1. Introduction
The artificial replacement of completely missing teeth with restoration of form, function and esthetics is critical to improving quality of life among edentulous patients [
1]. A majority of edentulous patients experience psychosocial problems due to criticism, embarrassment and low confidence levels. For decades, different techniques and materials, i.e., wood, ivory and metals, have been employed for artificial denture fabrication [
2]. Polymethyl methacrylate (PMMA) polymer denture resin material has been the material of choice for denture fabrication for the last 50 years, and has gained widespread acceptance due to its simplified processing and equipment, functional longevity, ease of maintenance, cost-effectiveness and esthetics [
3].
The longer life expectancy of the elderly population leads to a higher number of individuals needing an artificial removable prosthesis [
4]. Edentulous patients may lack manual dexterity and be unable to remove denture plaque. Therefore, PMMA denture patients are more susceptible to mucosal infections from bacterial and fungal species. In addition to various bacteria,
Candida albicans (fungi) are most commonly associated with denture-related oral infections [
5]. In order to overcome denture-related infections, different denture cleansers are used to effectively remove stains and food debris from the denture bases [
6]. At present, different PMMA denture cleaning and disinfection techniques include mechanical, chemical and physical methods. Mechanical methods used for denture cleaning include the use of a toothbrush with water [
7]. In their study, Veres et al. [
8] revealed that 60–90% of denture patients practice mechanical cleaning in association with products such as toothpaste, soap or water. However, use of an unsuitable toothbrush with a dentifrice may also lead to surface roughness, which allows more microbial colonization [
9]. In order to overcome drawbacks of mechanical cleaning, soaking PMMA denture bases in chemical disinfecting agents has gained more acceptance in clinical dentistry due to antimicrobial activity [
10]. Chemical agents commonly used for denture cleaning include sodium hypochlorite, glutaraldehyde and chlorine dioxide, 0.12% Chlorhexidine gluconate, sodium perborate and alkaline peroxide [
11]. The prosthesis is commonly immersed in the chemical agent for a specific duration for plaque removal and disinfection [
11]. Effervescent tablets yielding an alkaline peroxide dilution with water are the preferred denture cleansers [
12]. However, chemical disinfecting agents used for denture cleaning are known to damage acrylic resin, initiate surface staining or discoloration, and have been reported to be have cytotoxic ingredients [
11].
Apart from mechanical and chemical means of denture disinfection, microwave oven disinfection is an effortless and inexpensive method for PMMA dentures [
13,
14]. Microwave irradiation allows for disinfection of not just bacteria and fungal species, but can also eliminate viruses [
8]. Microwave irradiation can be a convenient, quick and cost effective household method for disinfecting PMMA dentures [
13]. Studies have revealed that microwave disinfection has more potency for denture disinfection compared to sodium hypochlorite alone [
8]. However, limited evidence is available to validate the disinfection protocol and standards for microwave irradiation to be a standard disinfection technique for acrylic dentures.
Previous studies investigating microwave disinfection of acrylic polymers have utilized high power (650 to 1400 watts) and increased exposure times (3 min, 5 min, 8, min, 10 min) [
12,
13,
14]. However, these irradiation parameters can result in physical damage to polymeric denture base resin, including its dimensional stability and mechanical properties [
15]. Therefore, it is critical to assess the low power and duration protocol for microwave irradiation in comparison to chemical disinfection for acrylic denture resin disinfection. It is hypothesized that the bacterial disinfection (cleaning efficacy) of PMMA denture base resin with a cleaning tablet or with microwave irradiation at low power (watt) and duration (1, 2 and 3 min) will be comparable. Therefore, the present study aimed to evaluate the disinfection efficacy of denture cleaning tablets (sodium perborate) and microwave irradiation at low power and duration (1, 2 and 3 min) for
E. coli,
S. aureus and
S. mutans cultured on the PMMA denture base polymer.
2. Materials and Methods
In the present study, sample preparation was performed at the Dr Ishrat-ul-Ebad Institute of Oral Health Sciences (Department of Prosthodontics); however, the microbiological testing along with the disinfection interventions were undertaken at the Pakistan Council of Scientific & Industrial Research Laboratories. (PCSIR). The study assessed the antibacterial disinfection of PMMA denture resin polymer using individual and combined use of distilled water (DW), microwave disinfection (MW) and denture cleaning agent (DC). Disinfection of PMMA polymer was assessed on bacteria cultured at 24, 36, 48 and 96 h and with disinfecting durations of 1 to 5 min.
2.1. Specimen Preparation
Sample size was calculated using Pass version 11 (NCSS Statistical software, Kaysville, UT, USA), employing one-way ANOVA with 99% confidence interval, 99% power of the test, and with means and standard deviation of
C. Albicans viable cells in groups: DW = 7.47 × 10
5, DC = 4.82 × 10
5, DW with MW 1 min = 4.49 × 10
5, DC with MW 1 min = 2.64 × 10
5, DC with MW 2 min = 0.00, DW with MW 3 min = 0.00, DC with M 3 min =0.00 [
16]. Sample size was calculated with at least 10 specimens per sub-group (total 12 subgroups). However, a total of 168 specimens were fabricated (
n = 14).
Test specimens (
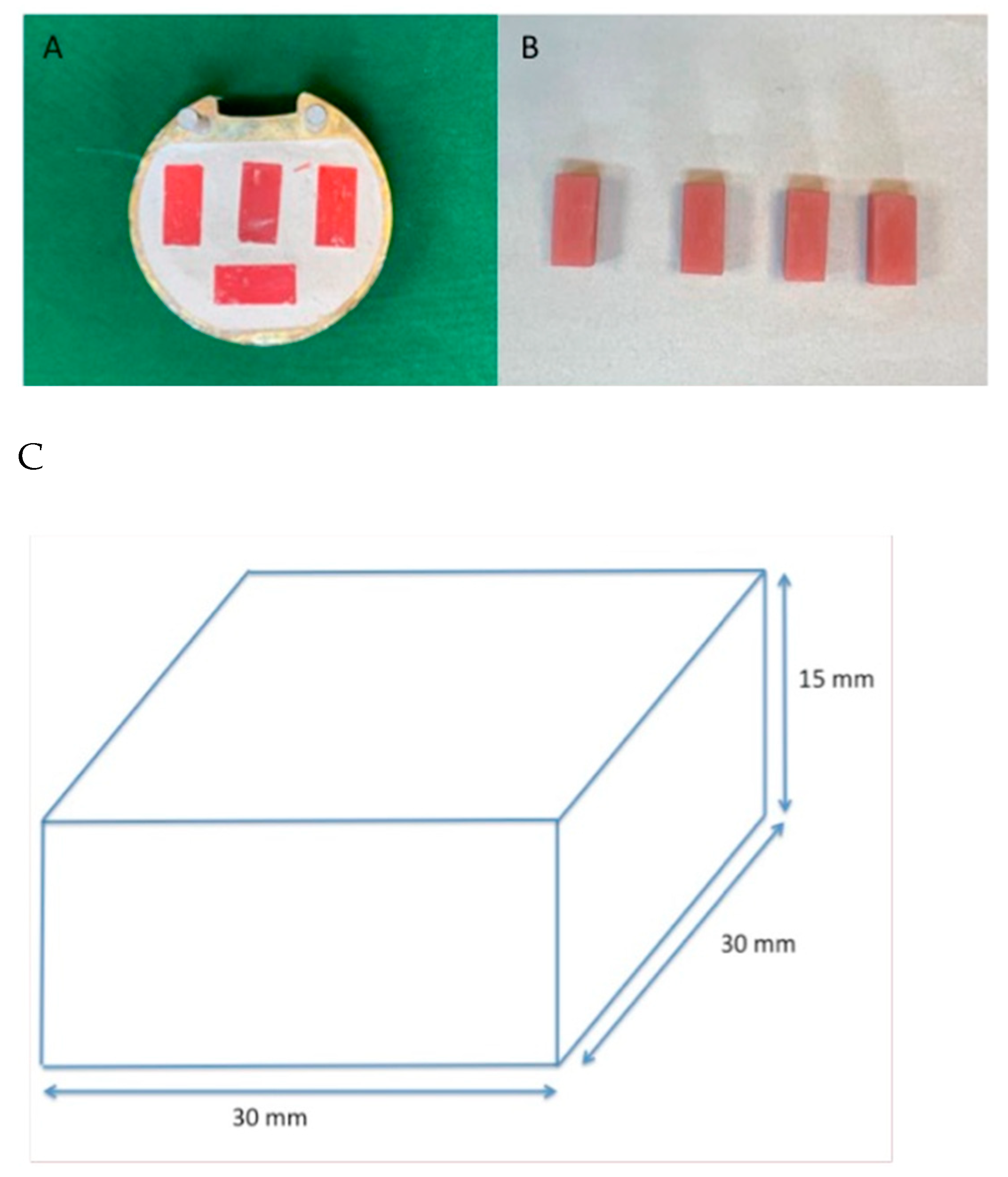
n = 168) of PMMA acrylic resin denture base were fabricated with the help of modelling wax (Yeti Dental GmbH, Engen, Germany) melted in a wax pot (Manfredi, San secondo di Pinerolo TO, Italy) and poured into a three-part preformed metal mold (30 × 30 × 15 mm). Wax patterns were impressed in a metallic denture flask filled with type III dental stone (Garrico Lab Stone, Heber Springs, AR, USA) to produce PMMA samples. De-waxing was performed using boiling water for 6 min. Heat polymerized PMMA acrylic resin was mixed and packed at a doughy stage according to manufacturer recommendations at a powder: liquid ratio, 2.3 g of polymer powder to 1 mL of liquid monomer (heat-cured acrylic provided by MR Dental, Plymouth, UK). A Hydraulic press was used for packing the denture base resin with a sheet of separating plastic between the two halves. Heat cure PMMA was polymerized in a thermostatically controlled water bath (Manfredi–Acrydig 12) and processed for 74 °C for two hours followed by 100 °C for one hour (
Figure 1).
All specimens were allowed to cool at room temperature before de-flasking and were immersed in distilled water at room temperature for 48 h for residual monomer elimination. The excess resin was trimmed with a metal bur (Denfac Acrylic trimming burs). All PMMA specimens were wet-polished with abrasive paper (# 1200, water resistant) and buffed (Dialap ML150P; Maruto, Tokyo, Japan). Final finishing was performed with an alumina-based abrasive (particle size: 0.3 μm). Post-finishing, all specimens were autoclaved at 121 °C for 15 min. For the purpose of reliability, a single operator prepared all the specimens.
2.2. Study Groups
All specimens were divided into three main groups based on disinfection techniques, which are as follows.
Group MW-DW: microwave (MW) radiation was used to disinfect the specimens contaminated with a mixture of three isolates immersed in distilled water in a glass beaker. The glass container was placed in the microwave oven and the specimens were sterilized at 450 W. Based on duration of MW radiation, specimens were divided into MW-DW1 (1 min), MW-DW2 (2 min) and MW-DW3 (3 min). Different specimens in each subgroup were assessed at 24 h, 36 h, 48 h and 96 h, respectively.
Group DC-DW: specimens were immersed in distilled water with a denture cleaning tablet (sodium perborate) (DC) (Fittydent international, GmbH, Wien, Austria) added to it. Based on the duration of immersion in DC, the specimens were divided into DC-DW1 (1 min), DC-DW2 (2 min) and DC-DW3 (3 min). Different specimens in each subgroup were assessed at 24 h, 36 h, 48 h and 96 h, respectively.
Group MW-DC-DW: the glass beaker containing 200 mL of distilled water in which a denture cleaning tablet was dissolved for five minutes was placed in the microwave oven and irradiated at 450 W. Based on duration of MW radiation, specimens were divided into MW-DC-DW1 (1 min), MW-DC-DW2 (2 min) and MW-DC-DW3 (3 min). The temperature of the solution was kept between 65 °C to 71 °C with ±2 °C. Different specimens in each subgroup were assessed at 24 h, 36 h, 48 h and 96 h, respectively. With five specimens in each subgroup, a total of 180 specimens in each disinfection group were employed.
Positive Control Group: in this group the acrylic resin specimens were immersed in glass beaker (250 mL size) containing 200 mL of distilled water at room temperature. The glass container was placed in the center of the microwave oven chamber (Samsung 2450 MHz, 800 W) but was not irradiated.
Negative Control Group: the purpose of this group was to establish the disinfection of the specimens and accuracy of the test. For each bacterium, sterilized specimens were placed in a container with sterilized water.
2.3. Biofilm Formation Assay
Overnight specimens of 0.1 mL of
E. coli (ATCC# 8739),
S. aureus (ATCC# 25923) and
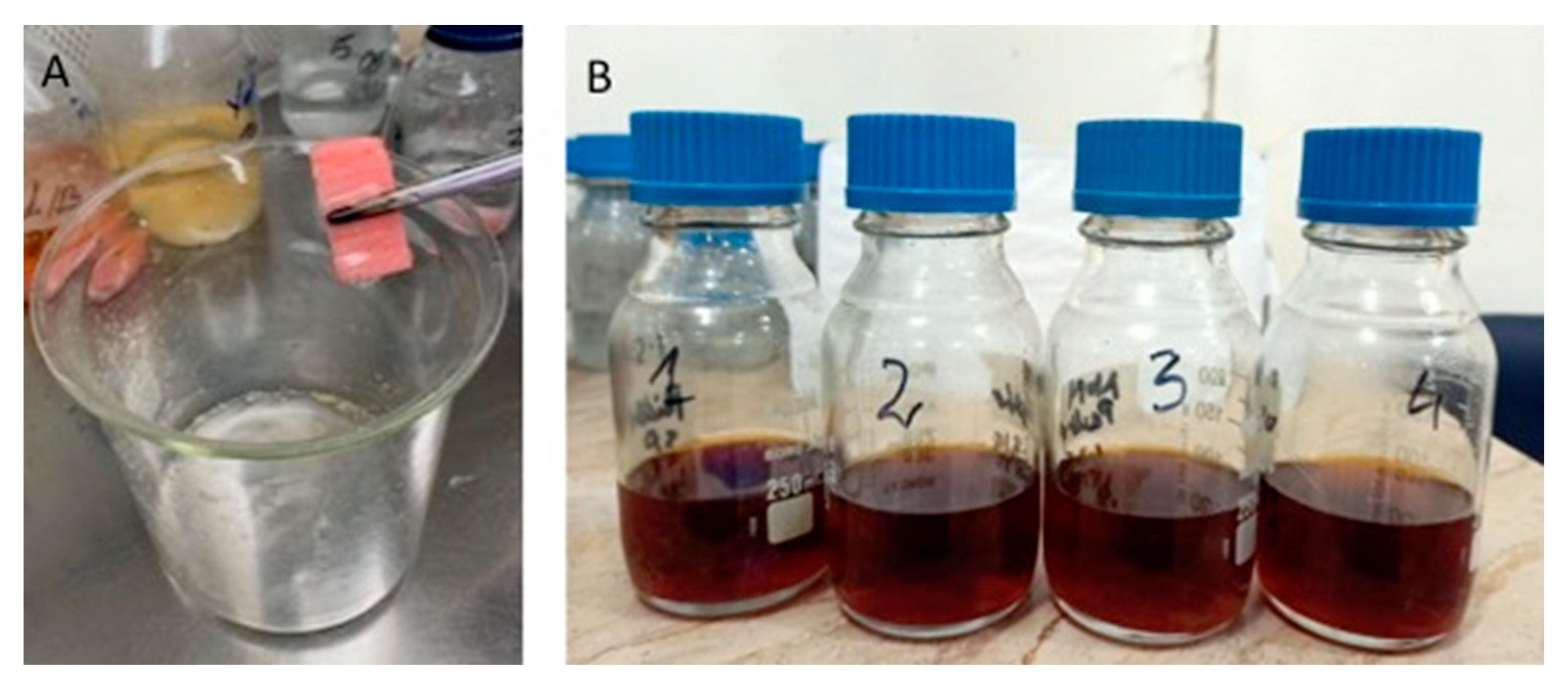
S. mutans (ATCC# 25175) subject isolates were inoculated into 100 mL of sterile Tryptic Soy Broth (TSB-Oxoid, Basingstoke, Hampshire, UK). The group contained a mixture of all three isolates. The sterile acrylic specimens were inoculated into each flask aseptically and incubated at 37 °C for 24 h, 36 h, 48 h and 96 h. After incubation, the acrylic specimens were collected and washed with distilled water to remove debris and loosely attached cells (
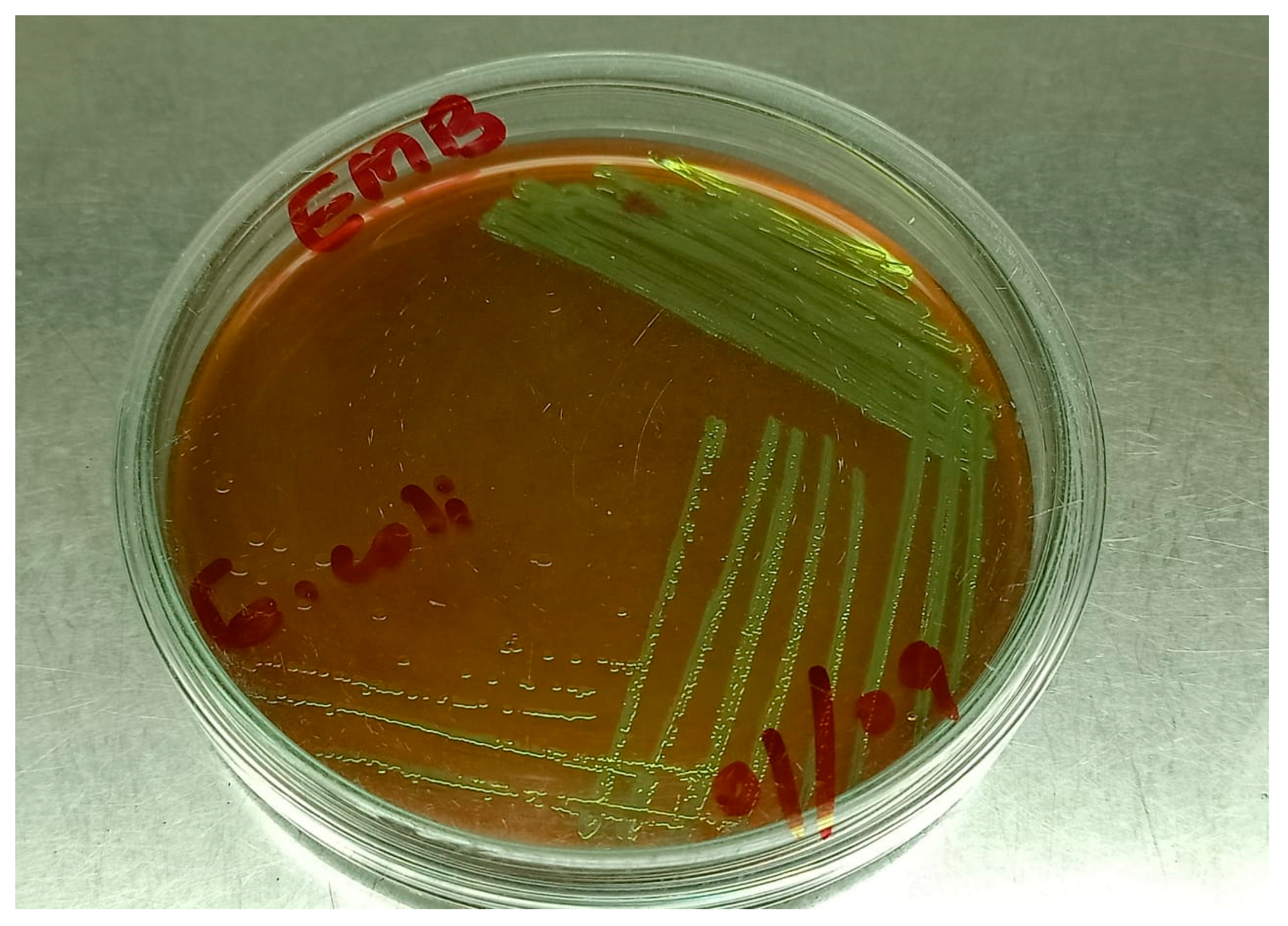
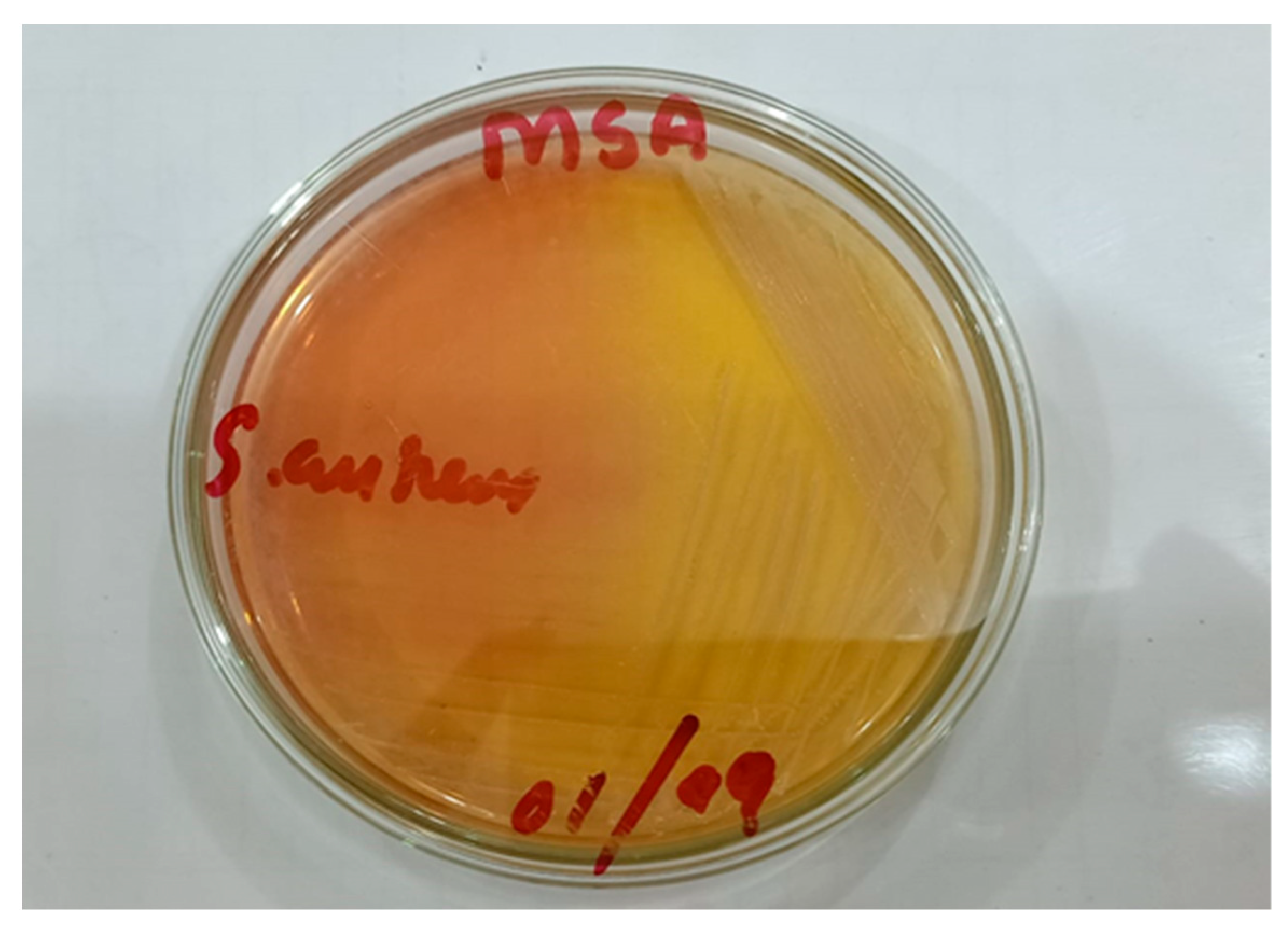
Figure 2). Specimens were placed in phosphate buffered saline (PBS) (pH-7) and vortexed for two minutes. After vortexing, the specimens were, as has been explained, exposed to three treatment regimens in study groups (MW-DW, DC-DW and MW-DC-DW) at different exposure times. For selective isolation of bacteria,
E. coli,
S. aureus and
S. mutans were cultured in Eosin Methylene Blue Agar (EMB Oxoid Basingstoke, Hampshire, UK) (
Figure 3), Baird-Parker Agar with egg yolk tellurite (Fisher Scientific, Port Salvo, Portugal) (
Figure 4) and Brain Heart Infusion (BHI) Broth (Difco, Detroit, MI, USA). The growth was monitored and CFU were counted.
2.4. Quantification of Biofilm
The PMMA slides were collected after 24 h to 96 h and adhesion was assessed using crystal violet binding assay. Bacterial growth was fixed with acetic acid, followed by staining with 3% crystal violet (Ezzy Stain) and washing with PBS at 7.0 pH. Heat fixation was performed for 30 s followed by acetone washing. For accuracy of assessment and measurements, the procedure was repeated twice (per sample).
2.5. Scanning Electron Microscopy
Scanning electron microscopy was carried out for the analysis of the production of extracellular matrix material and to observe the bacterial presence and disinfection on acrylic slides. Biofilm slides were divided into 4 mm sections and washed with distilled water to remove the debris and were then negatively stained with 0.02% Uranyl acetate for 30 s. These 4 mm slides were platinum coated in a coating machine (JEOL 3000 FC, Tokyo, Japan), and the sections showed the presence of biofilm material when examined directly in SEM (JOEL-JSM IT-100, Tokyo, Japan).
2.6. Statistical Analysis
Data were entered and analyzed using SPSS (IBM Statistics software version 21, New York, NY, USA). For average comparison among exposure time, Kruskal–Wallis analysis was applied to each of the bacteria (E. coli, S. aureus and S. mutan) by treatment and growth time as CFU count were not normally distributed. The Mann–Whitney test was applied for pair-wise comparison of each exposure time with treatment and growth time controlled. A p-value of < 0.05 was considered as statistically significant.
3. Results
Mean CFU comparison for
E. coli with the control for each disinfecting regime and growth time is presented in
Table 1. From the results, it was found that all the specimens incubated at 24, 36, 48 and 96 h and exposed to MW-DW-DC and MW-DW disinfection for 1, 2 and 3 min demonstrated significant difference in mean CFU of
E. coli compared to the control without disinfection. However, for the MW-DW-DC group, complete disinfection was achieved at 2 min of disinfection at any growth time (
p-value < 0.05). Conversely, for MW-DW disinfection, CFU was significantly zero at 3 min when compared with control at any growth time (
p-value ≤ 0.05). For DC-DW specimens, CFU levels were approximately zero at five minutes when compared with the control at different growth durations (
p-value ≤ 0.05) (
Table 1).
Mean CFU comparison for
S. aureus among the control for each disinfecting regime and growth times is presented in
Table 2. For MW-DW-DC, CFU were significantly zero at 2 min of disinfection when compared with control at any growth time (
p-value ≤ 0.05). For MW-DW specimens, CFU were significantly zero at 3 min of disinfection when compared with control at each growth time (
p-value ≤ 0.05). For DC-DW disinfection, CFU were significantly zero at five minutes when compared with control at each growth time (
p-value ≤ 0.05) (
Table 2).
Mean CFU comparison for
S. mutans with the control for each disinfecting regime and growth time is presented in
Table 3. For MW-DW-DC, CFU were significantly zero at 2 min when compared with control (
p-value ≤ 0.05). For MW-DW disinfection, CFU were significantly zero at three mins when compared it with control at each growth time (
p-value ≤ 0.05). For DC-DW, CFU were significantly zero at 5 min when compared with control at each growth time (
p-value ≤ 0.05) (
Table 3).
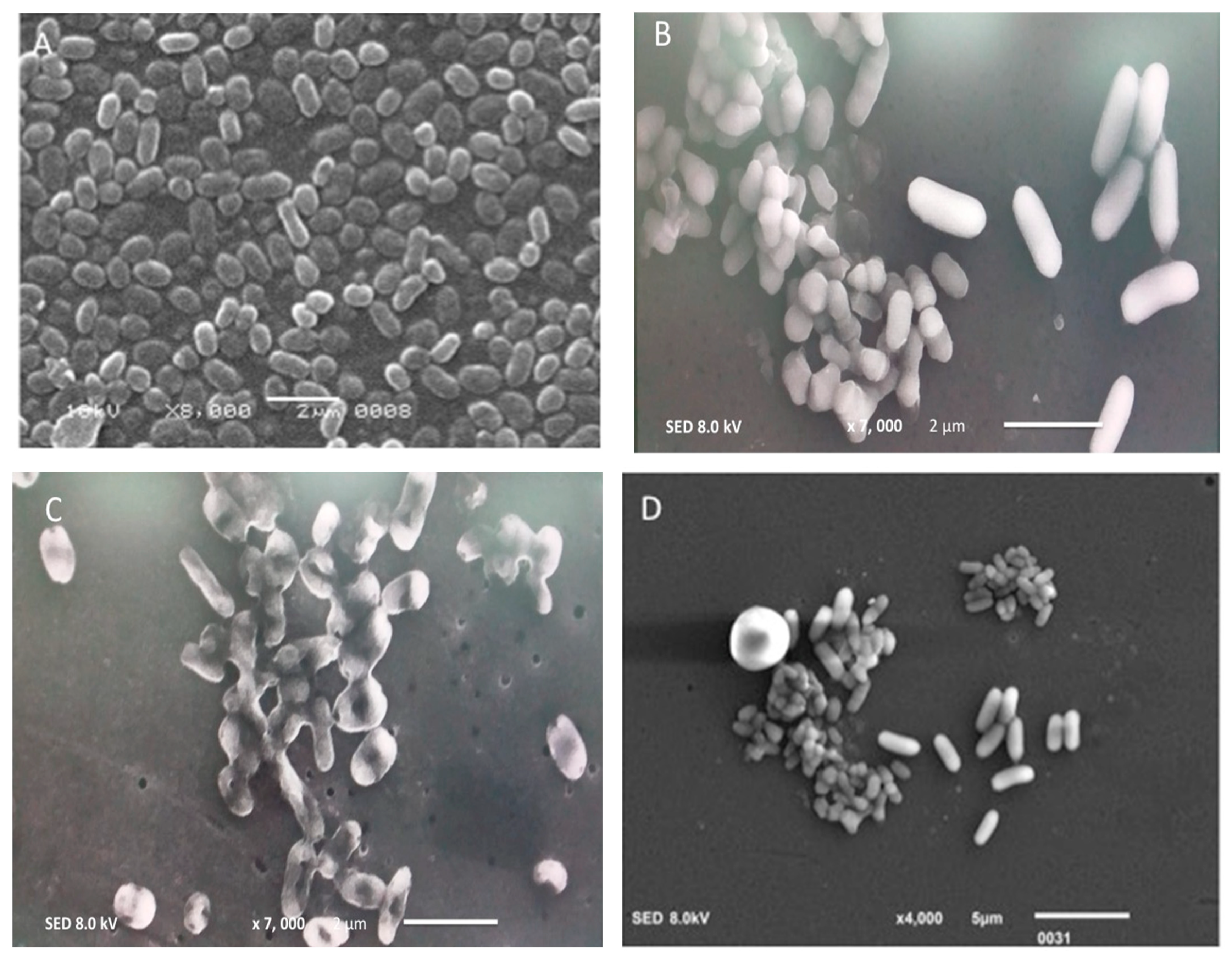
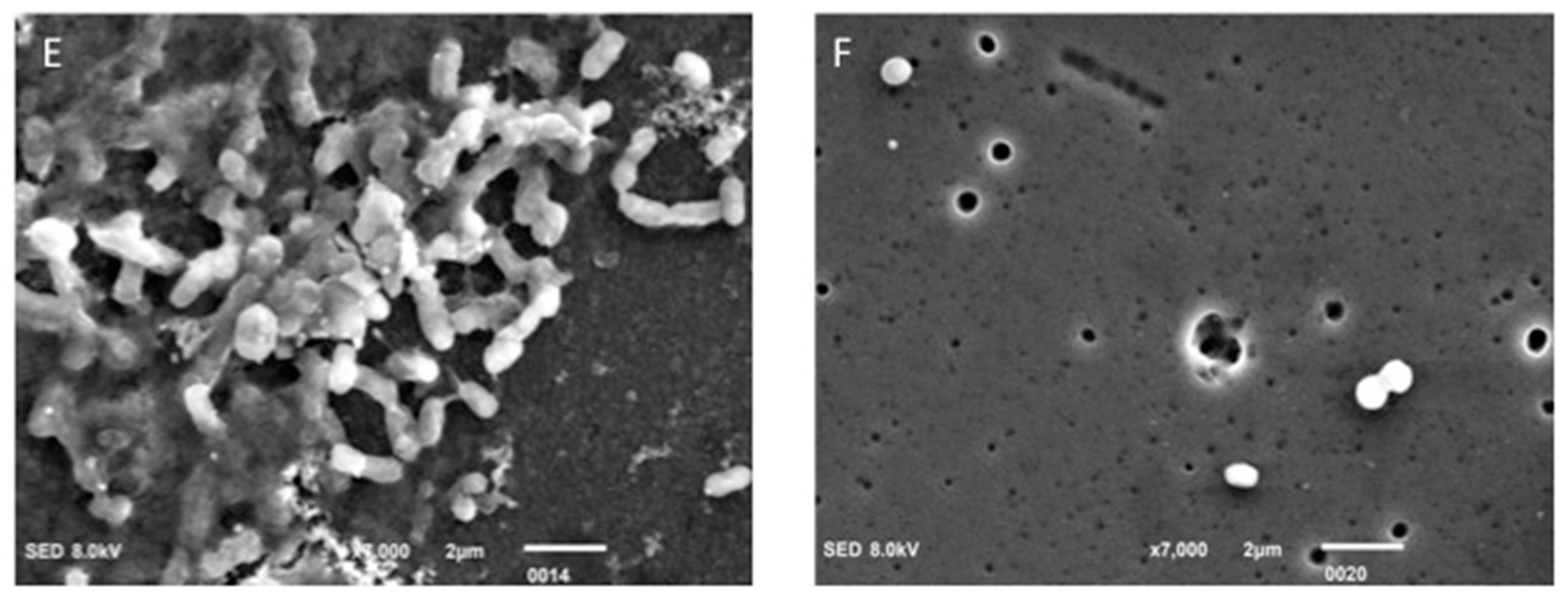
SEM analysis of the samples showed positive consortia-harboring cocci and bacilli (
Figure 5). Using SEM, live cells of
E. coli (rods),
S. aureus and
S. mutans (cocci) attached to the PMMA specimens were observed. After the disinfection procedure, dead cells were observed attached to the PMMA surface in the form of a small, agglomerated, mass of irregular-shaped cells (
Figure 5).
4. Discussion
The current study was conducted to evaluate the cumulative effect of microwave disinfection and a denture cleaning tablet (sodium perborate) with reduced time and power on the elimination of bacterial biofilm from PMMA denture base resin. It was based on the hypothesis that there will be no significant difference in cleaning efficacy of DC, MW and their combination on the disinfection of E. coli, S. aureus and S. mutans incubated on the PMMA denture base. Therefore, the postulated hypothesis was rejected, as all the tested groups displayed variable results of denture disinfection as compared to the control.
The possibility that a dental prosthesis can be a cause of infection and cross-contamination between patients and dental staff additionally stresses the need for disinfection [
17]. Dental appliance disinfection poses a significant problem for clinicians, particularly with regards to removable dentures [
18]. The results of the present study revealed that zero mean CFU was obtained after exposing PMMA to MW irradiation in combination with DC within 2 min (MW-DW-DC). In comparison, zero mean CFU for samples exposed to microwave alone (MW + DW) was obtained at 3 min. The one-minute exposure of acrylic specimen to MW irradiation showed 50% reduction in CFU for
E. coli, 24% for
S. aureus and 96% for
S. mutans. Conversely, the combination of MW and DC resulted in 97% reduction of
E. coli count, 96% for
S. aureus and 100% for
S. mutans after 1 min of exposure. Thus, a combination of MW irradiation with DC showed higher disinfection percentage of bacterial species in disinfection of PMMA polymer denture bases compared to MW and DC alone.
Considering the effectiveness of microwave disinfection, its role for denture decontamination has gained much attention in the past [
19]. Multiple previous pieces of research have used variable time and power to ascertain its efficacy for denture disinfection [
20]. Webb et al. first identified that an unmodified domestic microwave can perform denture disinfection [
10]. In the present study, the efficacy of microwave irradiation on acrylic resin contaminated with bacterial biofilm at different growth hours (24–36–48–96 h) was investigated keeping the power 450 W and irradiation time 1, 2 and 3 min. From the results, it was found that exposure to microwave irradiation took 3 min to achieve complete CFU count zero, i.e., complete removal of
S. aureus,
S. mutans and
E. coli from acrylic slides. Moreover, comparative analysis revealed that the increase in incubation period to 36 h resulted in an increased CFU count. However, this increase in count has not shown any impact on the disinfection capabilities of microwave radiation. These results are in line with the outcomes of the studies conducted by Baysan et al. and Dixon et al. [
21,
22]. These findings may be due to the fact that microwave irradiation alters structural integrity and cell membrane permeability [
23]. It also has detrimental effects on cell metabolism, thus leading to bacterial cell death. In contrast to microwave disinfection of PMMA polymer bases, a combination of chemical disinfection (denture cleaning tablets) and microwaving effectively and efficaciously disinfects the material faster than microwaving alone, within 2 min of exposure time [
24]. It is also important to note that the dentures in the present study were immersed in distilled water during microwave irradiation, a practice which has been a technique for eliminating microorganisms [
25].
It was also observed that chemical disinfection using DC displayed lower antimicrobial disinfection percentage than the combined use of MW and DC and MW alone at 1 min or 2 min disinfection time for all three bacteria. In the present study, the denture cleaning tablet used was Fittydent (Fittydent international, GmbH, Wien, Austria) According to the manufacturer information, the tablets containing sodium perborate not only clean removable dentures but also have antibacterial ability against bad odor microbes, dissolve tough stains and help in plaque removal [
26]. In case of bacterial biofilm, as the exposure time to the cleaning tablet increases the CFU count decreases, demonstrating the antimicrobial efficacy of the cleaning tablet used. There was 9% to 61% reduction in CFU count as the exposure increased from 1 to 3 min, and 96% to 100% of removal of CFU counts when it was exposed between 4 to 5 min. Thus, the cleaning tablet had more efficacy against bacterial biofilm when specimens were exposed for 4 to 5 min. The present result was in agreement with Silva et al., who evaluated the efficacy of commercial denture cleanser containing sodium perborate on the disinfection of acrylic specimens contaminated with
C. albicans and
S. mutans [
11]. They reported that denture cleaning tablets have effective antimicrobial efficacy against streptococcus species as compared to
C. albicans [
27].
It is worth mentioning that the current study was conducted in vitro, with inherent limitations when simulating in vivo environment. A more clinically relevant study protocol could be an ex vivo model, including the disinfection of a patient’s personal dentures in the oral cavity and experimental MW disinfection in the laboratory for CFU evaluation. It is pertinent to mention that denture-related stomatitis is commonly associated with
Candida albicans on the denture surface and oral cavity [
5]; therefore, further randomized controlled trials assessing the efficacy of microwave disinfection on the
Candida species are warranted. In light of the findings within the study limitation, MW disinfection in combination with denture cleaning agents are recommended for PMMA denture disinfection in denture wearers.



 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}