
Factors Affecting the Outcome of Periapical Surgery; a Prospective Longitudinal Clinical Study

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
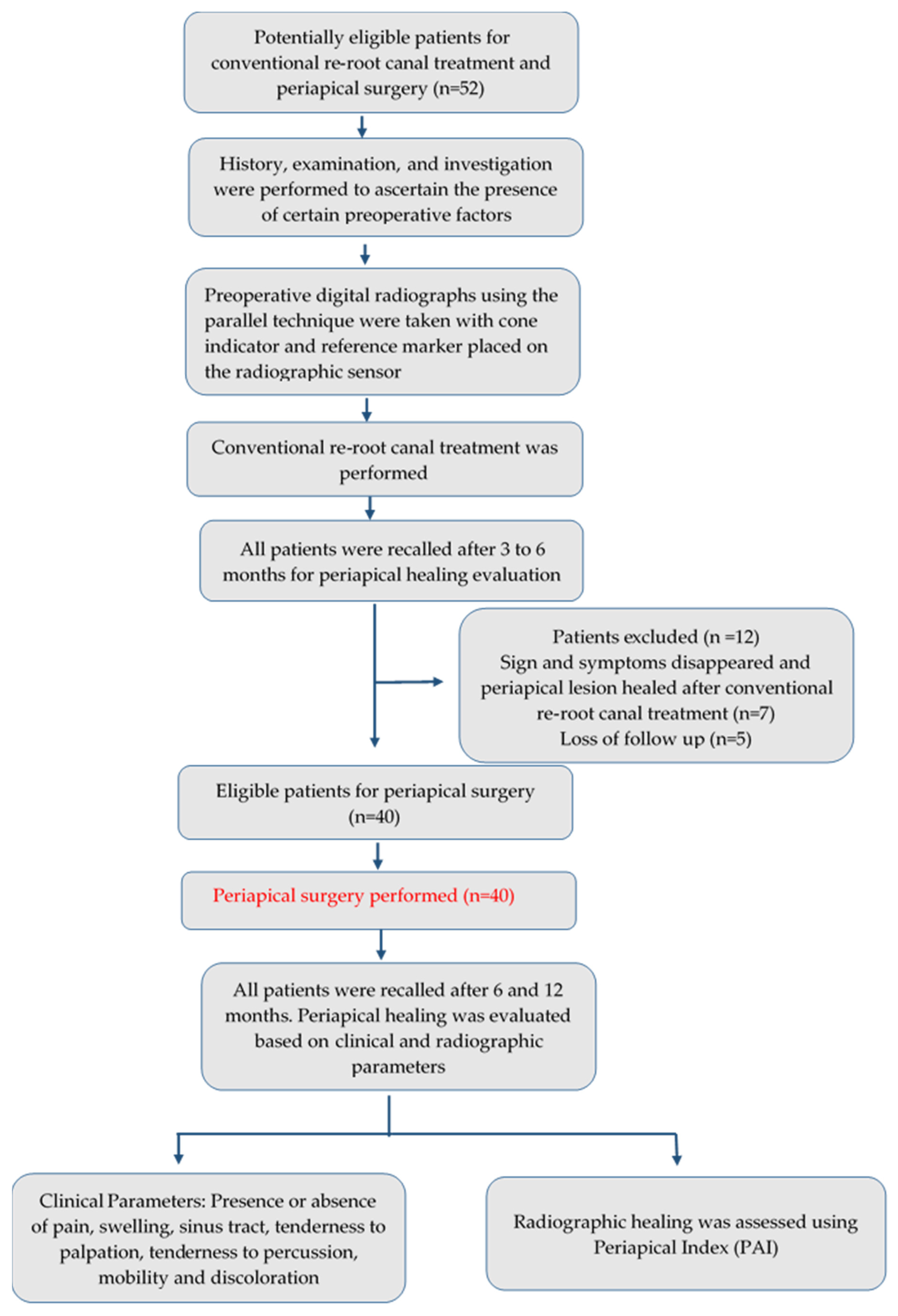
2. Materials and Methods
2.1. Study Setting and Ethical Approval
2.2. Inclusion and Exclusion Criteria
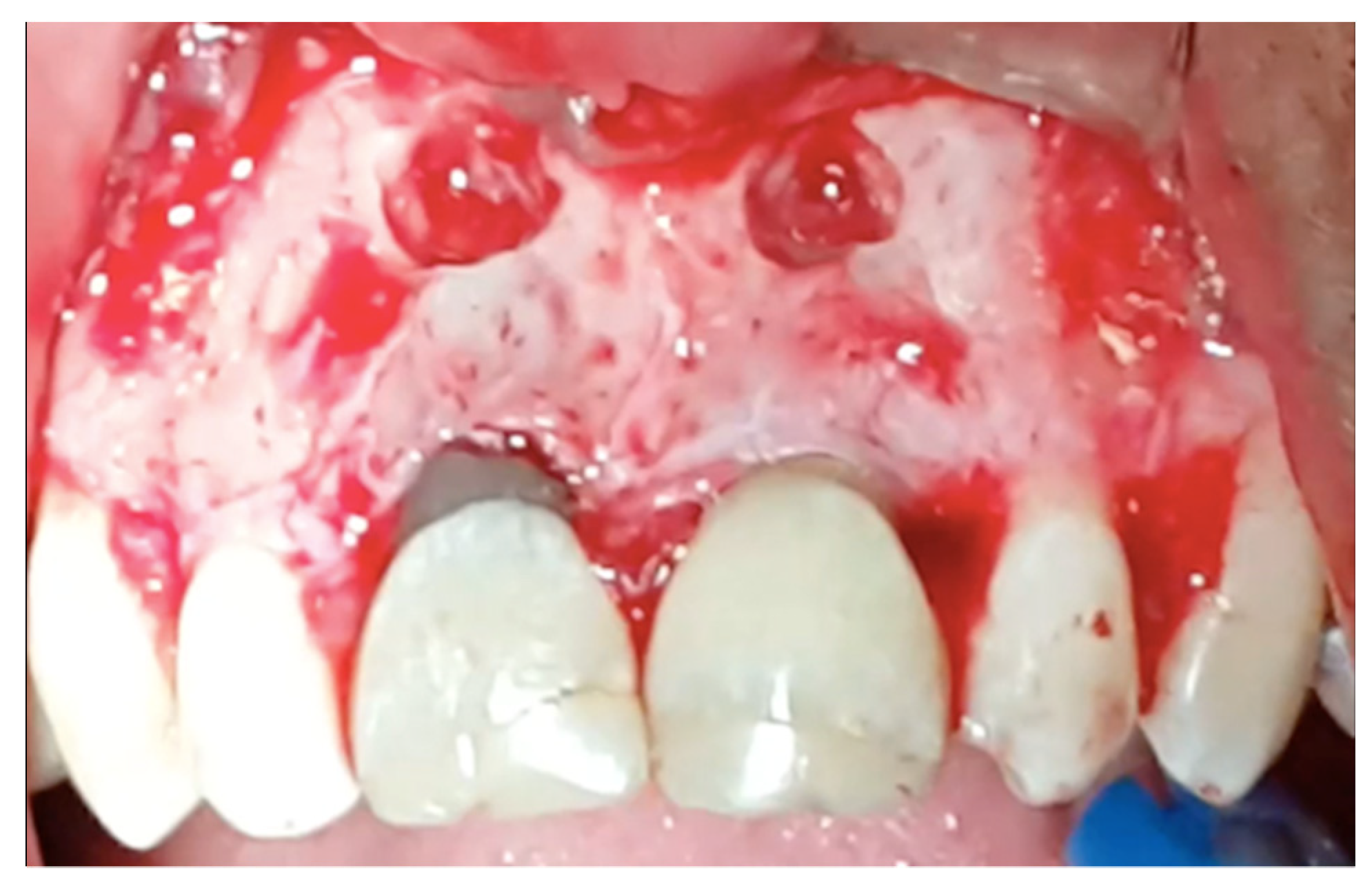
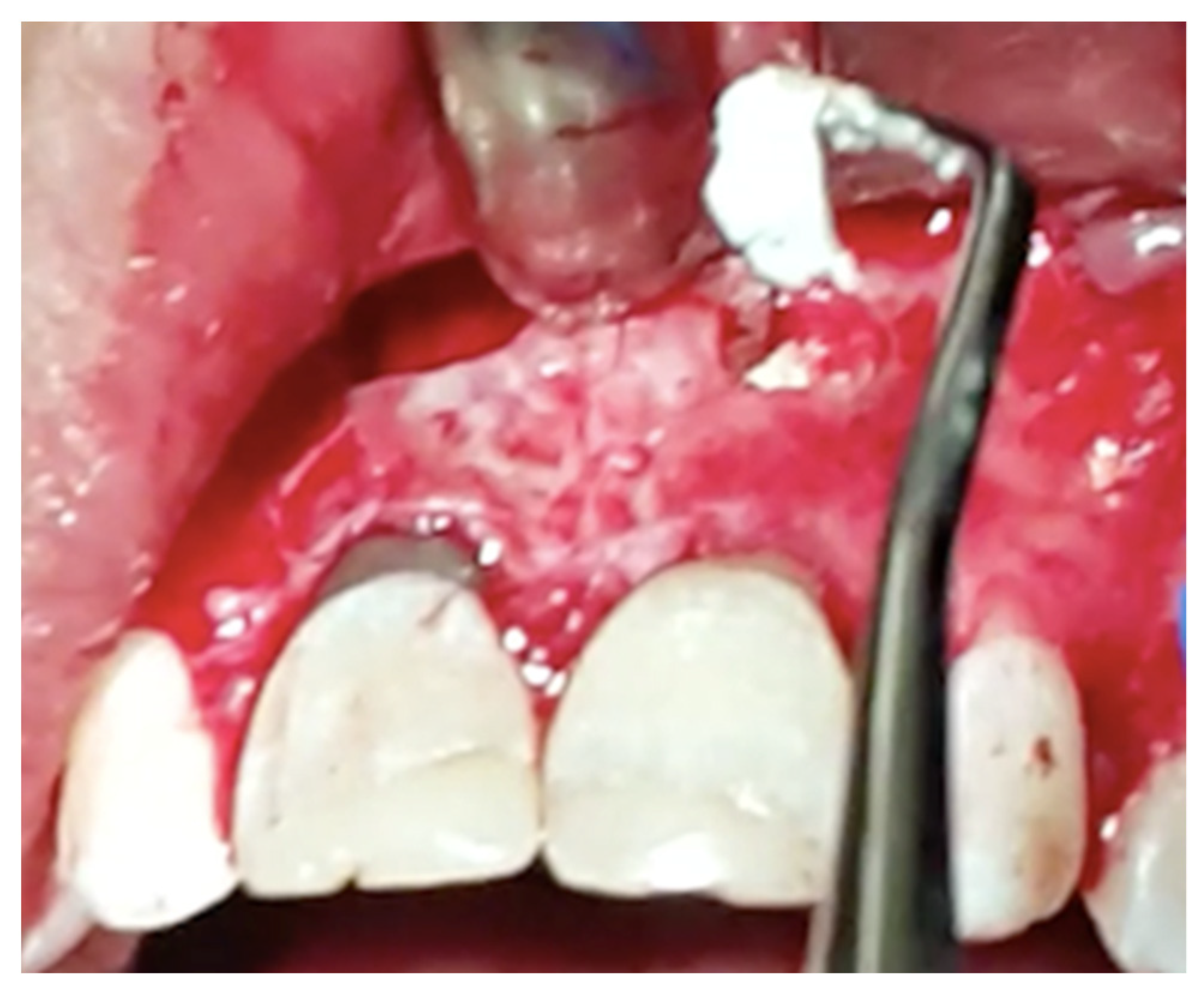
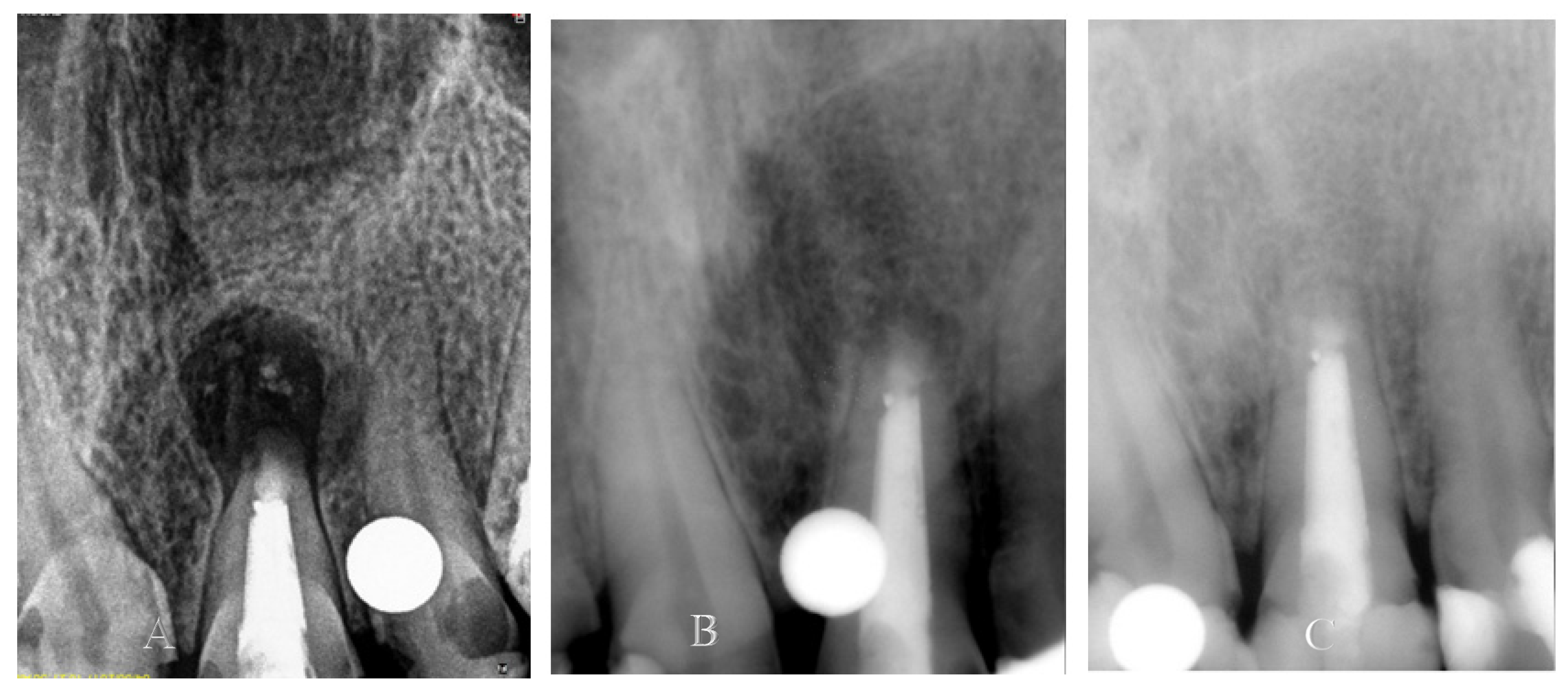
2.3. Clinical Procedure
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schilder, H.; Hargreaves, K.M. Filling root canals in three dimensions. J. Endod. 2006, 32, 281–290. [Google Scholar] [CrossRef]
- Alghamdi, F.; Alhaddad, A.J.; Abuzinadah, S. Healing of Periapical Lesions After Surgical Endodontic Retreatment: A Systematic Review. Cureus 2020, 12, e6916. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.A.; Anwar, M.F.; Ahmed, K.; Aftab, M.; Nazim, F.; Bari, M.F.; Mustafa, M.; Vohra, F.; Alrahlah, A.; Mughal, N.; et al. Baseline MMP expression in periapical granuloma and its relationship with periapical wound healing after surgical endodontic treatment. BMC Oral Health 2021, 21, 562. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Giménez, M.; Sánchez-Torres, A.; Gay-Escoda, C. Prognostic factors on periapical surgery: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e715–e722. [Google Scholar] [CrossRef]
- Segura-Egea, J.J.; Martín-González, J.; Castellanos-Cosano, L. Endodontic medicine: Connections between apical periodontitis and systemic diseases. Int. Endod. J. 2015, 48, 933–951. [Google Scholar] [CrossRef] [PubMed]
- Krall, E.A.; Sosa, C.A.; Garcia, C.; Nunn, M.E.; Caplan, D.J.; Garcia, R.I. Cigarette smoking increases the risk of root canal treatment. J. Dent. Res. 2006, 85, 313–317. [Google Scholar] [CrossRef]
- Peršić Bukmir, R.; Jurčević Grgić, M.; Brumini, G.; Spalj, S.; Pezelj-Ribaric, S.; Brekalo Pršo, I. Influence of tobacco smoking on dental periapical condition in a sample of Croatian adults. Wien. Klin. Wochenschr. 2016, 128, 260–265. [Google Scholar] [CrossRef]
- López-López, J.; Jané-Salas, E.; Martín-González, J.; Castellanos-Cosano, L.; Llamas-Carreras, J.M.; Velasco-Ortega, E.; Segura-Egea, J.J. Tobacco smoking and radiographic periapical status: A retrospective case-control study. J. Endod. 2012, 38, 584–588. [Google Scholar] [CrossRef]
- Ghattas Ayoub, C.; Aminoshariae, A.; Bakkar, M.; Ghosh, S.; Bonfield, T.; Demko, C.; Montagnese, T.A.; Mickel, A.K. Comparison of IL-1β, TNF-α, hBD-2, and hBD-3 Expression in the Dental Pulp of Smokers Versus Nonsmokers. J. Endod. 2017, 43, 2009–2013. [Google Scholar] [CrossRef]
- Melcher, A.H. On the Repair Potential of Periodontal Tissues. J. Periodontol. 1976, 47, 256–260. [Google Scholar] [CrossRef]
- Lin, L.; Chen, M.Y.H.; Ricucci, D.; Rosenberg, P.A. Guided Tissue Regeneration in Periapical Surgery. J. Endod. 2010, 36, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Von Arx, T.; Jensen, S.S.; Hänni, S.; Friedman, S. Five-year longitudinal assessment of the prognosis of apical microsurgery. J. Endod. 2012, 38, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Çalişkan, M.K.; Tekin, U.; Kaval, M.E.; Solmaz, M.C. The outcome of apical microsurgery using MTA as the root-end filling material: 2- to 6-year follow-up study. Int. Endod. J. 2016, 49, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Shinbori, N.; Grama, A.M.; Patel, Y.; Woodmansey, K.; He, J. Clinical Outcome of Endodontic Microsurgery That Uses EndoSequence BC Root Repair Material as the Root-end Filling Material. J. Endod. 2015, 41, 607–612. [Google Scholar] [CrossRef]
- Lui, J.N.; Khin, M.M.; Krishnaswamy, G.; Chen, N.N. Prognostic factors relating to the outcome of endodontic microsurgery. J. Endod. 2014, 40, 1071–1076. [Google Scholar] [CrossRef]
- Lustmann, J.; Friedman, S.; Shaharabany, V. Relation of pre- and intraoperative factors to prognosis of posterior apical surgery. J. Endod. 1991, 17, 239–241. [Google Scholar] [CrossRef]
- Allen, R.K.; Newton, C.W.; Brown, C.E. A statistical analysis of surgical and nonsurgical endodontic retreatment cases. J. Endod. 1989, 15, 261–266. [Google Scholar] [CrossRef]
- Rahbaran, S.; Gilthorpe, M.S.; Harrison, S.D.; Gulabivala, K. Comparison of clinical outcome of periapical surgery in endodontic and oral surgery units of a teaching dental hospital: A retrospective study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2001, 91, 700–709. [Google Scholar] [CrossRef]
- Kruse, C.; Spin-Neto, R.; Christiansen, R.; Wenzel, A.; Kirkevang, L.L. Periapical Bone Healing after Apicectomy with and without Retrograde Root Filling with Mineral Trioxide Aggregate: A 6-year Follow-up of a Randomized Controlled Trial. J. Endod. 2016, 42, 533–537. [Google Scholar] [CrossRef]
- Von Arx, T.; Peñarrocha, M.; Jensen, S. Prognostic factors in apical surgery with root-end filling: A meta-analysis. J. Endod. 2010, 36, 957–973. [Google Scholar] [CrossRef]
- Martins, C.M.; Sasaki, H.; Hirai, K.; Andrada, A.C.; Gomes-Filho, J.E. Relationship between hypertension and periapical lesion: An in vitro and in vivo study. Braz. Oral Res. 2016, 30, e78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreisler, M.; Gockel, R.; Aubell-Falkenberg, S.; Kreisler, T.; Weihe, C.; Filippi, A.; Kühl, S.; Schütz, S.; D’Hoedt, B. Clinical outcome in periradicular surgery: Effect of patient- and tooth-related factors—A multicenter study. Quintessence Int. 2013, 44, 53–60. [Google Scholar]
- Barone, C.; Dao, T.T.; Basrani, B.B.; Wang, N.; Friedman, S. Treatment Outcome in Endodontics: The Toronto Study-Phases 3, 4, and 5: Apical Surgery. J. Endod. 2010, 36, 28–35. [Google Scholar] [CrossRef]
- Zuolo, M.L.; Ferreira, M.O.F.; Gutmann, J.L. Prognosis in periradicular surgery: A clinical prospective study. Int. Endod. J. 2000, 33, 91–98. [Google Scholar] [CrossRef]
- Wesson, C.M.; Gale, T.M. Molar apicectomy with amalgam root-end filling: Results of a prospective study in two district general hospitals. Br. Dent. J. 2003, 195, 707–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peñarrocha-Diago, M.; Ortega-Sánchez, B.; García-Mira, B.; Maestre-Ferrín, L.; Peñarrocha-Oltra, D.; Gay-Escoda, C. A prospective clinical study of polycarboxylate cement in periapical surgery. Med. Oral Patol. Oral Cir. Bucal 2012, 17, 276–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, G.K.; Guthmiller, J.M. The impact of cigarette smoking on periodontal disease and treatment. Periodontol. 2000 2007, 44, 178–194. [Google Scholar] [CrossRef]
- Cabanillas-balsera, D.; Segura-Egea, J.J.; Bermudo-fuenmayor, M.; Martín-gonzález, J.; Jiménez-sánchez, M.C.; Areal-quecuty, V.; Sánchez-domínguez, B.; Montero-miralles, P.; Velasco-Ortega, E. Smoking and Radiolucent Periapical Lesions in Root Filled Teeth: Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 3506. [Google Scholar] [CrossRef]
- Bergström, J.; Babcan, J.; Eliasson, S. Tobacco smoking and dental periapical condition. Eur. J. Oral Sci. 2004, 112, 115–120. [Google Scholar]
- Krall, E.A.; Sosa, C.A.; Garcia, C.; Nunn, M.E.; Caplan, D.J.; Garcia, R.I. Cigarette smoking is associated with an acute impairment of microvascular function in humans. Clin. Sci. 2003, 104, 247–252. [Google Scholar]
- Kirkevang, L.L.; Wenzel, A. Risk indicators for apical periodontitis. Community Dent. Oral Epidemiol. 2003, 31, 59–67. [Google Scholar] [CrossRef]
- Rodriguez, F.R.; Taner, B.; Weiger, R.; Walter, C. Is smoking a predictor of apical periodontitis? Clin. Oral Investig. 2013, 17, 1947–1955. [Google Scholar] [CrossRef] [Green Version]
- Balto, H.A.; Alabdulaaly, L.; Bahammam, S.; Al-Ekrish, A.A. Comparative analysis of prevalence of apical periodontitis in smokers and non-smokers using cone-beam computed tomography. Saudi Dent. J. 2019, 31, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Jung, I.Y.; Lee, S.J.; Lee, C.Y.; Kim, E. Prognostic factors for clinical outcomes in endodontic microsurgery: A retrospective study. J. Endod. 2011, 37, 927–933. [Google Scholar] [CrossRef] [PubMed]
- Peñarrocha Diago, M.; Ortega Sánchez, B.; García Mira, B.; Martí Bowen, E.; Von Arx, T.; Gay Escoda, C. Evaluation of healing criteria for success after periapical surgery. Med. Oral Patol. Oral Cir. Bucal 2008, 13, 143–147. [Google Scholar]
- Segura-Egea, J.J.; Martín-González, J.; Cabanillas-Balsera, D.; Fouad, A.F.; Velasco-Ortega, E.; López-López, J. Association between diabetes and the prevalence of radiolucent periapical lesions in root-filled teeth: Systematic review and meta-analysis. Clin. Oral Investig. 2016, 20, 1133–1141. [Google Scholar] [CrossRef]
- Hsiao, A.; Glickman, G.; He, J. A retrospective clinical and radiographic study on healing of periradicular lesions in patients taking oral bisphosphonates. J. Endod. 2009, 35, 1525–1528. [Google Scholar] [CrossRef] [PubMed]
- Tortorici, S.; Difalco, P.; Caradonna, L.; Tetè, S. Traditional endodontic surgery versus modern technique: A 5-year controlled clinical trial. J. Craniofac. Surg. 2014, 25, 804–807. [Google Scholar] [CrossRef]
- Setzer, F.C.; Shah, S.B.; Kohli, M.R.; Karabucak, B.; Kim, S. Outcome of endodontic surgery: A meta-analysis of the literature—part 1: Comparison of traditional root-end surgery and endodontic microsurgery. J. Endod. 2010, 36, 1757–1765. [Google Scholar] [CrossRef]
- Abdinian, M.; Katiraei, M.; Zahedi, H.; Rengo, C.; Soltani, P.; Spagnuolo, G. Age Estimation Based on Pulp–Tooth Volume Ratio of Anterior Teeth in Cone-Beam Computed Tomographic Images in a Selected Population: A Cross-Sectional Study. Appl. Sci. 2021, 11, 9984. [Google Scholar] [CrossRef]
- Lowe, D.; Rogers, S. University of Washington Quality of Life Questionnaire (UW-QOL v4 and v4.1). Available online: http://www.headandneckcancer.co.uk/sites/default/files/assets/pages/UW-QOL-update-2018.pdf (accessed on 10 June 2021).
- Soltani, P.; Sami, S.; Yaghini, J.; Golkar, E.; Riccitiello, F.; Spagnuolo, G. Application of Fractal Analysis in Detecting Trabecular Bone Changes in Periapical Radiograph of Patients with Periodontitis. Int. J. Dent. 2021, 7, 3221448. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | N = 40 (%) |
|---|---|
| Age | |
| <30 years | 32 (80.0) |
| >30 years | 08 (20.0) |
| Gender | |
| Male | 28 (70.0) |
| Female | 12 (30.0) |
| Smoking | |
| Nonsmoker | 26 (65.0) |
| Smoker | 14 (35.0) |
| Preoperative pain | 22 (55.0) |
| Periapical lesion size | |
| ≤6 mm | 20 (50.0) |
| >6 mm | 20 (50.0) |
| Postoperative healing | 29 (72.5) |
| Characteristics | Periapical Healing | |||
|---|---|---|---|---|
| Yes (n = 29) | No (n = 11) | Total | p-Value | |
| Age in years | 0.025 ^ | |||
| <30 | 26 (81.3%) | 6 (18.8%) | 32 | |
| >30 | 3 (37.5%) | 5 (62.5%) | 8 | |
| Gender | ||||
| Male | 22 (78.6%) | 6 (21.4%) | 28 | 0.254 ^ |
| Female | 7 (58.3%) | 5 (41.7%) | 12 | |
| Smoking | ||||
| Nonsmoker | 22 (84.6%) | 4 (15.4%) | 26 | 0.029 ^ |
| Smoker | 7 (50.0%) | 7 (50.0%) | 14 | |
| Preoperative pain | ||||
| Yes | 15 (68.2%) | 7 (31.8%) | 22 | 0.723 ^ |
| No | 14 (77.8%) | 4 (22.2%) | 18 | |
| Periapical lesion size | ||||
| ≤6 mm | 20 (100%) | 0 (0.0%) | 20 | <0.001 ¥ |
| >6 mm | 09 (45.0%) | 11 (55.0%) | 20 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmed, M.A.; Mughal, N.; Abidi, S.H.; Bari, M.F.; Mustafa, M.; Vohra, F.; Alrahlah, A. Factors Affecting the Outcome of Periapical Surgery; a Prospective Longitudinal Clinical Study. Appl. Sci. 2021, 11, 11768. https://doi.org/10.3390/app112411768
Ahmed MA, Mughal N, Abidi SH, Bari MF, Mustafa M, Vohra F, Alrahlah A. Factors Affecting the Outcome of Periapical Surgery; a Prospective Longitudinal Clinical Study. Applied Sciences. 2021; 11(24):11768. https://doi.org/10.3390/app112411768
Chicago/Turabian StyleAhmed, Muhammad Adeel, Nouman Mughal, Syed Hani Abidi, Muhammad Furqan Bari, Mohammed Mustafa, Fahim Vohra, and Ali Alrahlah. 2021. "Factors Affecting the Outcome of Periapical Surgery; a Prospective Longitudinal Clinical Study" Applied Sciences 11, no. 24: 11768. https://doi.org/10.3390/app112411768