1. Introduction
Physiologically the human’s oral microflora consists of a mixture of organisms, which are common also to other anatomical districts. This bacterial charge is extremely complex, being composed of over 700 different species of bacteria [
1,
2,
3,
4,
5]. Humans are not randomly colonized and the diverse community that makes up the oral microbiome is finely tuned by nature to protect against diseases, and it is of great importance to maintain its natural diversity. This particular composition depends on numerous factors, some non-modifiable such as genetics, age, sex, change of dentition [
6], and some modifiable, including stress, nutrition, dental treatment, and diet [
7,
8,
9,
10]. The placement of removable orthodontic appliances creates a favorable environment for the accumulation of microbiota components and food residues, which, in time, may cause caries or exacerbate any pre-existing periodontal disease [
11,
12,
13,
14]. The appliances, both fixed and removable ones [
15,
16], may interfere with oral hygiene practice and cover considerable parts of the tooth surfaces, so an increase of the total microbial population as well as an altered microflora have been reported in relation to orthodontic treatment [
17].
Once dysbiosis occurs, the goal of treatment should be to restore the lost harmonic balance by maintaining good oral hygiene and modifying lifestyle factors such as diet and smoking. The indiscriminate use of antibiotics for the treatment of oral diseases should be avoided to safeguard the beneficial oral microbiota and avoid resistance to antibiotics. Prevention of caries should rely on the use of topical fluoride, and on measures to promote the elimination of the acidic environment, through reduced use of sucrose and acidic drinks (including the sugar-free ones), integration with agents that can reduce the production of acid and/or promote the generation of alkali in dental plaque. For periodontal diseases, therapeutic strategies should aim to mechanically reduce accumulated biofilm by mechanically removing plaque to levels compatible with oral health. This would reduce the inflammation and flow of Gingival Crevicular Fluid (GCF) and promote a favorable microenvironment to support the formation of a balanced microbiome. The role of the oral microbiome is important to prevent oral diseases.
Patients need to be aware of the implications for their oral health when undergoing recommended orthodontic treatment. On the other hand, when a patient accepts to undergo orthodontic treatment, including those using removable orthodontic devices, he should be reminded that it entails a commitment to a higher regimen of attention towards oral hygiene and health in patient’s home care [
18,
19].
The purpose of this review is to investigate the available evidence regarding the association between removable orthodontic appliances and both qualitative and quantitative changes of oral microbiota. Thus, the clinical research questions proposed are:
Do removable orthodontic appliances influence the quality and quantity of oral microbiota? Which are the effects of removable orthodontic appliances on the different bacterial species in the oral cavity?
2. Materials and Methods
2.1. Protocol
The present study was conducted by the Department of Dentistry at Vita-Salute San Raffaele University of Milan in association with the Unit of Hematology and Bone Marrow Transplantation at San Raffaele Hospital, Milan, Italy. This systematic review was performed in accordance with the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [
20,
21]. The analysis’ methods and inclusion criteria were specified in advance. No funding was given for the realization of the present review. This systematic review followed the PROSPERO protocol and it is registered on its database with the following registration number: CRD42019121762.
2.2. Search Strategy
The following electronic databases were searched from their respective sources: PubMed, Cochrane Library, Embase, Web of Science, Scopus, Ovid Medline and Dentistry & Oral Sciences Source; Gray literature was investigated on OpenGray (
www.opengrey.eu, accessed on 20 March 2021) and a manual research was conducted on the library of Vita Salute San Raffaele. To create an appropriate research question and review of the literature the PICOS strategy was used: orthodontic patients (patients—P), removable appliances (intervention—I), without orthodontic appliances (comparison—C); oral microbiota (outcome—O) [
22,
23].
The key words and combinations used in searching the databases were “(Functional appliance OR removable orthodontic appliance OR Frankel appliance OR Bionator OR LM activator OR Twin Block) AND oral microbiology”.
Articles published up to January 2020 were included without language and initial date restriction.
2.3. Eligibility Criteria
Initially, all articles were selected by title and abstract. Articles present in different databases were considered only once. In a second moment inclusion and exclusion criteria were applied.
The inclusion criteria were: The microbial analysis had to focus on the quality and quantity of changes in the mouth and not on the appliance and the statistical analysis of the studies had to be adequate [
24,
25]. All the articles included should have a statistical analysis of the results, at least two time points for analysis (with at least one before the beginning of treatment), and at least 10 patients analyzed. Only the studies which analyzed functional removable orthodontic appliances were included, in this way space maintainers, aligners or removable retainers were not considered [
26,
27,
28,
29,
30,
31,
32,
33].
The exclusion criteria were:
Patients with systemic diseases or under any condition that could influence oral microbiota or periodontal support tissues. Antibiotic therapy within three months before or during the study. No standardization and training in oral hygiene. Studies that did not specify the time of collection of samples [
34,
35,
36]. Case reports, case series, reviews, and author opinions.
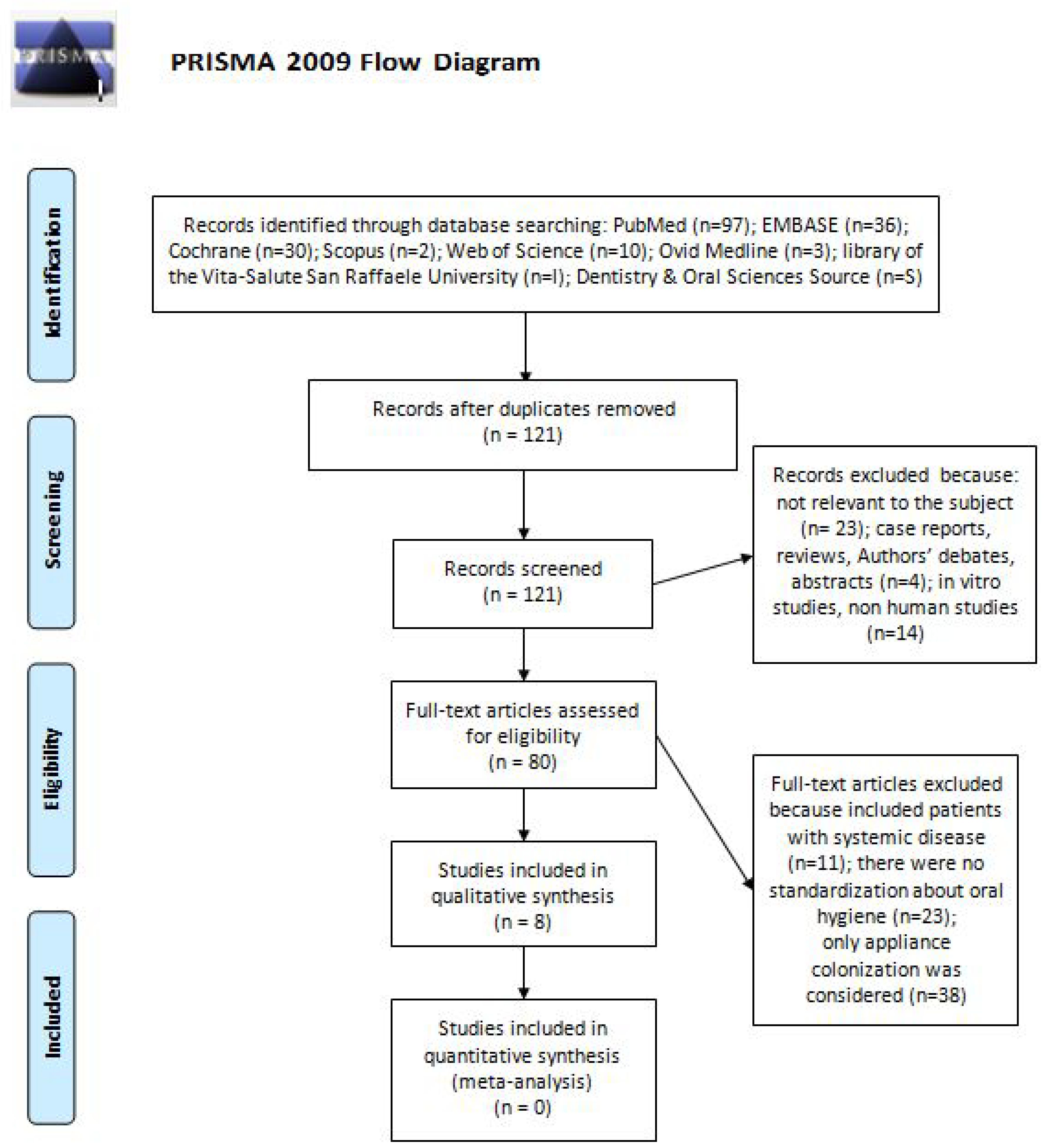
2.4. Sudy Selection
To minimize bias, two review authors, with experience in Oral Microbiology (LA) and Functional Orthodontics (MM), analyzed each selected paper and extracted data independently. If data were not clear enough, an attempt was made to contact the author by email. Any disagreement between the two reviewers was resolved by discussion or consultation with a third experienced author (MMa).
The selection of articles was processed according with the PRISMA guidelines (
Figure 1 ).
2.5. Data Selection
The following data was then collected from each included study: author/year publication, study design, sample size, sample/age/sex, type of appliance, collection time, collection method of analysis, microbial analysis outcome, and quality of the study (
Table 1) [
11,
37,
38,
39,
40,
41,
42,
43].
2.6. Risk of Bias and Quality Analysis
The methodological quality is “the extent to which the design and conduct of a study are likely to have prevented systematic errors (bias).” Different quality criteria can explain variation in the results of studies included in a systematic review. More rigorously designed (better “quality”) trials are more likely to reach results that are closer to the “truth”. The Swedish Council on Technology Assessment in Health Care Criteria for Grading Assessed Studies (SBU) method was adopted to report the level of evidence of this systematic review [
44]. To minimize the risk of bias during the inclusion of studies in the analysis, the two reviewers (LA and MM) applied independently the SBU criteria. When there was any disagreement concerning the relevance of an article, it was solved by the intervention of a third reviewer (MMa). This Protocol organized the articles in three grades according to their methodological quality, as
Table 2 shows.
Based on the grade of quality, four evidence levels were used (
Table 3).
The table shows the criteria used to define the level of evidence of the selected papers.
3. Results
From the initial 184 articles, 8 were selected as showed in the PRISMA flow diagram (
Figure 1) [
11,
37,
38,
39,
40,
41,
42,
43].
3.1. Quality of Evidence
Five of the eight chosen articles presented a moderate methodological quality [
11,
37,
39,
40,
42]: the major concern regarding these studies is the lack of blinded outcome assessment, diagnostic reliability tests, and reproducibility tests. One article had a high quality [
36] and the remaining two were classified as having a low quality [
41,
43]. Due to the absence of homogeneity in the study formulation, a meta-analysis could not be performed and a systematic review was realized.
When organizing the data according to pathogens, the following results were obtained.
3.2. Candida
All studies detected an increase of
Candida spp. concentration during therapy with removable orthodontic therapy [
11,
38,
39,
40,
41]. According to Jabur et al. study, removable orthodontic appliances induced an increase of
Candida level up to 13.3% after an average of five weeks and 20% after four months [
11].
On the contrary, the increase in
Candida was very low after three weeks [
38] and six months [
39].
In Addy’s study, the Candida prevalence after three weeks from the beginning of treatment resulted to be 46% in the control group and 52% of removable appliance wearers [
38].
Arendorf et al.’s study, noted a prevalence of
Candida of 57.6% for all study subjects, but the 39.4% of the sample was a prior
Candida-carrier, so only 18.2% became carriers five months after starting the therapy. Results of McNemar’s test showed a highly significant overall increase in
Candida prevalence while patients were wearing the appliances (
p < 0.001), especially in posterior and anterior palatal sites, respectively. However, the observed alteration was transient, since removal of the appliance was associated with a highly significant loss of carrier numbers (
p < 0.001), in fact, five months after the end of the therapy, only 42.4% of subjects reported
Candida colonies. This observation indicates that removable orthodontic appliances induces a persistent increase of
Candida colonies of only of 3% [
40].
Increasing numbers of microbiological counts of
Candida albicans were observed from baseline to one, three, and four months after therapy started, with a significant peak at the end of the first month (
p < 0.001) [
41].
According with Khanpayeh et al. study,
Candida colonies isolated from saliva six months after the beginning of the therapy with removable appliance belonged most frequently to
Candida spp. (25%) (
p = 0.001). Colony distribution included:
Candida albicans 25%,
Candida tropicalis 3%,
Candida parapsilosis 2%,
Candida krusei 1%, and
Candida kefyr 0%. Though, salivary carrier of
Candida species decreased with increasing duration of orthodontic treatment [
39].
3.3. Streptococcus mutans
All three articles [
37,
41,
43] which analyzed
S. mutans colonization of the mouth agreed that removable orthodontic appliance represents a promoting factor for the colonization of the oral cavity by this microorganism.
In Kundu et al.’s article a statistically significant increase of
S. mutans was recorded during orthodontic therapy with removable appliances, from the baseline to six months (
p < 0.001). Furthermore,
S. mutans bacterial counts were significantly higher than those of
Lactobacillus spp. and
Candida albicans at all timepoints (1–3–6 months) [
41].
The study that analyzed different interceptive removable appliances [
43], demonstrated a constant increase of
Lactobacillus and an increase of
S. mutans after 15 days, followed by a progressive decrease after 30 and 60 days.
The numbers of
S. mutans colonies showed a continuous increase during therapy from baseline to one month with statistical significance (
p < 0.05) [
37].
3.4. Lactobacillus
All the studies [
11,
41,
43] which quantitatively and qualitatively evaluated the difference of frequency in
Lactobacillus spp. demonstrated an increase in the microbiological counts.
Both Kundu et al. and Topaloglu et al. studies suggested that the microscopic counts of
Lactobacillus spp. increased significantly during orthodontic treatment with removable appliances from baseline to follow-up visits at 1, 3, and 6 months (
p < 0.05) [
41,
43].
Jabur et al. noted an increase (6.66%) in
Lactobacillus spp. after four months of therapy, too [
11].
3.5. Moraxella catharralis
According to Jabur et al., this pathogen was found in all patients analyzed, furthermore, its oral colonization incredibly increased with removable orthodontic appliances. After a mean of five weeks from the appliance use,
Moraxella prevalence was of 73.33% and after five months it reached 100% [
11].
3.6. Staphylococcus epidermidis
S. epidermidis colonization of the mouth also appears to be influenced by the use of removable appliances. As Jabur et al. stated, in patients using these devices the percentage increased up to 40% after an average of five weeks and peaked at 60% after four months [
11].
3.7. Others
The following results revealed that the changes in oral microbiota during treatment with removable orthodontic devices, involved also other bacterial species.
Petti et al. revealed that in supragingival and in subgingival plaque G+ cocci decreased after 6–8 weeks and increased at 6–7 months, with final values higher than baseline values. Gingivitis risk indices (bacterial count and G-rods) significantly increased progressively in 6–8 weeks. Among periodontitis risk indices, only supragingival rods and subgingival Spirochetes significantly increased at 6–7 months.
Aggregatibacter actinomycetemcomitans (Aa) was nearly absent [
40]. Anaerobic bacteria were detected in the subgingival dental plaque with the same density (n = 15.75%) at baseline and at three months, while the prevalence appeared increased, though not reaching statistical significance, at nine months (17.85%). The most important bacteria that cause periodontal tissue loss—
Aggregatibacter actinomycetemcomitans (Aa),
Porphyromonas gingivalis (Pg),
Tannerella forsythia (Tf), and
Prevotella nigrescens—were not detected in any patients [
42].
3.8. Outcomes Summary
Removable orthodontic appliances have the following effects on oral microflora:
Candida colonies increase, especially C. albicans species, during the first month of therapy, followed by a decrease after a few months.
S. mutans is the main microorganism to increase during the first months of therapy and the main increment occurs in the first 15 days.
Lactobacillus spp. microbiological count increases during the first months of therapy.
Moraxella catharralis and S. epidermidis values increase significantly during the first month of therapy.
Spirochaetes spp. significantly increases during the first 6–7 months of treatment.
Aa, Pg, Tf, and Prevotella nigrescens were not detected during therapy.
4. Discussion
The present systematic review is based on a low number of selected articles (n = 8) because of the reduced number of papers focused on this topic. Since we favored a strict and accurate study-selection process, the lack of standardization between the studies, the disparities in the category of devices analyzed and the variability in wearing-time did not allow to carry out a meta-analysis.
Any appliance or device placed in the oral cavity creates new retentive surfaces, promoting plaque accumulation and alteration of oral microflora. Consequently, the pH values and the buffering capacity of saliva significantly reduces during the therapy. This condition can promote an accumulation of cariogenic bacteria in dental plaque and saliva [
37]. Statistically significant increases were recorded in the following bacteria:
Streptococcus mutans, [
37,
41,
43],
Lactobacillus spp. [
11,
41,
43],
Staphylococcus epidermidis [
11],
Moraxella catharralis [
11], and subgingival Spirochetes [
42]. It was interesting to notice that the initial microorganism increment was followed by a progressive decrease towards more physiological values [
39]. The same happened to pH values, which seem to return to physiological levels after 6 months from the end of therapy [
40].
It was also demonstrated that previous orthodontic therapies do not alter the response of the oral microbiota to removable orthodontic treatment. Indeed, patients who have already undergone orthodontic treatment [
29,
30] have the same alterations in microorganisms of those who never wore orthodontic appliances [
25].
These results emphasize that removable orthodontic appliances, when inserted in the oral cavity, begin to accumulate plaque. However, it is not possible to understand whether the accumulation of plaque may depend on the material from which the device is made, because most published studies do not specify it. The microorganisms load increment could be strictly related to the appliance surface roughness as well as the time spent in the oral cavity. Generally, removable orthodontic appliances are made of heat-setting plastic or acrylic resin, which are both microporous and rough materials. The introduction of smoother surface removable devices could be more resilient for microorganisms and more biocompatible.
Therefore, it is essential that both patients and healthcare professionals embrace the concept of a balanced oral microbiota and its importance to oral and systemic health. Treatment sessions should include prevention strategies that promote active maintenance of oral health, rather than disease management. Oral health professionals can achieve this educating patients to appropriate lifestyle choice and an effective biofilm-formation control. This approach would maintain the beneficial properties of resident microbiota and would reduce the risk of dental disease and fungal infections.
There is a lack of studies rigorously designed to examine changes in the oral microbiota associated with removable orthodontic therapy; furthermore, a lot of heterogeneity was observed in the identified studies; therefore, further research is needed on this topic [
45].
5. Conclusions
With the limitations related to the studies analyzed and the culture method used, according to our systematic review, removable orthodontic appliances influence some oral bacterial species qualitatively and quantitatively. Moreover, the main changes seem to occur during the first 15 days, independently from the type of appliance. Nevertheless, after the end of the treatment, the concentration of pathogenic microorganisms seems to be leaning towards more physiological values.
Though, these changes promoted by orthodontic removable appliances appear to be transient.
Author Contributions
Conceptualization, A.L. and M.M. (Maurizio Manuelli); methodology, E.G.; software, M.T.L.S. and A.B.; validation, C.B., M.T.L.S. and F.C.; formal analysis, A.L. and P.A.; investigation, A.L.; resources, M.M (Maurizio Manuelli); data curation, M.N. and F.C.; writing—original draft preparation, M.M. (Marta Marcolina) and E.T.; writing—review and editing, V.B. and J.P.; visualization, E.G.; supervision, C.B. and R.G.; project administration, M.M. (Maurizio Manuelli). All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of IRCCS San Raffaele Scientific Institute, Milan, Italy (107/1NT/2017).
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bordenstein, S.R.; Theis, K.R. Host Biology in Light of the Microbiome: Ten Principles of Holobionts and Hologenomes. PLoS Biol. 2015, 13, e1002226. [Google Scholar] [CrossRef] [Green Version]
- Kilian, M.; Chapple, I.L.C.; Hannig, M.; Marsh, P.D.; Meuric, V.; Pedersen, A.M.L.; Tonetti, M.S.; Wade, W.G.; Zaura, E. The oral microbiome—An update for oral healthcare professionals. Br. Dent. J. 2016, 221, 657–666. [Google Scholar] [CrossRef]
- Sender, R.; Fuchs, S.; Milo, R. Are We Really Vastly Outnumbered? Revisiting the Ratio of Bacterial to Host Cells in Humans. Cell 2016, 164, 337–340. [Google Scholar] [CrossRef] [Green Version]
- Cho, I.; Blaser, M.J. The Human Microbiome: At the interface of health and disease. Nat. Rev. Genet. 2012, 13, 260–270. [Google Scholar] [CrossRef] [Green Version]
- Relman, D.A. The Human Microbiome and the Future Practice of Medicine. JAMA 2015, 314, 1127–1128. [Google Scholar] [CrossRef]
- Costalonga, M.; Herzberg, M.C. The oral microbiome and the immunobiology of periodontal disease and caries. Immunol. Lett. 2014, 162 Pt A, 22–38. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, B.; Peura, S.; Hammar, U.; Vicenzi, S.; Hedman, A.; Almqvist, C.; Andolf, E.; Pershagen, G.; Dicksved, J.; Bertilsson, S.; et al. Oral Microbiota Development in Early Childhood. Sci. Rep. 2019, 9, 19025. [Google Scholar] [CrossRef] [PubMed]
- Bowen, W.H.; Burne, R.A.; Wu, H.; Koo, H. Oral Biofilms: Pathogens, Matrix, and Polymicrobial Interactions in Microenvironments. Trends Microbiol. 2018, 26, 229–242. [Google Scholar] [CrossRef] [PubMed]
- García-Peña, C.; Álvarez-Cisneros, T.; Quiroz-Baez, R.; Friedland, R.P. Microbiota and Aging. A Review and Commentary. Arch. Med. Res. 2017, 48, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Hansen, T.H.; Kern, T.; Bak, E.G.; Kashani, A.; Allin, K.H.; Nielsen, T.; Hansen, T.; Pedersen, O. Impact of a vegan diet on the human salivary microbiota. Sci. Rep. 2018, 8, 5847. [Google Scholar] [CrossRef] [PubMed]
- Jabur, S.F. Influence of Removable Orthodontic Appliance on Oral Microbiological Status. J. Fac. Med. Baghdad 2008, 50, 4. [Google Scholar]
- Zachrisson, B.U. Oral hygiene for orthodontic patients: Current concepts and practical advice. Am. J. Orthod. 1974, 66, 487–497. [Google Scholar] [CrossRef]
- Gandini, P.; Schiavi, A.; Manuelli, M.; Camassa, D. Epidemiological survey of caries occurrence in school age children. Mondo Ortod. 1989, 14, 63–72. [Google Scholar] [PubMed]
- Lucchese, A.; Porcù, F.; Dolci, F. Effects of various stripping techniques on surface enamel. J. Clin. Orthod. 2001, 35, 691–695. [Google Scholar]
- Wang, Q.; Ma, J.B.; Wang, B.; Zhang, X.; Yin, Y.L.; Bai, H. Alterations of the oral microbiome in patients treated with the Invisalign system or with fixed appliances. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 633–640. [Google Scholar] [CrossRef]
- Lucchese, A.; Carinci, F.; Brunelli, G.; Monguzzi, R. Everstick® and Ribbond® fiber reinforced composites: Scanning Electron Microscope (SEM) comparative analysis. Eur. J. Inflam. 2011, 9, 73–79. [Google Scholar]
- Lucchese, A.; Bondemark, L.; Marcolina, M.; Manuelli, M. Changes in oral microbiota due to orthodontic appliances: A systematic review. J. Oral. Microbiol. 2018, 10, 1476645. [Google Scholar] [CrossRef] [Green Version]
- Manuelli, M. A peaceful man. Prog. Orthod. 2012, 13, 1. [Google Scholar] [CrossRef]
- Al Makhmari, S.A.; Kaklamanos, E.G.; Athanasiou, A.E. Short-term and long-term effectiveness of powered toothbrushes in promoting periodontal health during orthodontic treatment: A systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 753–766. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qual. Health Res. 2012, 22, 1435–1443. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Aydinbelge, M.; Cantekin, K.; Herdem, G.; Simsek, H.; Percin, D.; Parkan, O.M. Changes in periodontal and microbial parameters after the space maintainers application. Niger. J. Clin. Pract. 2017, 20, 1195–1200. [Google Scholar]
- D’Ercole, S.; Martinelli, D.; Tripodi, D. Influence of sport mouthguards on the ecological factors of the children oral cavity. BMC Oral Health 2014, 14, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucchese, A.; Carinci, F.; Brunelli, G. Skeletal effects induced by twin block in therapy of class ii malocclusion. Eur. J. Inflamm. 2012, 10, 83–87. [Google Scholar]
- Arikan, V.; Kizilci, E.; Ozalp, N.; Ozcelik, B. Effects of Fixed and Removable Space Maintainers on Plaque Accumulation, Periodontal Health, Candidal and Enterococcus Faecalis Carriage. Med. Princ. Pract. 2015, 24, 311–317. [Google Scholar] [CrossRef]
- Levrini, L.; Mangano, A.; Montanari, P.; Margherini, S.; Caprioglio, A.; Abbate, G.M. Periodontal health status in patients treated with the Invisalign(®) system and fixed orthodontic appliances: A 3 months clinical and microbiological evaluation. Eur. J. Dent. 2015, 9, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Farhadian, N.; Usefi Mashoof, R.; Khanizadeh, S.; Ghaderi, E.; Farhadian, M.; Miresmaeili, A. Streptococcus mutans counts in patients wearing removable retainers with silver nanoparticles vs those wearing conventional retainers: A randomized clinical trial. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 155–160. [Google Scholar] [CrossRef]
- Türköz, C.; Canigür Bavbek, N.; Kale Varlik, S.; Akça, G. Influence of thermoplastic retainers on Streptococcus mutans and Lactobacillus adhesion. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 598–603. [Google Scholar] [CrossRef] [PubMed]
- Walsh, L.J.; Healey, D.L. Prevention and caries risk management in teenage and orthodontic patients. Aust. Dent. J. 2019, 64 (Suppl. 1), S37–S45. [Google Scholar] [CrossRef]
- Guo, R.; Zheng, Y.; Liu, H.; Li, X.; Jia, L.; Li, W. Profiling of subgingival plaque biofilm microbiota in female adult patients with clear aligners: A three-month prospective study. Peer. J. 2018, 6, e4207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaklamanos, E.G.; Nassar, R.; Kalfas, S.; Al Halabi, M.; Kowash, M.; Hannawi, H.; Hussein, I.; Salami, A.; Hassan, A.; Senok, A.C. A single-centre investigator-blinded randomised parallel group clinical trial to investigate the effect of probiotic strains Streptococcus salivarius M18 and Lactobacillus acidophilus on gingival health of paediatric patients undergoing treatment with fixed orthodontic appliances: Study protocol. BMJ Open 2019, 9, e030638. [Google Scholar] [PubMed] [Green Version]
- Rego, R.O.; Oliveira, C.A.; dos Santos-Pinto, A.; Jordan, S.F.; Zambon, J.J.; Cirelli, J.A.; Haraszthy, V.I. Clinical and microbiological studies of children and adolescents receiving orthodontic treatment. Am. J. Dent. 2010, 23, 317–323. [Google Scholar] [PubMed]
- Gonçalves e Silva, C.R.; de Oliveira, L.D.; Leão, M.V.P.; Jorge, A.O.C. Candida spp. adherence to oral epithelial cells and levels of IgA in children with orthodontic appliances. Braz. Oral. Res. 2014, 28, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Kitada, K.; de Toledo, A.; Oho, T. Increase in detectable opportunistic bacteria in the oral cavity of orthodontic patients. Int. J. Dent. Hyg. 2009, 7, 121–125. [Google Scholar] [CrossRef]
- Batoni, G.; Pardini, M.; Giannotti, A.; Ota, F.; Giuca, M.R.; Gabriele, M.; Campa, M.; Senesi, S. Effect of removable orthodontic appliances on oral colonisation by mutans streptococci in children. Eur. J. Oral Sci. 2001, 109, 388–392. [Google Scholar] [CrossRef]
- Addy, M.; Shaw, W.C.; Hansford, P.; Hopkins, M. The effect of orthodontic appliances on the distribution of Candida and plaque in adolescents. Br. J. Orthod. 1982, 9, 158–163. [Google Scholar] [CrossRef]
- Khanpayeh, E.; Jafari, A.A.; Tabatabaei, Z. Comparison of salivary Candida profile in patients with fixed and removable orthodontic appliances therapy. Iran J. Microbiol. 2014, 6, 263–268. [Google Scholar]
- Arendorf, T.; Addy, M. Candidal carriage and plaque distribution before, during and after removable orthodontic appliance therapy. J. Clin. Periodontol. 1985, 12, 360–368. [Google Scholar] [CrossRef]
- Kundu, R.; Tripathi, A.M.; Jaiswal, J.N.; Ghoshal, U.; Palit, M.; Khanduja, S. Effect of fixed space maintainers and removable appliances on oral microflora in children: An in vivo study. J. Indian Soc. Pedod. Prev. Dent. 2016, 34, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Petti, S.; Barbato, E.; Simonetti D’Arca, A. Effect of orthodontic therapy with fixed and removable appliances on oral microbiota: A six-month longitudinal study. New Microbiol. 1997, 20, 55–62. [Google Scholar]
- Topaloglu-Ak, A.; Ertugrul, F.; Eden, E.; Ates, M.; Bulut, H. Effect of orthodontic appliances on oral microbiota—6 month follow-up. J. Clin. Pediatr. Dent. 2011, 35, 433–436. [Google Scholar] [CrossRef]
- Bondemark, L.; Holm, A.K.; Hansen, K.; Axelsson, S.; Mohlin, B.; Brattstrom, V.; Paulin, G.; Pietila, T. Long-term stability of orthodontic treatment and patient satisfaction. Angle Orthod. 2007, 77, 181–191. [Google Scholar] [CrossRef]
- Yan, D.; Liu, Y.; Che, X.; Mi, S.; Jiao, Y.; Guo, L.; Li, S. Changes in the Microbiome of the Inner Surface of Clear Aligners After Different Usage Periods. Curr. Microbiol. 2021, 78, 566–575. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).




{kind=link}