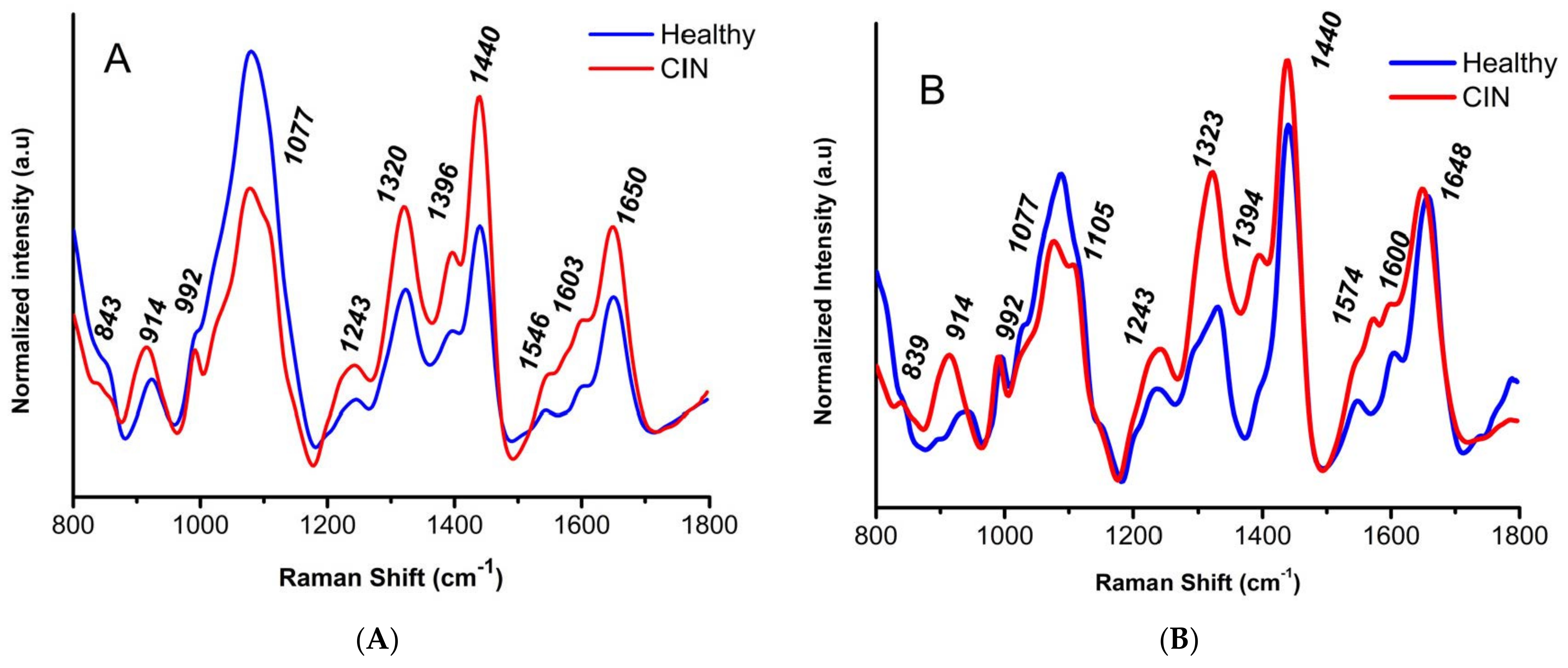
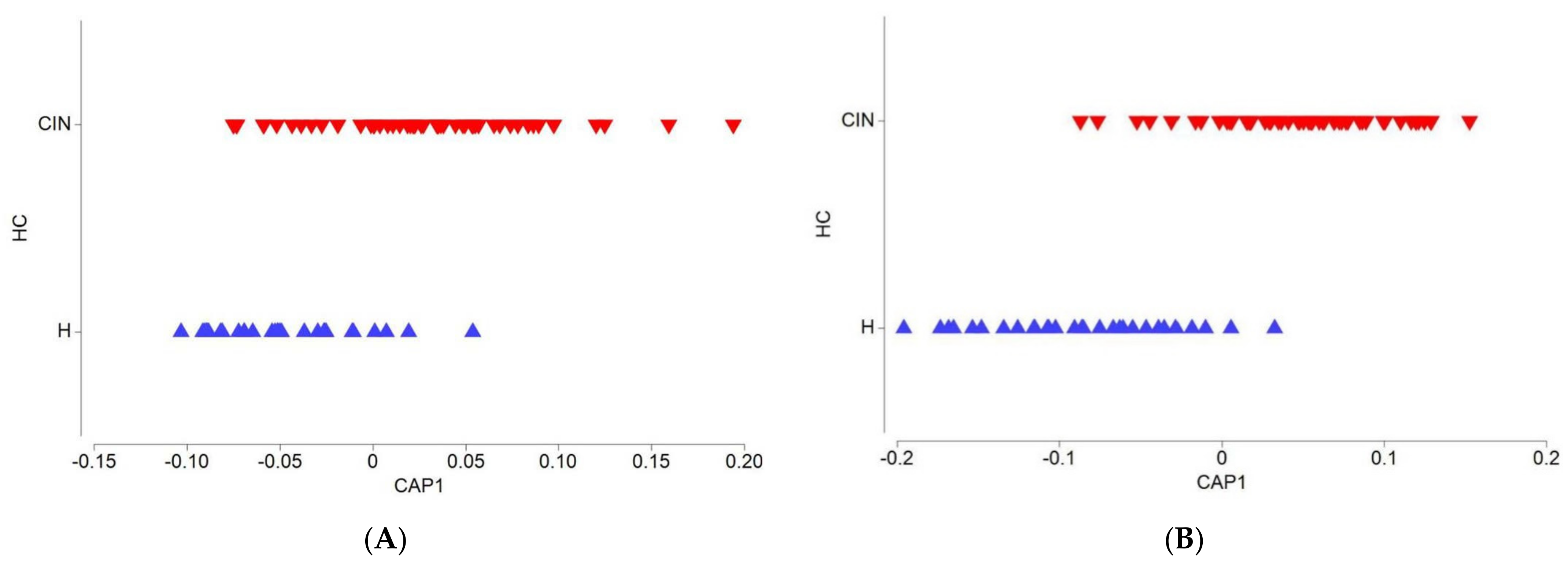
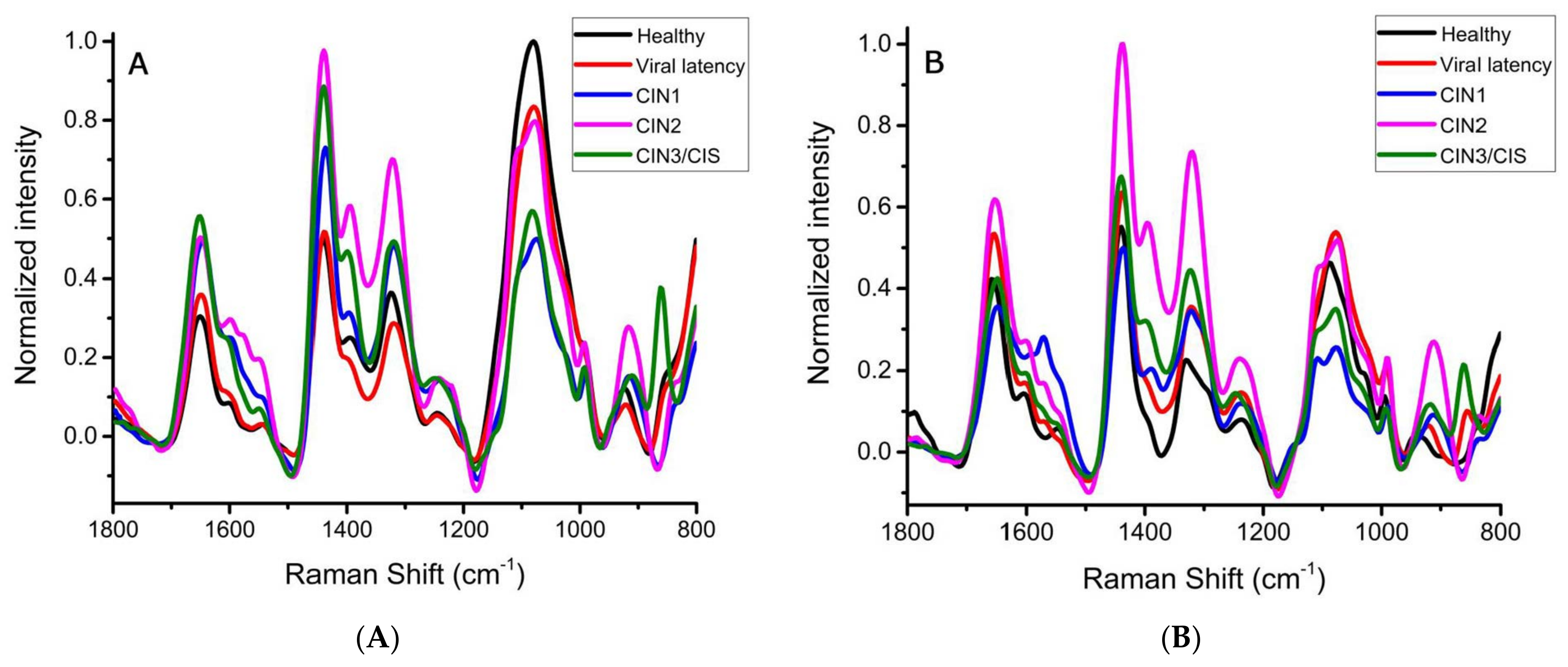
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Technical Guidance and Specifications of Medical Devices for Screening and Treatment of Precancerous Lesions in the Prevention of Cervical Cancer. 2020. Available online: https://www.who.int/publications-detail/9789240002630 (accessed on 5 February 2020).
- Bhatla, N.; Singhal, S. Primary HPV screening for cervical cancer. Best Pract. Res. Clin. Obs. Gynaecol. 2020, 65, 98–108. [Google Scholar] [CrossRef]
- Pan American Health Organization. Plan of Action for Cervical Cancer. Prevention and Control 2018–2030. 2018. Available online: https://www.paho.org/en/documents/plan-action-cervical-cancer-prevention-and-control-2018-2030 (accessed on 20 February 2020).
- Wuerthner, B.A.; Avila-Wallace, M. Cervical cancer: Screening, management, and prevention. Nurse Pract. 2016, 41, 18–23. [Google Scholar] [CrossRef]
- Ramos, I.R.; Meade, A.D.; Ibrahim, O.; Byrne, H.J.; McMenamin, M.; McKenna, M.; Malkin, A.; Lyng, F.M. Raman spectroscopy for cytopathology of exfoliated cervical cells. Faraday Discuss. 2016, 187, 187–198. [Google Scholar] [CrossRef] [Green Version]
- Gravitt, P.E.; Peyton, C.L.; Alessi, T.Q.; Wheeler, C.M.; Coutlée, F.; Hildesheim, A.; Schiffman, M.H.; Scott, D.R.; Apple, R.J. Improved Amplification of Genital Human Papillomaviruses. J. Clin. Microbiol. 2000, 38, 357–361. [Google Scholar] [CrossRef]
- Sichero, L.; Picconi, M.A.; Villa, L.L. The contribution of Latin American research to HPV epidemiology and natural history knowledge. Braz. J. Med. Biol. Res. 2020, 53, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Gustavsson, I.; Aarnio, R.; Myrnäs, M.; Hedlund-Lindberg, J.; Taku, O.; Meiring, T.; Wikström, I.; Enroth, S.; Williamson, A.-L.; Olovsson, M.; et al. Clinical validation of the HPVIR high-risk HPV test on cervical samples according to the international guidelines for human papillomavirus DNA test requirements for cervical cancer screening. Virol. J. 2019, 16, 107. [Google Scholar] [CrossRef] [Green Version]
- Wai, K.C.; Strohl, M.P.; Van Zante, A.; Ha, P.K. Molecular diagnostics in human papillomavirus-related head and neck squamous cell carcinoma. Cells 2020, 9, 500. [Google Scholar] [CrossRef] [Green Version]
- Cibas, E.S. Cervical, and Vaginal Cytology. In Cytology Diagnostic Principles and Clinical Correlates; Elsevier: Amsterdam, The Netherlands, 2009; Chapter 1; pp. 1–57. [Google Scholar]
- Bhatla, N.; Singhal, S.; Saraiya, U.; Srivastava, S.; Bhalerao, S.; Shamsunder, S.; Chavan, N.; Basu, P.; Purandare, C.N. Screening and management of preinvasive lesions of the cervix: Good clinical practice recommendations from the Federation of Obstetric and Gynecologic Societies of India (FOGSI). J. Obstet. Gynaecol. Res. 2020, 46, 201–214. [Google Scholar] [CrossRef]
- Auner, G.W.; Koya, S.K.; Huang, C.; Broadbent, B.; Trexler, M.; Auner, Z.; Elias, A.; Mehne, K.C.; Brusatori, M.A. Applications of Raman spectroscopy in cancer diagnosis. Cancer Metastasis Rev. 2018, 37, 691–717. [Google Scholar] [CrossRef] [Green Version]
- Lyng, F.M.; Traynor, D.; Ramos, I.R.M.; Bonnier, F.; Byrne, H.J. Raman spectroscopy for screening and diagnosis of cervical cancer. Anal. Bioanal. Chem. 2015, 407, 8279–8289. [Google Scholar] [CrossRef] [Green Version]
- Novikova, T. Optical techniques for cervical neoplasia detection. Beilstein J. Nanotechnol. 2017, 8, 1844–1862. [Google Scholar] [CrossRef] [Green Version]
- Keller, M.; Kanter, E.M.; Lieber, C.A.; Majumder, S.K.; Hutchings, J.; Ellis, D.L.; Beaven, R.B.; Stone, N.; Mahadevan-Jansen, A. Detecting temporal and spatial effects of epithelial cancers with Raman spectroscopy. Dis. Markers 2008, 25, 323–337. [Google Scholar] [CrossRef] [Green Version]
- Rubina, S.; Krishna, C.M. Raman spectroscopy in cervical cancers: An update. J. Cancer Res. Ther. 2015, 11, 10–17. [Google Scholar]
- Ostrowska, K.M.; Malkin, A.; Meade, A.; O’Leary, J.; Martin, C.; Spillane, C.; Byrne, H.J.; Lyng, F.M. Investigation of the influence of high-risk human papillomavirus on the biochemical composition of cervical cancer cells using vibrational spectroscopy. Analyst 2010, 135, 3087–3093. [Google Scholar] [CrossRef] [Green Version]
- Rubina, S.; Amita, M.; Kedar, K.D.; Bharat, R.; Krishna, C.M. Raman spectroscopy study on the classification of cervical cell specimens. Vib. Spectrosc. 2013, 68, 115–121. [Google Scholar] [CrossRef]
- Kearney, P. Raman spectral signatures of cervical exfoliated cells from liquid-based cytology samples. J. Biomed. Opt. 2017, 22, 105008. [Google Scholar] [CrossRef] [Green Version]
- Sitarz, K.; Czamara, K.; Bialecka, J.; Klimek, M.; Zawilinska, B.; Szostek, S.; Kaczor, A. HPV Infection Significantly Accelerates Glycogen Metabolism in Cervical Cells with Large Nuclei: Raman Microscopic Study with Subcellular Resolution. Int. J. Mol. Sci. 2020, 21, 2667. [Google Scholar] [CrossRef]
- Traynor, D.; Martin, C.; White, C.; Reynolds, S.; D’Arcy, T.; O’Leary, J.; Lyng, F. Raman Spectroscopy of Liquid-Based Cervical Smear Samples as a Triage to Stratify Women Who Are HPV-Positive on Screening. Cancers 2021, 13, 2008. [Google Scholar] [CrossRef]
- Wang, J.; Zheng, C.-X.; Ma, C.-L.; Zheng, X.-X.; Lv, X.-Y.; Lv, G.-D.; Tang, J.; Wu, G.-H. Raman spectroscopic study of cervical precancerous lesions and cervical cancer. Lasers Med. Sci. 2021, 36, 1855–1864. [Google Scholar] [CrossRef]
- Ceja-Fdez, A.; Carriles, R.; González-Yebra, A.L.; Vivero-Escoto, J.; de la Rosa, E.; López-Luke, T. Imaging and SERS Study of the Au Nanoparticles Interaction with HPV and Carcinogenic Cervical Tissues. Molecules 2021, 26, 3758. [Google Scholar] [CrossRef]
- Karunakaran, V.; Saritha, V.N.; Joseph, M.M.; Nair, J.B.; Saranya, G.; Raghu, K.G.; Sujathan, K.; Kumar, K.S.; Maiti, K.K. Diagnostic spectro-cytology revealing differential recognition of cervical cancer lesions by label-free surface enhanced Raman fingerprints and chemometrics. Nanomedicine 2020, 29, 102276. [Google Scholar] [CrossRef]
- Karunakaran, V.; Saritha, V.N.; Ramya, A.N.; Murali, V.P.; Raghu, K.G.; Sujathan, K.; Maiti, K.K. Elucidating Raman Image-Guided Differential Recognition of Clinically Confirmed Grades of Cervical Exfoliated Cells by Dual Biomarker-Appended SERS-Tag. Anal. Chem. 2021, 93, 11140–11150. [Google Scholar] [CrossRef]
- Traynor, D.; Duraipandian, S.; Martin, C.M.; O’Leary, J.J.; Lyng, F.M. Improved removal of blood contamination from ThinPrep cervical cytology samples for Raman spectroscopic analysis. J. Biomed. Opt. 2018, 23, 055001. [Google Scholar] [CrossRef]
- Behl, I.; Calado, G.; Ibrahim, O.; Malkin, A.; Flint, S.; Byrne, H.J.; Lyng, F.M. Development of methodology for Raman microspectroscopic analysis of oral exfoliated cells. Anal. Methods 2017, 9, 937–948. [Google Scholar] [CrossRef] [Green Version]
- Ramos, I.R.; Malkin, A.; Lyng, F.M. Current advances in the application of Raman spectroscopy for molecular diagnosis of cervical cancer. Biomed. Res. Int. 2015, 1–9. [Google Scholar] [CrossRef]
- Movasaghi, Z.; Rehman, S.; Rehman, I. Raman Spectroscopy of Biological Tissues. Appl. Spectrosc. Rev. 2007, 42, 493–541. [Google Scholar] [CrossRef]
- De Gelder, J.; De Gussem, K.; Vandenabeele, P.; Moens, L. Reference database of Raman spectra of biological molecules. J. Raman Spectrosc. 2007, 38, 1133–1147. [Google Scholar] [CrossRef]
- Traynor, D.; Duraipandian, S.; Bhatia, R.; Cuschieri, K.; Martin, C.M.; O’Leary, J.; Lyng, F.M. The potential of biobanked liquid-based cytology samples for cervical cancer screening using Raman. J. Biophotonics 2019, 12, e201800377. [Google Scholar] [CrossRef] [Green Version]
- Alrajjal, A.; Pansare, V.; Choudhury, M.S.R.; Khan, M.Y.A.; Shidham, V.B. Squamous intraepithelial lesions (SIL: LSIL, HSIL, ASCUS, ASC-H, LSIL-H) of uterine cervix and Bethesda system. CytoJournal 2021, 18, 16. [Google Scholar] [CrossRef]
- Da Rosa, M.I.; Medeiros, L.R.; Rosa, D.D.; Bozzeti, M.C.; Silva, F.R.; Silva, B.R. Human papillomavirus and cervical neoplasia. Cad. Saude Publica. 2009, 25, 953–964. [Google Scholar] [CrossRef] [Green Version]
- Mougin, C.; Dalstein, V.; Prétet, J.L.; Gay, C.; Schaal, J.P.; Riethmuller, D. Epidemiology of cervical papillomavirus infections. Recent knowledge. Presse Med. 2001, 30, 1017–1023. [Google Scholar] [PubMed]
- McMurray, H.R.; Nguyen, D.; Westbrook, T.F.; McAnce, D.J. Biology of human papillomavirus. J. Exp. Path 2001, 82, 15–33. [Google Scholar] [CrossRef] [PubMed]
- Vashisht, S.; Mishra, H.; Mishra, P.K.; Ekielski, A.; Talegaonkar, S. Structure, genome, infection cycle, and clinical manifestations associated with human papillomavirus. Curr. Pharm. Biotechnol. 2019, 20, 1260–1280. [Google Scholar] [CrossRef] [PubMed]
- Graham, S. The human papillomavirus replication cycle, and its links progression: A comprehensive review. Clin. Sci. 2017, 131, 2201–2221. [Google Scholar] [CrossRef] [Green Version]
- Harden, M.E.; Munger, K. Human papillomavirus molecular biology. Mutat. Res. Rev. Mutat. Res. 2017, 772, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Woolford, L.; Chen, M.; Dholakia, K.; Herrington, C.S. Towards automated cancer screening: Label-free classification of fixed cell samples using wavelength modulated Raman spectroscopy. J. Biophotonics 2018, 11, e201700244. [Google Scholar] [CrossRef] [Green Version]
- Zheng, C.; Qing, S.; Wang, J.; Lü, G.; Li, H.; Lü, X.; Ma, C.; Tang, J.; Yue, X. Diagnosis of cervical squamous cell carcinoma and cervical adenocarcinoma based on Raman spectroscopy and support vector machine. Photodiagnosis Photodyn. Ther. 2019, 27, 156–161. [Google Scholar] [CrossRef]
- Krishna, C.M.; Sockalingum, G.D.; Vadhiraja, B.M.; Maheedhar, K.; Rao, A.C.K.; Rao, L.; Ventéo, L.; Pluot, M.; Fernandes, D.J.; Vidyasagar, M.S.; et al. Vibrational spectroscopy studies of formalin-fixed cervix tissues. Biopolymers 2007, 85, 214–221. [Google Scholar] [CrossRef]
- Rubina, S.; Vidyasagar, M.S.; Murali Krishna, C. Raman Spectroscopic Study on prediction of treatment response in cervical cancers. J. Innov. Opt. Health Sci. 2013, 6, 1350014. [Google Scholar] [CrossRef]
- Shaikh, R.; Prabitha, V.G.; Dora, T.K.; Chopra, S.; Maheshwari, A.; Deodhar, K.; Rekhi, B.; Sukumar, N.; Krishna, C.M.; Subhash, N. A comparative evaluation of diffuse reflectance and Raman spectroscopy in the detection of cervical cancer. J. Biophotonics 2017, 10, 242–252. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Band (cm−1) C/N * | Raman Assignment | Increased Band Intensity in CIN Patients | Contributing Band at 50% of Statistical Significance | ||
|---|---|---|---|---|---|
| Cytoplasm * C | Nucleus * N | Cytoplasm | Nucleus | ||
| 843/839 | Deformative vibrations of amine groups/Polysaccharide structure | X | X | ||
| 861 | Phosphate group | X | X | X | |
| 914/914 | Proteins and lipids stretching, ribose vibration | X | X | ||
| 917 | C-C proline and valine stretching | X | X | ||
| 934 | C-C collagen skeleton | X | X | ||
| 942 | C-C stretching mode of proline and valine and protein backbone (alpha-hélix conformation)/glycogen | X | |||
| 951 | Stretching (CH3) of proteins (alpha helix) | X | |||
| 980 | C-C stretching β-sheet (proteins), =CH bending (lipids) | X | X | ||
| 992/992 | C-O ribose, C-C | X | |||
| 997 | C-O ribose, C-C | X | |||
| 1037 | Collagen | X | X | ||
| 1063 | C-C lipid skeleton stretching | X | X | ||
| 1077/1077 | symmetric PO2-stretching of DNA | X | |||
| 1080 | Phospholipids, phosphodiester nucleic acid groups, collagen | X | X | X | |
| 1085 | Nucleic acid phosphodiester groups | X | X | ||
| 1108/1105 | Cytosine, carbohydrates peak for solutions | X | X | X | |
| 1150 | C-C and C-N proteins and lipids stretching, glycogen | X | X | ||
| 1184 | Cytosine, adenine, guanine | X | |||
| 1209 | C-C6H5 tryptophan and phenylalanine stretching | X | X | ||
| 1234 | Guanine, amide III | X | X | ||
| 1243/1243 | NH2 guanine and cytosine, amide III. Asymmetric phosphate stretching modes | X | X | ||
| 1295 | CH2 deformation | X | X | ||
| 1311 | CH3 and/or CH2 collagen and lipids twisting | X | X | ||
| 1320/1323 | Guanine (RNA/DNA), CH in protein and carbohydrates | X | X | X | X |
| 1355 | Guanine | X | X | ||
| 1377 | T, A, G (DNA/RNA ring mode) | X | X | ||
| 1396/1394 | C=O symmetric stretching, CH2 deformation | X | X | X | |
| 1440/1440 | CH2 proteins and lipid bending | X | X | X | |
| 1445 | CH2 proteins and lipids bending | X | |||
| 1546/1574 | Amide II, nucleic acid modes, ring breathing modes in DNA bases | X | X | X | X |
| 1603/1600 | Adenine, guanine (RNA/DNA), C=C phenylalanine bending, amide I C=O stretching | X | X | X | X |
| 1608 | C=C phenylalanine and tyrosine | X | X | X | |
| 1650/1648 | Amide I (C=O stretching, C-N stretching and N-H proteins bending) | X | |||
| 1655 | Amide I collagen and protein | X | X | ||
| Group | Healthy | CIN | Total | Raman Classification Score % | |
|---|---|---|---|---|---|
| Cytoplasm | Healthy | 23 | 6 | 29 | 79.3 |
| CIN | 13 | 39 | 52 | 75.0 | |
| Overall classification efficiency 62/81 76.5% | |||||
| Incorrect classification 23.5% | |||||
| Nucleus | Healthy | 23 | 6 | 29 | 79.3 |
| CIN | 8 | 44 | 52 | 84.6 | |
| Overall classification efficiency 67/81 82.7% | |||||
| Incorrect classification 17.3% | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva-López, M.S.; Ilizaliturri Hernández, C.A.; Navarro Contreras, H.R.; Rodríguez Vázquez, Á.G.; Ortiz-Dosal, A.; Kolosovas-Machuca, E.S. Raman Spectroscopy of Individual Cervical Exfoliated Cells in Premalignant and Malignant Lesions. Appl. Sci. 2022, 12, 2419. https://doi.org/10.3390/app12052419
Silva-López MS, Ilizaliturri Hernández CA, Navarro Contreras HR, Rodríguez Vázquez ÁG, Ortiz-Dosal A, Kolosovas-Machuca ES. Raman Spectroscopy of Individual Cervical Exfoliated Cells in Premalignant and Malignant Lesions. Applied Sciences. 2022; 12(5):2419. https://doi.org/10.3390/app12052419
Chicago/Turabian StyleSilva-López, Mariana Sarai, César Arturo Ilizaliturri Hernández, Hugo Ricardo Navarro Contreras, Ángel Gabriel Rodríguez Vázquez, Alejandra Ortiz-Dosal, and Eleazar Samuel Kolosovas-Machuca. 2022. "Raman Spectroscopy of Individual Cervical Exfoliated Cells in Premalignant and Malignant Lesions" Applied Sciences 12, no. 5: 2419. https://doi.org/10.3390/app12052419