
Untargeted 1H-NMR Urine Metabolomic Analysis of Preterm Infants with Neonatal Sepsis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethical Statement
2.3. NMR Sample Preparation
2.4. NMR Experiments
2.5. Data Processing
2.6. Statistical Analysis of NMR Data
2.7. Pathway Analysis and Visualization
3. Results
3.1. Metabolic Profile Alterations of Preterms with EOS
3.1.1. EOS Preterms versus Non NICU Healthy Preterms
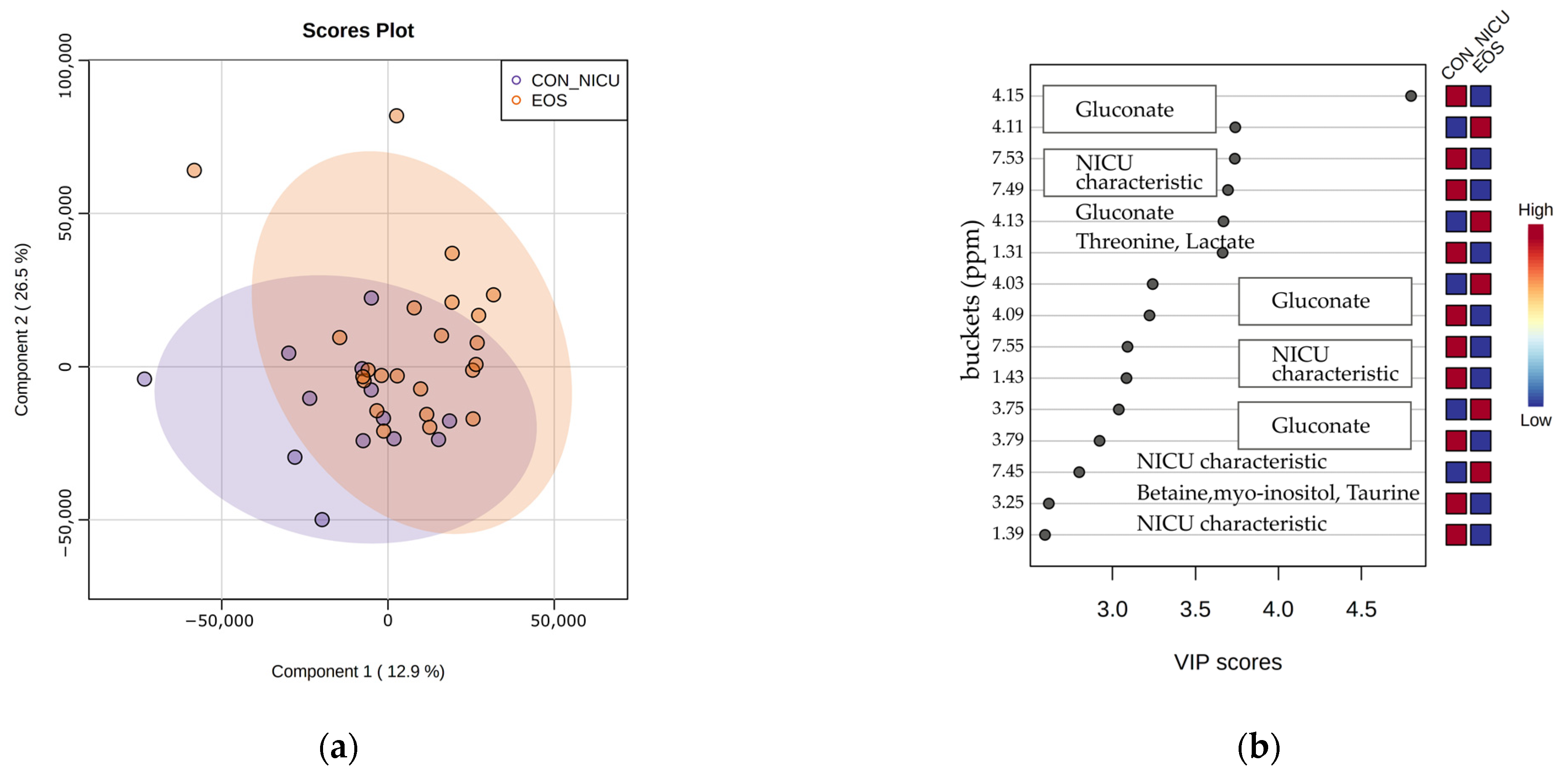
3.1.2. EOS Preterms Versus NICU Control Preterms
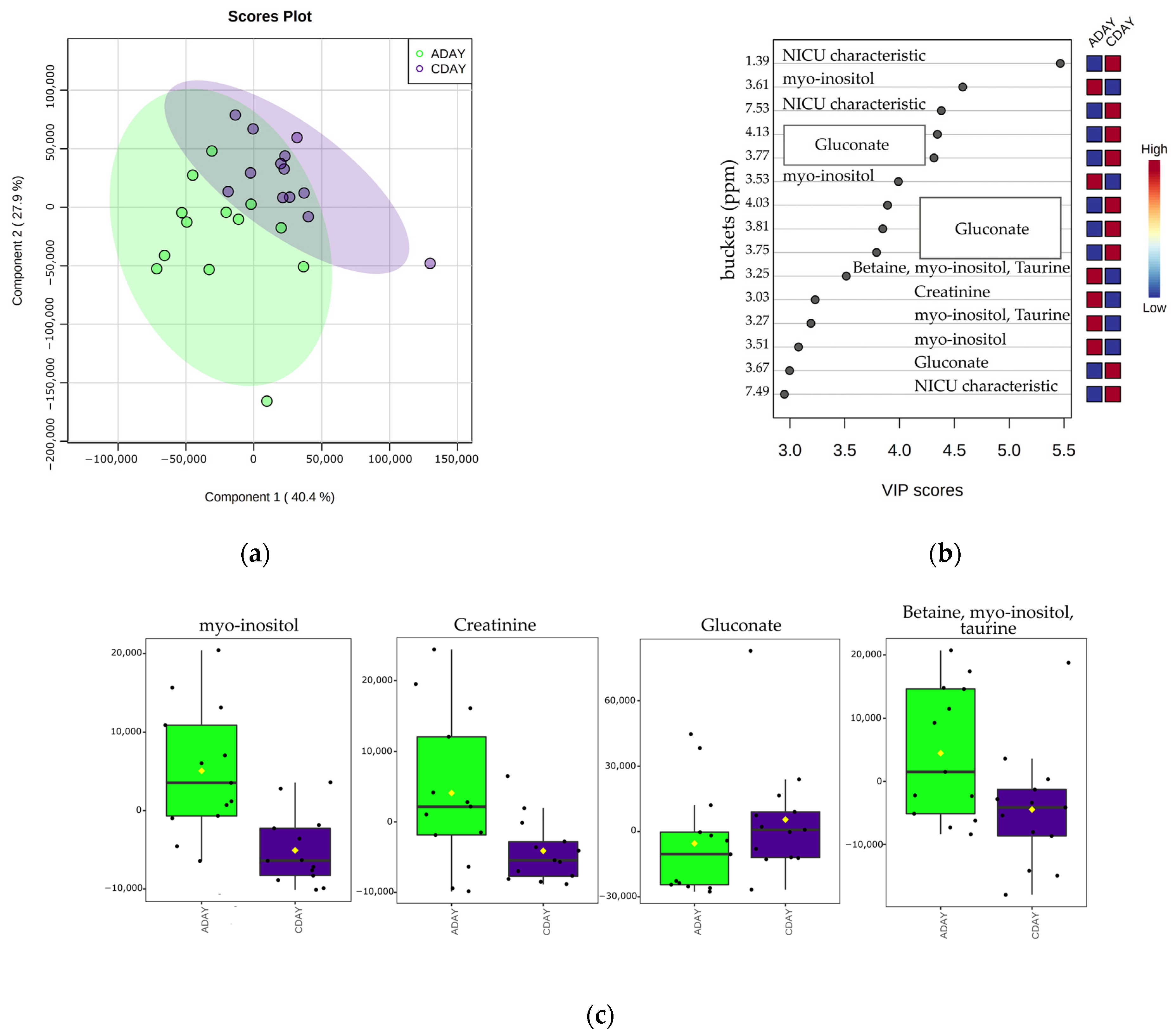
3.1.3. EOS Metabolic Profile Progression between First and Third Day of Life
3.2. Metabolic Profile Alterations of Preterms with LOS
3.2.1. LOS Preterms versus Non NICU Healthy Preterms
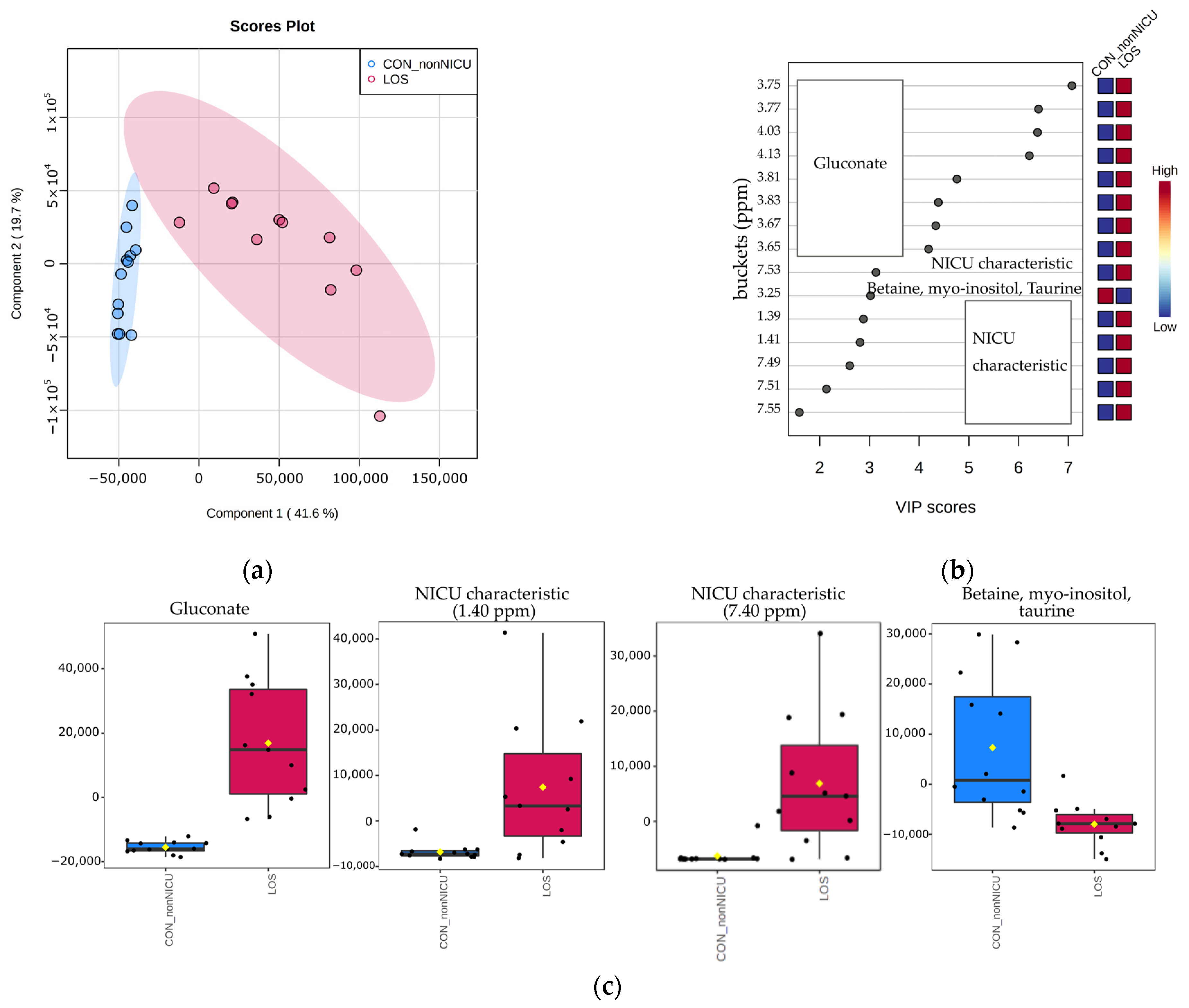
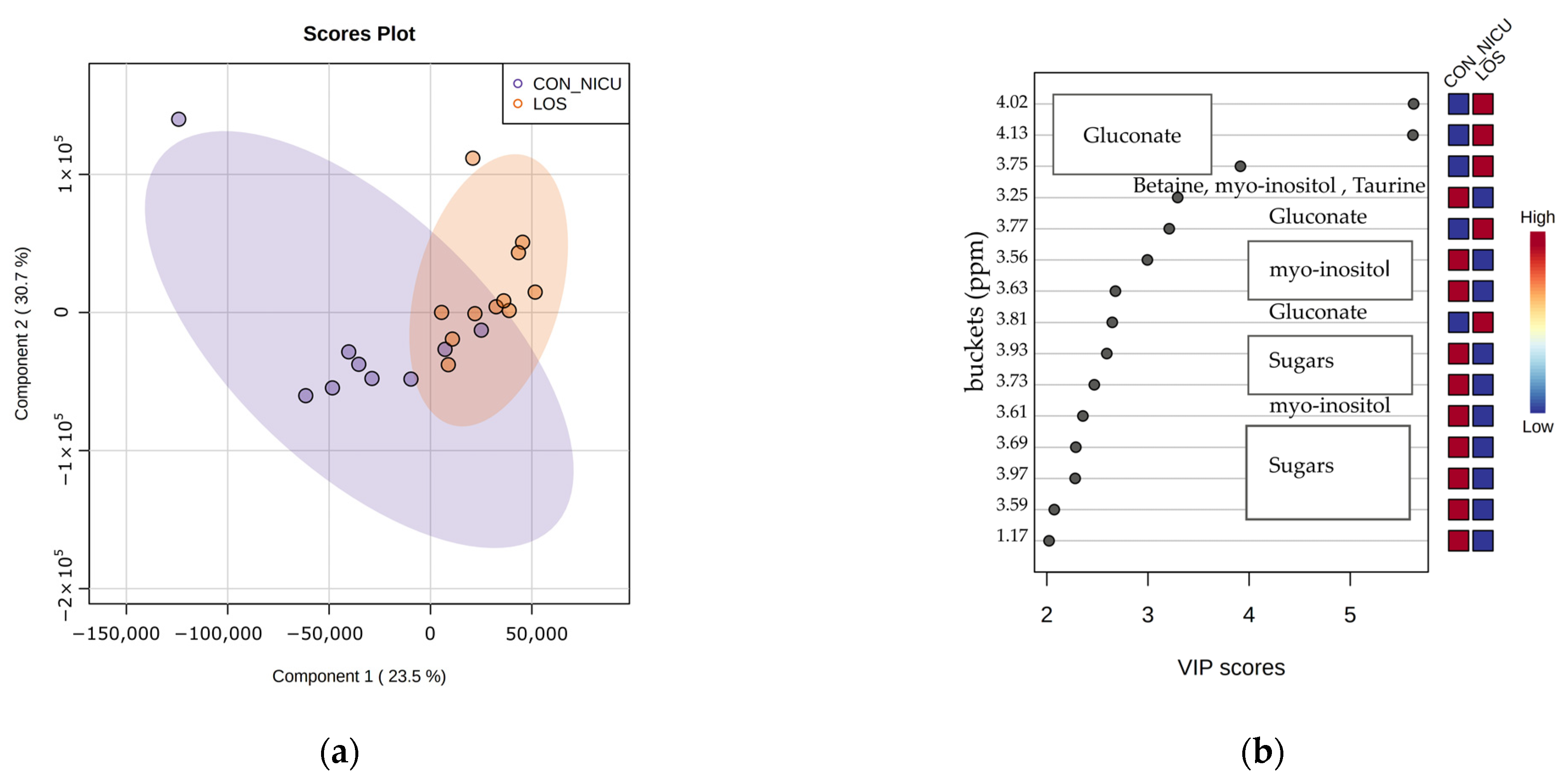
3.2.2. LOS Preterms Versus NICU Control Preterms
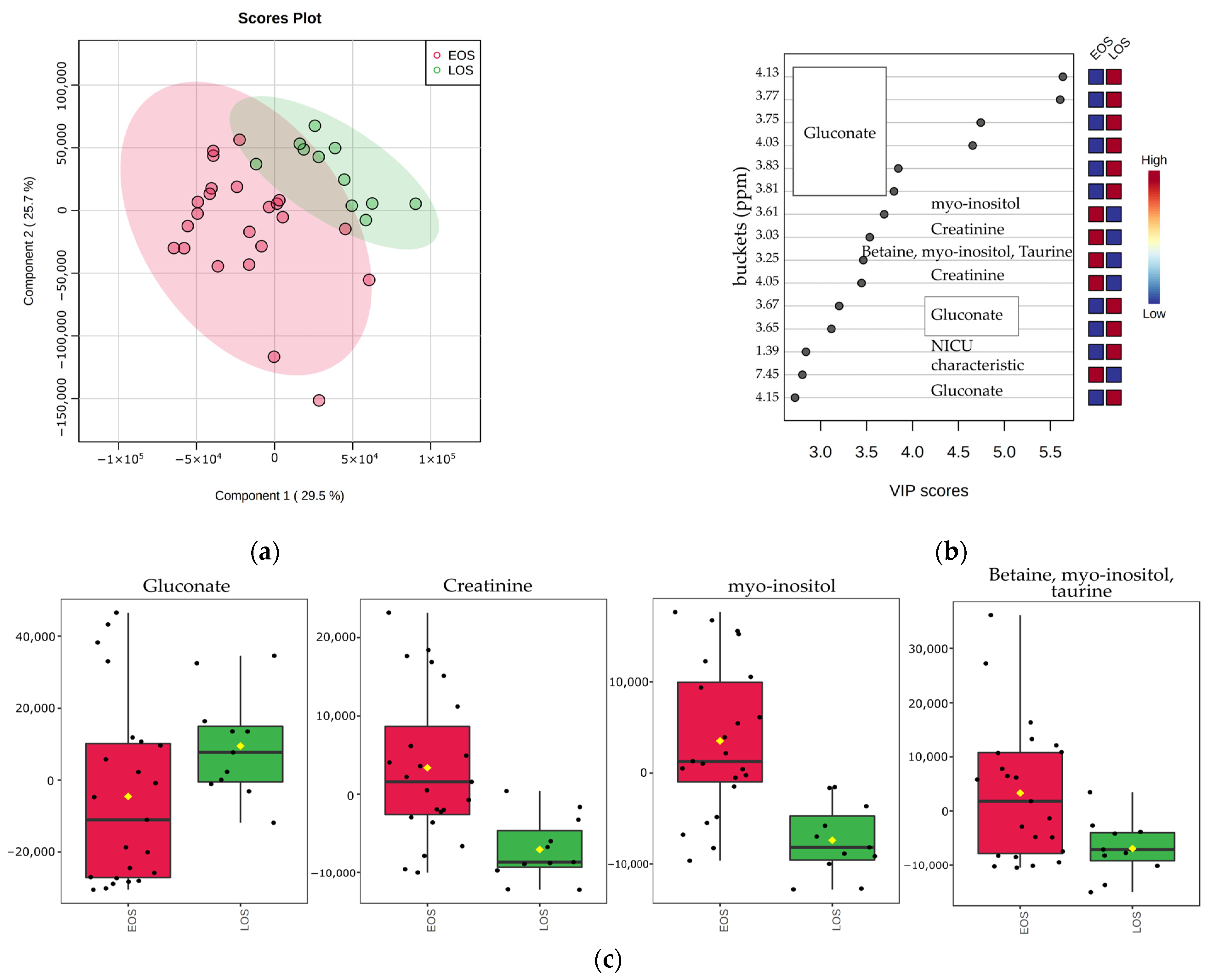
3.3. Metabolic Profile Alterations between EOS and LOS Neonates
3.4. Univariate Statistical Analysis
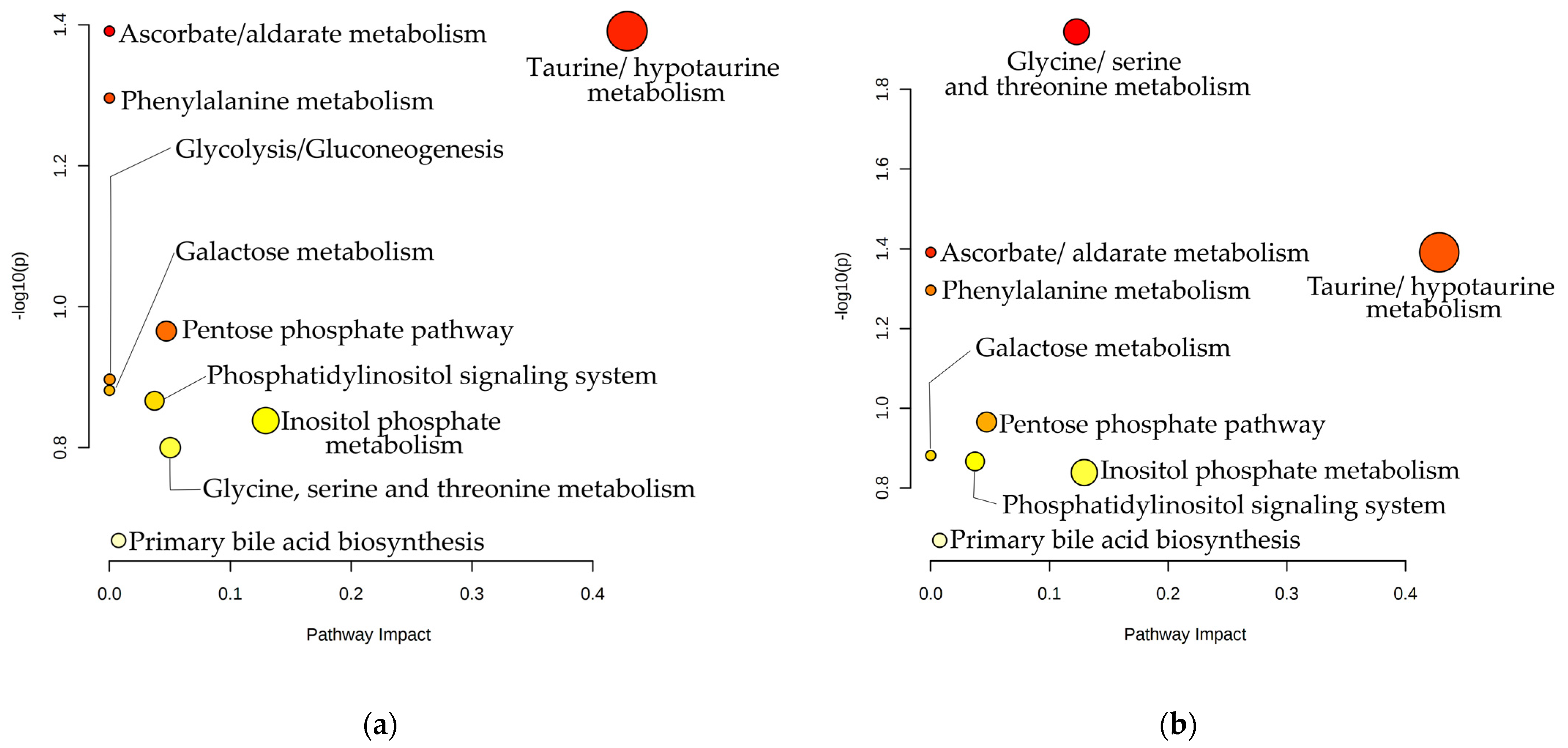
3.5. Pathway Analysis
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shane, A.L.; Sánchez, P.J.; Stoll, B.J. Neonatal Sepsis. Lancet 2017, 390, 1770–1780. [Google Scholar] [CrossRef]
- Vergnano, S.; Sharland, M.; Kazembe, P.; Mwansambo, C.; Heath, P.T. Neonatal Sepsis: An International Perspective. Arch. Dis. Child. Fetal Neonatal Ed. 2005, 90, 220–224. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Report on the Epidemiology and Burden of Sepsis: Current Evidence, Identifying Gaps and Future Directions; World Health Organization: Geneva, Switzerland, 2020; ISBN 9789240010789.
- Fanaroff, A.A.; Wright, L.L.; Stevenson, D.K.; Shankaran, S.; Donovan, E.P.; Ehrenkranz, R.A.; Younes, N.; Korones, S.B.; Stoll, B.J.; Tyson, J.E.; et al. Very-Low-Birth-Weight Outcomes of the National Institute of Child Health and Human Development Neonatal Research Network, May 1991 through December 1992. Am. J. Obstet. Gynecol. 1995, 173, 1423–1431. [Google Scholar] [CrossRef]
- Shah, G.S.; Budhathoki, S.; Das, B.K.; Mandal, R.N. Risk Factors in Early Neonatal Sepsis. Kathmandu Univ. Med. J. (KUMJ) 2006, 4, 187–191. [Google Scholar]
- Lim, W.H.; Lien, R.; Huang, Y.C.; Chiang, M.C.; Fu, R.H.; Chu, S.M.; Hsu, J.F.; Yang, P.H. Prevalence and Pathogen Distribution of Neonatal Sepsis among Very-Low-Birth-Weight Infants. Pediatrics Neonatol. 2012, 53, 228–234. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, R.G.; Kandefer, S.; Do, B.T.; Smith, P.B.; Stoll, B.J.; Bell, E.F.; Carlo, W.A.; Laptook, A.R.; Sánchez, P.J.; Shankaran, S.; et al. Late-Onset Sepsis in Extremely Premature Infants: 2000–2011. Pediatr. Infect. Dis. J. 2017, 36, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Ohlin, A.; Björkman, L.; Serenius, F.; Schollin, J.; Källén, K. Sepsis as a Risk Factor for Neonatal Morbidity in Extremely Preterm Infants. Acta Paediatr. Int. J. Paediatr. 2015, 104, 1070–1076. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Wolkowiez, M.; Moran, C.; Benjamin, D.K.; Cotten, C.M.; Clark, R.H.; Benjamin, D.K.; Smith, P.B. Early and Late Onset Sepsis in Late Preterm Infants. Pediatr. Infect. Dis. J. 2009, 28, 1052–1056. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.L.; Dorer, D.J.; Fleming, M.P.; Catlin, E.A. Clinical Outcomes of Near-Term Infants. Pediatrics 2004, 114, 372–376. [Google Scholar] [CrossRef]
- Tomashek, K.M.; Shapiro-Mendoza, C.K.; Davidoff, M.J.; Petrini, J.R. Differences in Mortality between Late-Preterm and Term Singleton Infants in the United States, 1995-2002. J. Pediatr. 2007, 151, 1995–2002. [Google Scholar] [CrossRef]
- Hornik, C.P.; Fort, P.; Clark, R.H.; Watt, K.; Benjamin, D.K.; Smith, P.B.; Manzoni, P.; Jacqz-Aigrain, E.; Kaguelidou, F.; Cohen-Wolkowiez, M. Early and Late Onset Sepsis in Very-Low-Birth-Weight Infants from a Large Group of Neonatal Intensive Care Units. Early Hum. Dev. 2012, 88, S69–S74. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention (CDC). Perinatal group B streptococcal disease after universal screening recommendations--United States 2003–2005. MMWR. Morb. Mortal. Wkly. Rep. 2007, 56, 701–705. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Trends in perinatal group B streptococcal disease—United States 2000–2006. MMWR. Morb. Mortal. Wkly. Rep. 2009, 58, 109–112. [Google Scholar]
- Dong, Y.; Speer, C.P. Late-Onset Neonatal Sepsis: Recent Developments. Arch. Dis. Child. Fetal Neonatal Ed. 2015, 100, F257–F263. [Google Scholar] [CrossRef] [Green Version]
- Bizzarro, M.J.; Raskind, C.; Baltimore, R.S.; Gallagher, P.G. Seventy-Five Years of Neonatal Sepsis at Yale: 1928–2003. Pediatrics 2005, 116, 595–602. [Google Scholar] [CrossRef]
- Leal, Y.A.; Álvarez-Nemegyei, J.; Velázquez, J.R.; Rosado-Quiab, U.; Diego-Rodríguez, N.; Paz-Baeza, E.; Dávila-Velázquez, J. Risk Factors and Prognosis for Neonatal Sepsis in Southeastern Mexico: Analysis of a Four-Year Historic Cohort Follow-Up. BMC Pregnancy Childbirth 2012, 12, 48. [Google Scholar] [CrossRef] [Green Version]
- Osrin, D.; Vergnano, S.; Costello, A.; Williams, L. Serious Bacterial Infections in Newborn Infants in Developing Countries. Curr. Opin. Infect. Dis. 2004, 17, 217–224. [Google Scholar] [CrossRef]
- Mukhopadhyay, S.; Puopolo, K.M. Risk Assessment in Neonatal Early Onset Sepsis. Semin. Perinatol. 2012, 36, 408–415. [Google Scholar] [CrossRef] [Green Version]
- Simonsen, K.A.; Anderson-Berry, A.L.; Delair, S.F.; Dele Davies, H. Early-Onset Neonatal Sepsis. Clin. Microbiol. Rev. 2014, 27, 21–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, L.; Li, P.; Pan, T.; Feng, X. Pathogens Responsible for Early-Onset Sepsis in Suzhou, China. Jpn. J. Infect. Dis. 2020, 73, 148–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itoh, K.; Aihara, H.; Takada, S.; Nishino, M.; Lee, Y.; Negishi, H.; Itoh, H. Clinicopathological Differences between Early-Onset and Late-Onset Sepsis and Pneumonia in Very Low Birth Weight Infants. Fetal Pediatr. Pathol. 1990, 10, 757–768. [Google Scholar] [CrossRef] [PubMed]
- Iroh Tam, P.Y.; Bendel, C.M. Diagnostics for Neonatal Sepsis: Current Approaches and Future Directions. Pediatr. Res. 2017, 82, 574–583. [Google Scholar] [CrossRef] [PubMed]
- Wynn, J.L. Defining Neonatal Sepsis. Curr. Opin. Pediatr. 2016, 28, 135–140. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.; Thakur, A.; Bhardwaj, C.; Kler, N.; Garg, P.; Singh, M.; Choudhury, S. Potential Biomarkers for Diagnosing Neonatal Sepsis. Curr. Med. Res. Pract. 2020, 10, 12–17. [Google Scholar] [CrossRef]
- Bingol, K. Recent Advances in Targeted and Untargeted Metabolomics by NMR and MS/NMR Methods. High-Throughput 2018, 7, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vignoli, A.; Ghini, V.; Meoni, G.; Licari, C.; Takis, P.G.; Tenori, L.; Turano, P.; Luchinat, C. High-Throughput Metabolomics by 1D NMR. Angew. Chem.-Int. Ed. 2019, 58, 968–994. [Google Scholar] [CrossRef]
- Sarafidis, K.; Chatziioannou, A.C.; Thomaidou, A.; Gika, H.; Mikros, E.; Benaki, D.; Diamanti, E.; Agakidis, C.; Raikos, N.; Drossou, V.; et al. Urine Metabolomics in Neonates with Late-Onset Sepsis in a Case-Control Study. Sci. Rep. 2017, 7, 45506. [Google Scholar] [CrossRef]
- Mardegan, V.; Giordano, G.; Stocchero, M.; Pirillo, P.; Poloniato, G.; Donadel, E.; Salvadori, S.; Giaquinto, C.; Priante, E.; Baraldi, E. Untargeted and Targeted Metabolomic Profiling of Preterm Newborns with Earlyonset Sepsis: A Case-Control Study. Metabolites 2021, 11, 115. [Google Scholar] [CrossRef]
- Fanos, V.; Caboni, P.; Corsello, G.; Stronati, M.; Gazzolo, D.; Noto, A.; Lussu, M.; Dessì, A.; Giuffrè, M.; Lacerenza, S.; et al. Urinary 1H-NMR and GC-MS Metabolomics Predicts Early and Late Onset Neonatal Sepsis. Early Hum. Dev. 2014, 90, 78–83. [Google Scholar] [CrossRef]
- Ludwig, C.; Viant, M.R. Two-Dimensional J-Resolved NMR Spectroscopy: Review of a Key Methodology in the Metabolomics Toolbox. Phytochem. Anal. 2010, 21, 22–32. [Google Scholar] [CrossRef]
- Huang, Y.; Yang, Y.; Cai, S.; Chen, Z.; Zhan, H.; Li, C.; Tan, C.; Chen, Z. General Two-Dimensional Absorption-Mode J-Resolved NMR Spectroscopy. Anal. Chem. 2017, 89, 12646–12651. [Google Scholar] [CrossRef] [PubMed]
- Georgakopoulou, I.; Chasapi, S.A.; Bariamis, S.E.; Varvarigou, A.; Spraul, M.; Spyroulias, G.A. Metabolic Changes in Early Neonatal Life: NMR Analysis of the Neonatal Metabolic Profile to Monitor Postnatal Metabolic Adaptations. Metabolomics 2020, 16, 58. [Google Scholar] [CrossRef] [PubMed]
- Pang, Z.; Chong, J.; Zhou, G.; de Lima Morais, D.A.; Chang, L.; Barrette, M.; Gauthier, C.; Jacques, P.É.; Li, S.; Xia, J. MetaboAnalyst 5.0: Narrowing the Gap between Raw Spectra and Functional Insights. Nucleic Acids Res. 2021, 49, W388–W396. [Google Scholar] [CrossRef]
- van den Berg, R.A.; Hoefsloot, H.C.J.; Westerhuis, J.A.; Smilde, A.K.; van der Werf, M.J. Centering, Scaling, and Transformations: Improving the Biological Information Content of Metabolomics Data. BMC Genom. 2006, 7, 142. [Google Scholar] [CrossRef] [Green Version]
- Gaude, E.; Chignola, F.; Spiliotopoulos, D.; Spitaleri, A.; Ghitti, M.; Garcìa-Manteiga, J.M.; Mari, S.; Giovanna, M. muma, an R package for metabolomics univariate and multivariate statistical analysis. Curr. Metab. 2013, 1.2, 180–189. [Google Scholar] [CrossRef]
- Tripathi, N.; Cotten, C.M.; Smith, P.B. Antibiotic Use and Misuse in the Neonatal Intensive Care Unit. Clin. Perinatol. 2012, 39, 61–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patton, L.; Li, N.; Garrett, T.J.; Ruoss, J.L.; Russell, J.T.; de la Cruz, D.; Bazacliu, C.; Polin, R.A.; Triplett, E.W.; Neu, J. Antibiotics Effects on the Fecal Metabolome in Preterm Infants. Metabolites 2020, 10, 331. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group A EOS (n = 23) | Group B LOS (n = 11) | Group C Control NICU (n = 14) | Group D Control Non NICU (n = 23) | |
|---|---|---|---|---|
| Male sex (n, %) | 8 (35) | 5 (45) | 9 (64) | 18 (75) |
| GA (weeks) | 34 (26–36) | 34 (25–36) | 35 (31–36) | 36 (35–36) |
| BW (gr) | 2150 (770–4060) | 1820 (690–2900) | 2085 (1630–3540) | 2740 (2100–3700) |
| Small for GA (n, %) | 5 (22) | 4 (36) | 2 (14) | 0(0) |
| Cesarian Section (n, %) | 8 (73) | 8 (73) | 11 (79) | 13 (57) |
| Apgar Score 1st min | 8 (3–9) | 8 (3–9) | 8 (7–9) | 9 (5–9) |
| Apgar Score 10th min | 9 (8–10) | 9 (8–10) | 9.5 (8–10) | 9 (7–10) |
| Antibiotics (n, %) | 23 (100) | 11 (100) | 1 (7) | 11 (48) |
| Premature Rupture of Membranes >18 h (n, %) | 1 (4.3) | 0 (0) | 3 (21.4) | 0 (0) |
| Mechanical Ventilation (n, %) | 17 (71) | 7 (64) | 4 (14) | 0 (0) |
| Nutrition | No | No | No | Breast milk |
| Laboratory findings | ||||
| B.C negative, CRP positive findings (n, %) | 17 (74) | 5 (45) | 0 (0) | 0 (0) |
| B.C positive, gram (+) (n, %) | 4 (17) | 5 (45) | 0 (0) | 0 (0) |
| B.C positive, gram (−) (n, %) | 1 (4) | 1 (10) | 0 (0) | 0 (0) |
| B.C positive, Fungi (n, %) | 1 (4) | 0 (0) | 0 (0) | 0 (0) |
| Metabolites | p-Value | Septic Group | |
|---|---|---|---|
| EOS versus healthy non NICU preterms | Taurine | 0.004 | |
| Gluconate | 8 × 10−5 | ||
| Lactose | 1 × 10−4 | ||
| Hippurate | 7 × 10−5 | ||
| LOS versus healthy non NICU preterms | Gluconate | 0.0007 | |
| Lactose | 0.01 | ||
| Betaine | 0.006 | ||
| N, N-Dimethylglycine | 0.005 | ||
| Hippurate | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Georgiopoulou, P.D.; Chasapi, S.A.; Christopoulou, I.; Varvarigou, A.; Spyroulias, G.A. Untargeted 1H-NMR Urine Metabolomic Analysis of Preterm Infants with Neonatal Sepsis. Appl. Sci. 2022, 12, 1932. https://doi.org/10.3390/app12041932
Georgiopoulou PD, Chasapi SA, Christopoulou I, Varvarigou A, Spyroulias GA. Untargeted 1H-NMR Urine Metabolomic Analysis of Preterm Infants with Neonatal Sepsis. Applied Sciences. 2022; 12(4):1932. https://doi.org/10.3390/app12041932
Chicago/Turabian StyleGeorgiopoulou, Panagiota D., Styliani A. Chasapi, Irene Christopoulou, Anastasia Varvarigou, and Georgios A. Spyroulias. 2022. "Untargeted 1H-NMR Urine Metabolomic Analysis of Preterm Infants with Neonatal Sepsis" Applied Sciences 12, no. 4: 1932. https://doi.org/10.3390/app12041932