
Association between IL-1A, IL-1B and IL-1RN Polymorphisms and Peri-Implantitis: A Systematic Review and Meta-Analysis

 ,
,  , ,
, ,
Abstract
:Feature Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
- P (Population)—Adult patients
- E (Exposure)—Genotype including selected polymorphisms of interleukin-1 and its antagonist
- C (Control)—Genotype not including selected polymorphisms of interleukin-1 and its antagonist
- O (Outcomes/Outcome)—Development of peri-implantitis
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Statistical Analysis
3. Results
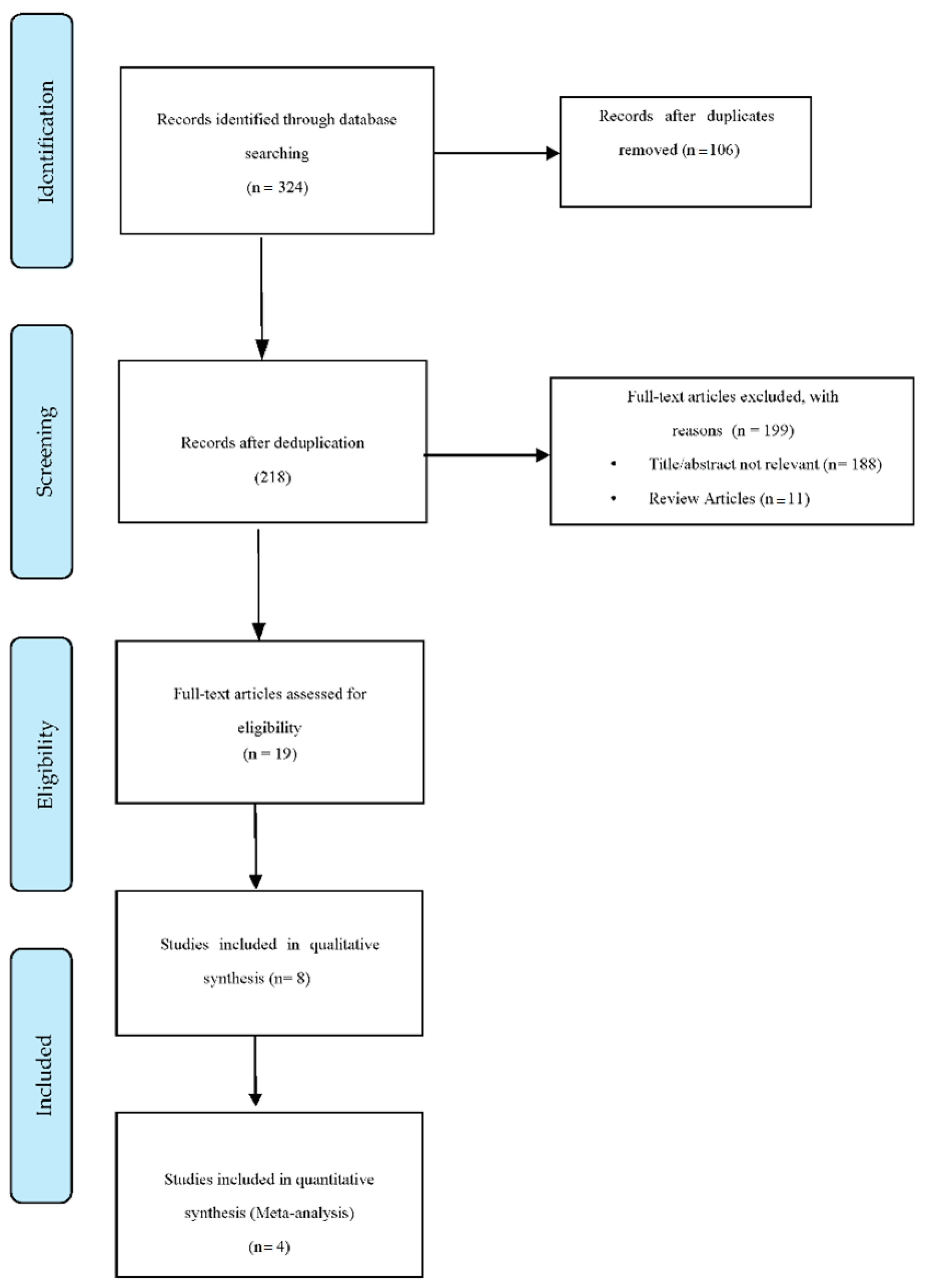
3.1. Study Selection
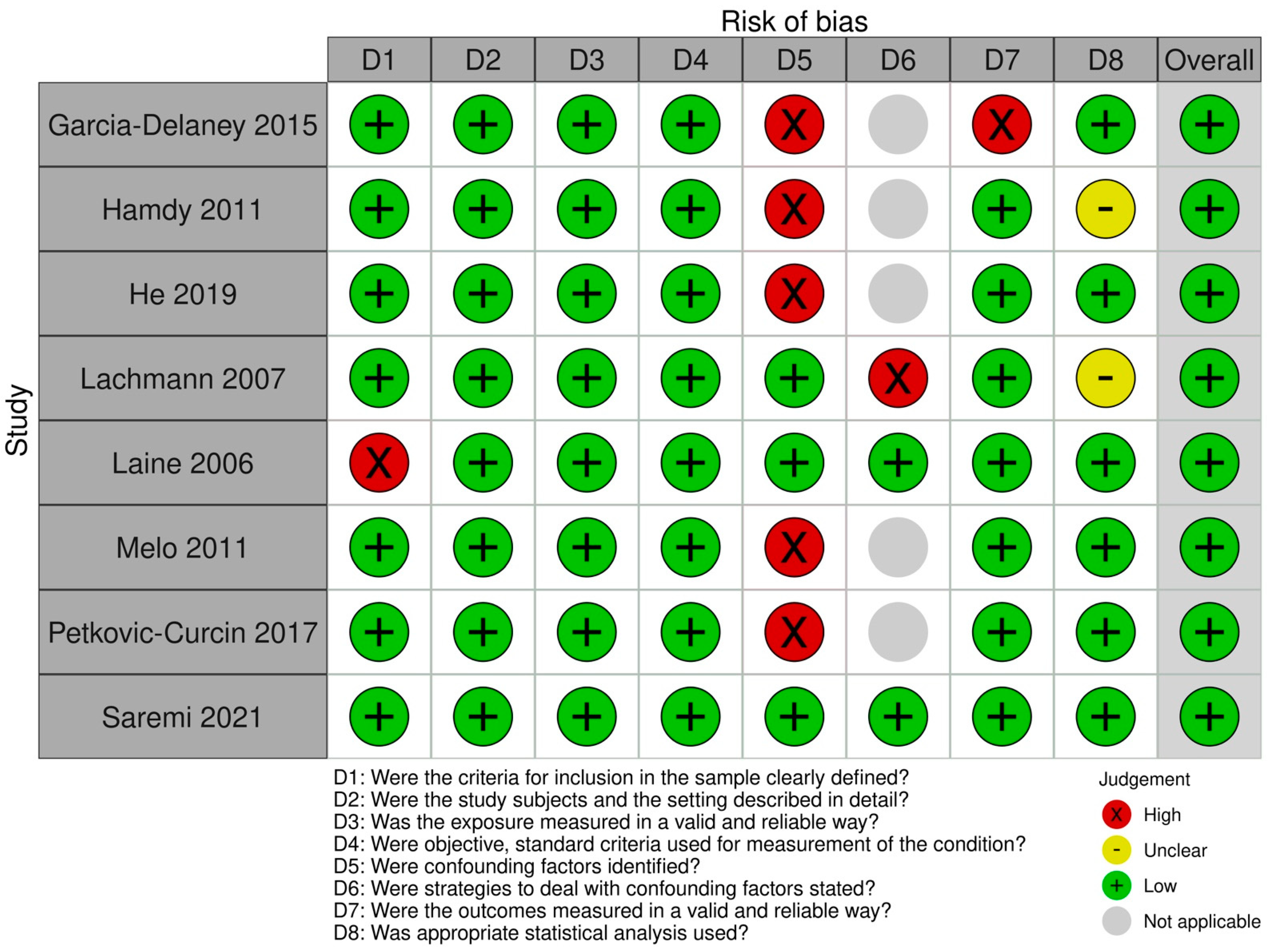
3.2. Results of the Bias Risk Assessment
3.3. Characteristics of the Studies
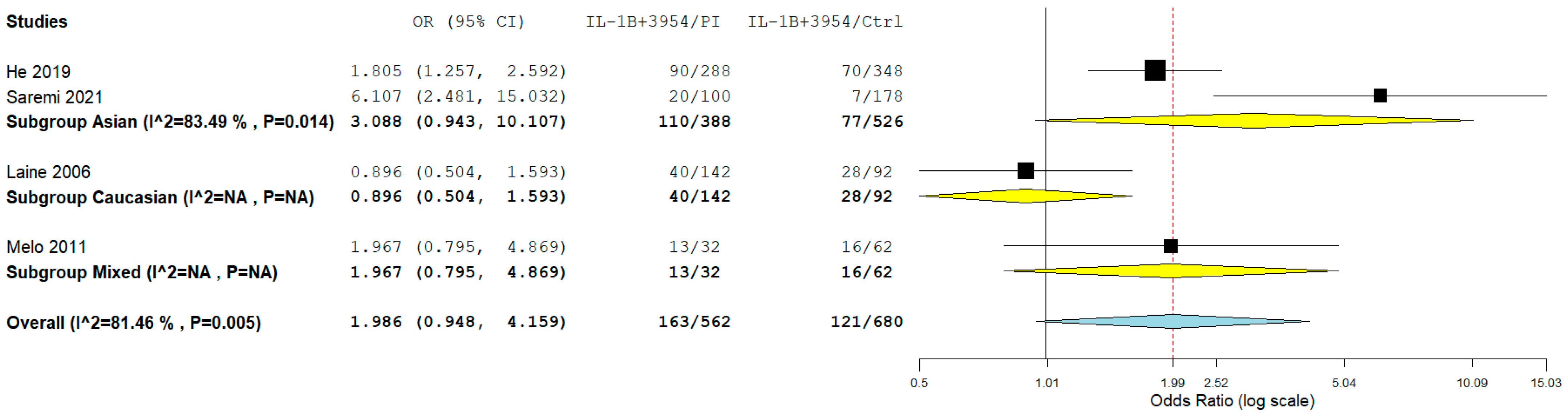
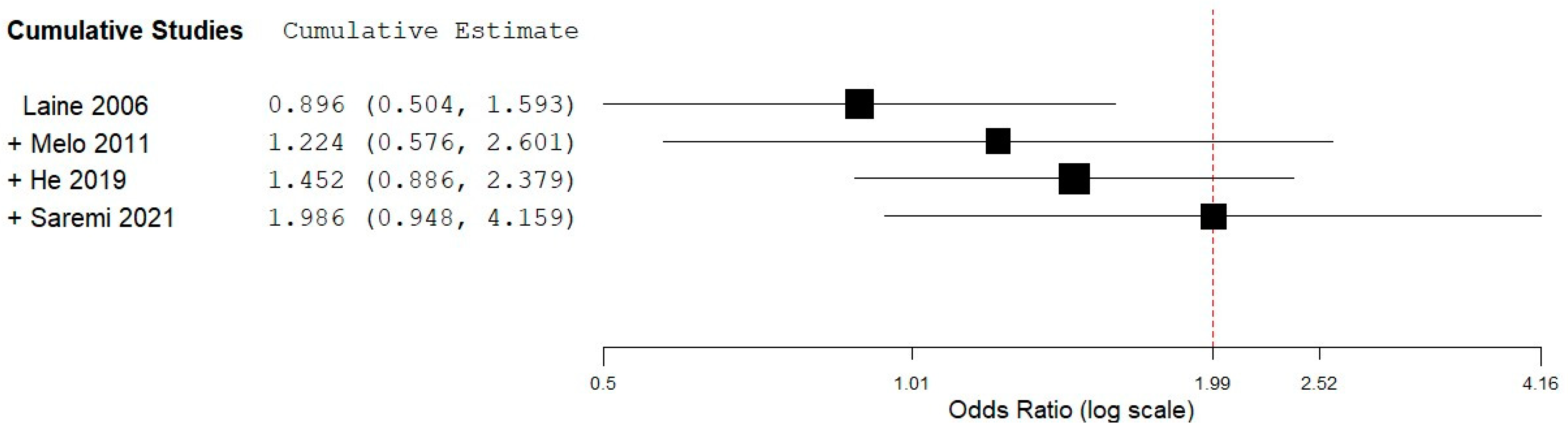
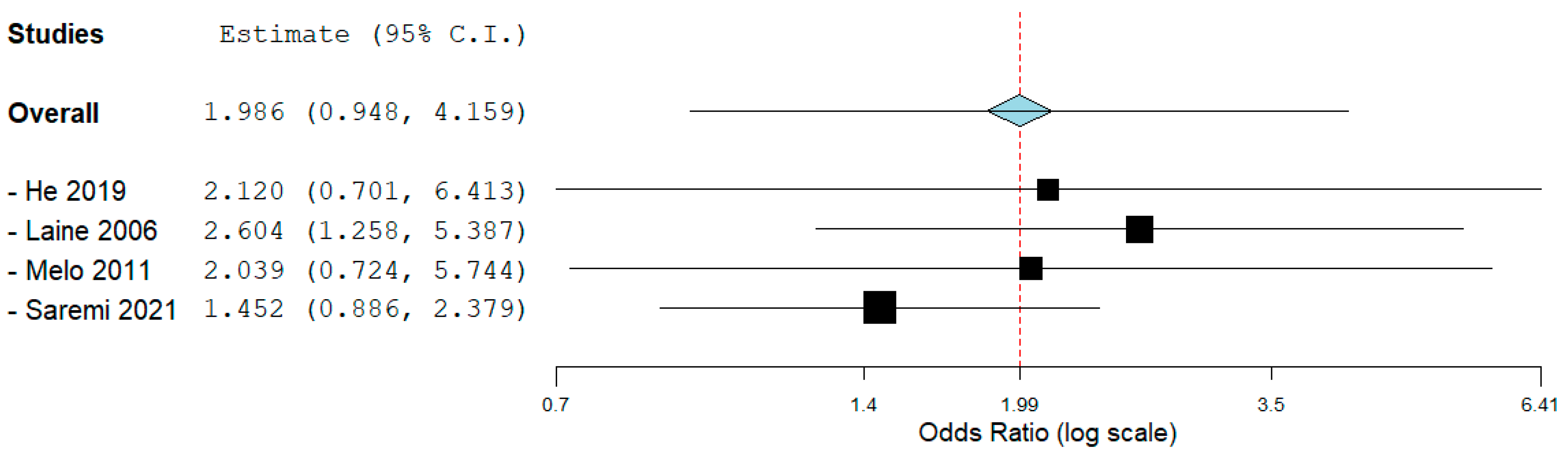
3.4. Meta-Analysis
3.5. Subgroup Analysis
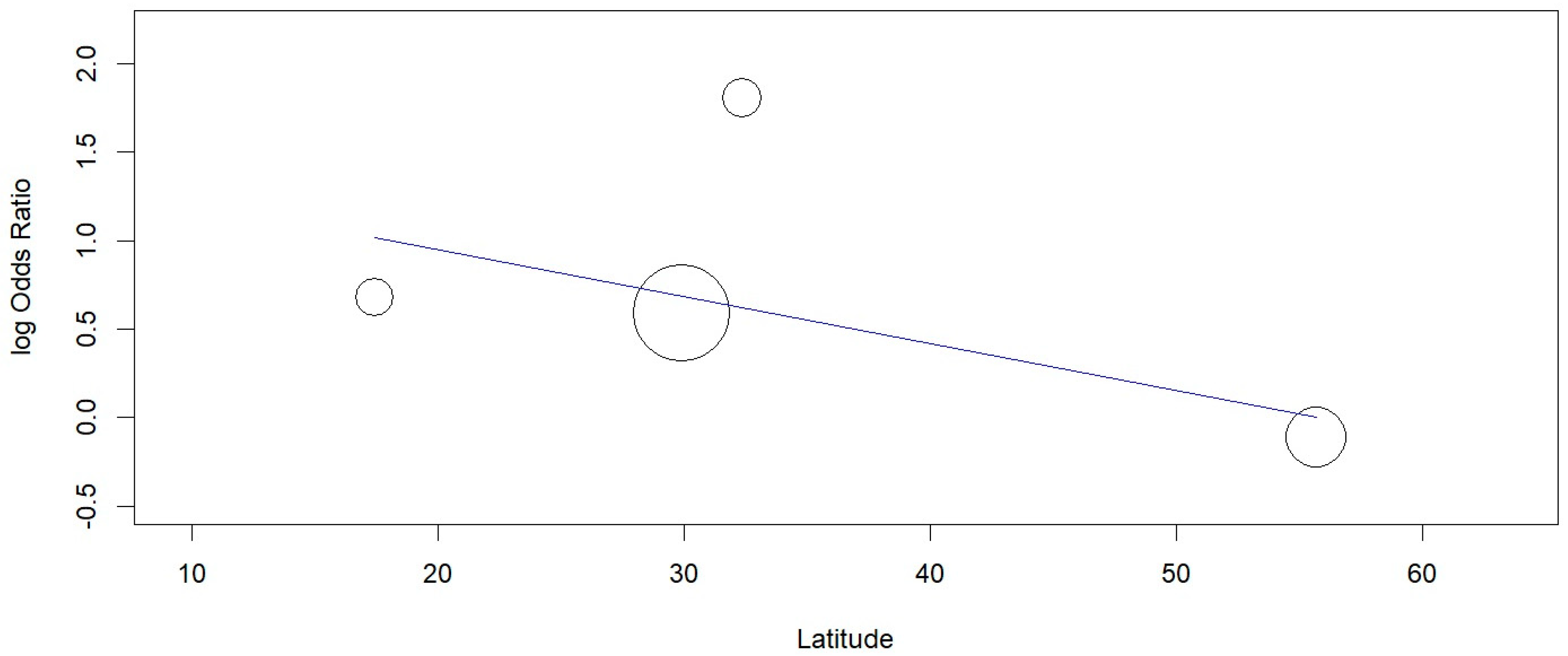
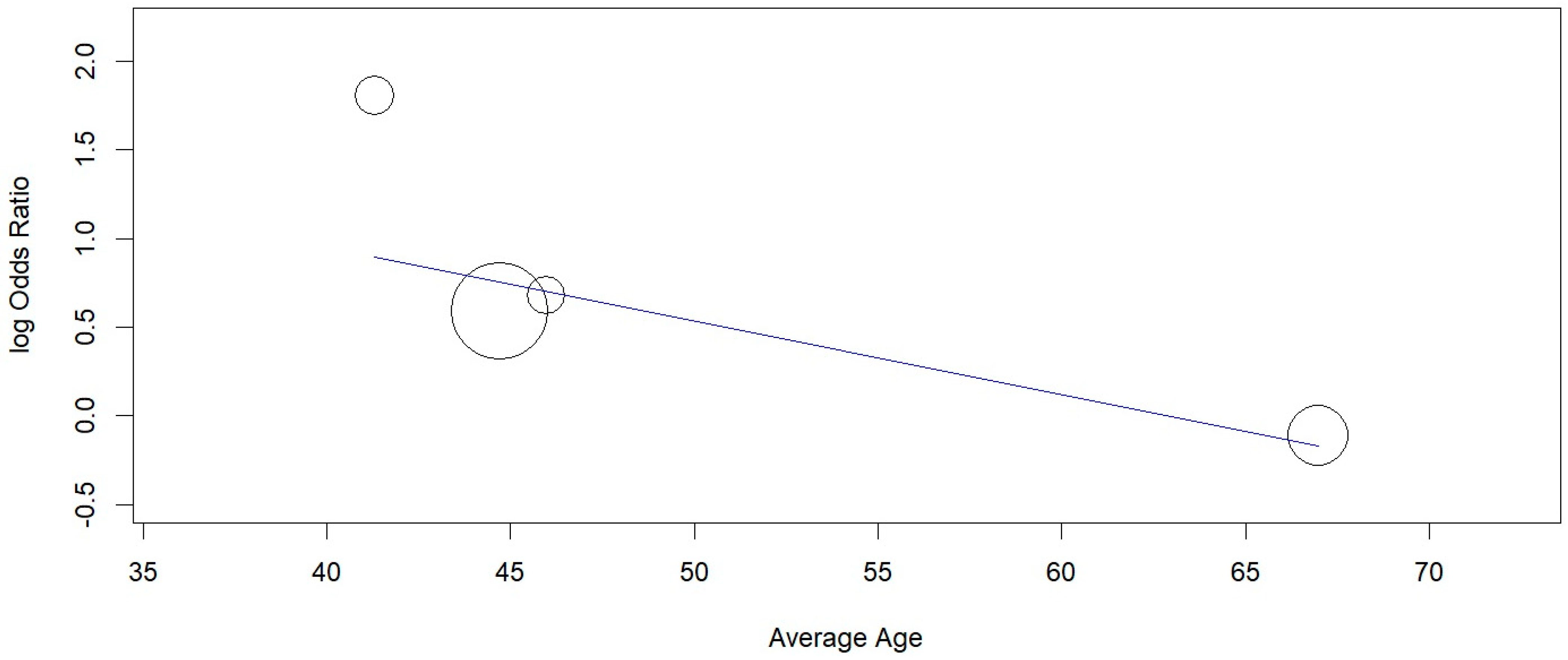
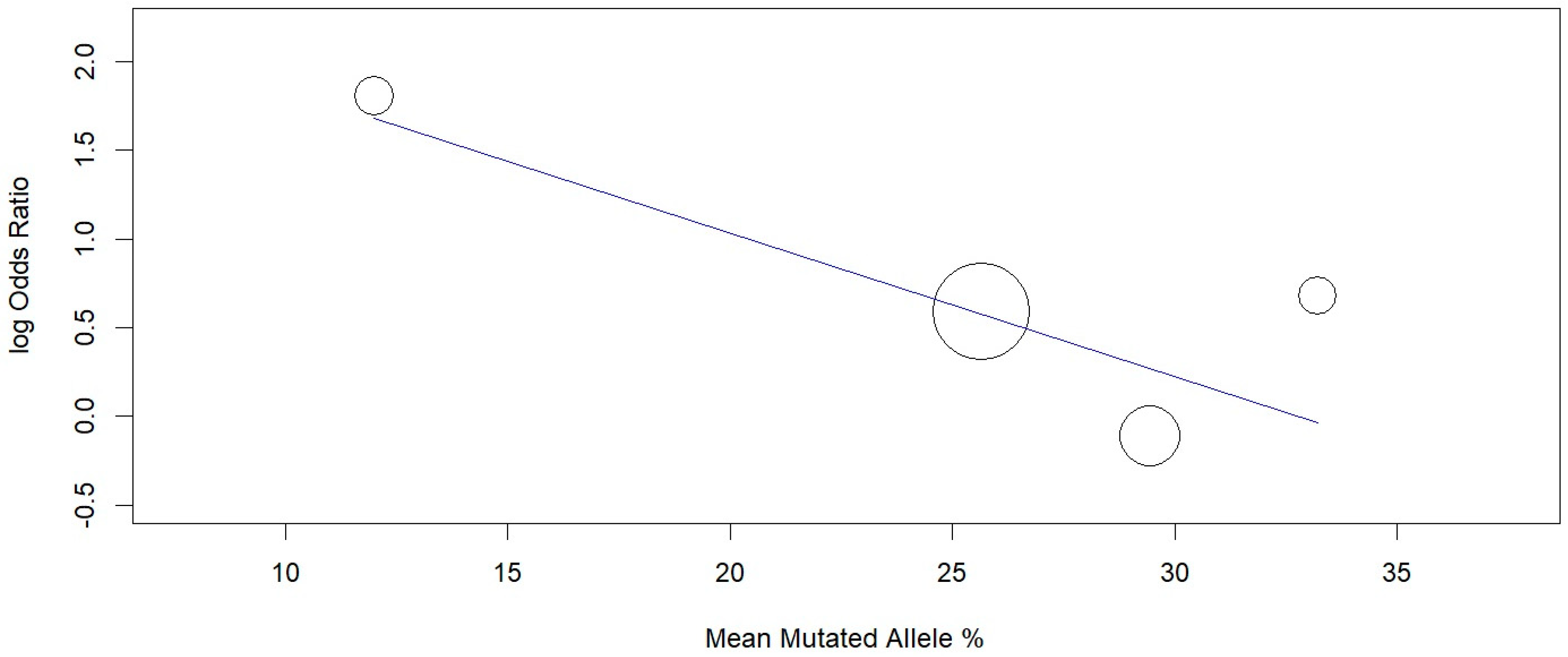
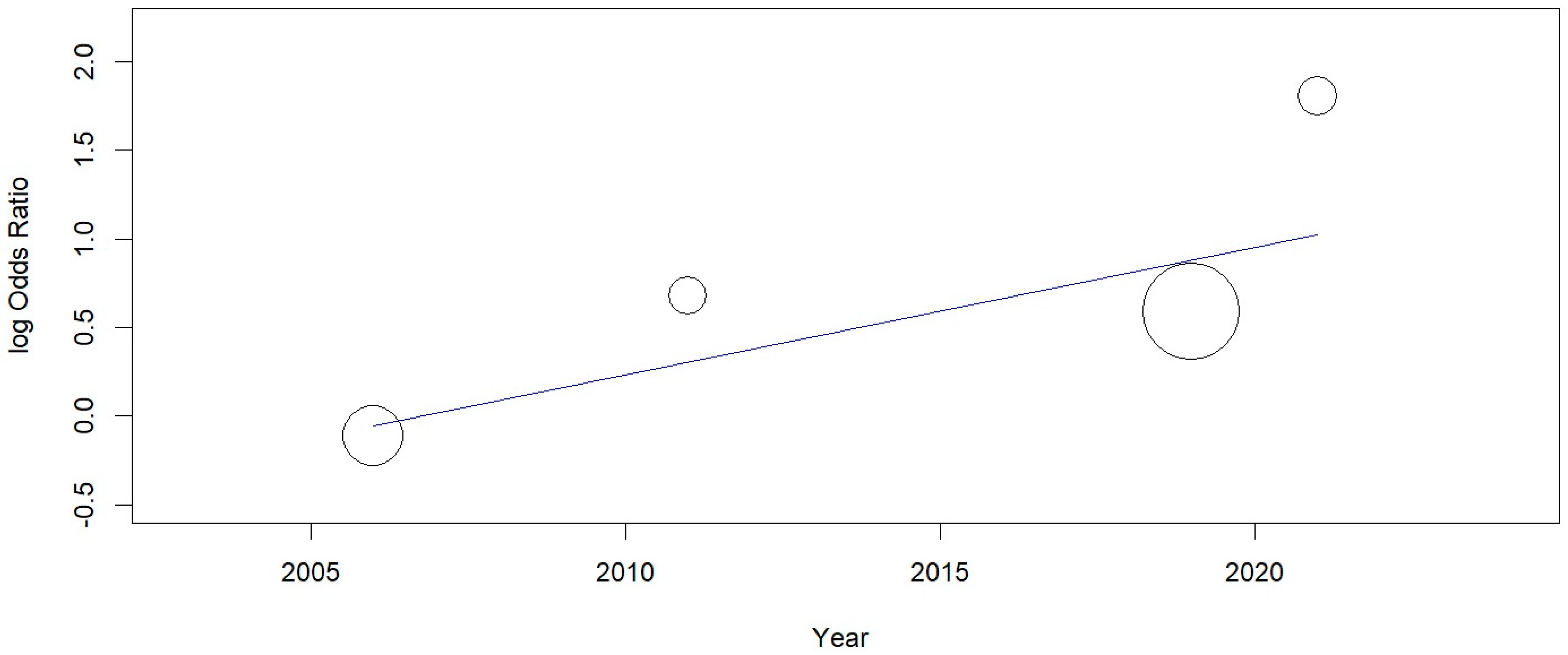
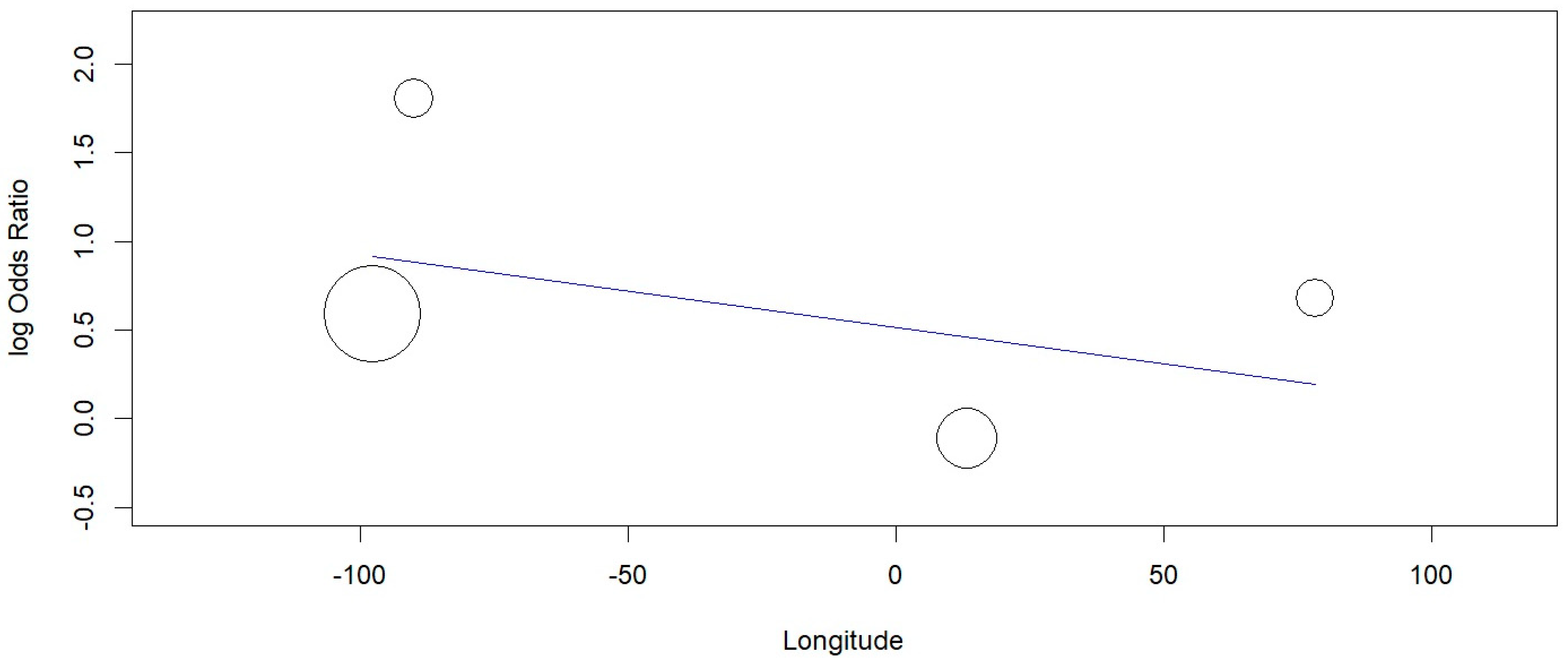
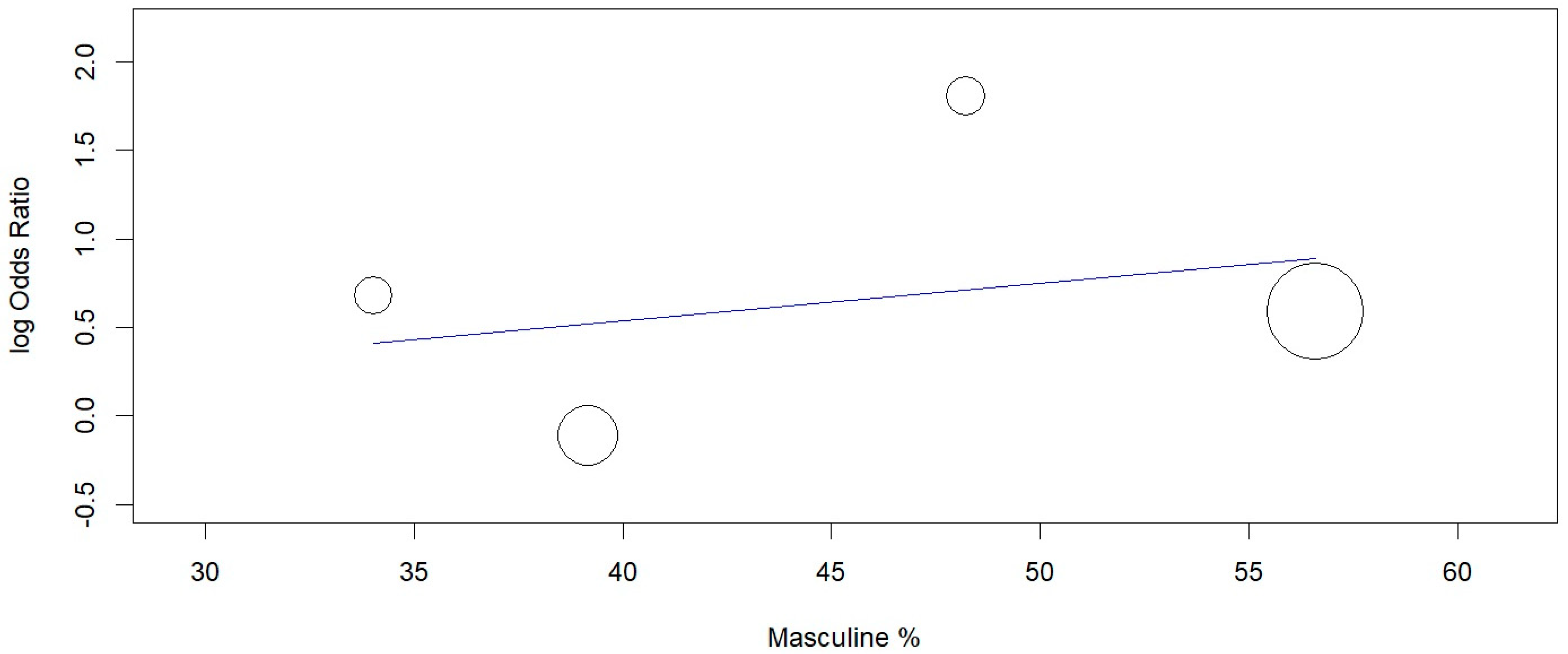
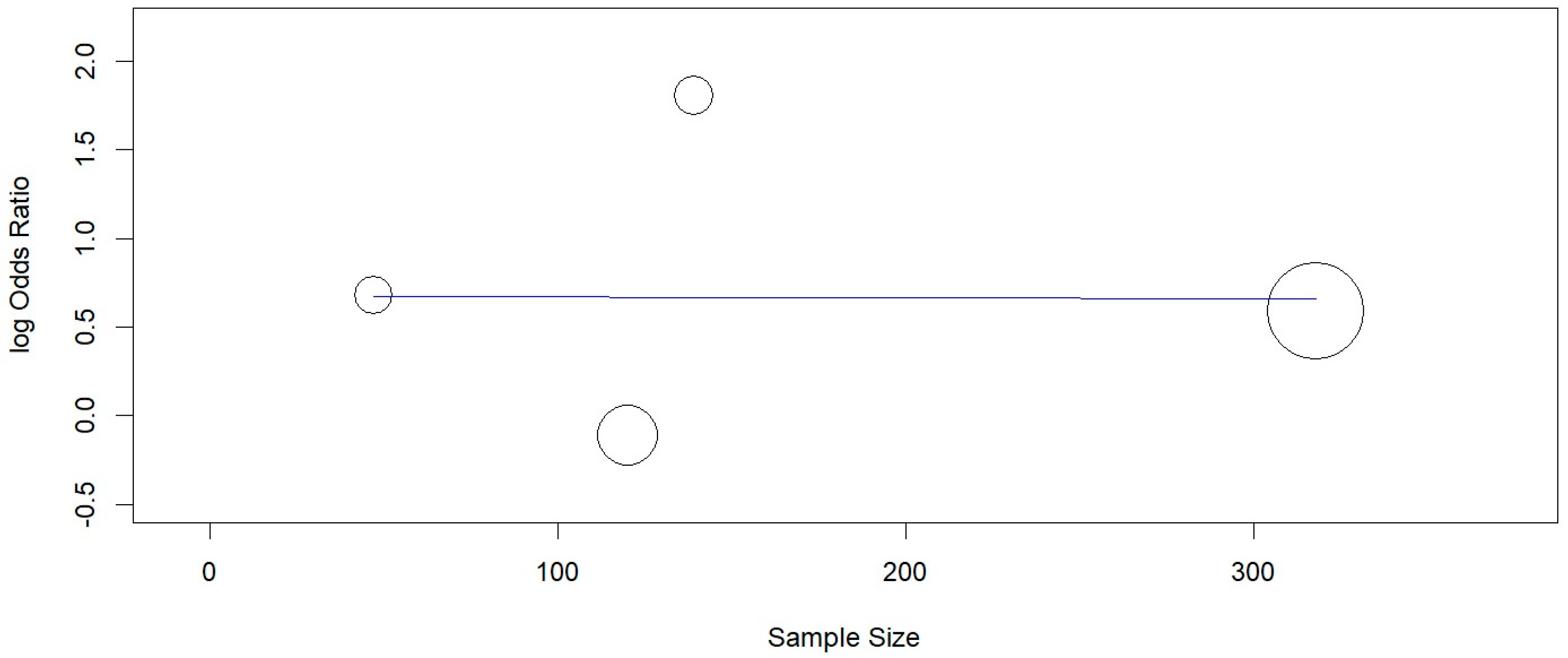
3.6. Meta-Regression
3.7. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year & Author | Latitude; Longitude (Degrees) | Sample Size | M/F (%) | Average Age of the Sample | Mean % of Mutated Allele |
|---|---|---|---|---|---|
| Garcia-Delaney, 2015 [33] | 32.363890; −86.298190 | Total: 54 PI: 27 Control: 27 | 37/63 | 53 | ND |
| Hamdy, 2011 [22] | −35.052770; 147.349560 | Total: 50 PI: 25 Control: 25 | 76/24 | 41 | ND |
| He, 2019 [24] | 29.894920; −97.677800 | Total: 318 PI: 144 Control: 174 | 57/43 | 45 | IL-1B +3954: 25.65 |
| Lachmann, 2007 [25] | −13.848923; −171.751145 | Total: 29 PI: 11 Control: 18 | 34/66 | 66 | ND |
| Laine, 2006 [21] | 55.702888; 13.194710 | Total: 120 PI: 71 Control: 49 | 39/61 | 67 | IL-1B +3954: 29.45 |
| Melo, 2011 [23] | 17.433660; 78.339010 | Total: 47 PI: 16 Control: 31 | 34/66 | 46 | IL-1B +3954: 33.22 |
| Petkovic-Curcin, 2017 [34] | 40.772770; −111.839100 | Total: 98 PI: 34 Control: 64 | 71/29 | 58 * | ND |
| Saremi, 2021 [26] | 32.331050; −90.170660 | Total: 139 PI: 50 Control: 89 | 49/51 | 41 | IL-1B +3954: 12 |
References
- Karoussis, I.K.; Kotsovilis, S.; Fourmousis, I. A comprehensive and critical review of dental implant prognosis in periodontally compromised partially edentulous patients. Clin. Oral Implant. Res. 2007, 18, 669–679. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Halbritter, S.; Harnisch, H.; Weber, H.P.; Buser, D. A retrospective analysis of patients referred for implant placement to a specialty clinic: Indications, surgical procedures, and early failures. Int. J. Oral Maxillofac. Implants 2008, 23, 1109–1116. [Google Scholar] [CrossRef] [PubMed]
- Tey, V.H.S.; Phillips, R.; Tan, K. Five-year retrospective study on success, survival and incidence of complications of single crowns supported by dental implants. Clin. Oral Implant. Res. 2017, 28, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Frizzera, F.; De Oliveira, G.J.P.L.; Shibli, J.A.; De Moraes, K.C.; Marcantonio, E.B.; Junior, E.M. Treatment of peri-implant soft tissue defects: A narrative review. Braz. Oral Res. 2019, 33, e073. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Berglundh, T.; Working Group 4 of Seventh European Workshop on Periodontology. Periimplant diseases: Where are we now?—Consensus of the Seventh European Workshop on Periodontology. J. Clin. Periodontol. 2011, 38, 178–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S286–S291. [Google Scholar] [CrossRef] [Green Version]
- Heitz-Mayfield, L.J.A. Peri-implant diseases: Diagnosis and risk indicators. J. Clin. Periodontol. 2008, 35 (Suppl. 8), 292–304. [Google Scholar] [CrossRef]
- Zitzmann, N.U.; Berglundh, T. Definition and prevalence of peri-implant diseases. J. Clin. Periodontol. 2008, 35, 286–291. [Google Scholar] [CrossRef]
- Atieh, M.A.; Alsabeeha, N.H.M.; Faggion, C.M., Jr.; Duncan, W.J. The Frequency of Peri-Implant Diseases: A Systematic Review and Meta-Analysis. J. Periodontol. 2013, 84, 1586–1598. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.-T.; Huang, Y.-W.; Zhu, L.; Weltman, R. Prevalences of peri-implantitis and peri-implant mucositis: Systematic review and meta-analysis. J. Dent. 2017, 62, 1–12. [Google Scholar] [CrossRef]
- Belibasakis, G.N. Microbiological and immuno-pathological aspects of peri-implant diseases. Arch. Oral Biol. 2014, 59, 66–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindhe, J.; Berglundh, T.; Ericsson, I.; Liljenberg, B.; Marinello, C. Experimental breakdown of peri-implant and periodontal tissues. A study in the beagle dog. Clin. Oral Implant. Res. 1992, 3, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.T.; Beck-Broichsitter, B.E.; Graetz, C.; Dmd, C.E.D.; Wiltfang, J.; Häsler, R. Peri-Implantitis versus Periodontitis: Functional Differences Indicated by Transcriptome Profiling. Clin. Implant Dent. Relat. Res. 2014, 16, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Fransson, C.; Lekholm, U.; Jemt, T.; Berglundh, T. Prevalence of subjects with progressive bone loss at implants. Clin. Oral Implant. Res. 2005, 16, 440–446. [Google Scholar] [CrossRef]
- Roos-Jansaker, A.-M.; Renvert, H.; Lindahl, C.; Renvert, S. Nine- to fourteen-year follow-up of implant treatment. Part III: Factors associated with peri-implant lesions. J. Clin. Periodontol. 2006, 33, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Tatakis, D.N. Interleukin-1 and bone metabolism: A review. J. Periodontol 1993, 64, 416–431. [Google Scholar]
- Nicklin, M.; Weith, A.; Duff, G.W. A Physical Map of the Region Encompassing the Human Interleukin-1α, Interleukin-1β, and Interleukin-1 Receptor Antagonist Genes. Genomics 1994, 19, 382–384. [Google Scholar] [CrossRef] [PubMed]
- Dinarello, C.A. Biologic basis for interleukin-1 in disease. Blood 1996, 87, 2095–2147. [Google Scholar] [CrossRef] [Green Version]
- Liao, J.; Li, C.; Wang, Y.; Ten, M.; Sun, X.; Tian, A.; Zhang, Q.; Liang, X. Meta-analysis of the association between common interleukin-1 polymorphisms and dental implant failure. Mol. Biol. Rep. 2014, 41, 2789–2798. [Google Scholar] [CrossRef]
- Dominici, R.; Cattaneo, M.; Malferrari, G.; Archi, D.; Mariani, C.; Grimaldi, L.; Biunno, I. Cloning and functional analysis of the allelic polymorphism in the transcription regulatory region of interleukin-1α. Immunogenetics 2002, 54, 82–86. [Google Scholar] [CrossRef]
- Laine, M.L.; Leonhardt, A.; Roos-Jansaker, A.-M.; Pena, A.S.; Van Winkelhoff, A.J.; Winkel, E.G.; Renvert, S. IL-1RN gene polymorphism is associated with peri-implantitis. Clin. Oral Implant. Res. 2006, 17, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Hamdy, A.A.; Ebrahem, M.A. The effect of interleukin-1 allele 2 genotype (IL-1a(-889) and IL-1b(+3954)) on the individual’s susceptibility to peri-implantitis: Case-control study. J. Oral Implant. 2011, 37, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Melo, R.F.; Lopes, B.M.V.; Shibli, J.A.; Junior, E.M.; Marcantonio, R.A.C.; Galli, G.M.T. Interleukin-1β and Interleukin-6 Expression and Gene Polymorphisms in Subjects with Peri-Implant Disease. Clin. Implant Dent. Relat. Res. 2012, 14, 905–914. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Jian, F.; He, T.; Tang, H.; Huang, B.; Wei, N. Analysis of the association of TNF-α, IL-1A, and IL-1B polymorphisms with peri-implantitis in a Chinese non-smoking population. Clin. Oral Investig. 2020, 24, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Lachmann, S.; Kimmerle-Müller, E.; Axmann, D.; Scheideler, L.; Weber, H.; Haas, R. Associations between peri-implant crevicular fluid volume, concentrations of crevicular inflammatory mediators, and composite IL-1A ?889 and IL-1B +3954 genotype: A cross-sectional study on implant recall patients with and without clinical signs of peri-implantitis. Clin. Oral Implant. Res. 2007, 18, 212–223. [Google Scholar] [CrossRef]
- Saremi, L.; Shafizadeh, M.; Esmaeilzadeh, E.; Ghaffari, M.E.; Mahdavi, M.H.; Amid, R.; Kadkhodazadeh, M. Assessment of IL-10, IL-1ß and TNF-α gene polymorphisms in patients with peri-implantitis and healthy controls. Mol. Biol. Rep. 2021, 48, 2285–2290. [Google Scholar] [CrossRef]
- Dereka, X.; Mardas, N.; Chin, S.; Petrie, A.; Donos, N. A systematic review on the association between genetic predisposition and dental implant biological complications. Clin. Oral Implant. Res. 2012, 23, 775–788. [Google Scholar] [CrossRef]
- Mohammadi, H.; Roochi, M.M.; Sadeghi, M.; Garajei, A.; Heidar, H.; Meybodi, A.A.; Dallband, M.; Mostafavi, S.; Mostafavi, M.; Salehi, M.; et al. Association between Interleukin-1 Polymorphisms and Susceptibility to Dental Peri-Implant Disease: A Meta-Analysis. Pathogens 2021, 10, 1600. [Google Scholar] [CrossRef]
- Jin, Q.; Teng, F.; Cheng, Z. Association between common polymorphisms in IL-1 and TNFα and risk of peri-implant disease: A meta-analysis. PLoS ONE 2021, 16, e0258138. [Google Scholar] [CrossRef]
- Lefebvre, C.; Glanville, J.; Briscoe, S.; Littlewood, A.; Marshall, C.; Metzendorf, M.-I.; Noel-Storr, A.; Rader, T.; Shokraneh, F.; Thomas, J.; et al. Chapter 4: Searching for and selecting studies. In Cochrane Handbook for Systematic Reviews of Intervention; Version 6.2.; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2019; Available online: www.training.cochrane.org/handbook (accessed on 2 April 2022).
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, SA, USA, 2017; Available online: https://reviewersmanual.joannabriggs.org/ (accessed on 2 April 2022).
- Wallace, B.C.; Dahabreh, I.J.; Trikalinos, T.A.; Lau, J.; Trow, P.; Schmid, C.H. Closing the Gap between Methodologists and End-Users: R as a Computational Back-End. J. Stat. Softw. 2012, 49, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Schünemann, H.J.; Vist, G.E.; Higgins, J.P.T.; Santesso, N.; Deeks, J.J.; Glasziou, P.; Akl, E.A.; Guyatt, G.H. Chapter 15: Interpreting results and drawing conclusions. In Cochrane Handbook for Systematic Reviews of Intervention; Version 6.2.; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2019; Available online: www.training.cochrane.org/handbook (accessed on 2 April 2022).
- Garcia-Delaney, C.; Sanchez-Garces, M.; Figueiredo, R.; Sánchez-Torres, A.; Escoda, C.G. Clinical significance of interleukin-1 genotype in smoking patients as a predictor of peri-implantitis: A case-control study. Med. Oral Patol. Oral Y Cir. Buccal 2015, 20, e737–e743. [Google Scholar] [CrossRef] [PubMed]
- Petkovic-Curcin, A.; Zeljic, K.; Cikota-Aleksic, B.; Dakovic, D.; Tatic, Z.; Magic, Z. Association of Cytokine Gene Polymorphism with Peri-implantitis Risk. Int. J. Oral Maxillofac. Implant. 2017, 3, e241–e248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cafiero, C.; Spagnuolo, G.; Marenzi, G.; Martuscelli, R.; Colamaio, M.; Leuci, S. Predictive Periodontitis: The Most Promising Salivary Biomarkers for Early Diagnosis of Periodontitis. J. Clin. Med. 2021, 10, 1488. [Google Scholar] [CrossRef] [PubMed]
- Huynh-Ba, G.; Lang, N.P.; Tonetti, M.S.; Zwahlen, M.; Salvi, G.E. Association of the compositeIL-1genotype with peri-implantitis: A systematic review. Clin. Oral Implant. Res. 2008, 19, 1154–1162. [Google Scholar] [CrossRef]
- Feloutzis, A.; Lang, N.P.; Tonetti, M.S.; Bürgin, W.; Brägger, U.; Buser, D.; Duff, G.W.; Kornman, K.S. IL-1 gene polymorphism and smoking as risk factors for peri-implant bone loss in a well-maintained population. Clin. Oral Implant. Res. 2003, 14, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Gruica, B.; Wang, H.-Y.; Lang, N.P.; Buser, D. Impact of IL-1 genotype and smoking status on the prognosis of osseointegrated implants. Clin. Oral Implant. Res. 2004, 15, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Kornman, K.S.; Crane, A.; Wang, H.-Y.; Giovlne, F.S.; Newman, M.G.; Pirk, F.W.; Wilson, T.G.; Higginbottom, F.L.; Duff, G.W. The interleukin-1 genotype as a severity factor in adult periodontal disease. J. Clin. Periodontol. 1997, 24, 72–77. [Google Scholar] [CrossRef]
- Armitage, G.C.; Wu, Y.; Wang, H.-Y.; Sorrell, J.; di Giovine, F.S.; Duff, G.W. Low Prevalence of a Periodontitis-Associated Interleukin-1 Composite Genotype in Individuals of Chinese Heritage. J. Periodontol. 2000, 71, 164–171. [Google Scholar] [CrossRef]
- Andreiotelli, M.; Koutayas, S.O.; Madianos, P.N.; Strub, J.R. Relationship between interleukin-1 genotype and peri-implantitis: A literature review. Quintessence Int. 2008, 39, 289–298. [Google Scholar]








| Year & Author | Type of Study | Polymorphisms Evaluated | Geographic Region | Inclusion Criteria | Exclusion Criteria | Smoking Habits | Time of Implant in Function (Months) | Outcome |
|---|---|---|---|---|---|---|---|---|
| Garcia-Delaney, 2015 [34] | Case-control | IL-1A −889 IL-1B +3954 IL-1RN +2018 | Spain | Systemically healthy patients; Peri-implantitis group: BOP or SUP (+); BL > 2 mm Control group: BOP (−); SUP (−); BL < 2 mm | - Cases with incomplete data or with dubious diagnosis | All smokers | ≥18 | IL-1 genotypes do not seem to be good predictors of peri-implantitis in the great majority of smoking patients. Furthermore, no synergic effect was found between IL-1 genotypes and heavy smokers. Patients with a previous history of periodontitis were more prone to peri-implantitis. |
| Hamdy, 2011 [22] | Case-control | IL-1A −889 IL-1B +3954 | Egypt | Systematically healthy patients; Peri-implantitis group: BOP (+); PPD > 4 mm; BL (+) | - Smokers; - History of antibiotic intake or periodontal treatment in previous 6 months | Non-smokers | ≥36 (implant placement) | The combination of the polymorphism in IL-1A −889 and IL-1B +3954, in patients with inflamed periodontal or peri-implant tissues, may act as a risk factor that increases tissue destruction. IL-1 gene polymorphism (IL-1A −889 and IL-1B +3954) may have a negative effect on treatment outcomes of peri-implantitis. |
| He, 2019 [24] | Case-control | IL-1A −889 IL-1B +3954 TNFα −308 | China | Peri-implantitis group: PPD ≥ 4 mm; BOP (+); GI (+); BL involving ≥ 2 threads compared to prosthetic placement Control group: Healthy peri-implant tissue; PPD < 3mm; BOP (−); BL (−) | - Smokers; - Pregnant or lactation; - General health problems (diabetes mellitus, HIV infection); - Intake of any antibiotics and anti-inflammatories in the last 3 months. | Non-smokers | ≥24 | The IL-1A −889 or IL-1B +3954 genetic polymorphisms were associated with the risk of peri-implantitis and periodontal status. |
| Lachmann, 2007 [25] | Case-control | IL-1A −889 IL-1B +3954 | Germany | - Systemic health in general; - Absence of medical conditions that compromise the immune system. Peri-implantitis group—PPD > 4 mm; BOP (+); BL (+) | ND | ND | ≥12 | The composite IL-1A −889 and IL-1B +3954 genotype investigated exerted only little influence on the peri-implant crevicular immune response, and this influence appeared to be of limited impact in sites with established peri-implantitis lesions. |
| Laine, 2006 [21] | Case-control | IL-1A −889 IL-1B +3954 IL-1B −511 IL-1RN (VNTR) | Sweden | Peri-implantitis group: BL involving ≥ 3 threads; BOP and/or SUP (+) | ND | Peri-implantitis group—76% smokers Control group—49% smokers | ≥24 | IL-1RN gene polymorphism is associated with peri-implantitis and may represent a risk factor for this disease. |
| Melo, 2011 [23] | Case-control | IL-1B +3954 IL-1B −511 IL-6 −174 | Brazil | - No medical history of chronic illness; - No history of antibiotic therapy or use of steroidal or AINE medications in the 6 months prior to the study. Control group: no mucosal bleeding, PD ≤ 4 mm, BOP and SUP (−) | - Smokers; - Pregnant or lactation; - Periodontitis | Non-smokers | ND | There was no correlation between the concentration of IL-1β and IL-6 in the crevicular sulcular fluid present in healthy or diseased osseointegrated implants in comparison with healthy teeth. The studied genetic polymorphisms had no influence on peri-implant disease. |
| Petkovic-Curcin, 2017 [35] | Case-control | IL-6 −174 IL-10 −1082 TNF-α −308 CD14 −159 IL-1RN (VNTR) | Serbia | Peri-implantitis group: PPD ≥ 4 mm, BOP +, GI (+); PI (+) and BL involving ≥ 2 threads compared to prosthetic replacement Control group: Healthy peri-implant tissue, BOP (−), PPD < 4 mm, BL (−) | ND | C—42% smokers PI—71% smoker | ≥24 | Smoking and the presence of TNFα-308 polymorphism may increase the risk for peri-implantitis, while CD14-159 polymorphism decreases the risk. The results also indicate significant association of CD14-159, TNFα-308, and IL6-174 genotypes and clinical parameters in the Serbian population. |
| Saremi, 2021 [26] | Case-control | IL-1B +3954 IL-10 −819 IL-10 −592 TNF-α −308 TNF-α −857 | Iran | - No history of periodontitis Peri-implantitis group: PPD > 5 mm; BOP (+) with or without SUP; BL ≥ 2 mm Control group: PPD < 4 mm; BL (−) | - Oral and periodontal diseases (except caries), - Current orthodontic treatment; - History of systemic diseases or any complication that compromises the immune system (diabetes, HIV, hepatitis, chemotherapy); - Pregnant or lactation | ND | ≥12 | Genetic polymorphisms of IL-10 −819, IL-10 −592 and IL-1B +3954 may play a role in the pathogenesis of peri-implantitis and increase its risk of occurrence. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardoso, J.M.; Duarte, S.; Ribeiro, A.C.; Mascarenhas, P.; Noronha, S.; Alves, R.C. Association between IL-1A, IL-1B and IL-1RN Polymorphisms and Peri-Implantitis: A Systematic Review and Meta-Analysis. Appl. Sci. 2022, 12, 6958. https://doi.org/10.3390/app12146958
Cardoso JM, Duarte S, Ribeiro AC, Mascarenhas P, Noronha S, Alves RC. Association between IL-1A, IL-1B and IL-1RN Polymorphisms and Peri-Implantitis: A Systematic Review and Meta-Analysis. Applied Sciences. 2022; 12(14):6958. https://doi.org/10.3390/app12146958
Chicago/Turabian StyleCardoso, José Maria, Sofia Duarte, Ana Clara Ribeiro, Paulo Mascarenhas, Susana Noronha, and Ricardo Castro Alves. 2022. "Association between IL-1A, IL-1B and IL-1RN Polymorphisms and Peri-Implantitis: A Systematic Review and Meta-Analysis" Applied Sciences 12, no. 14: 6958. https://doi.org/10.3390/app12146958