
Multifactorial Model Based on DWI-Radiomics to Determine HPV Status in Oropharyngeal Squamous Cell Carcinoma

 , , and
, , and
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. HPV Testing
2.3. MRI Acquisition Protocol
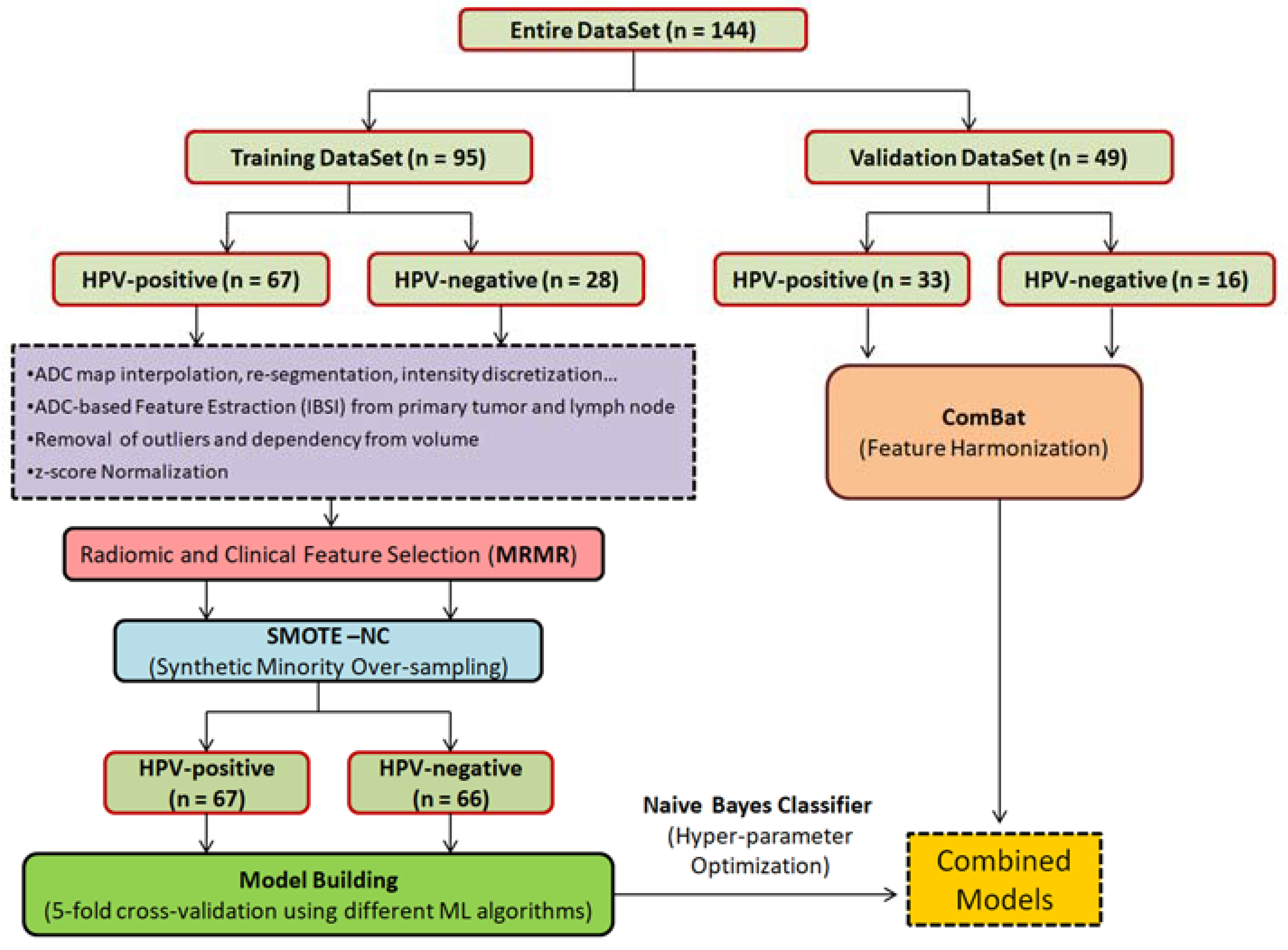
2.4. Image and Feature Processing
2.5. Machine Learning Modelling
3. Results
3.1. Patient Population
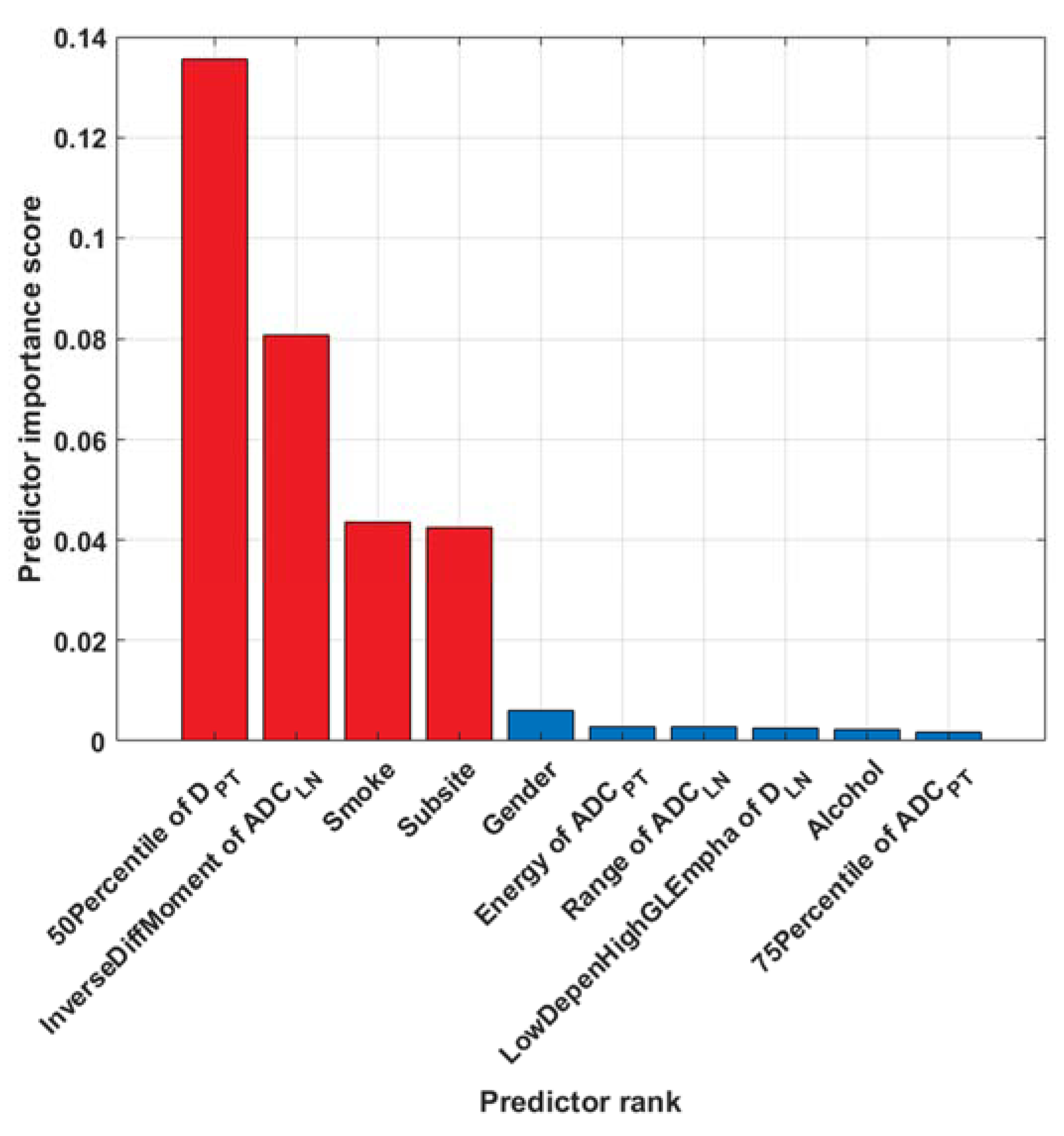
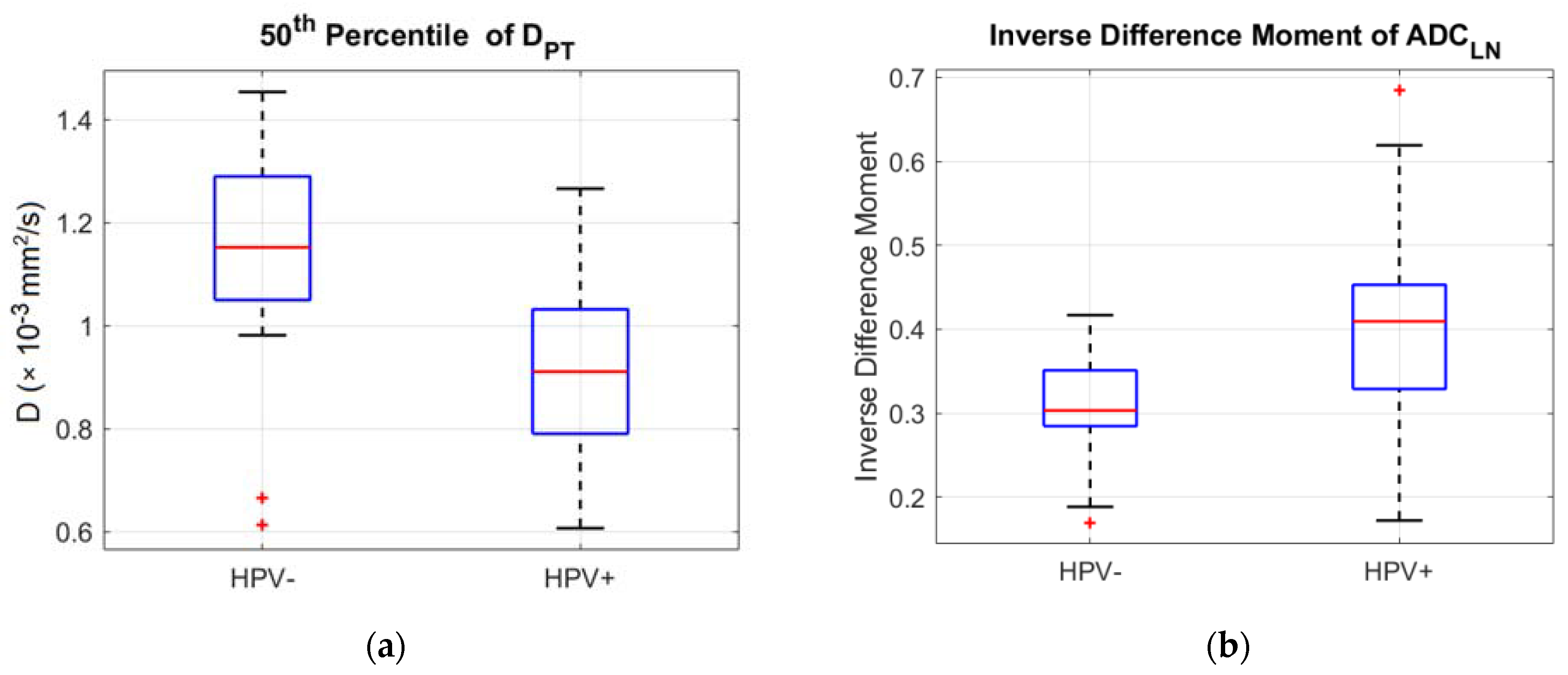
3.2. Machine Learning Modelling
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spiotto, M.T.; Taniguchi, C.M.; Klopp, A.H.; Colbert, L.E.; Lin, S.H.; Wang, L.; Frederick, M.J.; Osman, A.A.; Pickering, C.R.; Frank, S.J. Biology of the Radio- and Chemo-Responsiveness in HPV Malignancies. Semin. Radiat. Oncol. 2021, 31, 274–285. [Google Scholar] [CrossRef]
- O’Sullivan, B.; Lydiatt, W.M.; Haughey, B.H.; Brandwein-Gensler, M.; Glastonbury, C.M.; Shah, J.P.; Amin, M.B.; Edge, S.; Greene, F. HPV-mediated (p16+) oropharyngeal cancer. In AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017; pp. 113–121. [Google Scholar]
- Craig, S.G.; Anderson, L.A.; Schache, A.G.; Moran, A.G.; Graham, L.; Currie, K.; Rooney, K.; Robinso, M.; Upile, N.S.; Brooker, R.; et al. Recommendations for determining HPV status in patients with oropharyngeal cancers under TNM8 guidelines: A two-tier approach. Br. J. Cancer 2019, 120, 827–833. [Google Scholar] [CrossRef] [Green Version]
- Parvathaneni, U.; Lavertu, P.; Gibson, M.K.; Glastonbury, C.M. Advances in Diagnosis and Multi-disciplinary Management of Oro-pharyngeal Squamous Cell Carci-noma. State Art. Radiogr. 2019, 39, 2055–2068. [Google Scholar] [CrossRef]
- Vishwanath, V.; Jafarieh, S.; Rembielak, A. Imaging at Diagnosis Impacts Cancer Specific Survival of Patients with Cancer of the Oropharynx. Cancer 2019, 125, 2794–2802. [Google Scholar]
- Jansen, J.F.A.; Parra, C.; Lu, Y.; Shukla-Dave, A. Evaluation of head and neck tumors with functional MR imaging. Magn. Reson. Imaging. Clin. N. Am. 2016, 24, 123–133. [Google Scholar] [CrossRef] [Green Version]
- Erickson, B.J.; Korfiatis, P.; Akkus, Z.; Kline, T.L. Machine Learning for Medical Imaging. Radiographics 2017, 37, 505–515. [Google Scholar] [CrossRef]
- Giraud, P.; Giraud, P.; Gasnier, A.; El Ayachy, R.; Kreps, S.; Foy, J.P.; Durdux, C.; Huguet, F.; Burgun, A.; Bibault, J.E. Radiomics and Machine Learning for Radiotherapy in Head and Neck Cancers. Front. Oncol. 2019, 9, 174. [Google Scholar] [CrossRef] [Green Version]
- Yuan, Y.; Ren, J.; Shi, Y.; Tao, X. MRI-based radiomic signature as predictive marker for patients with head and neck squamous cell carcinoma. Eur. J. Radiol. 2019, 117, 193–198. [Google Scholar] [CrossRef]
- Haider, S.P.; Mahajan, A.; Zeevi, T.; Baumeister, P.; Reichel, C.; Sharaf, K.; Forghani, R.; Kucukkaya, A.S.; Kann, B.H.; Judson, B.L.; et al. PET/CT radiomics signature of human papilloma virus association in oropharyngeal squamous cell carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2978–2991. [Google Scholar] [CrossRef]
- Tanadini-Lang, S.; Balermpas, P.; Guckenberger, M.; Pavic, M.; Riesterer, O.; Vuong, D.; Bogowicz, M. Radiomic biomarkers for head and neck squamous cell carcinoma. Strahlenther. Onkol. 2020, 196, 868–878. [Google Scholar] [CrossRef]
- Salzillo, T.C.; Taku, N.; Wahid, K.A.; McDonald, B.A.; Wang, J.; van Dijk, L.V.; Rigert, J.M.; Mohamed, A.S.R.; Wang, J.; Lai, S.Y.; et al. Advances in Imaging for HPV-Related Oropharyngeal Cancer: Applications to Radiation Oncology. Semin. Radiat. Oncol. 2021, 31, 371–388. [Google Scholar] [CrossRef]
- Yu, K.; Zhang, Y.; Yu, Y.; Huang, C.; Liu, R.; Li, T.; Yang, L.; Morris, J.S.; Baladandayuthapani, V.; Zhu, H. Radiomic analysis in prediction of Human Papilloma Virus status. Clin. Transl. Radiat. Oncol. 2017, 7, 49–54. [Google Scholar] [CrossRef] [Green Version]
- Leijenaar, R.T.; Bogowicz, M.; Jochems, A.; Hoebers, F.J.; Wesseling, F.W.; Huang, S.H.; Chan, B.; Waldron, J.N.; O’Sullivan, B.; Rietveld, D.; et al. Development and validation of a radiomic signature to predict HPV (p16) status from standard CT imaging: A multicenter study. Br. J. Radiol. 2018, 91, 20170498. [Google Scholar] [CrossRef]
- Bagher-Ebadian, H.; Lu, M.; Siddiqui, F.; Ghanem, A.I.; Wen, N.; Wu, Q.; Liu, C.; Movsas, B.; Chetty, I.J. Application of radiomics for the prediction of HPV status for patients with head and neck cancers. Med. Phys. 2020, 47, 563–575. [Google Scholar] [CrossRef]
- Song, B.; Yang, K.; Garneau, J.; Lu, C.; Li, L.; Lee, J.; Stock, S.; Braman, N.M.; Koyuncu, C.F.; Toro, P.; et al. Radiomic Features Associated With HPV Status on Pretreatment Computed Tomography in Oropharyngeal Squamous Cell Carcinoma Inform Clinical Prognosis. Front. Oncol. 2021, 11, 744250. [Google Scholar] [CrossRef]
- Schouten, C.S.; de Graaf, P.; Bloemena, E.; Witte, B.I.; Braakhuis, B.J.; Brakenhoff, R.H.; Leemans, C.R.; Castelijns, J.A.; de Bree, R. Quantitative diffusion-weighted MRI parameters and human papillomavirus status in oropharyngeal squamous cell carcinoma. AJNR. Am. J. Neuroradiol. 2015, 36, 763–767. [Google Scholar] [CrossRef] [Green Version]
- Nakahira, M.; Saito, N.; Yamaguchi, H.; Kuba, K.; Sugasawa, M. Use of quantitative diffusion-weighted magnetic resonance imaging to predict human papilloma virus status in patients with oropharyngeal squamous cell carcinoma. Eur. Arch. Otorhinolaryngol. 2014, 271, 1219–1225. [Google Scholar] [CrossRef]
- Suh, C.H.; Lee, K.H.; Choi, Y.J.; Chung, S.R.; Baek, J.H.; Lee, J.H.; Yun, J.; Ham, S.; Kim, N. Oropharyngeal squamous cell carcinoma: Radiomic machine-learning classifiers from multiparametric MR images for determination of HPV infection status. Sci. Rep. 2020, 10, 17525. [Google Scholar] [CrossRef]
- Driessen, J.P.; van Bemmel, A.J.; van Kempen, P.M.; Janssen, L.M.; Terhaard, C.H.; Pameijer, F.A.; Willems, S.M.; Stegeman, I.; Grolman, W.; Philippens, M.E. Correlation of human papillomavirus status with apparent diffusion coefficient of diffusion-weighted MRI in head and neck squamous cell carcinomas. Head Neck. 2016, 38 (Suppl. 1), E613–E618. [Google Scholar] [CrossRef]
- Ward, M.J.; Thirdborough, S.M.; Mellows, T.; Riley, C.; Harris, S.; Suchak, K.; Webb, A.; Hampton, C.; Patel, N.N.; Randall, C.J.; et al. Tumour-infiltrating lymphocytes predict for outcome in HPV-positive oropharyngeal cancer. Br. J. Cancer. 2014, 110, 489–500. [Google Scholar] [CrossRef] [Green Version]
- Mena, M.; Taberna, M.; Tous, S.; Marquez, S.; Clavero, O.; Quiros, B.; Lloveras, B.; Alejo, M.; Leon, X.; Quer, M.; et al. Double Positivity for HPV-DNA/p16(Ink4a) is the Biomarker with Strongest Diagnostic Accuracy and Prognostic Value for Human Papillomavirus Related Oropharyngeal Cancer Patients. Oral. Oncol. 2018, 78, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Le Bihan, D.; Breton, E.; Lallemand, D.; Aubin, M.L.; Vignaud, J.; Laval-Jeantet, M. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology 1988, 168, 497–505. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging. 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Bettinelli, A.; Branchini, M.; De Monte, F.; Scaggion, A.; Paiusco, M. Technical Note: An IBEX adaption toward image biomarker standardization. Med. Phys. 2020, 47, 1167–1173. [Google Scholar] [CrossRef]
- Zhang, L.; Fried, D.V.; Fave, X.J.; Hunter, L.A.; Yang, J.; Court, L.E. Ibex: An open infrastructure software platform to facilitate collaborative work in radiomics. Med. Phys. 2015, 42, 1341–1353. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Leger, S.; Vallières, M.; Löck, S. Image biomarker standardisation initiative. arXiv 2020, arXiv:1612.07003. [Google Scholar]
- Park, B.W.; Kim, J.K.; Heo, C.; Park, K.J. Reliability of CT radiomic features reflecting tumour heterogeneity according to image quality and image processing parameters. Sci. Rep. 2020, 10, 3852. [Google Scholar] [CrossRef]
- Fortin, J.P.; Parker, D.; Tunç, B.; Watanabe, T.; Elliott, M.A.; Ruparel, K.; Roalf, D.R.; Satterthwaite, T.D.; Gur, R.C.; Gur, R.E.; et al. Harmonization of multi-site diffusion tensor imaging data. Neuroimage 2017, 161, 149–170. [Google Scholar] [CrossRef]
- Haga, A.; Takahashi, W.; Aoki, S.; Nawa, K.; Yamashita, H.; Abe, O.; Nakagawa, K. Standardization of imaging features for radiomics analysis. J. Med. Investig. 2019, 66, 35–37. [Google Scholar] [CrossRef]
- Ding, C.; Peng, H. Minimum redundancy feature selection from microarray gene expression data. J. Bioinform. Comput. Biol. 2005, 3, 185–205. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority over-sampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Bos, P.; van den Brekel, M.W.M.; Gouw, Z.A.R.; Al-Mamgani, A.; Waktola, S.; Aerts, H.J.W.L.; Beets-Tan, R.G.H.; Castelijns, J.A.; Jasperse, B. Clinical variables and magnetic resonance imaging-based radiomics predict human papillomavirus status of oropharyngeal cancer. Head Neck 2021, 43, 485–495. [Google Scholar] [CrossRef]
- Ravanelli, M.; Grammatica, A.; Tononcelli, E.; Morello, R.; Leali, M.; Battocchio, S.; Agazzi, G.M.; Buglione di Monale, E.; Bastia, M.; Maroldi, R.; et al. Correlation between Human Papillomavirus Status and Quantitative MR Imaging Parameters including Diffusion-Weighted Imaging and Texture Features in Oropharyngeal Carcinoma. AJNR. Am. J. Neuroradiol. 2018, 39, 1878–1883. [Google Scholar] [CrossRef]
- Vidiri, A.; Marzi, S.; Gangemi, E.; Benevolo, M.; Rollo, F.; Farneti, A.; Marucci, L.; Spasiano, F.; Sperati, F.; Di Giuliano, F.; et al. Intravoxel incoherent motion diffusion-weighted imaging for oropharyngeal squamous cell carcinoma: Correlation with human papillomavirus Status. Eur. J. Radiol. 2019, 119, 108640. [Google Scholar] [CrossRef]
- Martens, R.M.; Koopman, T.; Lavini, C.; Ali, M.; Peeters, C.F.W.; Noij, D.P.; Zwezerijnen, G.; Marcus, J.T.; Vergeer, M.R.; Leemans, C.R.; et al. Multiparametric functional MRI and 18F-FDG-PET for survival prediction in patients with head and neck squamous cell carcinoma treated with (chemo)radiation. Eur. Radiol. 2021, 31, 616–628. [Google Scholar] [CrossRef]
- de Perrot, T.; Lenoir, V.; Domingo Ayllón, M.; Dulguerov, N.; Pusztaszeri, M.; Becker, M. Apparent Diffusion Coefficient Histograms of Human Papillomavirus-Positive and Human Papillomavirus-Negative Head and Neck Squamous Cell Carcinoma: Assessment of Tumor Heterogeneity and Comparison with Histopathology. AJNR. Am. J. Neuroradiol. 2017, 38, 2153–2160. [Google Scholar] [CrossRef] [Green Version]
- Noij, D.P.; Martens, R.M.; Marcus, J.T.; de Bree, R.; Leemans, C.R.; Castelijns, J.A.; de Jong, M.C.; de Graaf, P. Intravoxel incoherent motion magnetic resonance imaging in head and neck cancer: A systematic review of the diagnostic and prognostic value. Oral Oncol. 2017, 68, 81–91. [Google Scholar] [CrossRef]
- Sharma, S.J.; Wittekindt, C.; Knuth, J.; Steiner, D.; Wuerdemann, N.; Laur, M.; Kroll, T.; Wagner, S.; Klussmann, J.P. Intraindividual homogeneity of 18F-FDG PET/CT parameters in HPV-positive OPSCC. Oral Oncol. 2017, 73, 166–171. [Google Scholar] [CrossRef]
- Moons, K.G.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [Green Version]
- Scott-Wittenborn, N.; Fakhry, C. Epidemiology of HPV Related Malignancies. Semin. Radiat. Oncol. 2021, 31, 286–296. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient and Tumor Characteristics | HPV-Negative | HPV-Positive | ||
|---|---|---|---|---|
| (n = 28) | (n = 67) | p-Value * | ||
| n | n | |||
| Gender | Male | 26 (93%) | 50 (75%) | 0.051 |
| Female | 2 (7%) | 17 (25%) | ||
| Age (mean ± SD) | 66.4 ± 9.3 | 64.4 ± 9.3 | 0.334 | |
| Tumor subsite | Tonsil | 10 (36%) | 42 (63%) | 0.023 |
| Base of the tongue | 18 (64%) | 25 (37%) | ||
| T-stage | T1 | 4 (14.3%) | 8 (11.9%) | |
| T2 | 5 (17.9%) | 24 (35.8%) | ||
| T3 | 4 (14.3%) | 7 (10.4%) | ||
| T4 | - | 28 (41.8%) | ||
| T4a | 15 (53.6%) | - | ||
| N-stage | N0 | 5 (17.9%) | 7 (10.4%) | |
| N1 | 4 (14.3%) | 29 (43.3%) | ||
| N2 | 5 (17.9%) | 28 (41.8%) | ||
| N3 | 14 (50%) | 3 (4.5%) | ||
| Smoke | No | 7 (25%) | 33 (49.3%) | 0.009 |
| Moderate | 2 (7.1%) | 11 (16.4%) | ||
| Heavy | 18 (64.3%) | 23 (34.3%( | ||
| Unknown | 1 (3.6%) | - | ||
| Alcohol intake | No | 11 (39.3%) | 43 (64.2%) | 0.001 |
| Moderate | 4 (14.3%) | 18 (26.9%) | ||
| Heavy | 11 (39.3%) | 5 (7.4%) | ||
| Unknown | 2 (7.1%) | 1 (1.5%) | ||
| Patient and Tumor Characteristics | HPV-Negative | HPV-Positive | |
|---|---|---|---|
| (n = 16) | (n = 33) | ||
| n | n | ||
| Gender | Male | 14 (88%) | 29 (88%) |
| Female | 2 (12%) | 4 (12%) | |
| Age (mean ± SD) | 66.3 ± 8.8 | 61.8 ± 11.5 | |
| Tumor subsite | Tonsil | 7 (44%) | 20 (61%) |
| Base of the tongue | 9 (56%) | 13 (39%) | |
| T-stage | T1 | 1 (6%) | 4 (12%) |
| T2 | 3 (19%) | 14 (43%) | |
| T3 | 1 (6%) | 2 (6%) | |
| T4 | - | 13 (39%) | |
| T4a | 11 (69%) | - | |
| N-stage | N0 | 2 (12.5%) | 4 (12.1%) |
| N1 | 2 (12.5%) | 16 (48.5%) | |
| N2 | 4 (25%) | 12 (36.4%) | |
| N3 | 8 (50%) | 1 (3%) | |
| Smoke | No | 2 (12.5%) | 24 (72.7%) |
| Moderate | 3 (18.8%) | 3 (9.1%) | |
| Heavy | 9 (56.3%) | 5 (15.2%) | |
| Unknown | 2 (12.5%) | 1 (3%) | |
| Alcohol intake | No | 3 (18.8%) | 26 (78.8%) |
| Moderate | 6 (37.5%) | 5 (15.1%) | |
| Heavy | 5 (31.3%) | - | |
| Unknown | 2 (12.5%) | 2 (6.1%) | |
| Model | Selected Features | Accuracy (%) | Sensitivity (%) | Specificity (%) | AUC |
|---|---|---|---|---|---|
| 1 | 50th Percentile of DPT, Inverse Difference Moment of ADCLN, Smoke, Subsite, Gender, Energy of ADCPT | 92 [86, 96] | 91 [82, 97] | 94 [85, 98] | 0.95 [0.89, 0.97] |
| 67 [52, 80] | 73 [54, 87] | 56 [30, 80] | 0.67 [0.45, 0.83] | ||
| 2 | 50th Percentile of DPT, Inverse Difference Moment of ADCLN, Smoke, Subsite, Gender | 89 [82, 94] | 88 [78, 95] | 91 [81, 97] | 0.95 [0.88, 0.98] |
| 67 [52, 80] | 76 [58, 89] | 50 [25, 75] | 0.81 [0.62, 0.92] | ||
| 3 | 50th Percentile of DPT, Inverse Difference Moment of ADCLN, Smoke, Subsite | 88 [81, 93] | 87 [76, 94] | 91 [81, 97] | 0.94 [0.88, 0.97] |
| 69 [56, 82] | 79 [61, 91] | 50 [25, 75] | 0.78 [0.60, 0.90] | ||
| 4 | 50th Percentile of DPT, Inverse Difference Moment of ADCLN, Smoke | 86 [79, 91] | 85 [74, 93] | 88 [78, 95] | 0.92 [0.86, 0.96] |
| 73 [59, 85] | 85 [68, 95] | 50 [25, 75] | 0.79 [0.62, 0.90] | ||
| 5 | 50th Percentile of DPT, Inverse Difference Moment of ADCLN | 82 [75, 88] | 79 [67, 88] | 89 [79, 96] | 0.91 [0.84, 0.95] |
| 67 [52, 80] | 70 [51, 84] | 63 [35, 85] | 0.66 [0.51, 0.80] | ||
| 6 | Smoke, Subsite, Gender, Alcohol | 85 [78, 90] | 90 [80, 96] | 76 [63, 85] | 0.87 [0.79, 0.92] |
| 80 [66, 90] | 94 [80, 99] | 50 [25, 75] | 0.82 [0.64, 0.93] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marzi, S.; Piludu, F.; Avanzolini, I.; Muneroni, V.; Sanguineti, G.; Farneti, A.; D’Urso, P.; Benevolo, M.; Rollo, F.; Covello, R.; et al. Multifactorial Model Based on DWI-Radiomics to Determine HPV Status in Oropharyngeal Squamous Cell Carcinoma. Appl. Sci. 2022, 12, 7244. https://doi.org/10.3390/app12147244
Marzi S, Piludu F, Avanzolini I, Muneroni V, Sanguineti G, Farneti A, D’Urso P, Benevolo M, Rollo F, Covello R, et al. Multifactorial Model Based on DWI-Radiomics to Determine HPV Status in Oropharyngeal Squamous Cell Carcinoma. Applied Sciences. 2022; 12(14):7244. https://doi.org/10.3390/app12147244
Chicago/Turabian StyleMarzi, Simona, Francesca Piludu, Ilaria Avanzolini, Valerio Muneroni, Giuseppe Sanguineti, Alessia Farneti, Pasqualina D’Urso, Maria Benevolo, Francesca Rollo, Renato Covello, and et al. 2022. "Multifactorial Model Based on DWI-Radiomics to Determine HPV Status in Oropharyngeal Squamous Cell Carcinoma" Applied Sciences 12, no. 14: 7244. https://doi.org/10.3390/app12147244