1. Introduction
Knee joint ligaments are essential structures that ensure joint stability during walking. Among these, the anterior cruciate ligament (ACL) is of particular interest because of some peculiarities. From one side, in physiological conditions, it seems to be fundamental since it contrasts the anterior sliding of the tibia and it sustains considerable loads [
1]. On the other hand, it seems that it is not so relevant in that people with partial or total ACL lesions can carry out relatively normal day life activity [
2]. Despite the attention that the topic has always attracted in the scientific community, the actual need for surgical reconstruction of an injured anterior cruciate ligament is still a matter of debate [
3,
4]. More than 30 years ago, the orthopedic community began to divide patients with ACL injuries into two categories depending on the functional compensatory ability they were able to put in place: copers and non-copers [
5]. Based on this classification, historically, about two-thirds of patients with ACL injury are defined as copers, and there is fair agreement to treat this type of patient conservatively [
6,
7].
The occurrence of coping with an ACL-deficient knee relies mostly on a balance between functional needs and psychological attitude, but the anatomical substratum of this clearing skill depends on several biomechanical adjustments. Early biomechanical studies [
8] underlined the possibility that the hamstrings can compensate for ACL deficiency. The external knee joint moment was shown to shift from flexor to extensor in the early phase of the stride cycle, and this effect was attributed to the hamstring’s increased activity. Quite a wide review of the interaction between muscle forces and ACL loading was performed by [
9]. In their investigation, the authors stated that not only can the muscles spanning the knee joint affect the loads on the knee’s internal structure but also non-knee-spanning muscles have to be considered in that they can change the ground reaction force and can transfer moments and forces to other anatomical segments due to the phenomenon of dynamic coupling. However, the most relevant effects on ACL loading are commonly attributed to the quadriceps, which act as an antagonist of the ligament, increasing the ACL load, and to the hamstrings, which act as an agonist to reduce the ACL load. However, their role is tightly dependent on the kinematic condition since the direction of their force and their relative moment arm at the knee depends on the joint angle [
9]. Furthermore, in physiological conditions, there are specific phases along the stride cycle in which the two muscle groups are activated, and this makes it difficult to understand how they influence the tension of the ligaments.
The effects of different muscle contractions on the knee ligaments’ tension during walking were thoroughly analyzed in previous work [
10] through the use of a musculoskeletal model that was specifically developed for that purpose. The results showed that the quadriceps, acting at the load acceptance phase and the late stance–early swing phase, are mainly responsible for the ACL tension in that, when removed, the load on this ligament decreases considerably at the load acceptance phase and reduces to close to zero at late stance–early swing phase. In contrast, the removal of the hamstrings has no relevant effect in the mentioned phases but instead results in an increase in ACL tension in the late swing phase when these muscles are active in physiological conditions. The change in the ligament’s tension of course depends on the changes in the knee kinematics, which, in turn, depend on the forces applied to the femur and tibia during motion. The relative motion between the distal femur and proximal tibia was studied through different techniques [
11,
12,
13,
14,
15] by always considering the intact knee. The change in stiffness and range of motion deriving from the systematic removal of different knee ligaments was instead analyzed in a cadaver study [
16].
To our best knowledge, the knee kinematics resulting from the removal of the ACL during walking and the consequent effects of changing the quadriceps and hamstrings activity have never been analyzed. The present work addressed this problem by using a musculoskeletal model to perform dynamic simulations. Digital models of the femur and the tibia were attached to the thigh and the shank segments, respectively, in such a way that only knee flexion–extension was imposed, while the remaining five degrees of freedom were left unconstrained, where they were controlled by the bone surface interactions and by the ligaments connecting the distal femur and the proximal tibia and determined by forward dynamics computation. The results, besides confirming the consolidated knowledge about the role of quadriceps and hamstrings, provided quantitative data that could be useful for better understanding the compensation mechanisms adopted by ACL-deficient subjects.
2. Materials and Methods
A three-dimensional dynamic musculoskeletal model [
10] was used to simulate the behavior of the knee joint during walking in different testing conditions. The model consisted of an articulated system of rigid bodies linked together by a series of rotation actuators (motors) that were animated by kinematic data corresponding to an unperturbed, normal walking cycle. The data that was used was extracted from our repository and referred to the average of 14 strides from 5 normal subjects who were males aged between 24 and 36 years and walking barefoot at their natural velocity. The SAFLo (Servizio di Analisi della Funzionalità Locomotoria) marker set protocol [
17] was used and it provided the kinematic data corresponding to the 6 degrees of freedom (d.o.f.) of the pelvis (anterior/posterior, medial/lateral, vertical displacements, anteversion/retroversion, frontal plane tilt and horizontal rotation), the 3 d.o.f. of the hip joint (flexion/extension, adduction/abduction and internal/external rotation), the 2 d.o.f. of the knee joint (flexion/extension and internal/external rotation) and the 2 d.o.f. of the ankle joint (plantar/dorsiflexion and pronation/supination). These data were normalized in time and referred to an ideal cycle duration of 1 s. Masses of body segments, corresponding to an ideal subject that was 1.72 m tall and had 70 kg of body mass, were obtained from an anthropometric table [
18]. The inverse dynamics problem solution provided us with the knee joint moments corresponding to this ideal subject. Digital models of the femur and the tibia, which were obtained through MRI images of a Caucasian male (age: 42 years, body height: 1.72 m, body mass: 70 kg) were attached to the thigh and the shank segments, respectively, in such a way that the only knee flexion–extension was imposed, while the remaining five d.o.f. were left unconstrained, where they were controlled by the interaction of the femoral condyles and tibial plateau surfaces and the knee joint ligaments (reproduced by several springs with non-linear characteristics) and resulting from the forward dynamics computation. The result was that, during the dynamic simulation of walking, the relative motion of the tibia and femur depended on the morphology of the femoral condyles in contact with the tibia plateaus, on the tension of the ligaments, on the muscle forces, and on the external forces and moments (ground reaction force, weight, and inertia of the shank and foot).
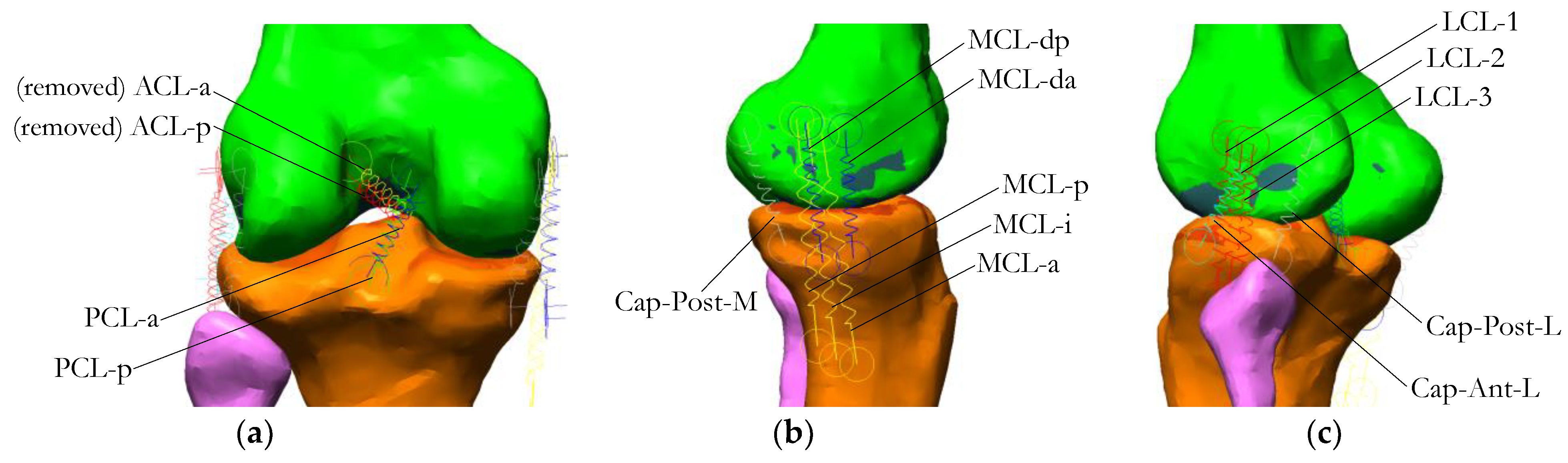
The 3D model of the knee included a detailed ligament structure (
Figure 1), which was composed of the anterior cruciate ligament (ACL, specifically removed for the purpose of this study), the posterior cruciate ligament (PCL), the lateral collateral ligament (LCL), the medial collateral ligament (subdivided in superficial and deep components (MCL and MCL-deep, respectively)) and the fibrous capsule, represented by its antero-lateral (Cap-Ant-L), posterior-lateral (Cap-Post-L) and posterior-medial (Cap-Post-M) bundles.
An exhaustive description of this model can be found in the cited publication [
10]. In the present study, the springs representing the two components of the ACL (
Figure 1a) were set at zero stiffness, which corresponded to removing the ACL from the model (‘NoACL’ condition), without any change in the external forces and moments applied. As in the previous work, the muscle forces were estimated using a static optimization algorithm, which applied the minimization of the maximum force criterion in relation to the muscle physiological cross-sectional area [
19]. The forces were transmitted directly to the bones as if the tendons were inextensible. Then, the force actuators corresponding to the hamstrings were set to zero force (‘NoACL-Ham’ condition), and, in a subsequent simulation, the quadriceps force was set to zero (‘NoACL-Quad’ condition). In all these conditions, the knee kinematics and the load on the remaining ligaments were analyzed.
Specifically, the average differences produced in the ligaments tensions and knee kinematics by the removal of the ACL with respect to the physiological context (‘Intact Knee’ condition) were measured in the predicted phases of ACL recruitment: load acceptance phase (0–26% of the gait cycle) and late stance–early swing phase (36–76% of the gait cycle).
The ACL recruitment during the gait cycle predicted in the previous study is reported in
Figure 2.
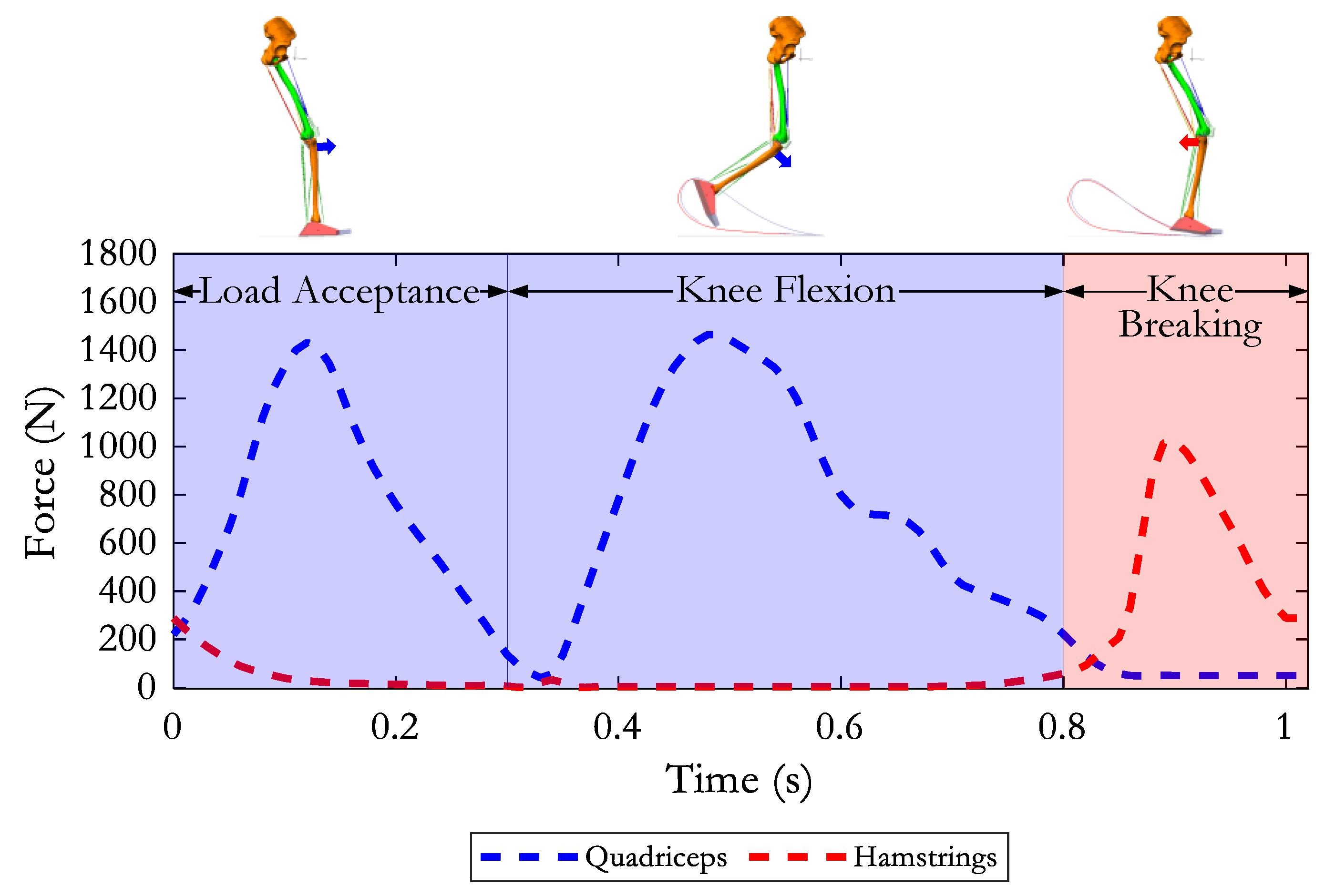
The sum of the predicted muscle forces in the quadriceps and hamstring muscle groups is depicted in
Figure 3 (for the purpose of this study, the gastrocnemius force is not represented). The light blue and pink areas correspond to the phases of the gait cycle in which the quadriceps and hamstring forces were predominant.
The changes produced by the subsequent removal of the quadriceps and hamstrings on the ACL-deficient knee were quantified by measuring the average difference in ligament tensions and knee kinematics between the ‘NoACL’ and ‘NoACL-Quad’ conditions and the ‘NoACL’ and ‘NoACL-Ham’ conditions, respectively. Specifically, the analysis was performed in the phases in which the muscle group of interest was dominating (
Figure 3): the ‘Load Acceptance’ phase (0–30% of the gait cycle) and ‘Knee Flexion’ phase (31–80% of the stride cycle) for the quadriceps muscle group, and the ‘Knee Breaking’ phase (81–100% of the gait cycle) for the hamstrings.
4. Discussion
Anterior cruciate ligament injury is a quite common occurrence, with an incidence of between 30 and 78 cases per 100,000 people per year [
20]. The role of a surrogate for ACL action played by the hamstrings has been widely studied [
21,
22,
23]. At the same time, tendency-to-atrophy exhibited by the quadriceps muscle was observed [
24] and was interpreted as the result of an arthrogenic inhibition aimed at reducing the load on the ACL [
25]. Nevertheless, the quadriceps volume and function are considered the pivotal elements on which the coping mechanism is founded [
26]. To our best knowledge, the effects of ACL removal on the remaining knee joint structures have never been quantified, as well as the compensation produced by the hamstrings and quadriceps in an ACL-deficient knee during walking. In the present work, we considered this problem by using a musculoskeletal model and forward dynamics simulation. The reproduction of the complex structure of the knee is very challenging, and any model must adopt simplifications. The main limitation of our musculoskeletal model is the lack of a soft interface between the femur and tibia surfaces representing the cartilage and the menisci. This could have reduced the presence of some erratic peaks in the forces obtained during the movement and could have yielded a smoother time course for all the computed variables. Furthermore, our model is to be considered a ‘generic model’ and could hardly become a ‘subject specific’ model, as would be desirable. In fact, due to some limitations in the software, the procedure to adapt the model to different sizes is quite troublesome, mainly because of the delicate procedure of ligament repositioning. The transfer of kinematic data from the data acquisition plaform to the model is also not so straightforward, and this makes the use of the model for individual data or different tasks rather demanding. In any case, our biomechanical musculoskeletal model contained the relevant functional elements of the knee joint and allowed for a dynamic simulation of what should happen if specific isolated elements are changed. In the present work, to predict the effects of ACL sacrifice and the changing of quadriceps and hamstring activity on the knee joint, we simulated a dramatic ACL removal, a reduction to zero of the hamstring force and a zeroing of the quadriceps force. The effects were observed at the level of knee kinematics and redistribution of the loads among the remaining ligaments.
4.1. Knee Kinematics
Our previous work [
10] showed that, during walking, the ACL is recruited in the load acceptance phase and at the late stance–early swing phase when the internal moment produced by the muscles is an extensor.
In the absence of the ACL, during the load acceptance phase, the tibia reaches a maximum anterior translation exactly at the same instant in which the ACL should express its maximum tension.
In the late stance–early swing phase, the forward traction transmitted to the tibia by the quadriceps would be compensated in an intact knee by the tension expressed by the ACL. In the absence of an ACL, the anterior translation of the tibia was increased and reached a maximum just before the mid-swing, at approximately the same time identified by Shelburne et al. [
1]. Then, as confirmed by these authors, the tibia recovered the same physiological translation in the second half of the swing phase as soon as the hamstring muscles were activated and exerted their posterior pulling action. Specifically, our results showed that the hamstring activity in an ACL-deficient knee prevented the anterior translation of the tibia from increasing further away from the physiological ranges, avoiding an average increase of 9 mm in the second half of the swing phase.
All these findings confirmed the hamstrings’ ability to compensate for the ligament deficit, demonstrating the importance of training these muscles during the rehabilitation program of ACL-deficient knee subjects. This aspect has been investigated and conceptually confirmed by [
26], but thanks to the dynamic simulation, this effect was quantified in our study.
Concerning the quadriceps, in our simulation, the inactivation of this muscle in an ACL-deficient knee resulted in an average reduction in the anterior translation of the tibia by 4 mm during load acceptance and by 9.5 mm during the large knee flexion compared with the knee with the ACL sacrificed and quadriceps active. This behavior supports the well-known tendency to atrophy of the quadriceps that arises in patients with an anterior cruciate rupture [
27].
4.2. Ligament Forces Redistribution
In the absence of the ACL, both the superficial and deep bundles of the MCL appeared overloaded in the load acceptance phase and even more so in the early swing phase. Specifically, the deep layer of the MCL exhibited the greatest increase in its tension. The posterior-lateral component of the fibrous capsule also had a mild increase during the load acceptance phase. In particular, Cap-Post-M, superficial MCL and deep MCL reached maximum tensions of 38 N, 94 N and 72 N, respectively, at the same time instant as the peak expected for an ACL in an intact knee. These increases in tension did not appear to be random but were well-calibrated so that when added together, they managed to produce the tension that was developed by ACL in the intact knee during the load acceptance phase (approximately 200 N). Hence, the prolonged recruitment of the superficial and deep MCLs in the first 20% of the cycle was probably required to compensate for the ACL deficiency in coping with an anterior tibial translation; instead, in the first half of the swing phase, the increase in MCL tension (superficial and deep) was even more consistent because it had to cope not only with the greater forward sliding of the tibia but also with its greater abduction. These results are in good agreement with the study of [
1]. No relevant changes in the loading of the lateral components of the capsule (Caps-Ant-L and Caps-Post-L) or the LCL and PCL were observed when the ACL was sacrificed. Thus, it appeared that the MCL (superficial and deep) was the main passive stabilizer of the anterior translation of the tibia when the ACL was lacking.
In the absence of the hamstrings, the main effects were observed again at the MCL components, where their recruitment along the whole swing phase was prolonged with a peak at late swing. However, in this condition, the whole capsule (Caps-Ant-L, Caps-Post-L and Caps-Post-M) also exhibited a peak of force at the end of the swing phase. The PCL, on the other hand, appeared completely relaxed in the late swing. This appeared to be the net consequence of the lack of restraint exerted by the hamstrings on the forward displacement of the tibia. No relevant changes in the LCL were observed with the hamstring removal during the late swing phase.
The deactivation of the quadriceps when the ACL was removed produced a reduction in the MCL and deep MCL tensions. On the other hand, it produced early and long-lasting recruitment of the PCL during the stance phase. Noticeable was the sharp loading of the LCL in the second half of load acceptance when the knee was recovering from its initial yielding. If we consider that in the same phase, the PCL was also starting to be loaded and the knee exhibited abnormal adduction (see
Figure 4b), we can recognize that the lack of the quadriceps made the knee more unstable, and this was demonstrated also by the frequent oscillations observed in almost all the variables in this condition (see the force in the Caps-Post-L in particular). However, the reduction in the quadriceps activity (which, over time, can lead to partial atrophy) would find its effectiveness in reducing the loads of all ligaments in general, with the exception of the PCL, which instead requires more consistent recruitment in the support phase.
It could be concluded that in subjects with ACL removal or severe lesions, in conservative rehabilitation treatment, the training of hamstrings aimed at the maintenance of good muscle tone would be of fundamental importance either to compensate for the ligament deficit and limit the anterior sliding of the tibia and to reduce the risk of injury to the MCL (the deep component in particular), which would reach very high tensions acting against the anterior tibial translation and valgus deflection. Not with the same objectives, similar treatment is also to be provided to the quadriceps to avoid excessive weakening. Other clinical considerations can be advanced in relation to patients undergoing ACL reconstruction. In this case, the strengthening of the hamstring and quadriceps muscles may be an important element in protecting the autograft from the risk of re-rupture during the gait cycle, with this being an activity that is permitted from day 0 in patients undergoing cruciate ligament reconstruction.
5. Conclusions
The actual need for surgical reconstruction of an injured anterior cruciate ligament is still a matter of debate for the scientific community. On the one hand, the ACL seems to be an essential structure that contrasts the anterior displacement of the tibia and sustains remarkable loads; on the other hand, it seems to be not so relevant in that it can be sacrificed in the total knee arthroplasty without any serious disadvantage. Nevertheless, to our best knowledge, the knee kinematics during walking resulting from the ACL sacrifice and the effects of quadriceps and hamstrings activity have never been quantified. Above all, our dynamic simulations provided a step forward in the understanding and quantification of the effects of ACL removal in terms of knee kinematics and ligament load redistribution: it appears that the MCL (superficial and deep) is the main passive stabilizer of the anterior translation of the tibia when the ACL is missing. Furthermore, thanks to the versatility of our musculoskeletal model, the compensation effects produced by the hamstrings and quadriceps in the ACL-deficient knee during walking were quantified and analyzed. Reducing the quadriceps activity (leading over time to partial atrophy) would allow for relieving all ligaments in general, except for the PCL, whereas, in the ACL-deficient knee, hamstring activity is crucial, not only to compensate for the absence of ACL in limiting the anterior tibial displacement but also to reduce the risk of MCL injury.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





