
The Use of Autogenous Teeth for Alveolar Ridge Preservation: A Literature Review

 ,
,  , ,
, ,  ,
, {kind=link}
Abstract
:1. Introduction
2. Alveolar Ridge Preservation in Extraction Sockets
2.1. Biological Effect of a Tooth Extraction
2.2. Alveolar Ridge Preservation: Concept and Bone Graft Materials Used
3. Autogenous Teeth as a Bone Graft Material
3.1. Biological Plausibility
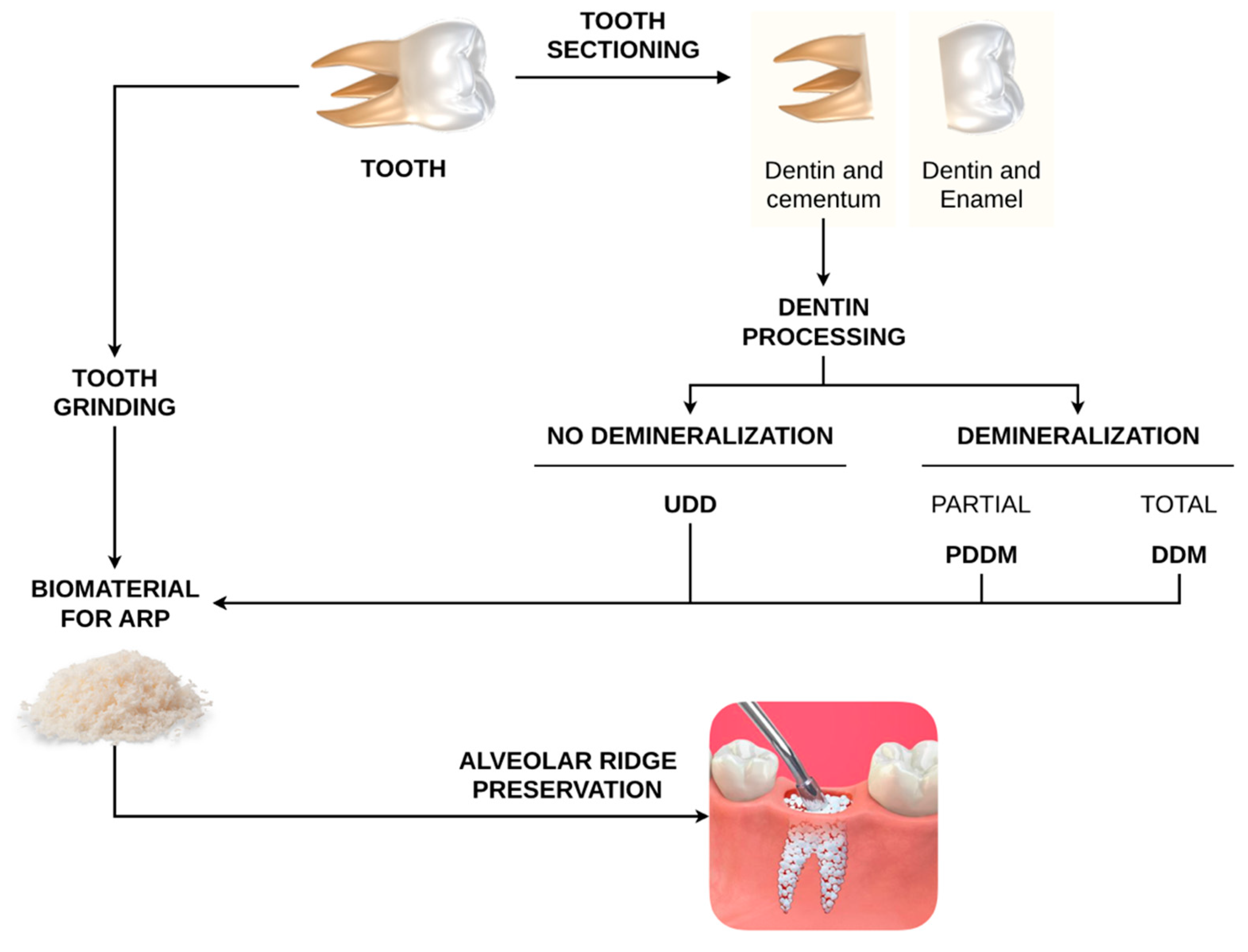
3.2. Dentin Processing
4. Demineralized Dentin Matrix (DDM)
4.1. Preclinical Studies
4.1.1. Histologic and Histomorphometric Outcomes
4.1.2. Immunohistochemistry Outcomes
4.2. Clinical Studies
4.2.1. Clinical Outcomes
4.2.2. Radiologic Outcomes
4.2.3. Histologic and Histomorphometric Outcomes
5. Partially Demineralized Dentin Matrix (PDDM)
5.1. Clinical Outcomes
5.2. Radiologic Outcomes
5.3. Histologic Outcomes
6. Undemineralized Dentin Matrix (UDD)
6.1. Preclinical Studies
Histologic and Histomorphometric Outcomes
6.2. Clinical Studies
6.2.1. Clinical Outcomes
6.2.2. Radiologic Outcomes
6.2.3. Histologic and Histomorphometry Outcomes
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Avila-Ortiz, G.; Elangovan, S.; Kramer, K.W.O.; Blanchette, D.; Dawson, D.V. Effect of alveolar ridge preservation after tooth extraction: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 950–958. [Google Scholar] [CrossRef]
- Ten Heggeler, J.M.A.G.; Slot, D.E.; Van Der Weijden, G.A. Effect of socket preservation therapies following tooth extraction in non-molar regions in humans: A systematic review. Clin. Oral Implants Res. 2011, 22, 779–788. [Google Scholar] [CrossRef]
- Avila-Ortiz, G.; Chambrone, L.; Vignoletti, F. Effect of alveolar ridge preservation interventions following tooth extraction: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46, 195–223. [Google Scholar] [CrossRef] [Green Version]
- Jambhekar, S.; Kernen, F.; Bidra, A.S. Clinical and histologic outcomes of socket grafting after flapless tooth extraction: A systematic review of randomized controlled clinical trials. J. Prosthet. Dent. 2015, 113, 371–382. [Google Scholar] [CrossRef]
- Tan, W.L.; Wong, T.L.T.; Wong, M.C.M.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implants Res. 2012, 23, 1–21. [Google Scholar] [CrossRef]
- Troiano, G.; Zhurakivska, K.; Lo Muzio, L.; Laino, L.; Cicciù, M.; Lo Russo, L. Combination of Bone Graft and Resorbable Membrane for Alveolar Ridge Preservation: A Systematic Review, Meta-analysis and Trial Sequential Analysis. J. Periodontol. 2017, 89, 46–57. [Google Scholar] [CrossRef]
- Van Der Weijden, F.; Dell’Acqua, F.; Slot, D.E. Alveolar bone dimensional changes of post-extraction sockets in humans: A systematic review. J. Clin. Periodontol. 2009, 36, 1048–1058. [Google Scholar] [CrossRef] [PubMed]
- Vignoletti, F.; Matesanz, P.; Rodrigo, D.; Figuero, E.; Martin, C.; Sanz, M. Surgical protocols for ridge preservation after tooth extraction: A systematic review. Clin. Oral Implants Res. 2012, 23, 22–38. [Google Scholar] [CrossRef] [PubMed]
- Ramanauskaite, A.; Sahin, D.; Sader, R.; Becker, J.; Schwarz, F. Efficacy of autogenous teeth for the reconstruction of alveolar ridge deficiencies: A systematic review. Clin. Oral Investig. 2019, 23, 4263–4287. [Google Scholar] [CrossRef] [PubMed]
- Bassir, S.; Alhareky, M.; Wangsrimongkol, B.; Jia, Y.; Karimbux, N. Systematic Review and Meta-Analysis of Hard Tissue Outcomes of Alveolar Ridge Preservation. Int. J. Oral Maxillofac. Implants 2018, 33, 979–994. [Google Scholar] [CrossRef] [PubMed]
- Stumbras, A.; Kuliesius, P.; Januzis, G.; Juodzbalys, G. Alveolar Ridge Preservation after Tooth Extraction Using Different Bone Graft Materials and Autologous Platelet Concentrates: A Systematic Review. J. Oral Maxillofac. Res. 2019, 10, 1–15. [Google Scholar] [CrossRef]
- Gual-Vaqués, P.; Polis-Yanes, C.; Estrugo-Devesa, A.; Ayuso-Montero, R.; Marí-Roig, A.; López-López, J. Autogenous teeth used for bone grafting: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2018, 23, e112–e119. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Johansson, C. Osteoinduction, osteoconduction and osseointegration. Eur. Spine J. 2001, 10, S96–S101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabatabaei, F.S.; Tatari, S.; Samadi, R.; Moharamzadeh, K. Different methods of dentin processing for application in bone tissue engineering: A systematic review. J. Biomed. Mat. Res. Part A 2016, 104, 2616–2627. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-K. Bone graft material using teeth. J. Korean Assoc. Oral Maxillofac. Surg. 2012, 38, 134–138. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.-K.; Lee, J.; Um, I.-W.; Kim, K.-W.; Murata, M.; Akazawa, T.; Mitsugi, M. Tooth-derived bone graft material. J. Korean Assoc. Oral Maxillofac. Surg. 2013, 39, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, D.; Zhou, L.; Lin, J.; Chen, J.; Huang, W.; Chen, Y. Immediate implant placement in anterior teeth with grafting material of autogenous tooth bone vs xenogenic bone. BMC Oral Health 2019, 19, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barone, A.; Borgia, V.; Covani, U.; Ricci, M.; Piattelli, A.; Lezzi, G. Flap versus flapless procedure for ridge preservation in alveolar extraction sockets: A histological evaluation in a randomized clinical trial. Clin. Oral Implants Res. 2015, 26, 806–813. [Google Scholar] [CrossRef]
- Barallat, L.; Ruíz-Magaz, V.; Levi, P.A.; Mareque-Bueno, S.; Galindo-Moreno, P.; Nart, J. Histomorphometric results in ridge preservation procedures comparing various graft materials in extraction sockets with nongrafted sockets in humans: A systematic review. Implant Dent. 2014, 23, 539–554. [Google Scholar] [CrossRef]
- De Risi, V.; Clementini, M.; Vittorini, G.; Mannocci, A.; De Sanctis, M. Alveolar ridge preservation techniques: A systematic review and meta-analysis of histological and histomorphometrical data. Clin. Oral Implants Res. 2015, 26, 50–68. [Google Scholar] [CrossRef]
- Vittorini Orgeas, G.; Clementini, M.; De Risi, V.; De Sanctis, M. Surgical Techniques for Alveolar Socket Preservation: A Systematic Review. Int. J. Oral Maxillofac. Implants 2013, 28, 1049–1061. [Google Scholar] [CrossRef] [Green Version]
- Horváth, A.; Mardas, N.; Mezzomo, L.A.; Needleman, I.G.; Donos, N. Alveolar ridge preservation. A systematic review. Clin. Oral Investig. 2013, 17, 341–363. [Google Scholar] [CrossRef]
- Chan, H.-L.; Lin, G.-H.; Fu, J.-H.; Wang, H.-L. Alterations in Bone Quality After Socket Preservation with Grafting Materials: A Systematic Review. Int. J. Oral Maxillofac. Implants 2013, 28, 710–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hürzeler, M.B.; Zuhr, O.; Schupbach, P.; Rebele, S.F.; Emmanouilidis, N.; Fickl, S. The socket-shield technique: A proof-of-principle report. J. Clin. Periodontol. 2010, 37, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Mourya, A.; Mishra, S.K.; Gaddale, R.; Chowdhary, R. Socket-shield technique for implant placement to stabilize the facial gingival and osseous architecture: A systematic review. J. Investig. Clin. Dent. 2019, 10, e12449. [Google Scholar] [CrossRef]
- Gharpure, A.S.; Bhatavadekar, N.B. Current evidence on the socket-shield technique: A systematic review. J. Oral Implantol. 2017, 43, 395–403. [Google Scholar] [CrossRef]
- Yeomans, J.D.; Urist, M.R. Bone Induction by Decalcified Dentine Implanted into Oral, Osseous and Muscle Tissues. Arch. Oral Biol. 1967, 12, 999–1008. [Google Scholar] [CrossRef]
- Bang, G.; Urist, M.R. Bone Induction in Excavation Chambers in Matrix of Decalcified Dentin. Arch. Surg 1967, 94, 781–789. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Lee, J.K.; Kim, K.-W.; Um, I.-W.; Murata, M. Healing Mechanism and Clinical Application of Autogenous Tooth Bone Graft Material; Pignatello, R., Ed.; IntechOpen: London, UK, 2013; Volume 395, ISBN 978-953-51-1051-4. [Google Scholar]
- Kim, Y.K.; Kim, S.G.; Oh, J.S.; Jin, S.C.; Son, J.S.; Kim, S.Y.; Lim, S.Y. Analysis of the inorganic component of autogenous tooth bone graft material. J. Nanosci. Nanotechnol. 2011, 11, 7442–7445. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Kim, S.G.; Bae, J.H.; Um, I.W.; Oh, J.S.; Jeong, K.I. Guided bone regeneration using autogenous tooth bone graft in implant therapy: Case series. Implant Dent. 2014, 23, 138–143. [Google Scholar] [CrossRef]
- Bessho, K.; Tanaka, N.; Matsumoto, J.; Tagawa, T.; Murata, M. Human Dentin-matrix-derived Bone Morphogenetic Protein. J. Dent. Res. 1991, 70, 171–175. [Google Scholar] [CrossRef]
- Boden, S.D.; Liu, Y.; Hair, G.A.; Helms, J.A.; Hu, D.; Racine, M.; Nanes, M.S.; Titus, L. LMP-1, A LIM-Domain Protein, Mediates BMP-6 Effects on Bone Formation. Endocrinology 1998, 139, 5125–5134. [Google Scholar] [CrossRef]
- Um, I.W. Demineralized Dentin Matrix (DDM) As a Carrier for Recombinant Human Bone Morphogenetic Proteins (rhBMP-2). In Advances in Experimental Medicine and Biology; Springer: Berlin, Germany, 2018; Volume 1077, pp. 487–499. ISBN 9789811309472. [Google Scholar]
- Um, I.-W.; Young-Kyun Kim, Y.-K.; Mitsugi, M. Demineralized dentin matrix scaffolds for alveolar bone engineering. J. Indian Prosthodont. Soc. 2017, 17, 120–127. [Google Scholar] [CrossRef]
- Minamizato, T.; Koga, T.; Takashi, I.; Nakatani, Y.; Umebayashi, M.; Sumita, Y.; Ikeda, T.; Asahina, I. Clinical application of autogenous partially demineralized dentin matrix prepared immediately after extraction for alveolar bone regeneration in implant dentistry: A pilot study. Int. J. Oral Maxillofac. Surg. 2017, 47, 125–132. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, Y.K.; Park, Y.H.; Park, J.C.; Ku, J.K.; Um, I.W.; Kim, J.Y. Evaluation of the healing potential of demineralized dentin matrix fixed with recombinant human bone morphogenetic protein-2 in bone grafts. Materials 2017, 10, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binderman, I.; Hallel, G.; Nardy, C.; Yaffe, A.; Sapoznikov, L. A Novel Procedure to Process Extracted Teeth for Immediate Grafting of Autogenous Dentin. JBR J. Interdiscip. Med. Dent. Sci. 2014, 2, 2–6. [Google Scholar] [CrossRef]
- Pang, K.-M.; Um, I.-W.; Kim, Y.-K.; Woo, J.-M.; Kim, S.-M.; Lee, J.-H. Autogenous demineralized dentin matrix from extracted tooth for the augmentation of alveolar bone defect: A prospective randomized clinical trial in comparison with anorganic bovine bone. Clin. Oral Implants Res. 2016, 28, 809–815. [Google Scholar] [CrossRef]
- Li, P.; Zhu, H.C.; Huang, D.H. Autogenous DDM versus Bio-Oss granules in GBR for immediate implantation in periodontal postextraction sites: A prospective clinical study. Clin. Implant Dent. Relat. Res. 2018, 20, 923–928. [Google Scholar] [CrossRef]
- Joshi, C.P.; Dani, N.H.; Khedkar, S.U. Alveolar ridge preservation using autogenous tooth graft versus beta-tricalcium phosphate alloplast: A randomized, controlled, prospective, clinical pilot study. J. Indian Soc. Periodontol. 2016, 20, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.; Sun, Y.; MacIejewska, I.; Qin, D.; Peng, T.; McIntyre, B.; Wygant, J.; Butler, W.T.; Qin, C. Distribution of SIBLING proteins in the organic and inorganic phases of rat dentin and bone. Eur. J. Oral Sci. 2008, 116, 104–112. [Google Scholar] [CrossRef] [Green Version]
- Park, M.; Mah, Y.J.; Kim, D.H.; Kim, E.S.; Park, E.J. Demineralized deciduous tooth as a source of bone graft material: Its biological and physicochemical characteristics. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 307–314. [Google Scholar] [CrossRef]
- Minetti, E.; Giacometti, E.; Gambardella, U.; Contessi, M.; Ballini, A.; Marenzi, G.; Celko, M.; Mastrangelo, F. Alveolar socket preservation with different autologous graft materials: Preliminary results of a multicenter pilot study in human. Materials 2020, 13, 1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reis-Filho, C.R.; Silva, E.R.; Martins, A.B.; Pessoa, F.F.; Gomes, P.V.N.; De Araújo, M.S.C.; Miziara, M.N.; Alves, J.B. Demineralised human dentine matrix stimulates the expression of VEGF and accelerates the bone repair in tooth sockets of rats. Arch. Oral Biol. 2012, 57, 469–476. [Google Scholar] [CrossRef]
- De Oliveira, G.S.; Miziara, M.N.; Silva, E.R.D.; Ferreira, E.L.; Biulchi, A.P.F.; Alves, J.B. Enhanced bone formation during healing process of tooth sockets filled with demineralized human dentine matrix. Aust. Dent. J. 2013, 58, 326–332. [Google Scholar] [CrossRef]
- Gharpure, A.S.; Bhatavadekar, N.B. Clinical efficacy of tooth-bone graft: A systematic review and risk of bias analysis of randomized control trials and observational studies. Implant Dent. 2017, 26, 119–134. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.-H.; Lee, J.-H. Study of bone healing pattern in extraction socket after application of demineralized dentin matrix material. J. Korean Assoc. Oral Maxillofac. Surg. 2011, 37, 365–374. [Google Scholar] [CrossRef]
- Park, S.-M.; Um, I.-W.; Kim, Y.-K.; Kim, K.-W. Clinical application of auto-tooth bone graft material. J. Korean Assoc. Oral Maxillofac. Surg. 2012, 38, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.-S. Autogenous fresh demineralized tooth graft prepared at chairside for dental implant. Maxillofac. Plast. Reconstr. Surg. 2015, 37, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Nadershah, M.; Zahid, T.M. Use of Autogenous Dentin Graft in Mandibular Third Molar Extraction Sockets: A Split-Mouth Randomized Double-Blind Study. Int. J. Pharm. Res. Allied Sci. 2019, 8, 73–79. [Google Scholar]
- Calvo-Guirado, J.L.; Cegarra Del Pino, P.; Sapoznikov, L.; Delgado Ruiz, R.A.; Fernández-Domínguez, M.; Gehrke, S.A. A new procedure for processing extracted teeth for immediate grafting in post-extraction sockets. An experimental study in American Fox Hound dogs. Ann. Anat. 2018, 217, 14–23. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Maté-Sánchez De Val, J.E.; Ramos-Oltra, M.L.; Martínez, C.P.A.; Ramírez-Fernández, M.P.; Maiquez-Gosálvez, M.; Gehrke, S.A.; Fernández-Domínguez, M.; Romanos, G.E.; Delgado-Ruiz, R.A. The use of tooth particles as a biomaterial in post-extraction sockets. Experimental study in dogs. Dent. J. 2018, 6, 12. [Google Scholar] [CrossRef] [Green Version]
- Pohl, S.; Binderman, I.; Tomac, J. Maintenance of alveolar ridge dimensions utilizing an extracted tooth dentin particulate autograft and platelet-rich fibrin: A retrospective radiographic cone-beam computed tomography study. Materials 2020, 13, 1083. [Google Scholar] [CrossRef] [Green Version]
- Dwivedi, A.; Kour, M. A neoteric procedure for alveolar ridge preservation using autogenous fresh mineralized tooth graft prepared at chair side. J. Oral Biol. Craniofac. Res. 2020, 10, 535–541. [Google Scholar] [CrossRef]
- Del Canto-Díaz, A.; De Elío-Oliveros, J.; Del Canto-Díaz, M.; Alobera-Gracia, M.A.; Del Canto-Pingarrón, M.; Martínez-González, J.M. Use of autologous tooth-derived graft material in the post-extraction dental socket. Pilot study. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e53–e60. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C.; Camino, J.; Nally, M.; Quirynen, M.; Martínez, B.; Pinto, N. Combining autologous particulate dentin, L-PRF, and fibrinogen to create a matrix for predictable ridge preservation: A pilot clinical study. Clin. Oral Investig. 2019, 24, 1151–1160. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Pang, K.; Yun, P.; Leem, D.; Um, I. Long-term follow-up of autogenous tooth bone graft blocks with dental implants. Clin. Case Rep. 2016, 5, 108–118. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Labrador, L.; Martín-Ares, M.; Ortega-Aranegui, R.; López-Quiles, J.; Martínez-González, J.M. Autogenous dentin graft in bone defects after lower third molar extraction: A split-mouth clinical trial. Materials 2020, 13, 3090. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; System, B.; Kim, Y.; Um, I.; Murata, M. Clinical Report Tooth Bank System for Bone Regeneration-Safety Report. J. Hard Tissue Biol. 2014, 23, 371–376. [Google Scholar] [CrossRef] [Green Version]
- Minetti, E.; Berardini, M.; Trisi, P. A New Tooth Processing Apparatus Allowing to Obtain Dentin Grafts for Bone Augmentation: The Tooth Transformer. Open Dent. J. 2019, 13, 6–14. [Google Scholar] [CrossRef]
- Schwarz, F.; Hazar, D.; Becker, K.; Parvini, P.; Sader, R.; Becker, J. Short-term outcomes of staged lateral alveolar ridge augmentation using autogenous tooth roots. A prospective controlled clinical study. J. Clin. Periodontol. 2019, 46, 969–976. [Google Scholar] [CrossRef]
- Reddy, G.V.; Abhinav, A.; Malgikar, S.; Bhagyashree, C.; Babu, P.R.; Reddy, G.J.; Sagar, S.V. Clinical and Radiographic Evaluation of Autogenous Dentin Graft and Demineralized Freeze-Dried Bone Allograft with Chorion Membrane in the Treatment of Grade II and III Furcation Defects: A Randomized Controlled Trial. Indian J. Dent. Sci. 2019, 11, 10–13. [Google Scholar] [CrossRef]
- Jun, S.H.; Ahn, J.S.; Lee, J.I.; Ahn, K.J.; Yun, P.Y.; Kim, Y.K. A prospective study on the effectiveness of newly developed autogenous tooth bone graft material for sinus bone graft procedure. J. Adv. Prosthodont. 2014, 6, 528–538. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.-K.; Jun, S.-H.; Um, I.-W.; Kim, S. Evaluation of the Healing Process of Autogenous Tooth Bone Graft Material Nine Months after Sinus Bone Graft: Micromorphometric and Histological Evaluation. J. Korean Assoc. Maxillofac. Plast. Reconstr. Surg. 2013, 35, 310–315. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.K.; Kim, S.G.; Byeon, J.H.; Lee, H.J.; Um, I.U.; Lim, S.C.; Kim, S.Y. Development of a novel bone grafting material using autogenous teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, 496–503. [Google Scholar] [CrossRef]
- Gomes, M.F.; De Abreu, P.P.; Cantarelli Morosolli, A.R.; Araújo, M.M.; Vilela Goulart, M.D.G. Densitometric analysis of the autogenous demineralized dentin matrix on the dental socket wound healing process in humans. Braz. Oral Res. 2006, 20, 324–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadkhodazadeh, M.; Ghasemianpour, M.; Soltanian, N.; Sultanian, G.R.; Ahmadpour, S.; Amid, R. Effects of fresh mineralized dentin and cementum on socket healing: A preliminary study in dogs. J. Korean Assoc. Oral Maxillofac. Surg. 2015, 41, 119–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valdec, S.; Pasic, P.; Soltermann, A.; Thoma, D.; Stadlinger, B.; Rücker, M. Alveolar ridge preservation with autologous particulated dentin—A case series. Int. J. Implant Dent. 2017, 3, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cenicante, J.; Botelho, J.; Machado, V.; Mendes, J.J.; Mascarenhas, P.; Alcoforado, G.; Santos, A. The Use of Autogenous Teeth for Alveolar Ridge Preservation: A Literature Review. Appl. Sci. 2021, 11, 1853. https://doi.org/10.3390/app11041853
Cenicante J, Botelho J, Machado V, Mendes JJ, Mascarenhas P, Alcoforado G, Santos A. The Use of Autogenous Teeth for Alveolar Ridge Preservation: A Literature Review. Applied Sciences. 2021; 11(4):1853. https://doi.org/10.3390/app11041853
Chicago/Turabian StyleCenicante, João, João Botelho, Vanessa Machado, José João Mendes, Paulo Mascarenhas, Gil Alcoforado, and Alexandre Santos. 2021. "The Use of Autogenous Teeth for Alveolar Ridge Preservation: A Literature Review" Applied Sciences 11, no. 4: 1853. https://doi.org/10.3390/app11041853