
Pain Perception during Orthodontic Treatment with Fixed Appliances

 , ,
, ,
Abstract
:1. Introduction
- Physiological parameters: pulse, blood pressure, and sweating;
- Behavioral parameters: facial expressions (closed eyes, open mouth, dilated nostrils, hollow tongue), high-pitched crying, and body movements (kicking, closed fists) [16]. Still, there are some scales to determine pain intensity.
- Verbal scales—used at the time of presentation or during treatment, which classifies pain in 3, 5 or 7 grades: absent/weak/mild/moderate/intense/severe/extreme pain [15].
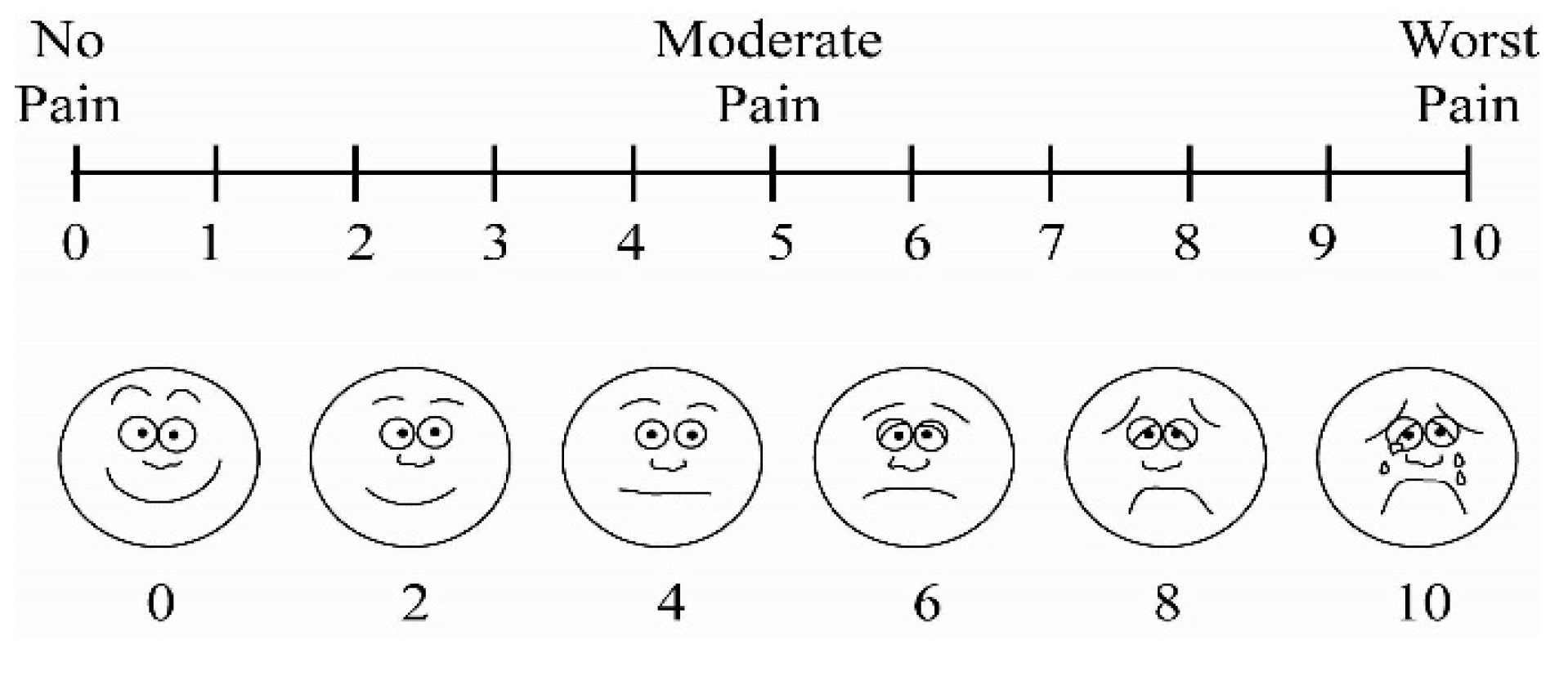
- Visual analog scales—these consist of a line with a length of 10 cm, oriented vertically/horizontally, whose extremes are two terms: “no pain” and “the greatest possible pain” [17].
- Numerical scales—in these cases, the patient is asked to quantify pain using numerical values between 0 and 10 or 0 and 100 (0 representing no pain and 10/100 extreme pain). These scales are easier to understand, providing at the same time a better description of pain intensity, and frequently replace verbal/visual scales [17].
- Behaviorally anchored scales—these quantify the intensity of pain based on its effect on behavior and describe the impact of pain on daily activities [17].
2. Materials and Methods
3. Results
4. Discussion
- The force applied—both small and large forces cause tooth displacement, but in the case of smaller intensity forces that reduce and avoid periodontal ligament hyalinization, the displacement coefficient is bigger;
- The patient’s age can influence the displacement coefficient; thus, in the case of adults, the tooth displacement rate is lower than in children due to the increased alveolar bone density and the diminution of cell response effectiveness [12].
5. Conclusions
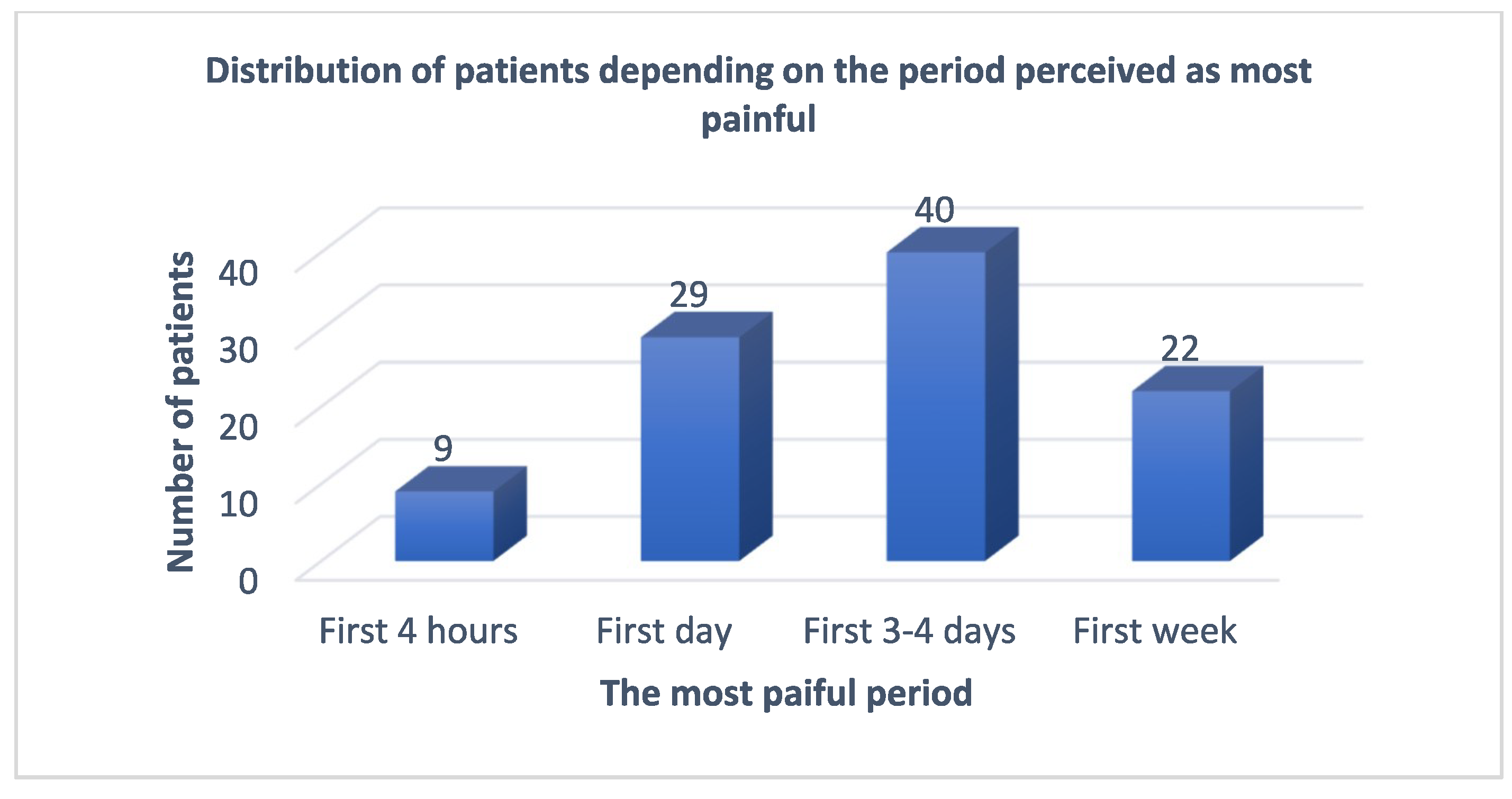
- The period perceived as most painful by patients treated with fixed orthodontic appliances was during the first 3–4 days after placement.
- Most patients required analgesic medication during the fixed orthodontic treatment, the most frequent being Nurofen, ketonal, and paracetamol.
- The mean value of the pain sensation felt was significantly higher in the case of the male sex compared to the female sex in all four age groups. Patients suffer the intensity of perceived pain differently as they grow older.
- The most painful procedure was represented by ring cementation in all age groups, with the highest pain intensity in the 18–24 age group.
- In cases where the clinical situation and the treatment plan allow, the cemented rings should be replaced with orthodontic tubes. If not, we will have to recommend an analgesic medication, especially 3 to 4 days after putting in the fixed orthodontic appliance.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Questionnaire
- Name:
- Age:
- (a)
- 12 to 18 years
- (b)
- 18 to 24 years
- (c)
- 24 to 30 years
- (d)
- over 30 years
- Sex:
- (a)
- male
- (b)
- female
- (c)
- other
- General health status:
- (a)
- Good
- 5.
- The most painful period was:
- (a)
- the first 4 h
- (b)
- the first day
- (c)
- the first 3–4 days
- (d)
- the first week
- 6.
- Pain was more intense:
- (a)
- during the day
- (b)
- at night
- (c)
- during the day and the night
- 7.
- 8.
- The drugs administered for pain relief were: Which was the most effective in fighting pain
- (a)
- Ketonal/Ibuprofen/Nurofen
- (b)
- Metamizole
- (c)
- Paracetamol
- (d)
- Other (mention them)
- 9.
- Mention the most painful procedure:
- (a)
- ring cementation
- (b)
- use of separating elastics
- (c)
- arch activation
- (d)
- elastic traction

References
- Alansari, R.A. Youth Perception of Different Orthodontic Appliances. Patient Prefer. Adher. 2020, 14, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Fujiyama, K.; Honjo, T.; Suzuki, M.; Matsuoka, S.; Deguchi, T. Analysis of pain level in cases treated with Invisalign aligner: Comparison with fixed edgewise appliance therapy. Prog. Orthod. 2014, 15, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bucur, S.M.; Chibelean, M.; Pacurar, M.; Sita, D.D.; Zetu, I.N. Ethical considerations in Orthodontics and Dentofacial Orthopaedics. Rev. Rom. Bioet. 2014, 12, 80–84. [Google Scholar]
- Yamaguchi, M.; Fukasawa, S. Is Inflammation a Friend or Foe for Orthodontic Treatment?: Inflammation in Orthodontically Induced Inflammatory Root Resorption and Accelerating Tooth Movement. Int. J. Mol. Sci. 2021, 22, 2388. [Google Scholar] [CrossRef]
- D’Apuzzo, F.; Nucci, L.; Delfino, I.; Portaccio, M.; Minervini, G.; Isola, G.; Serino, I.; Camerlingo, C.; Lepore, M. Application of Vibrational Spectroscopies in the Qualitative Analysis of Gingival Crevicular Fluid and Periodontal Ligament during Orthodontic Tooth Movement. J. Clin. Med. 2021, 10, 1405. [Google Scholar] [CrossRef]
- Mansour, A.Y. A comparison of orthodontic elastic forces: Focus on reduced inventory. J. Orthod. Sci. 2017, 6, 136–140. [Google Scholar] [CrossRef]
- Nucera, R.; Gatto, E.; Borsellino, C.; Aceto, P.; Fabiano, F.; Matarese, G.; Perillo, L.; Cordasco, G. Influence of bracket-slot design on the forces released by superelastic nickel-titanium alignment wires in different deflection configurations. Angle Orthod. 2014, 84, 541–547. [Google Scholar] [CrossRef] [Green Version]
- McNamara, C.; Drage, K.J.; Sandy, J.R.; Ireland, A.J. An evaluation of clinicians’ choices when selecting archwires. Eur. J. Orthod. 2010, 32, 54–59. [Google Scholar] [CrossRef] [Green Version]
- Foster, T.D. A Textbook of Orthodontics, 3rd ed.; Blackwell Scientific Publications: Boston, MA, USA, 1990; pp. 123–129. [Google Scholar]
- Proffit, W.R.; Fields, H.W., Jr. 1992 Contemporary Orthodontics, 2nd ed.; Mosby Year Book: Mount Joy, PA, USA, 1992; pp. 12–18. [Google Scholar]
- D’Apuzzo, F.; Cappabianca, S.; Ciavarella, D.; Monsurrò, A.; Silvestrini-Biavati, A.; Perillo, L. Biomarkers of Periodontal Tissue Remodeling during Orthodontic Tooth Movement in Mice and Men: Overview and Clinical Relevance. Sci. World J. 2013, 2013, 105873. [Google Scholar] [CrossRef] [Green Version]
- Miles, T.S.; Nauntofte, B.; Svensson, P. Clinical Oral Physiology; Quintessence Publishing Co., Ltd.: New Malden, UK, 2004; pp. 45–61. [Google Scholar]
- Jeon, H.H.; Teixeira, H.; Tsai, A. Mechanistic Insight into Orthodontic Tooth Movement Based on Animal Studies: A Critical Review. J. Clin. Med. 2021, 10, 1733. [Google Scholar] [CrossRef]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef] [PubMed]
- Grassia, V.; Rotolo, R.P.; Nucci, L.; D’Apuzzo, F.; Perillo, L. Bullying and malocclusion in adolescence: A case report. South Eur. J. Orthod. Dentofac. Res. 2020, 7, 17–20. [Google Scholar] [CrossRef]
- Patel, V. Non-completion of Active Orthodontic Treatment. Br. J. Orthod. 1992, 19, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Bergius, M.; Berggren, U.; Kiliaridis, S. Experience of pain during an orthodontic procedure. Eur. J. Oral Sci. 2002, 110, 92–98. [Google Scholar] [CrossRef]
- Available online: https://assessment-module.yale.edu/im-palliative/visual-analogue-scale (accessed on 3 April 2021).
- Asiry, M.A. Biological aspects of orthodontic tooth movement: A review of literature. Saudi J. Biol. Sci. 2018, 25, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- Anthonappa, R.P.; Ashley, P.; Bonetti, D.L.; Lombardo, G.; Riley, P. Non-pharmacological interventions for managing dental anxiety in children. Cochrane Database Syst. Rev. 2017, 2017, CD012676. [Google Scholar] [CrossRef] [Green Version]
- Scheurer, P.A.; Firestone, A.R.; Burgin, W.B. Perception of pain as a result of orthodontic treatment with fixed appliances. Eur. J. Orthod. 1996, 18, 349–357. [Google Scholar] [CrossRef]
- Fernandes, L.M.; Skoglund, L. Pain and discomfort experienced after placement of a conventional or a superelastic NiTi aligning archwire. A randomized clinical trial. J. Orofac. Orthop. 1998, 59, 331–339. [Google Scholar] [CrossRef]
- Aslihan, M.E.; Dincer, B. Perception of pain during orthodontic treatment with fixed appliances. Eur. J. Orthod. 2004, 26, 79–85. [Google Scholar]
- Rakhshan, H.; Rakhshan, V. Pain and discomfort perceived during the initial stage of active fixed orthodontic treatment. Saudi Dent. J. 2015, 27, 81–87. [Google Scholar] [CrossRef] [Green Version]
- White, L.W. Pain and cooperation in orthodontic treatment. J. Clin. Orthod. 1984, 18, 572–575. [Google Scholar] [PubMed]
- Krishnan, V. Orthodontic pain: From causes to management—A review. Eur. J. Orthod. 2007, 29, 170–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergius, M.; Kiliardis, S.; Berggren, U. Pain in orthodontics: A review and discussion of the literature. J. Orofac. Orthop. 2000, 61, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Bud, E.; Vlasa, A.; Chibelean, M.; Martha, K.; Păcurar, M.; Bud, A.; Esian, D. Factors Associated with Pain Intensity in Patients Undergoing Orthodontic Treatment Based on Mini-Implants. J. Interdiscip. Med. 2021, 6, 74–81. [Google Scholar] [CrossRef]
- Ingersoll, D.B. Behavioral Aspects in Dentistry; Appleton Century Crofts: Norwalk, CT, USA, 1982; pp. 14–32. [Google Scholar]
- Olteanu, C.D.; Şerbănescu, A.; Boşca, A.B.; Mihu, C.M. Orthodontic tooth movement following analgesic treatment with Aspirin and Algocalmin. An experimental study. Rom. J. Morphol. Embryol. 2015, 56, 1339–1344. [Google Scholar]
- Arias, O.R.; Marquez-Orozco, M.C. Aspirin, acetaminophen, and ibuprofen: Their effects on orthodontic tooth movement. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 364–370. [Google Scholar] [CrossRef]
- Nandi, M.; Schreiber, K.L.; Martel, M.O.; Cornelius, M.; Campbell, C.M.; Haythornthwaite, J.A.; Smith, M.T.; Wright, J.; Aglio, L.S.; Strichartz, G.; et al. Sex differences in negative affect and postoperative pain in patients undergoing total knee arthroplasty. Biol. Sex Differ. 2019, 10, 23. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Procedure | Age Group | Mean | p Value |
|---|---|---|---|
| Elastic separation | 12–18 | 2.09 | 0.04 |
| Ring cementation | 18–24 | 2.21 | 0.00 |
| Arch activation | 24–30 | 2.14 | 0.00 |
| Elastic traction | >30 | 1.07 | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olteanu, C.D.; Bucur, S.-M.; Chibelean, M.; Bud, E.S.; Păcurar, M.; Feștilă, D.G. Pain Perception during Orthodontic Treatment with Fixed Appliances. Appl. Sci. 2022, 12, 6389. https://doi.org/10.3390/app12136389
Olteanu CD, Bucur S-M, Chibelean M, Bud ES, Păcurar M, Feștilă DG. Pain Perception during Orthodontic Treatment with Fixed Appliances. Applied Sciences. 2022; 12(13):6389. https://doi.org/10.3390/app12136389
Chicago/Turabian StyleOlteanu, Cristian Doru, Sorana-Maria Bucur, Manuela Chibelean, Eugen Silviu Bud, Mariana Păcurar, and Dana Gabriela Feștilă. 2022. "Pain Perception during Orthodontic Treatment with Fixed Appliances" Applied Sciences 12, no. 13: 6389. https://doi.org/10.3390/app12136389