1. Introduction
Regenerative medicine has developed tremendously in recent years, in fields like skin regeneration and wound healing. Age, traumas, tumors, congenital defects and other degenerative diseases are some of the reasons why this branch of medicine is becoming commonly used and under development [
1,
2].
Nowadays, diseases with difficult prognosis entail other approaches that can help improve outcomes. In addition, this approach can be used in a wide range of organ systems and contexts, namely dermal wounds [
3,
4]. The main purpose is to replace or regenerate damaged tissues. Therefore, regenerative therapy applies differentiated cells, stem cells with specific characteristics, to regenerate damaged tissues [
1,
2].
Stem cells, being the future of regenerative medicine, are one of the most researched topics in the scientific community. These undifferentiated cells are capable of differentiation into different cell lines, as well as unlimited proliferation [
1,
5].
In matters of potency the only totipotent stem cells are those derived from the blastomere, being able to differentiate into every cell of the organism. The blastocyst-derived stem cells can differentiate into every cell, except the placenta, and are thus classified as pluripotent. Cells originated from the fetus are considered multipotent, being capable of generating limited cell lineages [
1,
6].
There are several types of stem cell and they are used due to their therapeutic potential, thought to derive essentially from their secreted cytokines [
7,
8]. These cells are capable of self-renewal and can be very useful in treating skin diseases where no other treatment was proven efficient, in chronic diseases and even in wound regeneration [
7,
8]. Stem cells can be used either directly in the damaged tissue or through scaffolds encapsulating these cells [
1,
9].
Nowadays, skin diseases, specifically chronic wounds, require a lot of attention, as they are associated with very expensive and usually ineffective treatment processes. Therefore, the exploitation of the regenerative therapies’ potential in this domain is very relevant [
10].
This review analyses the most relevant stem cell types used in skin regeneration and tissue engineering techniques used to deliver them. Also, a discussion on the importance and potential of the application of cell/scaffold-based therapies on wound healing, as well as other technologies like hydrogels and three-dimensional (3D) models, is addressed.
2. Skin Anatomy and Histology
The skin performs fundamental functions like maintaining homeostasis (regulating the body temperature through sweat) and the protection of the internal organs from the outside environment [
11]. Moreover, this organ has the capability of self-healing and renewal. It includes three different layers: epidermis, dermis and hypodermis (
Figure 1). The epidermis is composed mainly by the
stratum granulosum,
stratum lucidum,
stratum corneum,
stratum spinosum and
stratum basale, and is also responsive for the external stimuli because of its abundant nerve endings. The dermis is important to maintain the skin’s elasticity and structure since this layer is rich in fibroblasts. Finally, the hypodermis is able to store energy and preserve the body temperature since it consists principally of adipose tissue and blood vessels [
12].
Moreover, the skin is a complex organ constituted by different tissues that, when intact, can provide protection from microorganisms as well as other external environmental aggressions. However, in cases when this barrier is breached, for example in wounds, various cell types work together with signaling factors and matrix interaction to re-establish the tissue function and integrity [
13].
3. Mechanisms of Injury and Healing
Skin injury occurs due to direct exposure to potentially harmful mechanical, thermal, chemical or microbial action. The most important cells in regeneration are the tissue-resident stem cells, that have the capability of self-renewing, as well as to differentiate in more specialized cell types and achieve homeostasis. Therefore, when the local and systemic environments change completely, these stem cells exhibit notable plasticity [
13,
15].
The adult skin has two different ways of responding to wounds: regeneration or repair. Wound regeneration means that the tissue is capable of replacing the damaged cells for new, fully functioning normal cells, with no scar formation. On the other hand, wound repair refers to the inability to produce normal cells, and therefore fibrotic tissue is produced and consequently a scar is observed [
16,
17]. As a result, immediately after an injury, hemostasis occurs, which is followed by other processes such as vasoconstriction, coagulation pathway activation, thrombosis and release of cytokines. Therefore, a wound, depending on the extent of the injury, can heal in one/two weeks naturally, in healthy skin [
12,
18,
19,
20].
The epidermis in mammals consists in a stratified squamous epithelium that is maintained by the consecutive proliferation and differentiation of cells from the basal layer. As cells differentiate, they give rise to suprabasal cells, granular layer cells and enucleated corneocytes [
21]. Being the most exposed layer of the skin, the epidermis suffers constant injuries and needs to rapidly re-epithelialize to close the lesion site. Furthermore, the epithelial cells and the fibroblasts in the dermis have to migrate and proliferate. In case the wound is not successfully closed, dehydration, inflammation and, in more severe cases, death can occur [
21].
When a lesion occurs, fibroblasts and macrophages respond by releasing growth factors that promote fibroblast migration and further proliferation, as well as inflammatory cytokines that induce an immune response. Also, fibroblasts are responsible for the production of collagen and extracellular matrix (ECM) proteins that contribute to fibrosis and scar formation [
21]. In the wound site, the accumulation of macrophages and immune cells occurs with the purpose of eliminating microorganisms and to produce growth factors to aid in fibroblast repopulation, re-epithelization and ECM remodeling [
21].
The wound suffers different stages until the skin barrier is stable again, otherwise a disturbance in the normal process of wound healing can advance to the development of a chronic wound [
22]. A chronic wound is characterized as loss of skin or other tissues that were not able to heal throughout the normal time that is required. In addition, the treatment of these wounds can be long-lasting and create a huge challenge for contemporary medicine [
23,
24]. Therefore, there is a huge necessity to develop different methods that can target the complex biology of chronic-wounds. Some new approaches based on using biomaterials, biologics and cell-based therapies are emerging, and knowing the importance of abnormal inflammation, some studies are focusing on the importance of the immunomodulatory therapies [
25,
26]. The enhancing of wound healing using active agents-incorporated bioactive wound-dressings, as well as skin equivalents to repair and regenerate specific skin compartments, are also being explored [
26].
The wound delay can be provoked by a number of factors, such as renal disease, diabetes, trauma, advanced age and obesity [
15,
22]. Moreover, other local factors like infection, exudates, hypoxia and ischemia can impact in the healing process. Therefore, stem cells have a therapeutic application in cases where the wound-healing process is compromised. Besides, mesenchymal stem cells (MSC)-induced vascular endothelial growth factor (VEGF) production can also promote skin regeneration [
27]. When there are metabolic diseases associated with the skin lesion, proper treatment for the disease should be taken into consideration [
28].
4. Types of Wound
A wound consists in any disorder or injury that occurs in the skin and can be either open or closed depending on their nature [
29]. The difference is that when the skin is punctured, cut or torn the wound is named open [
10].
Wounds can be categorized as acute or chronic depending on their causes and consequences. They are caused by trauma, pressure, burns or cuts. Normally, acute wounds go through an appropriate and organized process which results in a rapid reestablishment of anatomical and functional integrity. On the other hand, chronic wounds have four main types: post-surgical wounds, venous ulcers, diabetic ulcers and pressure ulcers. These wounds have heterogeneous etiology and presentation, cannot achieve normal integrity, and the healing process is delayed by around three months. In association there can be an infection, biofilm formation, high protease activity, recurrent injury (neuropathy), gangrene, hypoxia or ischemia. Moreover, the process of healing is determined by different factors such as the patient’s age, environment or the presence of other diseases [
20,
28,
30].
A perfect healed wound is characterized by an area that returns to normal anatomical structure, appearance and function after the injury. In addition, a minimally healed wound is defined by the restoration of anatomical continuity without achieving sustained function results, which means that the wound can reappear [
30,
31]. Wound evaluation and further classification includes numerous factors such as the determination of the wound perimeter, surface area and tissue viability [
30,
31].
In cases where the skin contacts directly with the external environment, various types of damage can occur, such as burns, ulcers or wounds. This can result in the loss of variable volumes of extracellular matrix in the dermal or epidermal layer. Moreover, according to the depth, wounds can be categorized as epidermal, deep partial-thickness, superficial partial-thickness and full-thickness [
32].
5. Phases and Complications of the Wound-Healing Process
Wounds have diverse causes, namely injuries, pathologic conditions or even surgeries. There are four phases that characterize wound healing: hemostasis, inflammation, granulation/proliferation and tissue reconstruction/remodeling (
Figure 2). If these steps do not occur in a consecutive order and at the appropriate moment, the healing process is compromised and will fail or be abnormal. In addition, there can be complications such as the development of chronic wounds, infections and even keloids or hypertrophic scars derived from an excessive wound-healing process [
28,
31,
33]. The main causes of chronic wounds are diabetic disease or other metabolic pathologies, inappropriate keratinocytes proliferation, some medications (chemotherapeutic drugs, glucocorticoid steroids, non-steroidal anti-inflammatory drugs), impaired angiogenesis, severe wounds extended into the dermis or even deeper layers, and lack of appropriate coverage. All these conditions contribute with a moist environment for the wound bed that provides protection [
28].
Promptly after the skin injury, a blood clot and a platelet plug seals the wound temporarily, and this mechanism prevents blood loss and initiates the molecular cascade [
31]. Therefore, in the first phase, hemostasis and inflammatory response occur, and the damaged epithelial and the blood clot release chemotactic factors to recruit immune cells that have a major role in the inflammation. This phase is important to prevent infections and remove necrotic and apoptotic cells from the lesion site. The feedback to the inflammatory cues is the appearance of neutrophils, followed by circulating monocytes that differentiate into mature tissue macrophages and mast cells afterwards [
28,
31]. In the second phase, these cells secrete chemokines and other molecules (IL-1α, IL-33), such as growth factors (TGF-β), that help in the development of granulation tissue and migration/proliferation of fibroblasts and keratinocytes. These cells also secrete some toxic mediators such as reactive oxygen species and proteases that can be destructive to the surrounding tissues [
31]. Therefore, the excess of these cells infiltration (especially macrophages and neutrophils) and the delayed inflammation might restrain rather than enhance the process of healing. Therefore, this can be a cause of chronic wound situation and the constant tissue-destroying nature of this type of wound [
28,
31]. In the third phase, a re-epithelialization occurs, as well as wound contraction, important to the next phases of tissue remodeling [
34,
35]. The tissue remodeling phase is defined by declined cellularity and matrix remodeling. Consequently, originally disordered collagen fibers are cross-linked and rearranged [
31].
There are several techniques to target the healing phases using different materials and bioactive molecules. Antibiotic drugs can be used to prevent and clear bacterial colonization in early phases. Moreover, growth factors like epidermal growth factor (EGF), platelet-derived growth factor (PDGF) or basic fibroblast growth factor can stimulate growth and proliferation in a middle stage of the healing process [
20,
34]. Another example is the use of immunomodulatory molecules (IL-4) to modulate macrophages function to achieve wound repair. Therefore, a lot of techniques and strategies can be used to help regenerate skin tissue and accelerate the healing process [
34,
36].
However, when the process is disordered, chronic wounds are created, exhibiting persistent inflammation, biofilm development, microorganism recruitment and release of platelet-derived factors. Therefore, growth factors are truly important since they are the focal regulatory points of repair. In normal wounds when the dermal defect is closed, and the epithelization complete there are signals to stop the repair process. However, when these signals are inefficient, the process of repair may continue and form an excessive scar [
30,
37].
The main physical manifestations of chronic wounds can be described as necrosis, persistent inflammation and exudation. Concerning the exudate components, they can have destructive effects in the wound because of their corrosive potential, resulting in continuous extracellular matrix degradation. Moreover, the presence of exudate can be the first indicator of systemic complications [
30].
6. Recent Innovative Strategies in Wound-Healing Regeneration
Recent studies support the concept that MSCs can be appropriated for treating chronic wounds. Moreover, autologous stem cells are the most popular approach, mainly MSCs derived from adipose tissue (ASCs) and from the bone-marrow (BM-MSCs). However, umbilical cord blood was also mentioned because of the beneficial effects shown on wound healing [
23,
38,
39].
The skin tissue engineering process is truly complex because it relies on various factors: the appropriate choice of biomaterial, the design of a convenient platform (to mimic functional and structural properties of skin) and cell selection. One of the aims is to develop scaffolds containing cells and other molecules to restore damaged tissues. Moreover, the matrix provided by the scaffold is good for the cells to reside and proliferate, but it also needs instructive cues to multiply in a regenerative microenvironment [
34]. For instance, continued and slow release of molecules, such as growth factors from scaffolds, can help in the skin regeneration process. The combination of stem cells and a 3D biomaterial printing (capable of mimicking the extracellular matrix) has several advantages, such as the regeneration properties placed locally [
3]. This technique limitations are related to the biomaterials properties that need to be compatible with the cells and the printing requirements [
3].
The primary features that the hydrogel scaffold needs to have are biocompatibility, anti-bacterial capacity, proper mechanical characteristics, injectable capacity and water retention [
40]. Furthermore, the ability to sustain damage by external forces, maintaining the stability of its structure, is fundamental. The injective capacity is relevant due to the ability to attach to the wound (long term) and an excellent cell biocompatibility that is capable of increasing differentiation and proliferation [
40].
On the other hand, there are still several points that need improvement, such as the crosslinking reagents added to hydrogels. They are necessary because otherwise the hydrogels would have weak mechanical properties, which means they would be incapable of maintaining their shape and size [
41].
The process of healing is based on four healing phases, as mentioned before, which implicate interactions between different cell types, a platform and bioactive factors [
34]. In addition, structural engineering of scaffolds or hydrogels is another approach, which obligates the study of different matrices and their properties. It is important to consider that a particular design of a scaffold is appropriate for each specific type of wound [
42,
43].
In addition, 3D bioprinting of skin is a promising technology which has long been anticipated in the fields of drug and cosmetic development, mainly due to the decrease of ethical issues related to animal testing. This innovative technology allows the production of in vitro skin tissues for wound healing applications and shows great potential in fields like transplantation and development of skin equivalents [
42,
43]. In 2015, Procter and Gamble (P&G) and Rokit started working on research projects that focus on bioprinted human skin models [
42,
43]. Recent studies have shown successful bioprinted skin tissue containing two different cell types (fibroblasts and keratinocytes) and have achieved promising results. Nevertheless, for this technologies to reach their full potential, there are still several challenges that need to be surpassed [
43].
7. Cell-Based Therapies in Wound Healing
The clinical application of living cells in regenerative medicine should always be undertaken under good manufacturing practices (GMP) standards. This means that any skin substitute development involving living cells implies a quality control programme previously defined and validated [
2,
44].
The role of stem cells in wound healing is not fully understood until this day. However, it is known that they are responsible for the removal of necrotic and dead cells, wound vascularization, diminishing scar formation, wound contraction and inducing re-epithelization. All these factors mean that stem cells favour wound healing and help reduce local inflammation. In addition, MSCs probably use signaling as the most important mechanism to induce regeneration [
3,
16,
17,
28].
Under stimulation of various inflammatory cytokines, the transplanted MSCs release plenty of growth factors that coordinate various activities. Endothelial cells, fibroblasts and stem cells are triggered to promote tissue repair by stimulating proliferation, migration and differentiation of the most important cell types (keratinocytes and fibroblasts), increasing angiogenesis and restraining leukocyte transmigration [
45]. Moreover, MSCs have the capability to release immunosuppressive factors that suppress immune cells proliferation, and this anti-inflammatory effect helps to reduce the scar and optimize tissue repair [
28,
46]. The skin regeneration varies upon the wound’s microenvironment, which depends itself from systemic factors (like systemic diseases or inflammation) [
7].
Stem cell secretome, such as conditioned media or purified exosomes, is another viable therapeutic option. It helps to solve some problems related to living cells such as infection transmission, tumorigenicity and immune compatibility. In addition, MSCs-derived exosomes-extracellular nano-vesicles that transfer active cargoes between cells-are another promising therapy that can promote cell migration, proliferation, angiogenesis and re-epithelization [
23,
35].
8. Mesenchymal Stem Cells
MSCs were initially characterized by Friedenstein’s group as being similar to fibroblasts and adherent to plastic surfaces. Also, these cells were first discovered in the bone marrow [
47,
48]. In addition, they are defined by the International Society of Cellular Therapy as cells with plastic-adherence ability and that are capable of in vitro differentiation into three different cell lines (adipocytic, osteoblastic and chondrocytic). Moreover, they have the ability to express the surface markers CD73, CD90 and CD105 and do not exhibit hematopoietic markers such as CD14, CD45, CD34, CD19/HLA-DR and CD11b/CD79 [
5,
7]. They can be isolated from different tissues such as bone marrow, adipose tissue, umbilical cord, umbilical cord blood, placenta, dermis and nerve tissue [
5,
7]. These cells persist in the lesion site even after it has healed and are responsible for scars development, fibrosis, inflammation, angiogenesis and formation of granulation tissue [
5,
18,
49].
MSCs have immunosuppressive and immunomodulatory characteristics (releasing cytokines, growth factors and chemokines) which makes them a great option for allogeneic transplantation [
9,
16,
18,
49]. Furthermore, the MSCs’ conditioned medium has also been shown to stimulate the regeneration of damaged tissues [
5,
50,
51,
52,
53,
54].
8.1. Bone Marrow Mesenchymal Stem Cells
BM-MSCs are the most well-described MSCs, having weak immunogenicity (important for transplants) and possessing a promising wound-healing capacity [
16,
55].
On the other hand, this type of mesenchymal stem cells has a very invasive harvest method, which consists in aspiration from the iliac crest. Therefore, it requires anesthesia and has risks for the patient, which, in comparison with adipose-derived stem cells, represents a disadvantage. Furthermore, the number of cells collected from this method is usually low [
7,
55,
56].
BM-MSCs have been used in several studies and have shown efficacy regarding chronic wounds [
3,
7,
16].
8.2. Adipose-Derived Stem Cells
Adipose tissue is another source of multipotent stem cell. Moreover, these cells have identical characteristics in comparison to BM-MSCs. ASCs can differentiate into several lineages (chondrogenic, osteogenic, myogenic and adipogenic) as a feedback to specific stimuli [
19,
57]. These cells are heterogeneous, pluripotent and are isolated using liposuction aspirates or excised fat samples. Therefore, they can be obtained with minimal donor morbidity. For that reason, ASCs are easier to obtain in comparison to BM-MSCs due to reduced patient discomfort [
7,
23].
In addition, ASCs can be immediately administered after collection, which means these cells do not need to suffer differentiation in culture or in vitro expansion. As a result, this eliminates the time-consuming steps of in vitro expansion, which makes it quicker to use these cells in comparison with BM-MSCs [
7,
23].
Furthermore, studies have shown that allogeneic T lymphocytes do not proliferate in ASCs culture as a consequence of the cell surface histocompatibility antigen reduction, which inhibits mixed lymphocyte reaction. This fact suggest that ASCs are more suitable for autotransplantation due to their immunocompatibility [
12,
19]. Also, ASCs can be applied in tissue regeneration since the application of these cells accelerates the re-epithelialization of cutaneous wounds by promoting human dermal fibroblast proliferation directly (cell contact) or by paracrine secretion (growth factors) [
12,
19]. Furthermore, the regeneration potential of these cells is being evaluated, focusing on diverse medical problems like burn wounds and diabetic ulcers [
3].
8.3. Umbilical Cord Derived and Extra-Fetal Tissue Stem Cells
Another source of hematopoietic stem cells that can be used for various treatments is human umbilical cord blood. Other alternative stem cell sources are the extra fetal tissues such as Wharton’s jelly, placental tissue, amniotic tissue and umbilical cord-lining tissue [
7].
Stem cells isolated from the umbilical cord have been designated as umbilical cord MSCs (UC-MSCs), represented in
Figure 3. Normally, these cells exhibit functional and immunophenotypic characteristics identical to BM-MSCs. For this reason, UC-MSCs can be used to promote regeneration and tissue repair and are considered a promising alternative to BM-MSCs [
57]. The possibility to differentiate into epidermal tissue has been shown, suggesting the potential of UC-MSCs clinical application [
7,
13,
22,
57].
8.4. Skin Stem Cells
The skin is the largest organ in the human body, being a protective barrier between the external and internal environment [
15]. This organ exhibits enormous regenerative potential since it possesses different stem cell types, responsible for maintaining homeostasis and regulating skin damage. These cells are present in different compartments of the skin; in the epidermis there are three stem cell populations (interfollicular, sebaceous glands and bulge area) which are responsible for the superficial layer homeostasis.
Since epidermal stem cells (EPSCs) are a multipotent type of stem cell, they are fundamental to the differentiation and formation of the functional epidermis. The dermis possesses stem cells from the dermal papilla of hair follicles and a population of perivascular stem cells [
7,
58].
However, among these different populations of stem cells, EPSCs are of particular interest because of their accessibility and abundance. Keratinocytes are the most relevant cells that belong to the EPSCs population. In addition, these cells are easy to obtain which means there are no ethical issues concerning their use [
28].
It is important to note that an efficacious treatment to increase skin regeneration and wound healing would be the stimulation of these cell populations. For example, in full-thickness wounds (damage extends into subcutaneous tissue or even beyond, muscle and bone) cells from hair follicles migrate to the wound site, which means these cells contribute to wound healing. Langton et al. validates this fact by demonstrating a delay in early stages of wound healing in mutant mice which did not possess hair follicles [
22,
59].
Epidermal Stem Cells in Cutaneous Wound Healing
As previously mentioned, wound healing is truly important to repair skin defects and to achieve tensile strength and barrier function. However, serious damage that exceeds the skin regenerative capacity threatens the organism and an effective treatment is required. Concerning wound treatment, it should be long-lasting and depends upon specific medical skills, which constitutes a major challenge. That is the reason why EPSCs are considered a promising choice since they are simple to isolate, accessible and possess skin regenerative capacity [
58].
Skin grafts (autografts and allografts) have an important role in wound healing, but face some limitations such as the donor site, immune rejection, infection and scarring. In situations like extensive burns, less skin is available for grafts, so skin substitutes are a promising choice, such as Nile Tilapia fish skin (NTFS) [
28,
60].
The commercial skin substitutes consist of a matrix with or without cells that replaces the skin and mimics its functions, which has some limitations like the lack of appropriate mechanical properties. However, the failure of these substitutes is associated with low content of EPSCs, which means that the enrichment with these cells can form an ideal self-renewing epidermis [
28,
58].
Concerning nerve regeneration, one of the most usual peripheral nerve injuries results from transactions, which usually happens because of skin penetrating trauma, compression and over-stretching. There are a few therapeutic options and grafts that can be a viable option (autologous grafts and allografts) [
61].
The therapeutic strategies most used are the skin substitutes and cultured epidermal autografts (CEAs), which are derived from unpurified cell cultures from the epidermis (containing EPSCs). However, since chronic wounds have a complicated pathogenesis, sometimes many grafts and skin substitutes do not work as expected. The negative cycle of excessive inflammation and dysregulation of matrix metalloproteinases can be interrupted with a transplantation of CEAs enriched with EPSCs on a compatible extracellular matrix [
58].
See
Table 1 for an overall summary of the different types of MSCs and their advantages and limitations.
9. Stem Cell Delivery Methods
Regarding treatment, cell delivery methods are a very important aspect that is often neglected [
62]. Stem cells can be applied in several ways: systemically, which does not allow local specific treatment and is less efficient as local injections; topical, which is an excellent alternative in cases of skin wounds; and bioscaffolds, which are the most promising delivery method (
Figure 4) [
7,
63].
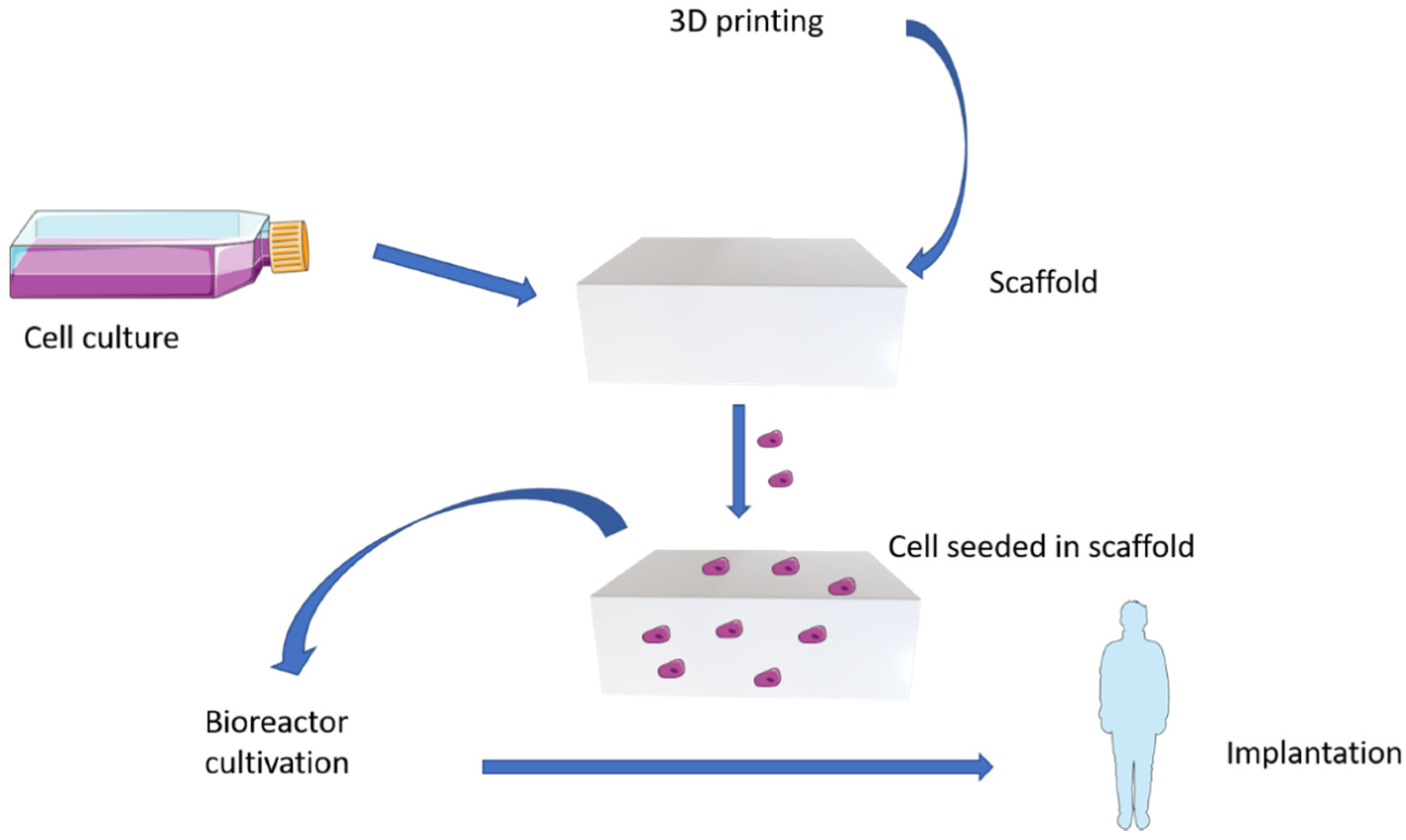
Bioscaffolds are 3D-printed with biocompatible materials generating 3D patterns, which enable the incorporation of cells (in this case stem cells) or biomolecules that remain viable. They are composed of natural organic materials, synthetic organic materials or even inorganic porous materials, allowing stem cells to be seeded in controlled spaces, protected and promoting their self-renewal and survival [
7,
64,
65,
66,
67]. The advantages of this method are due to the ability to produce an identical scaffold with homogeneous distribution, that can incorporate an identical and well-defined dose, being easy to apply [
64,
65,
66]. In addition, some studies have shown that using bioscaffolds accelerates wound healing when compared to other techniques, increasing cell graft longevity, remodeling of ECM and improving cell viability [
7,
14,
62]. Thus, when compared with intradermal injection, bioscaffolds have shown better results in wound healing, reducing scar formation and improving the skin’s biomechanical properties [
63].
On the other hand, there are some disadvantages in the use of stem-cell therapies, for example, the delivery methods that are not yet optimized, the best stem cell populations are not identified yet and there is a risk of tumorigenicity and immunogenicity. The wound itself can have a hostile environment for stem cells due to inflammation, hypoxia or even oxidative stress. Also, topical application does not allow the control of cell density that is placed locally and delivers the cells in a non-protected way [
7].
10. In Vitro Models
The convenient use of different models (in vitro/in vivo) is relevant for wound-healing studies, better understanding of the mechanism present in the cascade and to discover improved ways of enhancing healing, thereby preventing abnormal scars [
33,
68]. For instance, in vitro models allow a different approach since it is possible to make a direct quantitative examination, in specific cell types, of a certain effect without taking into consideration other factors. Despite the valuable information provided by the in vitro models they do not completely correlate with the in vivo reaction/effect [
68].
There are different in vitro models of tissue repair that can help us to understand cell signaling in response to cell injury or stress. For example, in optimal conditions, keratinocytes derived from a skin biopsy can be expanded in vitro to generate cultured epithelial autografts in three to four weeks [
22].
The in vivo models are needed since the in vitro ones do not represent the mechanisms and interactions present in the skin itself, like cells metabolism, signaling mechanisms, and the effect of the extracellular matrix concerning structure [
68].
Regarding wound healing, most assays use two-dimensional (2D) cell cultures or cells in monolayer, due to the availability of the materials needed. However, it has become more common to perform these assays in 3D models, capturing better the complexity of the human skin and cell to cell interactions in the process of skin healing [
33].
In 2D cell culture, the wound healing assay consists in damaging the confluent monolayer (wounding) to create a cell-free space in which cells can proliferate in order to repair the damage. There are several methods, the most common being the scratch assay which is mechanical. Other methods used are thermal (excessive heat), optical (laser) or electrical wounding (pulses of high voltage) [
33]. The main advantage of the scratch assay is its simple protocol in which a sharp object is used to destroy the monolayer. Afterwards, cell migration is recorded and analyzed. On the other hand, the disadvantages are the possible irregularity of the scratches and extracellular matrix coatings destruction [
33]. Another mechanical method is stamping (destroying the cells by crushing them) which has the advantage of not destroying the extracellular matrix when compared to the previous one [
33].
The 3D wound-healing model is not yet standardized, but it consists in different models of skin substitutes and the data analysis is mainly histological [
33].
11. In Vivo Models
Human stem cells can provide substantial opportunities, contributing with differentiated and undifferentiated cells that can be used in drug discovery, gene therapy and regenerative medicine. Moreover, stem cells can also be transduced ex vivo and the manipulated cells reintroduced into the host, which means another therapeutic approach for some specific diseases [
10].
However, the selection of the most appropriated stem cells, to obtain the required efficacy in wound healing, is a challenge. Embryonic stem cells possess a great capability of self-renewal, but there are some ethical issues regarding the use of these cells. Adult stem cells derived from the peripheral blood, umbilical cord, bone marrow or adipose tissue have limited capacity of self-renewal but their therapeutic application in human skin tissues are more acceptable [
10]. In addition, endogenous stem cell populations can have a role in several steps of wound healing, such as neovascularization and tissue remodeling.
Concerning embryonic stem cells, they are pluripotent and can differentiate into three primary germ layers (endoderm, mesoderm, ectoderm), as well as into keratinocytes (when some specific growth factors are present). Keratinocytes are fundamental since they are able to produce multilayered epidermis in culture. However, the ethical controversial (cells have to be harvested from live embryos) and the potential immune rejections redirect regenerative medicine into other types of cell [
10,
69].
An alternative, is the use of induced pluripotent stem cells (iPSCs). These cells are engineered from adult somatic cells (keratinocytes and fibroblasts) applying transcription factors such as KLF4, Sox-2 and c-Myc. Several studies refer to significant development in the differentiation of the mouse. Ref. Yoriko et al., demonstrated that rodent dermal papilla cells when removed from the hair follicles and transplanted intact into the recipient skin induce the development of the hair follicle and consequent hair growth [
70]. These cells are a good choice in chronic wound treatment and in unresolved wounds because of their multipotent capacity and limited immunoreactivity [
10]. iPSCs’ ability to differentiate into different cell types and the unlimited growth was demonstrated in some in vivo models. Ref. Ryoji et al., developed an in vivo transplantation model named as a clustering-dependent embryoid body transplantation method, which was used in nude mice and could be adequately connected to the nerve fibers, epidermis and arrector pili muscles without tumorigenesis [
71]. In addition, Ref. Karl et al., also used these cells to generate a human 3D skin from iPSCs-derived fibroblasts, iPSCs-derived keratinocytes and iPSCs-derived melanocytes [
72].
MSCs are used in various chronic and acute injuries. For instance, Ref. Evangelos et al., followed green fluorescent protein (GFP)-labeled bone marrow transplanted into non-GFP mice to understand how these cells react in cutaneous wounds and found evidence of improvement of the wounds. This study found GFP positive stem cells in the sebaceous gland, hair follicles and epidermis twenty one days after the transplantation of GFP bone marrow cells [
10,
73].
In addition, the process of wound healing is considered different among species, although some phases like inflammation, cell proliferation, blood clotting and extracellular matrix remodeling remain equal. For example, some lower vertebrates like fish (zebrafish) and amphibians (axolotl) have the capacity to regenerate skin perfectly. On the other hand, for adult mammals like humans it is more difficult to achieve this total regeneration, consequently the formation of a scar prevents the complete recovery of the skin function. Sheep and rats are animal models commonly used to provide important information about the regeneration of missing structures [
3,
21]. However, as previously mentioned, there are various in vivo studies verifying the use of stem cells as a therapeutic option for wound healing. Regarding anatomical similarities the porcine model is the most identical wound-healing model, having similar healing mechanisms to humans [
3].
Concerning our research group, the rat animal model is frequently used for skin lesion situations. The first approach to a new treatment entails a thorough biocompatibility assessment (hydrogel, bioscaffolds or others) by their subcutaneous implantation in the animal by a cutaneous incision, and recovery for 3, 7, 15 and 30 days. A histopathological analysis is performed following International Organization for Standartization (ISO) 10993-6:2016 (Biological evaluation of medical devices—Part 6: Tests for local effects after implantation). The treatments selected according to previous scoring are applied to the rat skin lesion model.
The ovine model is also a great choice because of its phylogenetic proximity to humans regarding mechanical characteristics and musculoskeletal size [
74]. For that reason, our group uses the ovine, as a more complex animal model, as a scale-up perspective to human medicine. Critical skin defects are applied to the sheep’s dorso and previously best-performing treatments are applied to the sheep on a daily basis. Furthermore, a thorough histopathological analysis of the lesion site and surrounding tissues is performed.
12. Future Cell Applications and Biomaterials
In the future, MSCs will continue to be a subject of interest and relevance in the medical field, as they had for the past decades [
3]. The main focus will be the jump between the most commonly used animal models and the clinical application of these therapies in human clinical cases, taking into account all the limitations explained above. The secretome role in wound healing will also continue to be studied [
3].
Furthermore, the construction of bioengineered regenerative 3D models and its use in wound healing, will allow stem cells within a 3D matrix to be applied locally [
3]. Therefore, our group has been involved in the development of equipment that is capable of identifying damaged tissues (such as skin wounds) and releases the bioscaffold with stem cells directly in the lesion site with software that is able to identify and delimit the lesion area and the materials needed. The 3D scaffolds will continue to be refined and tested with different materials to determine which are the best options to create the ultimate combination [
67]. Hopefully, in the near future, it will be possible to treat lesions in a quick and easy way with a device that can be used in hospitals to treat several different damaged tissues and organs (skin, soft tissue and others).
13. Conclusions
As discussed in this review, stem cells are the future of regenerative medicine, being a subject of interest worldwide. Modern medicine has increasingly shown interest in alternative treatment methods such as stem cells, which gives them the opportunity to show their potential and relevance in chronic and debilitating diseases, especially in those where current treatment is not effective [
8].
Supplementary research is needed to characterize MSCs and to provide more information about their effect in the wound-healing process. Moreover, further analysis of clinical and experimental applications of these cells is required with the purpose of determining the optimal source of stem cells and the most useful delivery technique [
10].
In the past few years, substantial information on skin reparation mechanisms has been gathered and high-end therapeutic strategies developed, thus promoting a significant upgrade of scientific knowledge [
23]. Furthermore, skin lesions and chronic skin diseases have a major impact on modern society, being a significant burden to both clinical institutions and patients, thus increasing the potential of stem cells [
20]. Future efforts need to focus on the wound-healing complexity and other pathologies associated. Delivery techniques have been developed to introduce stem cells in skin wounds using tissue engineering and biomaterials. The interaction between biomaterials, stem cells and the wound bed still require further comprehension to achieve more efficient treatments. For this purpose, clinical trials are fundamental since they provide information on in vivo systems, representing individual, wound type and dimension diversity [
23].


 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}