
The Incidence and Intensity of Postendodontic Pain and Flareup in Single and Multiple Visit Root Canal Treatments: A Systematic Review and Meta-Analysis

 , , ,
, , ,  , ,
, , 
Abstract
:1. Introduction
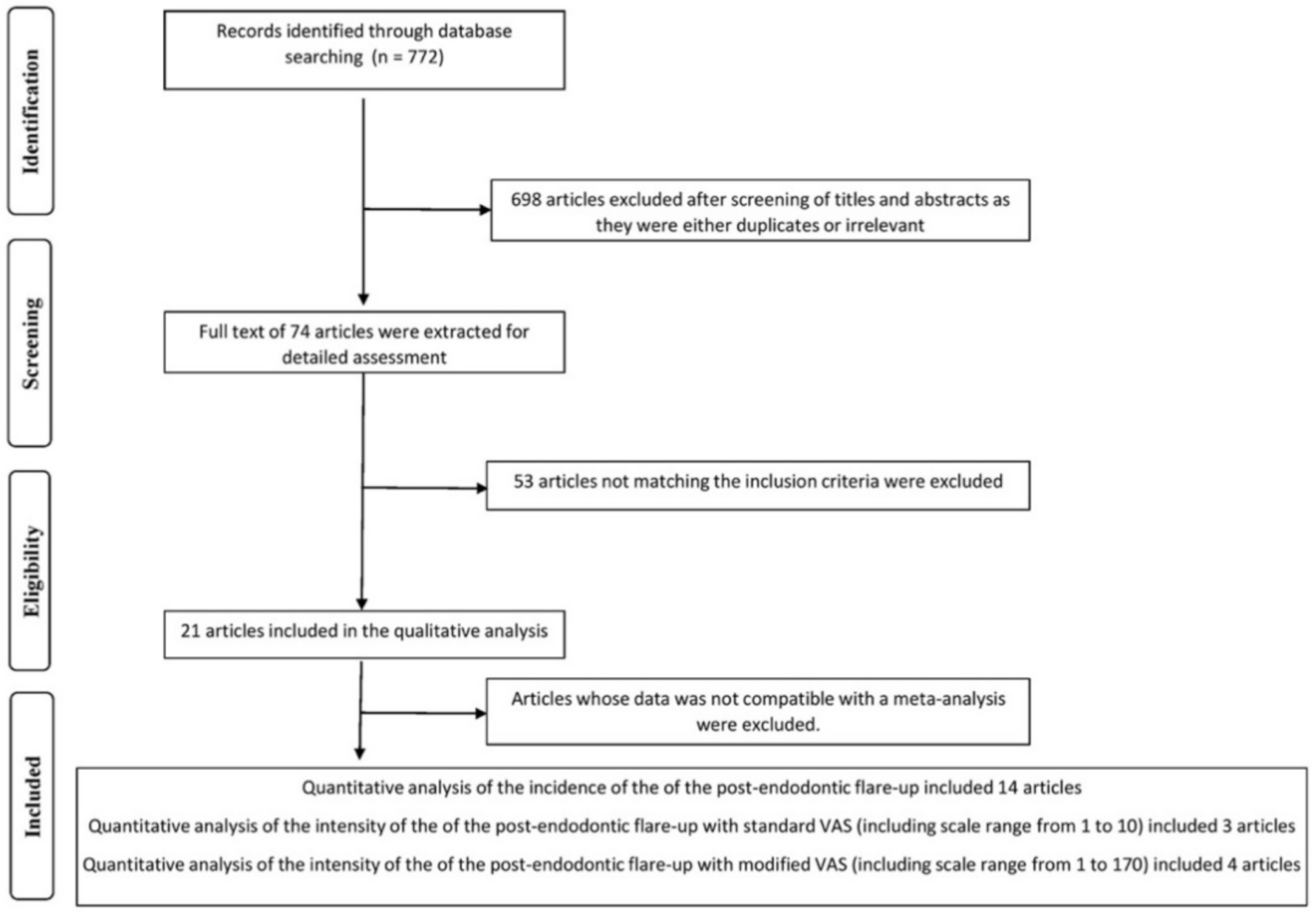
2. Materials and Methods
- The study must be conducted on permanent vital teeth.
- The outcome must have been measured post treatment or post initiation of treatment.
- Clinical procedure was described in detail.
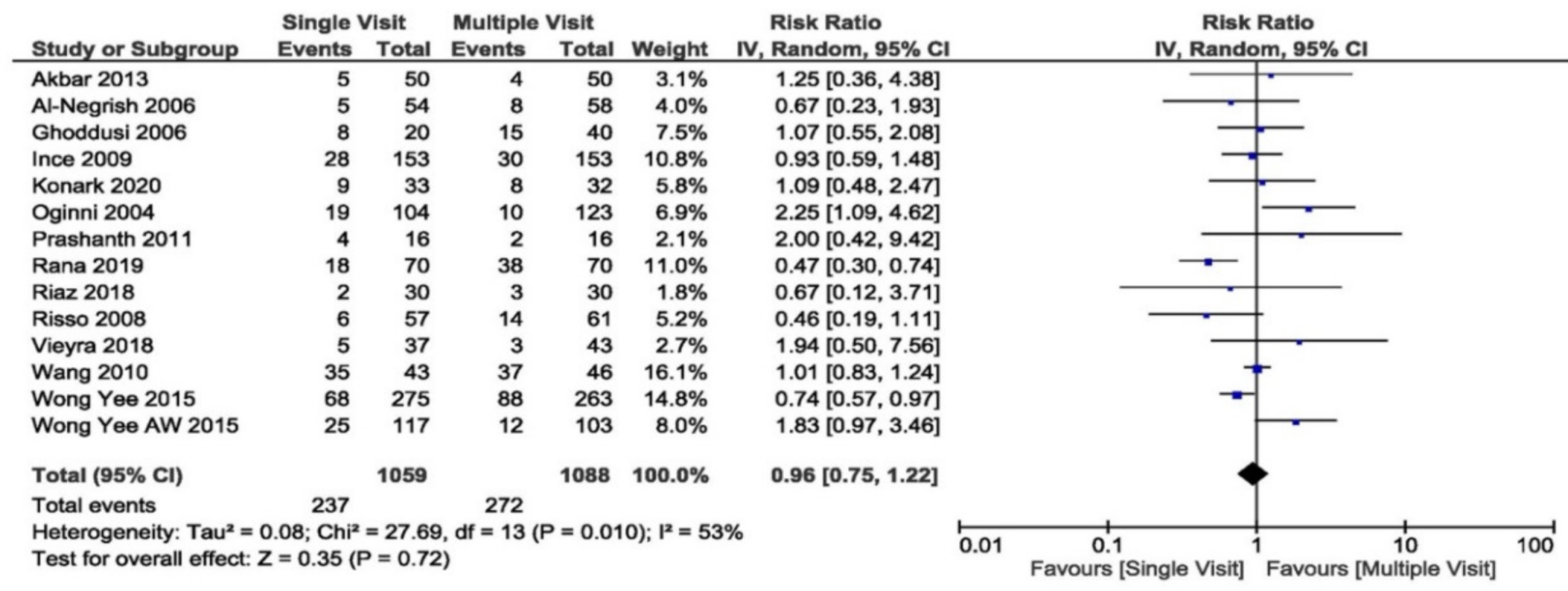
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gutmann, J.L. Clinical, radiographic, and histologic perspectives on success and failure in endodontics. Dent. Clin. N. Am. 1992, 36, 379–392. [Google Scholar] [PubMed]
- Calhoun, R.L.; Landers, R.R. One-appointment endodontic therapy: A nationwide survey of endodontists. J. Endod. 1982, 8, 35–40. [Google Scholar] [CrossRef]
- Walton, R.; Fouad, A. Endodontic interappointment flare-Ups: A prospective study of incidence and related factors. J. Endod. 1992, 18, 172–177. [Google Scholar] [CrossRef]
- Imura, N.; Zuolo, M. Factors associated with endodontic flare-ups: A prospective study. Int. Endod. J. 1995, 28, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Inamoto, K.; Kojima, K.; Nagamatsu, K.; Hamaguchi, A.; Nakata, K.; Nakamura, H. A Survey of the Incidence of Single-Visit Endodontics. J. Endod. 2002, 28, 371–374. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, M.; Figini, L.; Gagliani, M.; Lodi, G. Single versus multiple visits for endodontic treatment of permanent teeth. Cochrane Database Syst. Rev. 2016, 2016, CD005296. [Google Scholar] [CrossRef]
- Rao, K.N.; Kandaswamy, R.; Umashetty, G.; Rathore, V.P.S.; Hotkar, C.; Patil, B.S. Post-Obturation pain following one-visit and two-visit root canal treatment in necrotic anterior teeth. J. Int. Oral Health 2014, 6, 28–32. [Google Scholar] [CrossRef] [Green Version]
- Keskin, C.; Demiryurek, E.; Ozyurek, T. Postoperative Pain after Single-Versus-Multiple Visit Root Canal Treatment in Teeth with Vital or Non-Vital Pulps in a Turkish Population. Asian J. Sci. Res. 2015, 8, 413–420. [Google Scholar] [CrossRef]
- Siqueira, J.F.; Barnett, F. Interappointment pain: Mechanisms, diagnosis, and treatment. Endod. Top. 2004, 7, 93–109. [Google Scholar] [CrossRef]
- Jafarzadeh, H.; Udoye, C.I.; Aguwa, E.N.; Habibi, M. Flare-up Incidence and Related Factors in Nigerian Adults. J. Contemp. Dent. Pr. 2011, 12, 120–123. [Google Scholar] [CrossRef]
- Iqbal, M.; Kurtz, E.; Kohli, M. Incidence and factors related to flare-ups in a graduate endodontic programme. Int. Endod. J. 2009, 42, 99–104. [Google Scholar] [CrossRef]
- Tsesis, I.; Faivishevsky, V.; Fuss, Z.; Zukerman, O. Flare-ups after Endodontic Treatment: A Meta-analysis of Literature. J. Endod. 2008, 34, 1177–1181. [Google Scholar] [CrossRef]
- Sathorn, C.; Parashos, P.; Messer, H. The prevalence of postoperative pain and flare-up in single- and multiple-visit endodontic treatment: A systematic review. Int. Endod. J. 2007, 41, 91–99. [Google Scholar] [CrossRef]
- Siqueira, J.F. Microbial causes of endodontic flare-ups. Int. Endod. J. 2003, 36, 453–463. [Google Scholar] [CrossRef]
- Seltzer, S.; Naidorf, I.J. Flare-ups in endodontics: I. Etiological factors. J. Endod. 1985, 11, 472–478. [Google Scholar] [CrossRef]
- Torabinejad, M.; Kettering, J.D.; McGraw, J.C.; Cummings, R.R.; Dwyer, T.G.; Tobias, T.S. Factors associated with endodontic interappointment emergencies of teeth with necrotic pulps. J. Endod. 1988, 14, 261–266. [Google Scholar] [CrossRef]
- Priyanka, S. Flare-Ups in Endodontics—A Review. IOSR J. Dent. Med Sci. 2013, 9, 26–31. [Google Scholar] [CrossRef]
- Wang, C.; Xu, P.; Ren, L.; Dong, G.; Ye, L. Comparison of post-obturation pain experience following one-visit and two-visit root canal treatment on teeth with vital pulps: A randomized controlled trial. Int. Endod. J. 2010, 43, 692–697. [Google Scholar] [CrossRef]
- Wong, A.W.-Y.; Zhang, S.; Li, S.K.-Y.; Zhu, X.; Zhang, C.; Chu, C.-H. Incidence of post-obturation pain after single-visit versus multiple-visit non-surgical endodontic treatments. BMC Oral Health 2015, 15, 96. [Google Scholar] [CrossRef] [Green Version]
- Wong, A.W.-Y.; Tsang, C.S.-C.; Zhang, S.; Li, K.-Y.; Zhang, C.; Chu, C.-H. Treatment outcomes of single-visit versus multiple-visit non-surgical endodontic therapy: A randomised clinical trial. BMC Oral Health 2015, 15, 162. [Google Scholar] [CrossRef] [Green Version]
- Patil, A.A.; Joshi, S.B.; Bhagwat, S.; Patil, S.A. Incidence of Postoperative Pain after Single Visit and Two Visit Root Canal Therapy: A Randomized Controlled Trial. J. Clin. Diagn. Res. 2016, 10, ZC09–ZC12. [Google Scholar] [CrossRef] [PubMed]
- Alomaym, M.A.A.; AlDohan, M.F.M.; Alharbi, M.J.; Alharbi, N.A. Single versus multiple sitting endodontic treatment: Incidence of postoperative pain—A randomized controlled trial. J. Int. Soc. Prev. Community Dent. 2019, 9, 172. [Google Scholar] [CrossRef] [PubMed]
- Ghoddusi, J.; Javidi, M.; Zarrabi, M.H.; Bagheri, H. Flare-ups incidence and severity after using calcium hydroxide as intracanal dressing. N. Y. State Dent. J. 2006, 72, 24–28. [Google Scholar] [PubMed]
- Al-Negrish, A.R.S.; Habahbeh, R. Flare up rate related to root canal treatment of asymptomatic pulpally necrotic central incisor teeth in patients attending a military hospital. J. Dent. 2006, 34, 635–640. [Google Scholar] [CrossRef]
- Risso, P.; Cunha, A.; Araujo, M.; Luiz, R. Postobturation pain and associated factors in adolescent patients undergoing one- and two-visit root canal treatment. J. Dent. 2008, 36, 928–934. [Google Scholar] [CrossRef]
- Ince, B.; Ercan, E.; Dalli, M.; Dulgergil, C.T.; Zorba, Y.O.; Colak, H. Incidence of Postoperative Pain after Single- and Multi-Visit Endodontic Treatment in Teeth with Vital and Non-Vital Pulp. Eur. J. Dent. 2009, 3, 273–279. [Google Scholar] [CrossRef] [Green Version]
- Al-Omiri, M.K.; Iqbal, A.; Akbar, I. Flare-up Rate in Molars with Periapical Radiolucency in One-Visit vs Two-Visit Endodontic Treatment. J. Contemp. Dent. Pr. 2013, 14, 414–418. [Google Scholar] [CrossRef]
- Rana, S.A.A.; Akhtar, M.; Jameel, M.; Rana, M.A.; Nazir, A.; Kashif, M. Frequency of Post Obturation Pain after Single versus Multiple Visits Endodontic Therapy by using Hybrid Root Canal Preparation Technique. Int. J. Med. Res. Health Sci. 2019, 8, 78–84. [Google Scholar]
- Singh, A.; Kumar, A.; Nazeer, J.; Singh, R.; Singh, S. Incidence of postoperative flare-ups after single-visit and multiple-visit endodontic therapy in permanent teeth. J. Indian Soc. Pedod. Prev. Dent. 2020, 38, 79–83. [Google Scholar] [CrossRef]
- Vieyra, J.; Ocampo, F.; Acosta, O. Incidence of Flare-Ups and Apical Healing after Single-Visit or Two Visits Treatment of Teeth with Necrotic Pulp and Apical Periodontitis after a Two-Year Control Period. A Randomized Clinical Trial. 2018. Available online: https://clinicaltrials.gov/ct2/show/NCT02815189 (accessed on 23 October 2020).
- Garg, A.; Singh, S. Incidence of post-operative pain after single visit and multiple visit root canal treatment: A randomized controlled trial. J. Conserv. Dent. 2012, 15, 323–327. [Google Scholar] [CrossRef] [Green Version]
- Prashanth, M.B.; Tavane, P.N.; Abraham, S.; Chacko, L. Comparative Evaluation of Pain, Tenderness and Swelling followed by Radiographic Evaluation of Periapical Changes at Various Intervals of Time following Single and Multiple Visit Endodontic Therapy: An in vivo Study. J. Contemp. Dent. Pr. 2011, 12, 187–191. [Google Scholar] [CrossRef]
- Tarale, K. Post-operative Pain Analysis between Single Visit and Two Visit Root Canal Treatments using Visual Analogue Scale: An In Vivo Study. J. Dent. Allied Sci. 2013, 2, 8–15. [Google Scholar] [CrossRef]
- Riaz, A.; Maxood, A.; Abdullah, S.; Saba, K.; Din, S.U.; Zahid, S. Comparison of frequency of post-obturation pain of single versus multiple visit root canal treatment of necrotic teeth with infected root canals. A Randomized Controlled Trial. J. Pak. Med. Assoc. 2018, 68, 1429–1433. [Google Scholar]
- DiRenzo, A.; Gresla, T.; Johnson, B.R.; Rogers, M.; Tucker, D.; BeGole, E.A. Postoperative pain after 1- and 2-visit root canal therapy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2002, 93, 605–610. [Google Scholar] [CrossRef] [Green Version]
- Oginni, A.O.; Udoye, C.I. Endodontic flare-ups: Comparison of incidence between single and multiple visit procedures in patients attending a Nigerian teaching hospital. BMC Oral Health 2004, 4, 4. [Google Scholar] [CrossRef] [Green Version]
- Sindhu, S.; Nadig, R.R.; Pai, V.S.; Nair, S. Endodontic Flare Ups- An Overview. Int. J. Contemp. Med. Res. 2015, 2, 220–225. [Google Scholar]
- Jalali, P.; Hasselgren, G. Endodontic inter-appointment flare-ups: An example of chaos? Dent. Hypotheses 2015, 6, 44. [Google Scholar] [CrossRef]
- Trope, M.; Delano, E.O.; Ørstavik, D. Endodontic treatment of teeth with apical periodontitis: Single vs. Multivisit treatment. J. Endod. 1999, 25, 345–350. [Google Scholar] [CrossRef]
- González-Moles, M.A.; González, N.M. Bacterial infections of pulp and periodontal origin. Med. Oral Patol. Oral Cir. Bucal 2004, 9, 32–34. [Google Scholar]
- Sathorn, C.; Parashos, P.; Messer, H.H.; And, P.P. Effectiveness of single- versus multiple-visit endodontic treatment of teeth with apical periodontitis: A systematic review and meta-analysis. Int. Endod. J. 2005, 38, 347–355. [Google Scholar] [CrossRef]
- Oliet, S. Single-visit endodontics: A clinical study. J. Endod. 1983, 9, 147–152. [Google Scholar] [CrossRef]
- Caviedes-Bucheli, J.; Gutierrez-Guerra, J.E.; Salazar, F.; Pichardo, D.; Moreno, G.C.; Munoz, H.R. Substance P receptor expression in healthy and inflamed human pulp tissue. Int. Endod. J. 2006, 40, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Ekblom, A.; Hansson, P. A thin-section and freeze-fracture study of the pulp blood vessels in feline and human teeth. Arch. Oral Biol. 1984, 29, 413–424. [Google Scholar] [CrossRef]
- Eleazer, P.D.; Eleazer, K.R. Flare-up rate in pulpally necrotic molars in one-visit versus two-visit endodontic treatment. J. Endod. 1998, 24, 614–616. [Google Scholar] [CrossRef]
- Raju, T.B.V.G.; Seshadri, A.; Vamsipavani, B.; Abhilash, K.; Subhash, A.V.; Kumari, K.V.H. Evaluation of Pain in Single and Multi Rooted Teeth Treated in Single Visit Endodontic Therapy. J. Int. Oral Health 2014, 6, 27–32. [Google Scholar]
- Penesis, V.A.; Fitzgerald, P.I.; Fayad, M.I.; Wenckus, C.S.; BeGole, E.A.; Johnson, B.R. Outcome of One-visit and Two-visit Endodontic Treatment of Necrotic Teeth with Apical Periodontitis: A Randomized Controlled Trial with One-year Evaluation. J. Endod. 2008, 34, 251–257. [Google Scholar] [CrossRef]
- Peters, L.B.; Wesselink, P.R. Periapical healing of endodontically treated teeth in one and two visits obturated in the presence or absence of detectable microorganisms. Int. Endod. J. 2002, 35, 660–667. [Google Scholar] [CrossRef]
- Kvist, T.; Molander, A.; Dahlen, G.; Reit, C. Microbiological Evaluation of One- and Two-Visit Endodontic Treatment of Teeth with Apical Periodontitis: A Randomized, Clinical Trial. J. Endod. 2004, 30, 572–576. [Google Scholar] [CrossRef]
- Bashetty, K.; Hegde, J. Comparison of 2% chlorhexidine and 5.25% sodium hypochlorite irrigating solutions on postoperative pain: A randomized clinical trial. Indian J. Dent. Res. 2010, 21, 523–527. [Google Scholar] [CrossRef]
- Law, A.; Nixdorf, D.R.; Aguirre, A.; Reams, G.; Tortomasi, A.; Manne, B.; Harris, D.; National Dental PBRN Collaborative Group. Predicting Severe Pain after Root Canal Therapy in the National Dental PBRN. J. Dent. Res. 2015, 94, 37S–43S. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. no | First Author/Country/Year [Reference Number] | Sample after Dropouts (Groups) | Vital/Nonvital Tooth | Intra Canal Medicament | Pain Assessment [Pre/Postoperative] | Pain Assessment Scale | Follow up Visits Postoperatively | Outcome Measure (Pain/Flare) | Frequency/Incidence of Pain/Flare among Groups | Statistical Significance | Authors Conclusions/Suggestions |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | DiRenzo/USA/2002 [35] | 72 patients (Single visit: 39, Multiple visits: 33) | Vital and nonvital teeth | Sterile cavity | Preoperative and post obturation pain | Modified VAS | 6, 12, 24, and 48 h | Pain | Evenly distributed minimal pain within 24 to 48 h | No statistically significant difference | No difference in postoperative pain between two visits. |
| 2 | Oginni/Nigeria/2004 [36] | 222 patients (Single visit: 102, Multiple visits: 120) | Vital and nonvital teeth | Not mentioned | Preoperative Interappointment Post obturation | None/Slight/Moderate/Severe | 1st, 7th and 30th day | Pain/flare up | Flareups seen in both groups 10 flareups (Pain or swelling) in multiple visits 19 flareups in a single visit. | A significant difference was seen between single and multiple visits. | Higher incidence of post obturation pain and flareups following single-visit procedures. |
| 3 | Ghoddusi/Iran/2006 [23] | 60 patients (Single visit, Multiple visit, Multiple visit with intracanal medicament) | Nonvital teeth | Calcium hydroxide for 1 week | Postoperative | Modified VAS | Recalled after 72 h | Pain/swelling | The frequency of pain was seen more with multiple visits. Frequency/incidence of pain and swelling more in a single visit. | A significant difference in the incidence and severity of pain between multiple visits and pain/swelling between single and multiple visits. | Intracanal dressing (Calcium hydroxide) could be effective to decrease postoperative pain and swelling. |
| 4 | Al-Negrish/Jordan/2006 [24] | 112 (Single visit: 54 Multiple visits: 58) | Nonvital teeth | Calcium hydroxide for 1 week | Postoperative | No pain, slight pain, moderate pain, and severe pain | 2 and 7 days post obturation | Pain/swelling | The pain was seen in both groups. After 2 days, the flareup rate was 9.2% for a single visit and 13.8% for two visits. After 7 days the flareup rate was 1.8% for one visit and 5.2% for the two visits. | No significant difference in incidence and degree of postoperative pain. | There was no difference in the flareup rate between single and two appointment techniques. The rate of flareup was 11.6 and 3, 6 after 2 and 7 days, respectively |
| 5 | Risso/Brazil/2008 [25] | 118 patients (One visit: 57, Two visits: 61) | Nonvital teeth | Calcium hydroxide | Preoperative and post obturation | VAS | 10 day follow up [recorded after 6, 12 and 24 h and then 24 h during 9 following days] | Pain/flareup | The frequency of pain was seen in 10.5% (6/57) in one visit group and 23(14/61) in two visit group. Flareup was seen in 1.75% (1/57) in one visit group and 1.65% (1/61) in two visit group. | No statistically significant difference between the groups. | The pain was observed more in two visit group. No difference was seen in the intensity of post obturation pain. |
| 6 | Ince/Turkey/2009 [26] | 306 (single visit: 153, Multiple visits: 153) | Vital and nonvital teeth | Sterile cavity | Postoperative pain | No, mild, moderate and severe pain | 3 days post obturation | Pain | Postoperative pain occurred in 107 patients in a single visit and 106 patients in multiple visits. It occurred in 35 patients with vital pulp and 23 patients with nonvital pulp. | No significant difference in postoperative pain between the two groups | Postoperative pain after endodontic therapy is related to preoperative pain. |
| 7 | Wang/China/2010 [18] | 89 (one visit: 43, two visits: 46) | Vital teeth | Calcium hydroxide for 1 week | Preoperative and post obturation | Modified Verbal descriptor scale [VDS] | 6, 24, 48 h and 1 week after obturation | Pain/flareups | No pain or slight pain was observed between both groups. Flareup and slight swelling were seen in 1 in each group. | No statistically significant difference in the incidence and intensity of post obturation pain. | The experience of incidence and intensity of post obturation pain in vital teeth was similar following one or two-visit. |
| 8 | Prashanth/India/2011 [32] | 32 (single visit—vital pulp, necrotic pulp, multiple visit—vital pulps, necrotic pulp) | Vital and nonvital teeth | Not mentioned | Post obturation | Unclear (mild, moderate, severe) | 48 h (postoperative pain). 1 week, 4 to 6 weeks. | Pain/swelling/tenderness | After 48 h, pain in necrotic pulp groups. Tenderness in 25% in single visit vital teeth, 12.5% in single visit non vital and multiple visit vital teeth after 48 h. | No statistically significant difference was seen during the 48 h of follow up. | There was no difference in postoperative pain, tenderness/swelling between single and multiple visits. |
| 9 | Singh/India/2012 [33] | 188 (single visit: 94 two visits: 94) | Vital and nonvital teeth | Sterile cavity | Preoperative and postoperative pain | Modified Heft Parker visual analogue scale | 6, 12, 24 and 48 h | Pain | Incidence and intensity of post obturation pain were similar in both the groups, but the multivisit group experienced more pain compared to a single visit. | No significant difference was seen | Multivisit endodontics does not reduce the incidence of pain. |
| 10 | Tarale/India/2013 [34] | 60 patients (one visit: 20, two visits: 20 with medicament and without: 20) | Vital and nonvital teeth | Calcium hydroxide | Preoperative and post obturation | Modified VAS, | 6, 12, 24 and 48 h | Pain | After 6 h, one visit had more pain. No difference among all groups after 12, 24 and 48 h. | No statistically significant difference was seen after 6, 12, 24 and 48 h. | Postoperative pain was the same with a single and multivisit appointment with or without calcium hydroxide dressing. |
| 11 | Akbar/Saudi Arabia/2013 [27] | 100 patients (one visit: 50, two visits: 50) | Nonvital teeth | Calcium hydroxide | Post obturation | Not specified | Daily for 7 days | Flareups | 5 patients in one visit and 4 patients in two visits experienced flareups. | No statistically significant difference was seen with no of visits, age, and gender | Postoperative flareups have no relationship with one visit or two visits. |
| 12 | Rao/India/2014 [7] | 148 (single visit: 74, two visits: 74) | Nonvital teeth | Not mentioned | Post obturation | Modified VAS | After 6 h, 24 h, 48 h, and 7 days | Pain | The single-visit group experienced slightly less pain than two visit group at all study intervals | No statistically significant difference was seen | The post obturation pain was similar between patients treated either in one appointment or with two appointments. |
| 13 | Wong/China/2015 [19] | 538 (single visit: 275, multiple visits: 263) | Vital and nonvital teeth | Calcium hydroxide | Preoperative and post obturation | 10 point Likert scale—No pain to extreme pain | 1 week after obturation | pain | A day later, 68 teeth for a single visit and 88 teeth for two visits and after 7 days, 11 for a single visit, 14 for two visits had pain. | No significant difference in the incidence of post obturation pain after one day or seven days among the groups | The single visit group had a lower intensity of pain than the multiple visit group |
| 14 | Wong/China/2015 [20] | 220 teeth (single visit: 117, multiple visits: 103 teeth) | Vital and nonvital teeth | Calcium hydroxide for a week | Postoperative pain | 10 point Likert scale—No pain to extreme pain | 1 week after obturation and 18 months after treatment | Pain/tenderness on percussion | Postoperative pain after 1 week, 21% in a single visit and 12% in multiple visits. After 18 months it was 0.9% and 1.0%, respectively. | No statistically significant difference was seen. | The prevalence of postoperative pain was the same between the two treatment groups. |
| 15 | Keskin/Turkey/2015 [8] | 288 patients (single visit: 140, Multiple visits: 148) | Vital and nonvital teeth | Calcium hydroxide | Postoperative pain | VAS | 24, 48 and 72 h | Pain | The intensity of pain reduced over the followup. The majority of patients from both groups reported no pain. | No significant difference in the incidence of postoperative pain. | No difference was seen between single vs. multiple visits. The intensity of postoperative pain does not depend on the vitality of the pulp, gender, and tooth type. |
| 16 | Patil/India/2016 [21] | Single visit: 32, Two visits: 33 | Vital and nonvital teeth | Sterile cavity | Preoperative and postoperative pain | Modified Heft-Parker VAS | 6 h, 12 h, 24 h, and 48 h, respectively. After 1 week clinical evaluation of pain was done | Pain | The incidence of pain was higher in the multivisit group when compared to the single-visit group after 6 h, 12 h, and 24 h. After 48 h, there was no difference in pain experienced between the two groups | No significant difference was seen | Multiple visit endodontics does not reduce the pain incidence. Incidence of pain is the same when compared between one visit or two visits. |
| 17 | Riaz/Pakistan/2018 [34] | Single visit: 30, Multiple visits: 30 | Nonvital teeth | Calcium hydroxide for 5 days | Preoperative and postoperative | VAS | 48 h | Pain | The pain was observed in 2 patients in a single visit and 3 patients in multiple visits | No statistically significant difference between the two groups | Pain frequency is similar in a single visit or multivisit |
| 18 | Vieyra/USA/2018 [26] | 97 (one visit: 46, two visits: 51) | Nonvital teeth | Calcium hydroxide for 1 week | Postoperative pain | No, mild, moderate and severe pain | 2 year follow up | pain/swelling | Moderate pain was observed in 5% of the treatment cases and 16.67% of the retreatment cases. | Statistically, a significant difference was seen with the occurrence of flareups when comparing treatment cases with retreatment cases. | A higher incidence of flareups was seen in teeth that require retreatment than the primary treatment. |
| 19 | Rana/Pakistan/2019 [28] | 140 (single visit: 70, two visits: 70) | Vital teeth nonvital teeth | Sterile cavity | Preoperative Post operatively pain | Heft-parker VAS | 24 h | Pain | The pain was less in single visit (18 patients) than two visit group (38 patients) | A highly statistically significant difference was seen between both groups | Single-visit endodontic therapy is better than multiple visits endodontic about post obturation pain. Post obturation of pain was not related to age and gender. |
| 20 | Alomaym/Saudi Arabia/2020 [22] | 390 patients (single visit: 195, multiple visit: 195) | Vital and nonvital teeth | Calcium hydroxide | Preoperatively | VAS, Modified Heft Parker | 6,12,24 and 48 h post obturation | Pain/flare ups | Incidence and intensity of pain were more in a single visit. | No statistically significant difference was seen between multiple visits and a single visit | The incidence of pain was more in a single visit when compared to multivisit. |
| 21 | Konark/India/2020 [29] | 64 (single visit: 32, multiple visits: 32) | Vital teeth | Not mentioned | Preoperative and post obturation | VAS | 24, 48, 72 (h), 1 week, 1,3,6 and 9 (months) | Flareups (Pain, discomfort, swelling, tenderness on percussion, etc.) | At all intervals, postoperative pain was more in the multivisit group when compared with a single visit group except 24 and 48 h interval. Incidence of discomfort and swelling was less in a single visit | Statistically, a significant difference was seen concerning discomfort, gingival swelling, and tenderness to percussion between groups. | Single-visit endodontic therapy showed encouraging results. Postoperative pain was higher in multiple visits compared to the single-visit group. |
| S.no | First Author/Country/Year [Reference Number] | 1. Was True Randomisation Used for the Assignment of Participants to Treatment Groups? | 2. Was Allocation to Treatment Groups Concealed? | 3. Were Treatment Groups Similar at the Baseline? | 4. Were Participants Blind to Treatment Assignments? | 5. Were Those Delivering Treatment Blind to Treatment Assignment? | 6. Were Outcomes Assessors Blind to Treatment Assignment? | 7. Were Treatment Groups Treated Identically other than the Intervention of Interest? | 8. Was Follow up Complete and If Not, Were Differences between Groups in Terms of Their Follow up Adequately Described and Analyzed? | 9. Were Participants Analyzed in the Groups to which They Were Randomised? | 10. Were Outcomes MEASURED in the Same Way for Treatment Groups? | 11. Were Outcomes Measured Reliably? | 12. Was Appropriate Statistical Analysis Used? | 13. Was the Trial Design Appropriate, and any Deviation from the Standard RCT Design Accounted for in the Conduct and Analysis of the Trial? | The Overall Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | DiRenzo/USA/2002 [35] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 2 | Oginni/Nigeria/2004 [36] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 3 | Ghoddusi/Iran/2006 [23] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 4 | Al-Negrish/Jordan/2006 [24] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 5 | P.A. Risso/Brazil/2008 [25] | Yes | No | Unclear | NO | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 6 | Ince/Turkey/2009 [26] | Yes | No | Unclear | NO | NO | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 7 | Wang/China/2010 [18] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 8 | Prashanth/India/2011 [32] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 9 | Singh/India/2012 [33] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 10 | Tarale/India/2013 [34] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 11 | Akbar/Saudi Arabia/2013 [27] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 12 | Rao/India/2014/ [7] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 13 | Wong/China/2015 [19] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 14 | Wong/China/2015 [20] | Yes | No | Unclear | No | No | no | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 15 | Keskin/Turkey/2015 [8] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 16 | Patil/India/2016 [21] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 17 | Riaz/Pakistan/2018 [34] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 18 | Vieyra/USA/2018 [26] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 19 | Rana/Pakistan/2019 [28] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 20 | Alomaym/Saudi Arabia/2020 [22] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
| 21 | Konark/India/2020 [29] | Yes | No | Unclear | No | No | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vishwanathaiah, S.; Maganur, P.C.; Khanagar, S.B.; Chohan, H.; Testarelli, L.; Mazzoni, A.; Gupta, A.A.; Raj, A.T.; Bhandi, S.; Mehta, D.; et al. The Incidence and Intensity of Postendodontic Pain and Flareup in Single and Multiple Visit Root Canal Treatments: A Systematic Review and Meta-Analysis. Appl. Sci. 2021, 11, 3358. https://doi.org/10.3390/app11083358
Vishwanathaiah S, Maganur PC, Khanagar SB, Chohan H, Testarelli L, Mazzoni A, Gupta AA, Raj AT, Bhandi S, Mehta D, et al. The Incidence and Intensity of Postendodontic Pain and Flareup in Single and Multiple Visit Root Canal Treatments: A Systematic Review and Meta-Analysis. Applied Sciences. 2021; 11(8):3358. https://doi.org/10.3390/app11083358
Chicago/Turabian StyleVishwanathaiah, Satish, Prabhadevi C Maganur, Sanjeev B Khanagar, Hitesh Chohan, Luca Testarelli, Alessandro Mazzoni, Archana A Gupta, A. Thirumal Raj, Shilpa Bhandi, Deepak Mehta, and et al. 2021. "The Incidence and Intensity of Postendodontic Pain and Flareup in Single and Multiple Visit Root Canal Treatments: A Systematic Review and Meta-Analysis" Applied Sciences 11, no. 8: 3358. https://doi.org/10.3390/app11083358