1. Introduction
Fixed orthodontic treatment is necessary in many types of dental anomalies. Positive aspects such as improved function, aesthetics, and self-esteem are also accompanied by side effects such as white spots, root resorption, pain (90% of cases), dental abrasions and microfractures, periodontal problems, and intra- and extra-oral lesions [
1]. Lately, aligners have been developed as a less visible, less irritating, easier to clean and more comfortable treatment than conventional fixed therapy. The characteristics of the forces transmitted by the aligners depend largely on the properties of the materials used, their thickness and profile complexity, the degree of activation, and the use of accessory elements. Thermoplastic devices made of thicker materials produce a higher force, and thinner ones a lower force [
2].
Nitric oxide (NO) is a pleiotropic biological mediator involved in intestinal motility, platelet aggregation and adhesion, bone tissue formation and destruction, apoptosis, neurotransmission, the regulation of vascular tone, and immunological functions [
3,
4]. It has a short in vivo half-life (a few seconds or less). Thus, levels of more stable metabolites such as nitrite (NO
2−) and nitrate (NO
3−) anions have been used for the indirect quantification of NO in biological fluids. Altered NO levels have been associated with septic status, sexual intercourse, infections, hypertension, exercise, type II diabetes mellitus, hypoxia, and cancer [
4,
5].
Since it is fat-soluble, NO is not stored but is synthesised de novo and diffuses freely across lipid membranes. NO has the potential to exert its effects on target cells through various mechanisms. For example, the NO-mediated activation of the enzyme guanylyl cyclase (GC) catalyses the formation of the secondary messenger 3′,5′-cyclic guanosine monophosphate (cGMP). cGMP is involved in several biological functions such as the regulation of smooth muscle contractility, cell survival, cell proliferation, axonal guidance, synapse plasticity, inflammation, and angiogenesis [
5].
Nitric oxide is also considered a regulator of bone response to mechanical stress as it mediates adaptive bone formation (increased levels reduce osteoclastic activity and vice versa) and the pathological effects of lipopolysaccharides (LPS), tumour necrosis factor (TNF), interleukin 1 (IL-1) and other cytokines; regulates leukocytes and epithelial cell adhesion; inhibits T cell proliferation; and enhances natural killer (NK) cell activity, among other immune-related processes [
6,
7].
Given that any local oral change involves oxidative stress, we hypothesised that salivary nitric oxide may be a specific and sensitive marker for changes produced by orthodontic appliances.
Saliva is easy to collect and store and contains high quality DNA. However, research on its usage for diagnostic purposes is still in its early stages, and progress is limited by the lack of strict study protocols that allow a direct comparison of results from several independent laboratories [
1].
The aim of the study is to quantify salivary NO levels by both rapid and specific methods and to demonstrate that it is a valid, specific, and sensitive biomarker for bone changes determined by the application of different types of braces. Moreover, the study aims to highlight the impact of fixed orthodontic equipment on the oxidative status of the oral cavity in comparison to thermoplastic aligners, as fixed bracers exert stronger forces and more friction on the oral soft tissue, which can cause inflammation, lesions, and a shift in the oxidative status of the oral cavity.
2. Material and Methods
2.1. Study Groups
We recruited 30 patients (
Table 1) and divided them into 3 groups: control group (C), consisting of 6 women and 4 men (aged 18–30 years, mean 25.6 years); metal braces group (M), consisting of 5 women and 5 men (aged 16–30 years, mean 26.8 years); and the aligners group (A), with 8 women and 2 men (aged 18–30 years, mean 25.4 years).
On the day of saliva sampling, the patients were asked not to brush their teeth with toothpaste (to avoid chemical interaction between saliva and toothpaste) and not to eat or drink water 30 min prior to sampling. All the patients were encouraged to maintain oral hygiene. After the fitting of dental braces, the patients were asked to use 500 mg of paracetamol in case of pain.
Written informed consent concerning saliva sampling and inclusion in the study was obtained in all cases. The study was approved by the Ovidius University Bioethics Committee in accordance with the principles of the Declaration of Helsinki (revised 2000, Edinburgh).
2.2. Application of Dental Braces
In the study, we used Micro Sprint metal braces produced by Forestadent Bernhard Förster GmbH (Pforzheim, Germany) and made of one-piece stainless steel. These braces are the smallest on the market and have a flat profile with no sharp edges to minimize the discomfort to the cheeks. All the springs initially used were 0.12 nickel-titanium (Ni-Ti), Alexander LTS shape produced by American Orthodontics (Murfreesboro, TN, USA). The composite (Enlight) and primer (Ortho Solo) were produced by Ormco (Orange, CA, USA). Briefly, the exposed dental crowns were dried, and a 37% phosphoric acid solution was applied for 30 s and then rinsed with distilled water. Brackets were applied according to the standard protocol.
In the case of aligners, prior impressions were made with Orthoprint alginate (Zhermack SpA, Rome, Italy). The material was prepared according to the manufacturer’s instructions, placed in prefabricated spoons, and inserted into the oral cavity with gentle pressure from posterior to anterior so that the alginate could flow into depressions and record details as faithfully as possible. After removal and inspection, the impressions were washed with water, disinfected, and sent to the technical laboratory to manufacture the model [
8]. The individualized aligners were produced by Scheu Dental GmbH (Am Burgberg, Germany) using polyethylene terephthalate glycol-copolyester, which meets the biocompatibility requirements for medical products.
2.3. Saliva Collection and Storage
Unstimulated saliva was collected in 4 time points: T0 before application; T1—at 2 weeks; T2—at 30 days; and T3—at 60 days after application. For saliva collection, patients rinsed the oral cavity with double distilled water; they were then asked to sit in a relaxed position with the head bent forward to promote fluid accumulation in the anterior part of the oral cavity. They were asked to swallow first, then for 5 min to spit into a tube-pan system without moving their tongue and cheeks. Each saliva sample was centrifuged immediately after collection at 14,000 rpm for 10 min, and the supernatant was transferred to sterile airtight tubes and stored without freeze–thaw cycles at −20 °C until analysis [
9].
2.4. Detection and Quantification of Nitric Oxide by ELISA
The Total Nitric Oxide and Nitrate/Nitrite Parameter Assay Kit (R&D Systems Inc., Minneapolis, MN, USA) was used for an accurate quantitative determination of nitric oxide in the collected saliva. The determination of nitric oxide concentration is based on the enzymatic conversion of nitrate to nitrite by nitrate reductase, followed by the colorimetric detection of nitrite secondary to the Griess reaction. Treatment of the nitrate-containing saliva with the Griess reagent forms a pink-red azo dye through a two-step diazotization reaction—the acidic NO
2− produced by a diazotizing agent reacts with sulfanilic acid to produce the diazonium ion, which reacts with N-(1-naphthyl)ethylenediamine in an azo coupling reaction to form the pink-red azo dye which absorbs light at 540–570 nm [
8,
9,
10].
The kit requires two testing stages because NO- has a very short half-life (less than 0.1 s) and cannot be identified as such. The first step involves the quantification of endogenous nitrite. In the second step, nitrate is converted to nitrite using nitrate reductase, thus, quantifying total nitrite. The difference between total nitrite and endogenous nitrite matches the nitrate concentration representing the NO- level.
Prior to analysis, saliva was prepared according to the manufacturer’s instructions, requiring double dilution with reagent diluent (1×). All reagents were brought to room temperature prior to use. Double distilled water was used for the reconstruction and dilution of the reagents to avoid contamination with nitrates or nitrites. After completing all the steps according to the kit instructions, the samples were analysed by spectrophotometry (T Tecan SunriseTM, Männedorf, Switzerland) to quantify NO.
2.5. Determination of Total and Inducible Nitrite
All reagents and standards were prepared according to the procedures outlined above. A total of 50 μL of reaction diluent (1X) was placed in blank wells. A total of 50 μL of the test sample was added to the blank wells, over which 25 μL of NADH and 25 μL of nitrate reductase were added. The resulting solutions were mixed thoroughly, covered with adhesive tape, and incubated at 37 °C for 30 min. After incubation, 50 μL of Griess Reagent I and 50 μL of Griess Reagent II were added to all wells, mixing by gently tapping the side of the plate. Afterwards, the plates were re-incubated for 10 min at room temperature. Finally, the absorbance of each well was read using a spectrophotometer equipped with a microplate reader (Tecan SunriseTM, Männedorf, Switzerland) at a wavelength of 540 nm.
2.6. Detection and Quantification of Nitric Oxide by Semi-Quantitative Method
A quick qualitative and semi-quantitative detection of salivary NO was performed with Nitric Oxide Saliva Test Strips (Berkeley, CA, USA) at similar time points for both the control and test groups: T0 before application; T1—at 2 weeks; T2—at 30 days; and T3—at 60 days. The strip was placed on the tongue for 10 s, folded and kept in contact for another 10 s. The result was compared with the colorimetric map available on the box for the semi-quantitative assessment (depleted, low, threshold, target, high). All the evaluations were carried out twice, with no differences between them.
2.7. Statistical Analysis
Microsoft Excel 360 software with Statistical Analysis Pack (Microsoft Corporation 2018) was used for the statistical evaluation. Endogenous nitrates were calculated by interpolation using the regression curve equation. The minimum accepted regression coefficient was 0.95 to ensure accurate mathematical interpolation. Total nitrates were calculated in a similar manner, and the concentration of inducible nitrates was computed as the difference between the total and endogenous nitrite concentration. Since the samples were diluted, the concentration was multiplied by the dilution factor.
The results were expressed as mean ± standard deviation. The mean values were compared using the ANOVA test. The Pearson correlation test was used to identify potential correlations between the analysed variables. A p-value < 0.05 was considered statistically significant.
4. Discussions
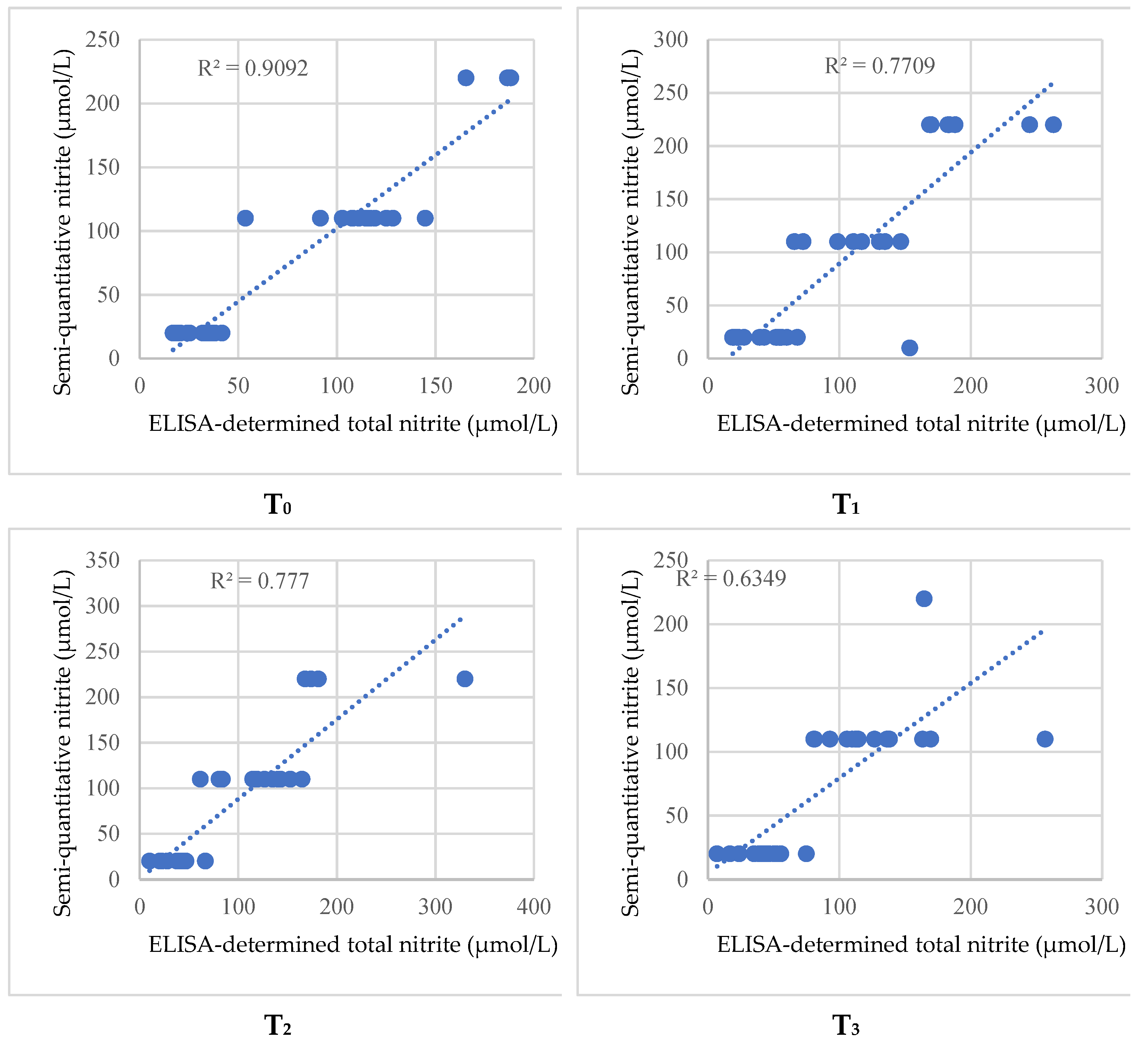
In our study, the rapid test showed an increase in total nitrite in metal appliance wearers similar to ELISA for both T1 and T2 moments, as demonstrated by the statistical analysis. Moreover, the total nitrite concentration determined by the two methods (ELISA and Nitric Oxide Saliva Test Strips) displayed a strong correlation at all time points and for all three groups, suggesting that rapid testing could be used in daily practice as a substitute for a more expensive and laborious method with similar results.
Oxidative stress determined by free radicals mainly affects the cellular lipid component and is the subject of current research, although results are conflicting. This study also found a difference between the inducible nitrate levels in the metal bracers sub-group, compared to the sub-group treated with thermoplastic aligners, suggesting a higher impact of the metallic bracers on the oral cavity oxidative status. Nitric oxide is a free radical that plays an important role as a regulator of various physiological and pathological mechanisms in the body. In the oral cavity, it may act as a non-specific antimicrobial defence system by inhibiting bacterial growth or by enhancing macrophage-mediated cytotoxicity. There are two main transformation mechanisms: reduction in the enzyme reductase, released by certain bacteria, which converts nitrate (NO
3−) to nitrite (NO
2−); or by facilitated reduction by certain bacterial products resulting from the microflora of dental plaque, forming nitric oxide and nitric acid (which ionises to NO
3−). Enzymatically, it can also be produced from L-arginine by nitric oxide synthase (NOS), which has three isoforms: neuronal NOS (nNOS; Type I, NOS−1); inducible NOS (iNOS; Type II, NOS-2), which is present in various cells and tissues and is produced by immunocompetent cells—such as macrophages infected by the bacteria involved in regulating inflammatory reactions; and endothelial NOS (eNOS; Type III, NOS-3), which is found in vascular endothelial cells [
11]. iNOS levels are significantly increased following tissue trauma (when cells are activated by external stimuli) and probably participates in the development of periodontal disease [
11].
Regarding NO levels, Ka et al. showed similar mean values in patients with different oral cancers compared to orthodontic fixed appliances wearers [
12]. Similarly, salivary NO levels in smokers are significantly higher than in non-smokers. In oral pathologies such as Behcet’s disease and recurrent aphthous stomatitis, the elevated salivary values may guide the clinician as to the degree of severity and reflect serum values [
11,
13].
According to Shama et al., nitric oxide levels do not show considerable changes during one year of wearing orthodontic fixed appliances. Alarcon et al. demonstrated increases in NO levels from day 7 to day 30 since treatment initiation. In our study, total, endogenous, and inducible nitrite concentrations were determined in patients with fixed metal appliances and aligners and compared to a control group. The results revealed a statistically significant increase in total and inducible nitrite in the case of fixed metal appliances, compared to aligners and the control group. This elevation can be considered a physiological response to the presence of foreign bodies in the oral cavity [
14,
15]. A potential mechanism for the rise in inducible nitrates in the metal brackets sub-group is the interplay between the metal ions released by the device, and endogenous and bacterial metabolites that can lead to the formation of free radicals [
16]. Furthermore, metal brackets have a more rigid and retentive surface that comes into intimate contact with oral soft tissues such as the cheeks, which can lead to the interaction of metal ions with surrounding cells, which, in turn, can lead to inflammation. Moreover, the normal movement of the oral cavity causes friction between the hard and irregular surface of the metal brackets, which can cause microlesions that can then cause an increase in oxidative stress and the production of free radicals [
16]. Finally, during sleeping hours, both types of devices come into intimate contact with the oral mucosa, being pressed into it by the normal sleeping position. While the thermoplastic aligners have a smooth and regulated surface that is better tolerated by the oral mucosa, the metallic brackets can cause mechanical lesions to the mucosa that, ultimately, lead to inflammation. Aligner wearers registered similar values compared to the control group except for a non-significant increase in the inducible nitrite. Since inducible nitrite is a quantification of free radicals and, thus, a measure of oxidative stress [
17], the results suggest the minimal invasiveness of aligner devices when compared to fixed metal devices. The level of oxidative stress expressed by the level of inducible nitrite returns to values close to baseline after a period of 60 days for both treatments.
Research investigating rapid nitrite quantification identified a positive correlation with salivary flow and caries incidence, especially in patients with high levels of daily stress [
18,
19].
A recent study assessed thermoplastic aligners that have self-ligating brackets with low friction and force exertion, regarding the oxidative stress of the oral cavity. The authors evaluated the patients at 30 and 90 days of treatment and highlighted an increase in oxidative stress in the first 30 days of treatment, followed by a return to base values after 90 days. The authors concluded that both methods impact salivary oxidative status similarly and note the importance of friction and other forces exerted on the saliva oxidative status [
20].
Another recent study assessed the manifestation of oxidative stress in patients treated with fixed metallic appliances. The authors measured ROS in the patients’ blood and the antioxidant defence (AD) and found that orthodontic treatments with fixed metal appliances can induce short-term systemic oxidative stress. This study highlights that fixed metallic appliances can cause microlesions that can lead to the formation of free radicals and shows that the shift of the oxidative status is traceable in other bodily fluids [
21]. As microlesions form, there is a shift in the oxidative status of the oral cavity which favours the release of oxygen and nitrogen reactive species. As this phenomenon continues in time, it is possible that the oxidative status shift can be detected in other body fluids [
21]. Additionally, metal brackets are also known to release nickel [
22] and chromium [
23]. This phenomenon further contributes to the shift of the oxidative status towards the formation of free radicals, further impacting all oxygen and nitrogen reactive species levels.
The alternatives to orthodontic treatment with vestibular appliances (those used in research) and aligners are the lingual technique and the self-ligation system. They also involve appliances with brackets bonded to the tooth using different mechanisms. We consider that aligners are the only real replacement of the classic system.
Limitations: A nitrate-rich diet together with the activity of commensal nitrate-reducing bacteria also increase salivary nitrate/nitrite levels by excretion or local production. The confounding effect of diet-derived nitrate could not be eliminated, as none of the patients followed a low-nitrate diet prior to saliva sampling. The small sample size was another limiting factor, as well as the overall lack of high-quality clinical trials working with saliva for the quantification of reactive oxygen and nitrogen species.
In our study, the rapid test showed an increase in total nitrite in metal appliances wearers similar to ELISA for both the T1 and T2 moments, as demonstrated by the statistical analysis. Moreover, total nitrite concentration determined by the two methods (ELISA and Nitric Oxide Saliva Test Strips) displayed a strong correlation at all time points and for all three groups, suggesting that rapid testing could be used in daily practice as a substitute to a more expensive and laborious method with similar results.



 ,
, 

{kind=link}