
Augmented, Virtual and Mixed Reality in Dentistry: A Narrative Review on the Existing Platforms and Future Challenges

 ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
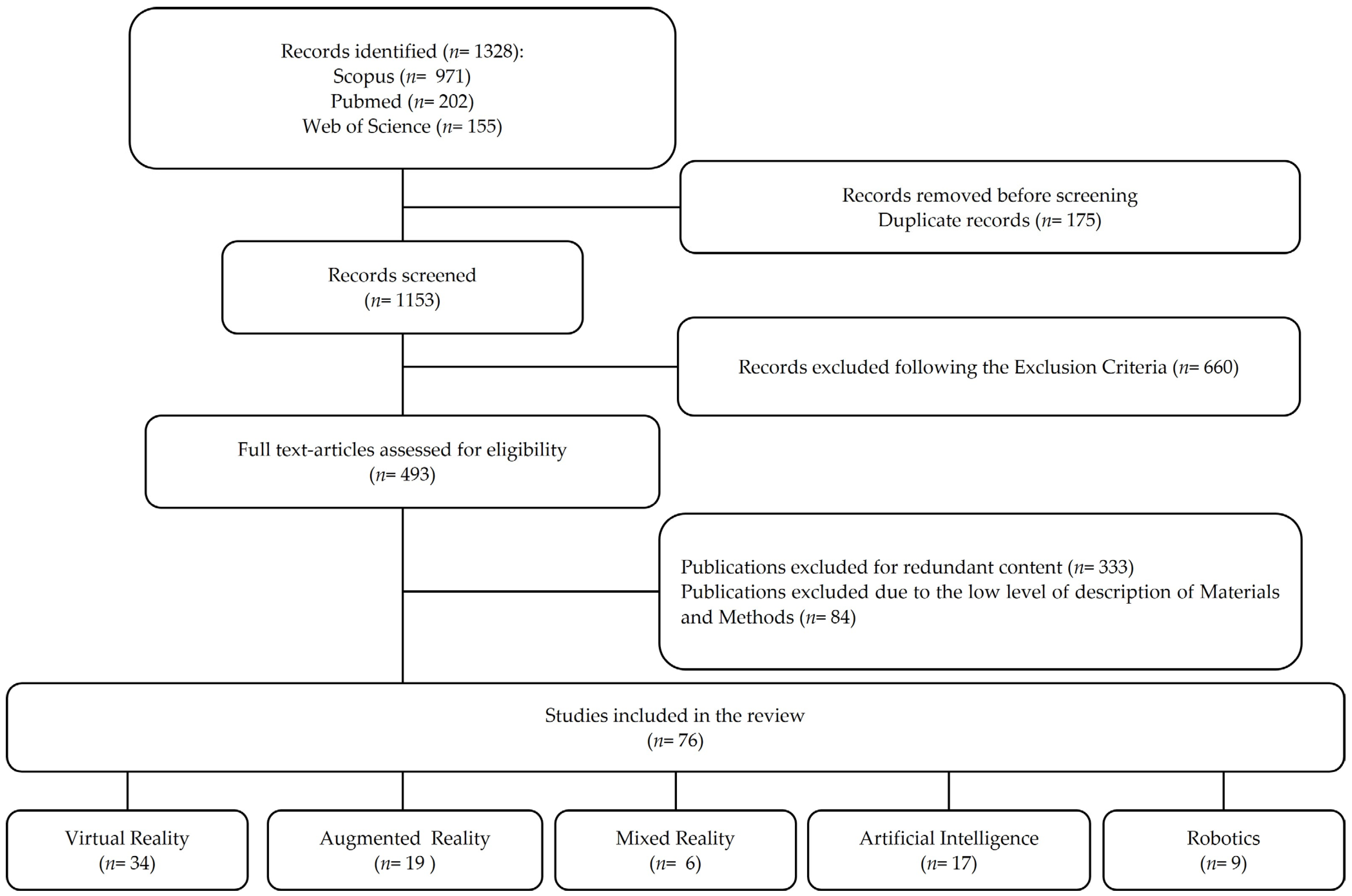
2. Materials and Methods
3. Results
3.1. Applications in Teaching Dental Morphology
3.2. Applications in Pre-Clinical Education
3.3. Applications in Clinical Practice
3.4. Applications in Dental Phobia
3.5. Applications in Patient Education
3.6. Dentist–Patient Communication Tools
3.7. Artificial Intelligence and Robotics
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Orsini, G.; Tosco, V.; Monterubbianesi, R.; Orilisi, G.; Putignano, A. A New Era in Restorative Dentistry. In The First Outstanding 50 Years of “Università Politecnica delle Marche”: Research Achievements in Life Sciences; Longhi, S., Monteriù, A., Freddi, A., Aquilanti, L., Ceravolo, M.G., Carnevali, O., Giordano, M., Moroncini, G., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 319–334. ISBN 978-3-030-33832-9. [Google Scholar]
- Flavián, C.; Ibáñez-Sánchez, S.; Orús, C. The Impact of Virtual, Augmented and Mixed Reality Technologies on the Customer Experience. J. Bus. Res. 2019, 100, 547–560. [Google Scholar] [CrossRef]
- Favaretto, M.; Shaw, D.; De Clercq, E.; Joda, T.; Elger, B.S. Big Data and Digitalization in Dentistry: A Systematic Review of the Ethical Issues. Int. J. Environ. Res. Public Health 2020, 17, 2495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zitzmann, N.U.; Matthisson, L.; Ohla, H.; Joda, T. Digital Undergraduate Education in Dentistry: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 3269. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.-K.; Yang, C.-H.; Hsieh, Y.-H.; Wang, J.-C.; Hung, C.-C. Augmented Reality (AR) and Virtual Reality (VR) Applied in Dentistry. Kaohsiung J. Med. Sci. 2018, 34, 243–248. [Google Scholar] [CrossRef]
- Joda, T.; Bornstein, M.M.; Jung, R.E.; Ferrari, M.; Waltimo, T.; Zitzmann, N.U. Recent Trends and Future Direction of Dental Research in the Digital Era. Int. J. Environ. Res. Public. Health 2020, 17, 1987. [Google Scholar] [CrossRef] [Green Version]
- Farronato, M.; Maspero, C.; Lanteri, V.; Fama, A.; Ferrati, F.; Pettenuzzo, A.; Farronato, D. Current State of the Art in the Use of Augmented Reality in Dentistry: A Systematic Review of the Literature. BMC Oral Health 2019, 19, 135. [Google Scholar] [CrossRef] [Green Version]
- Fraccastoro, F. Dal Mono al Suono Immersivo in Il Suono Immersivo, 1st ed.; Paguro Edizioni: Salerno, Italy, 2021; Volume 5, pp. 23–44. [Google Scholar]
- Joda, T.; Gallucci, G.O.; Wismeijer, D.; Zitzmann, N.U. Augmented and Virtual Reality in Dental Medicine: A Systematic Review. Comput. Biol. Med. 2019, 108, 93–100. [Google Scholar] [CrossRef]
- Baethge, C.; Goldbeck-Wood, S.; Mertens, S. SANRA—A Scale for the Quality Assessment of Narrative Review Articles. Res. Integr. Peer Rev. 2019, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Green, B.N.; Johnson, C.D.; Adams, A. Writing Narrative Literature Reviews for Peer-Reviewed Journals: Secrets of the Trade. J. Chiropr. Med. 2006, 5, 101–117. [Google Scholar] [CrossRef] [Green Version]
- Chiodera, G.; Orsini, G.; Tosco, V.; Monterubbianesi, R.; Manauta, J.; Devoto, W.; Putignano, A. Essential Lines: A Simplified Filling and Modeling Technique for Direct Posterior Composite Restorations. Int. J. Esthet. Dent. 2021, 16, 168–184. [Google Scholar]
- Iwanaga, J.; Kamura, Y.; Nishimura, Y.; Terada, S.; Kishimoto, N.; Tanaka, T.; Tubbs, R.S. A New Option for Education during Surgical Procedures and Related Clinical Anatomy in a Virtual Reality Workspace. Clin. Anat. 2021, 34, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Uruthiralingam, U.; Rea, P.M. Augmented and Virtual Reality in Anatomical Education—A Systematic Review. Adv. Exp. Med. Biol. 2020, 1235, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Küçük, S.; Kapakin, S.; Göktaş, Y. Learning Anatomy via Mobile Augmented Reality: Effects on Achievement and Cognitive Load. Anat. Sci. Educ. 2016, 9, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Reymus, M.; Liebermann, A.; Diegritz, C. Virtual Reality: An Effective Tool for Teaching Root Canal Anatomy to Undergraduate Dental Students—A Preliminary Study. Int. Endod. J. 2020, 53, 1581–1587. [Google Scholar] [CrossRef]
- Moussa, R.; Alghazaly, A.; Althagafi, N.; Eshky, R.; Borzangy, S. Effectiveness of Virtual Reality and Interactive Simulators on Dental Education Outcomes: Systematic Review. Eur. J. Dent. 2021. [Google Scholar] [CrossRef]
- Suvinen, T.I.; Messer, L.B.; Franco, E. Clinical Simulation in Teaching Preclinical Dentistry. Eur. J. Dent. Educ. 1998, 2, 25–32. [Google Scholar] [CrossRef]
- Ball, C.; Huang, K.-T.; Francis, J. Virtual Reality Adoption during the COVID-19 Pandemic: A Uses and Gratifications Perspective. Telemat. Inform. 2021, 65, 101728. [Google Scholar] [CrossRef]
- Tabatabai, S. COVID-19 Impact and Virtual Medical Education. J. Adv. Med. Educ. Prof. 2020, 8, 140–143. [Google Scholar] [CrossRef]
- Roy, E.; Bakr, M.M.; George, R. The Need for Virtual Reality Simulators in Dental Education: A Review. Saudi Dent. J. 2017, 29, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Eve, E.J.; Koo, S.; Alshihri, A.A.; Cormier, J.; Kozhenikov, M.; Donoff, R.B.; Karimbux, N.Y. Performance of Dental Students versus Prosthodontics Residents on a 3D Immersive Haptic Simulator. J. Dent. Educ. 2014, 78, 630–637. [Google Scholar] [CrossRef]
- de Boer, I.R.; Wesselink, P.R.; Vervoorn, J.M. Student Performance and Appreciation Using 3D vs. 2D Vision in a Virtual Learning Environment. Eur. J. Dent. Educ. 2016, 20, 142–147. [Google Scholar] [CrossRef]
- Kwon, H.-B.; Park, Y.-S.; Han, J.-S. Augmented Reality in Dentistry: A Current Perspective. Acta Odontol. Scand. 2018, 76, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Vávra, P.; Roman, J.; Zonča, P.; Ihnát, P.; Němec, M.; Kumar, J.; Habib, N.; El-Gendi, A. Recent Development of Augmented Reality in Surgery: A Review. J. Healthc. Eng. 2017, 2017. [Google Scholar] [CrossRef]
- Yamaguchi, S.; Ohtani, T.; Ono, S.; Yamanishi, Y.; Sohmura, T.; Yatani, H. Intuitive Surgical Navigation System for Dental Implantology by Using Retinal Imaging Display. Implant. Dent. Rapidly Evol. Pract. 2011. [Google Scholar] [CrossRef] [Green Version]
- Durham, M.; Engel, B.; Ferrill, T.; Halford, J.; Singh, T.P.; Gladwell, M. Digitally Augmented Learning in Implant Dentistry. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 387–398. [Google Scholar] [CrossRef]
- Jo, Y.-J.; Choi, J.-S.; Kim, J.; Kim, H.-J.; Moon, S.-Y. Virtual Reality (VR) Simulation and Augmented Reality (AR) Navigation in Orthognathic Surgery: A Case Report. Appl. Sci. 2021, 11, 5673. [Google Scholar] [CrossRef]
- Ayoub, A.; Pulijala, Y. The Application of Virtual Reality and Augmented Reality in Oral & Maxillofacial Surgery. BMC Oral Health 2019, 19, 238. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.-W.; Lee, J.Y. Virtual Surgical Planning and Three-Dimensional Simulation in Orthognathic Surgery. In The Surgery-First Orthognathic Approach: With Discussion of Occlusal Plane-Altering Orthognathic Surgery; Choi, J.-W., Lee, J.Y., Eds.; Springer: Singapore, 2021; pp. 159–183. ISBN 9789811575419. [Google Scholar]
- Fushima, K.; Kobayashi, M. Mixed-Reality Simulation for Orthognathic Surgery. Maxillofac. Plast. Reconstr. Surg. 2016, 38, 13. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Kim, H.; Kim, Y. Virtual Reality and Augmented Reality in Plastic Surgery: A Review. Arch. Plast. Surg. 2017, 44, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arikatla, V.S.; Tyagi, M.; Enquobahrie, A.; Nguyen, T.; Blakey, G.H.; White, R.; Paniagua, B. High Fidelity Virtual Reality Orthognathic Surgery Simulator. Proc. SPIE Int. Soc. Opt. Eng. 2018, 10576, 1057612. [Google Scholar] [CrossRef]
- Khanagar, S.B.; Al-Ehaideb, A.; Vishwanathaiah, S.; Maganur, P.C.; Patil, S.; Naik, S.; Baeshen, H.A.; Sarode, S.S. Scope and Performance of Artificial Intelligence Technology in Orthodontic Diagnosis, Treatment Planning, and Clinical Decision-Making—A Systematic Review. J. Dent. Sci. 2021, 16, 482–492. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, P.; Milgrom, P.; Getz, T. Treating Fearful Dental Patients: A Practical Behavioral Approach. J. Dent. Pract. Adm. 1987, 4, 140–147. [Google Scholar]
- Getka, E.J.; Glass, C.R. Behavioral and Cognitive-Behavioral Approaches to the Reduction of Dental Anxiety. Behav. Ther. 1992, 23, 433–448. [Google Scholar] [CrossRef]
- Gauthier, J.; Savard, F.; Hallé, J.-P.; Dufour, L. Flooding and Coping Skills Training in the Management of Dental Fear. Scand. J. Behav. Ther. 1985, 14, 3–15. [Google Scholar] [CrossRef]
- Raghav, K.; Van Wijk, A.J.; Abdullah, F.; Islam, M.N.; Bernatchez, M.; De Jongh, A. Efficacy of Virtual Reality Exposure Therapy for Treatment of Dental Phobia: A Randomized Control Trial. BMC Oral Health 2016, 16, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krijn, M.; Emmelkamp, P.M.G.; Olafsson, R.P.; Biemond, R. Virtual Reality Exposure Therapy of Anxiety Disorders: A Review. Clin. Psychol. Rev. 2004, 24, 259–281. [Google Scholar] [CrossRef]
- Baus, O.; Bouchard, S. Moving from Virtual Reality Exposure-Based Therapy to Augmented Reality Exposure-Based Therapy: A Review. Front. Hum. Neurosci. 2014, 8, 112. [Google Scholar] [CrossRef] [Green Version]
- Custódio, N.B.; Costa, F.D.S.; Cademartori, M.G.; da Costa, V.P.P.; Goettems, M.L. Effectiveness of Virtual Reality Glasses as a Distraction for Children During Dental Care. Pediatr. Dent. 2020, 42, 93–102. [Google Scholar]
- Vassend, O.; Willumsen, T.; Hoffart, A. Effects of Dental Fear Treatment on General Distress. The Role of Personality Variables and Treatment Method. Behav. Modif. 2000, 24, 580–599. [Google Scholar] [CrossRef] [PubMed]
- Berggren, U. Reduction of Fear and Anxiety in Adult Fearful Patients. Int. Dent. J. 1987, 37, 127–136. [Google Scholar] [PubMed]
- Hoffman, H.G.; Sharar, S.R.; Coda, B.; Everett, J.J.; Ciol, M.; Richards, T.; Patterson, D.R. Manipulating Presence Influences the Magnitude of Virtual Reality Analgesia. Pain 2004, 111, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, H.G.; Garcia-Palacios, A.; Patterson, D.R.; Jensen, M.; Furness, T.; Ammons, W.F. The Effectiveness of Virtual Reality for Dental Pain Control: A Case Study. Cyberpsychol. Behav. 2001, 4, 527–535. [Google Scholar] [CrossRef]
- Gujjar, K.R.; Sharma, R.; Jongh, A.D. Virtual Reality Exposure Therapy for Treatment of Dental Phobia. Dent. Update 2017, 44, 423–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gujjar, K.R.; van Wijk, A.; Sharma, R.; de Jongh, A. Virtual Reality Exposure Therapy for the Treatment of Dental Phobia: A Controlled Feasibility Study. Behav. Cogn. Psychother. 2018, 46, 367–373. [Google Scholar] [CrossRef]
- Heidari, E.; Newton, J.T.; Banerjee, A. Minimum Intervention Oral Healthcare for People with Dental Phobia: A Patient Management Pathway. Br. Dent. J. 2020, 229, 417–424. [Google Scholar] [CrossRef]
- Felemban, O.M.; Alshamrani, R.M.; Aljeddawi, D.H.; Bagher, S.M. Effect of Virtual Reality Distraction on Pain and Anxiety during Infiltration Anesthesia in Pediatric Patients: A Randomized Clinical Trial. BMC Oral Health 2021, 21, 321. [Google Scholar] [CrossRef]
- Hendrix, C.; Barfield, W. The Sense of Presence within Auditory Virtual Environments. Presence Teleoperators Virtual Environ. 1996, 5, 290–301. [Google Scholar] [CrossRef]
- Rajguru, C.; Obrist, M.; Memoli, G. Spatial Soundscapes and Virtual Worlds: Challenges and Opportunities. Front. Psychol. 2020, 11, 569056. [Google Scholar] [CrossRef]
- Stein, C.; Santos, N.M.L.; Hilgert, J.B.; Hugo, F.N. Effectiveness of Oral Health Education on Oral Hygiene and Dental Caries in Schoolchildren: Systematic Review and Meta-Analysis. Community Dent. Oral Epidemiol. 2018, 46, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, M.; Rakhshanderou, S.; Ramezankhani, A.; Noroozi, M.; Armoon, B. Oral Health Education and Promotion Programmes: Meta-Analysis of 17-Year Intervention. Int. J. Dent. Hyg. 2018, 16, 59–67. [Google Scholar] [CrossRef]
- Jimenez, Y.A.; Cumming, S.; Wang, W.; Stuart, K.; Thwaites, D.I.; Lewis, S.J. Patient Education Using Virtual Reality Increases Knowledge and Positive Experience for Breast Cancer Patients Undergoing Radiation Therapy. Support. Care Cancer 2018, 26, 2879–2888. [Google Scholar] [CrossRef]
- Bekelis, K.; Calnan, D.; Simmons, N.; MacKenzie, T.A.; Kakoulides, G. Effect of an Immersive Preoperative Virtual Reality Experience on Patient Reported Outcomes: A Randomized Controlled Trial. Ann. Surg. 2017, 265, 1068–1073. [Google Scholar] [CrossRef]
- Lombardi, R.E. The Principles of Visual Perception and Their Clinical Application to Denture Esthetics. J. Prosthet. Dent. 1973, 29, 358–382. [Google Scholar] [CrossRef]
- Moussa, C.; Hardan, L.; Kassis, C.; Bourgi, R.; Devoto, W.; Jorquera, G.; Panda, S.; Abou Fadel, R.; Cuevas-Suárez, C.E.; Lukomska-Szymanska, M. Accuracy of Dental Photography: Professional vs. Smartphone’s Camera. BioMed Res. Int. 2021, 2021, e3910291. [Google Scholar] [CrossRef]
- Grischke, J.; Johannsmeier, L.; Eich, L.; Griga, L.; Haddadin, S. Dentronics: Towards Robotics and Artificial Intelligence in Dentistry. Dent. Mater. 2020, 36, 765–778. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Larrivée, N.; Lee, A.; Bilaniuk, O.; Durand, R. Use of Artificial Intelligence in Dentistry: Current Clinical Trends and Research Advances. J. Can. Dent. Assoc. 2021, 87, l7. [Google Scholar] [PubMed]
- Abouzeid, H.L.; Chaturvedi, S.; Abdelaziz, K.M.; Alzahrani, F.A.; AlQarni, A.A.S.; Alqahtani, N.M. Role of Robotics and Artificial Intelligence in Oral Health and Preventive Dentistry—Knowledge, Perception and Attitude of Dentists. Oral Health Prev. Dent. 2021, 19, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Park, W.J.; Park, J.-B. History and Application of Artificial Neural Networks in Dentistry. Eur. J. Dent. 2018, 12, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.; Abbasi, M.S.; Zuberi, F.; Qamar, W.; Halim, M.S.B.; Maqsood, A.; Alam, M.K. Artificial Intelligence Techniques: Analysis, Application, and Outcome in Dentistry—A Systematic Review. BioMed Res. Int. 2021, 2021, 9751564. [Google Scholar] [CrossRef]
- Hung, M.; Voss, M.W.; Rosales, M.N.; Li, W.; Su, W.; Xu, J.; Bounsanga, J.; Ruiz-Negrón, B.; Lauren, E.; Licari, F.W. Application of Machine Learning for Diagnostic Prediction of Root Caries. Gerodontology 2019, 36, 395–404. [Google Scholar] [CrossRef]
- Udod, O.A.; Voronina, H.S.; Ivchenkova, O.Y. Application of Neural Network Technologies in the Dental Caries Forecast. Wiadomosci Lek. Wars. Pol. 2020, 73, 1499–1504. [Google Scholar] [CrossRef]
- Tandon, D.; Rajawat, J.; Banerjee, M. Present and Future of Artificial Intelligence in Dentistry. J. Oral Biol. Craniofacial Res. 2020, 10, 391–396. [Google Scholar] [CrossRef]
- Schwendicke, F.; Krois, J. Data Dentistry: How Data Are Changing Clinical Care and Research. J. Dent. Res. 2021, 220345211020265. [Google Scholar] [CrossRef]
- Lee, J.-H.; Kim, D.-H.; Jeong, S.-N.; Choi, S.-H. Detection and Diagnosis of Dental Caries Using a Deep Learning-Based Convolutional Neural Network Algorithm. J. Dent. 2018, 77, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Gürel, G.; Paolucci, B.; Iliev, G.; Filtchev, D.; Schayder, A. The Fifth Dimension in Esthetic Dentistry. Int. J. Esthet. Dent. 2021, 16, 10–32. [Google Scholar] [PubMed]
- Schwendicke, F.; Elhennawy, K.; Paris, S.; Friebertshäuser, P.; Krois, J. Deep Learning for Caries Lesion Detection in Near-Infrared Light Transillumination Images: A Pilot Study. J. Dent. 2020, 92, 103260. [Google Scholar] [CrossRef]
- Casalegno, F.; Newton, T.; Daher, R.; Abdelaziz, M.; Lodi-Rizzini, A.; Schürmann, F.; Krejci, I.; Markram, H. Caries Detection with Near-Infrared Transillumination Using Deep Learning. J. Dent. Res. 2019, 98, 1227–1233. [Google Scholar] [CrossRef] [Green Version]
- Aubreville, M.; Knipfer, C.; Oetter, N.; Jaremenko, C.; Rodner, E.; Denzler, J.; Bohr, C.; Neumann, H.; Stelzle, F.; Maier, A. Automatic Classification of Cancerous Tissue in Laserendomicroscopy Images of the Oral Cavity Using Deep Learning. Sci. Rep. 2017, 7, 11979. [Google Scholar] [CrossRef] [Green Version]
- Johari, M.; Esmaeili, F.; Andalib, A.; Garjani, S.; Saberkari, H. Detection of Vertical Root Fractures in Intact and Endodontically Treated Premolar Teeth by Designing a Probabilistic Neural Network: An Ex Vivo Study. Dentomaxillofacial Radiol. 2016, 46, 20160107. [Google Scholar] [CrossRef] [Green Version]
- Ekert, T.; Krois, J.; Meinhold, L.; Elhennawy, K.; Emara, R.; Golla, T.; Schwendicke, F. Deep Learning for the Radiographic Detection of Apical Lesions. J. Endod. 2019, 45, 917–922.e5. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, M.; Inamoto, K.; Shibata, N.; Ariji, Y.; Yanashita, Y.; Kutsuna, S.; Nakata, K.; Katsumata, A.; Fujita, H.; Ariji, E. Evaluation of an Artificial Intelligence System for Detecting Vertical Root Fracture on Panoramic Radiography. Oral Radiol. 2020, 36, 337–343. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, F.; Fan, S.; Chow, J.K.-F. Robotics in Dental Implantology. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 513–518. [Google Scholar] [CrossRef]
- Yuan, F.S.; Wang, Y.; Zhang, Y.P.; Sun, Y.C.; Wang, D.X.; Lyu, P.J. Study on the Appropriate Parameters of Automatic Full Crown Tooth Preparation for Dental Tooth Preparation Robot. Zhonghua Kou Qiang Yi Xue Za Zhi 2017, 52, 270–273. [Google Scholar]
- Adel, S.; Zaher, A.; El Harouni, N.; Venugopal, A.; Premjani, P.; Vaid, N. Robotic Applications in Orthodontics: Changing the Face of Contemporary Clinical Care. BioMed Res. Int. 2021, 2021, e9954615. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, R. Writing Narrative Style Literature Reviews. Med. Writ. 2015, 24, 230–235. [Google Scholar] [CrossRef]
- Tiu, J.; Cheng, E.; Hung, T.-C.; Yu, C.-C.; Lin, T.; Schwass, D.; Al-Amleh, B. Effectiveness of Crown Preparation Assessment Software As an Educational Tool in Simulation Clinic: A Pilot Study. J. Dent. Educ. 2016, 80, 1004–1011. [Google Scholar] [CrossRef]
- Makransky, G.; Petersen, G.B. The Cognitive Affective Model of Immersive Learning (CAMIL): A Theoretical Research-Based Model of Learning in Immersive Virtual Reality. Educ. Psychol. Rev. 2021, 33, 937–958. [Google Scholar] [CrossRef]
- Radianti, J.; Majchrzak, T.A.; Fromm, J.; Wohlgenannt, I. A Systematic Review of Immersive Virtual Reality Applications for Higher Education: Design Elements, Lessons Learned, and Research Agenda. Comput. Educ. 2020, 147, 103778. [Google Scholar] [CrossRef]
- Meola, A.; Cutolo, F.; Carbone, M.; Cagnazzo, F.; Ferrari, M.; Ferrari, V. Augmented Reality in Neurosurgery: A Systematic Review. Neurosurg. Rev. 2017, 40, 537–548. [Google Scholar] [CrossRef]
- Amantini, S.N.S.R.; Montilha, A.A.P.; Antonelli, B.C.; Leite, K.T.M.; Rios, D.; Cruvinel, T.; Lourenço Neto, N.; Oliveira, T.M.; Machado, M.A.A.M. Using Augmented Reality to Motivate Oral Hygiene Practice in Children: Protocol for the Development of a Serious Game. JMIR Res. Protoc. 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Pandrangi, V.C.; Gaston, B.; Appelbaum, N.P.; Albuquerque, F.C.; Levy, M.M.; Larson, R.A. The Application of Virtual Reality in Patient Education. Ann. Vasc. Surg. 2019, 59, 184–189. [Google Scholar] [CrossRef]
- Alauddin, M.S.; Baharuddin, A.S.; Mohd Ghazali, M.I. The Modern and Digital Transformation of Oral Health Care: A Mini Review. Healthc. Basel Switz. 2021, 9, 118. [Google Scholar] [CrossRef] [PubMed]
- Khanagar, S.B.; Al-ehaideb, A.; Maganur, P.C.; Vishwanathaiah, S.; Patil, S.; Baeshen, H.A.; Sarode, S.C.; Bhandi, S. Developments, Application, and Performance of Artificial Intelligence in Dentistry—A Systematic Review. J. Dent. Sci. 2021, 16, 508–522. [Google Scholar] [CrossRef] [PubMed]
- Weinbaum (Weaver), D.; Veitas, V. Open Ended Intelligence: The Individuation of Intelligent Agents. J. Exp. Theor. Artif. Intell. 2017, 29, 371–396. [Google Scholar] [CrossRef] [Green Version]
- Revilla-León, M.; Gómez-Polo, M.; Vyas, S.; Barmak, A.B.; Özcan, M.; Att, W.; Krishnamurthy, V.R. Artificial Intelligence Applications in Restorative Dentistry: A Systematic Review. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef] [PubMed]
- Buchner, J.; Buntins, K.; Kerres, M. The Impact of Augmented Reality on Cognitive Load and Performance: A Systematic Review. J. Comput. Assist. Learn. 2021, 38, 285–303. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Original articles describing the application of virtual, augmented and mixed reality, artificial intelligence, and robotics in dentistry (at least one of them) Available in the English language Published in peer-reviewed academic or professional journals | Opinion or narrative discussions that did not report on the use of virtual and or augmented reality, artificial intelligence, and robotics in dentistry. Detailed programming for virtual reality, abstracts, conference proceedings, letters to the editor and, case reports were excluded. |
| PerioSim® | Dentsim™ | IDEA | Simodont® | Voxel Man | CDS | |
|---|---|---|---|---|---|---|
| Teeth Used | Animated | Plastic teeth | Animated | Animated | Animated | Animated |
| Right And Left Operation | Available | Available | Available | Available | Available | Available |
| Reported Real Life Experience | Tactile sensation is realistic for teeth but not for gingiva | Realistic experience using plastic teeth on a real manikin | Tactile sensation still needs to be tuned to simulate a genuine sensation | 3D images are realistic. However, the texture of healthy decayed and restored tooth structure still needs improvement | / | / |
| Ergonomic Postures | No | Yes | No | Yes | No | Yes |
| Direct Transfer of Data to Program Instructor/Tutor | Not available | Yes Run time control. Application enables the instructor to control run time grades. | Yes The software contains a replay mode. Upon completion of a specified task, it can be watched in full by the student or the instructor. | Yes Allows the instructor to watch six simulators live at once and record all preparations for evaluation in order to give feedback later. | Not available | Yes Operating procedures are recorded and can be reviewed to facilitate in training, grading and verifying. |
| Instant Feed Back | No | Yes | Yes | Yes | Yes | Yes |
| Exam Simulation | Yes | Yes | No | Yes | Yes | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monterubbianesi, R.; Tosco, V.; Vitiello, F.; Orilisi, G.; Fraccastoro, F.; Putignano, A.; Orsini, G. Augmented, Virtual and Mixed Reality in Dentistry: A Narrative Review on the Existing Platforms and Future Challenges. Appl. Sci. 2022, 12, 877. https://doi.org/10.3390/app12020877
Monterubbianesi R, Tosco V, Vitiello F, Orilisi G, Fraccastoro F, Putignano A, Orsini G. Augmented, Virtual and Mixed Reality in Dentistry: A Narrative Review on the Existing Platforms and Future Challenges. Applied Sciences. 2022; 12(2):877. https://doi.org/10.3390/app12020877
Chicago/Turabian StyleMonterubbianesi, Riccardo, Vincenzo Tosco, Flavia Vitiello, Giulia Orilisi, Franco Fraccastoro, Angelo Putignano, and Giovanna Orsini. 2022. "Augmented, Virtual and Mixed Reality in Dentistry: A Narrative Review on the Existing Platforms and Future Challenges" Applied Sciences 12, no. 2: 877. https://doi.org/10.3390/app12020877