Self-Expandable Retainer for Endoscopic Visualization in the External Auditory Canal: Proof of Concept in Human Cadavers


 and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Self-Expandable Retainers
2.3. Tympanomeatal Flap Elevation and SER Placement
2.4. Study Definition and Data Analysis
2.5. Statistical Analysis
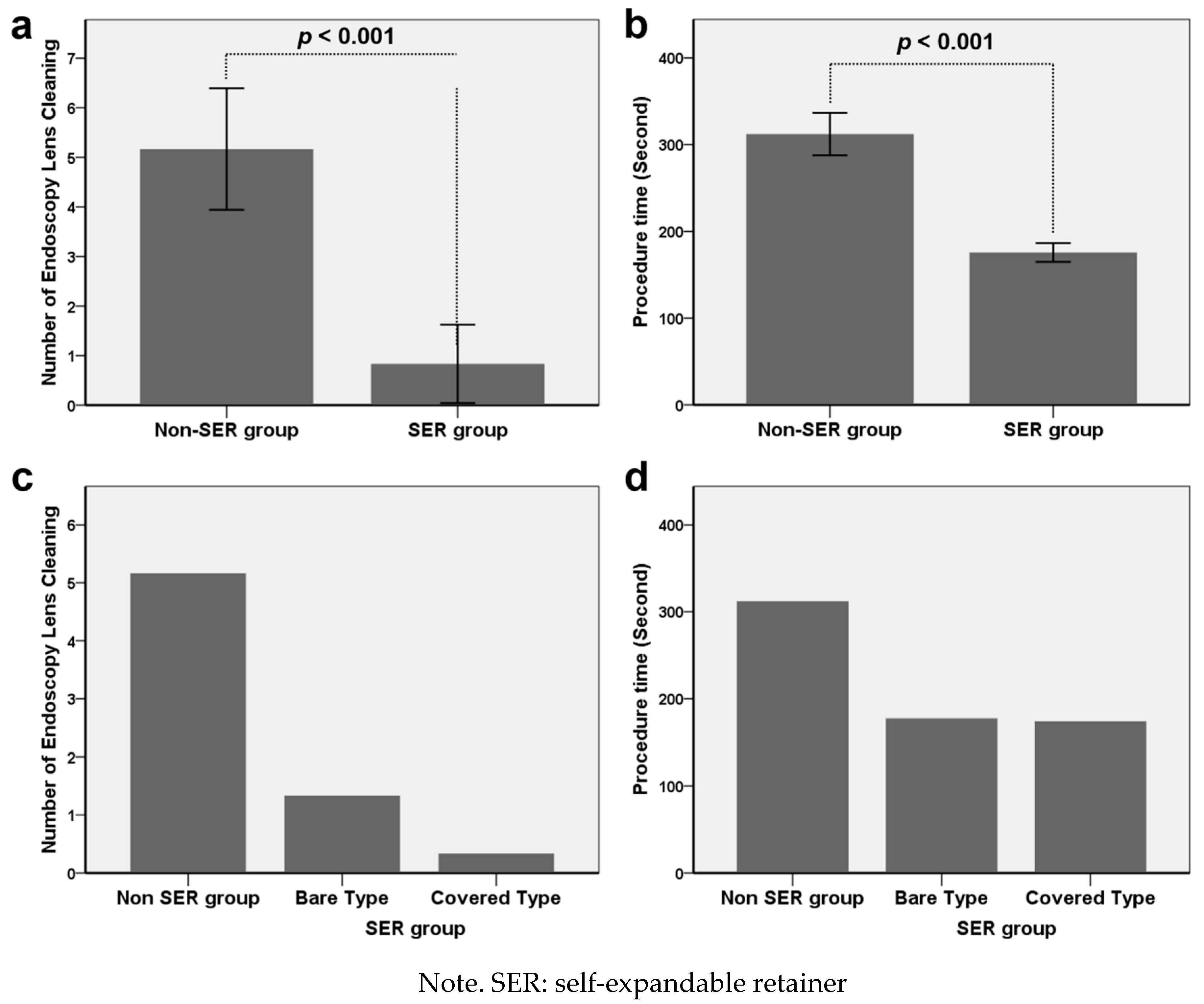
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kapadiya, M.; Tarabichi, M. An overview of endoscopic ear surgery in 2018. Laryngoscope Investig. Otolaryngol. 2019, 4, 365–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiringoda, R.; Kozin, E.D.; Lee, D.J. Outcomes in Endoscopic Ear Surgery. Otolaryngol. Clin N. Am. 2016, 49, 1271–1290. [Google Scholar] [CrossRef] [PubMed]
- Tarabichi, M. Endoscopic management of acquired cholesteatoma. Am. J. Otol. 1997, 18, 544–549. [Google Scholar] [PubMed]
- Tarabichi, M. Endoscopic middle ear surgery. Ann. Otol. Rhinol. Laryngol. 1999, 108, 39–46. [Google Scholar] [CrossRef]
- Mitchell, S.; Coulson, C. Endoscopic ear surgery: A hot topic? J. Laryngol. Otol. 2017, 131, 117–122. [Google Scholar] [CrossRef]
- Anson, B.J.; Donaldson, J.A. Surgical Anatomy of the Temporal Bone; Saunders: Philadelphia, PA, USA, 1981; Volume 31. [Google Scholar]
- Bojrab, D.I.; Bruderly, T.; Abdulrazzak, Y. Otitis externa. Otolaryngol. Clin. N. Am 1996, 29, 761–782. [Google Scholar]
- Preyer, S. Endoscopic ear surgery—A complement to microscopic ear surgery. HNO 2017, 65, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Tarabichi, M. Endoscopic transcanal middle ear surgery. Indian J. Otolaryngol. Head Neck Surg. 2010, 62, 6–24. [Google Scholar] [CrossRef] [Green Version]
- Parelkar, K.; Thorawade, V.; Marfatia, H.; Shere, D. Endoscopic cartilage tympanoplasty: Full thickness and partial thickness tragal graft. Braz. J. Otorhinolaryngol. 2019. [Google Scholar] [CrossRef]
- Anschuetz, L.; Bonali, M.; Guarino, P.; Fabbri, F.B.; Alicandri-Ciufelli, M.; Villari, D.; Caversaccio, M.; Presutti, L. Management of Bleeding in Exclusive Endoscopic Ear Surgery: Pilot Clinical Experience. Otolaryngol. Head Neck Surg. 2017, 157, 700–706. [Google Scholar] [CrossRef]
- Das, A.; Mitra, S.; Ghosh, D.; Kumar, S.; Sengupta, A. Does tranexamic acid improve intra-operative visualisation in endoscopic ear surgery? A double-blind, randomised, controlled trial. J. Laryngol. Otol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Swarup, A.; le Nobel, G.J.; Andrysek, J.; James, A.L. The Current Limitations and Future Direction of Instrument Design for Totally Endoscopic Ear Surgery: A Needs Analysis Survey. Otol. Neurotol. 2018, 39, 778–784. [Google Scholar] [CrossRef]
- Schuknecht, H.F.; Gulya, A.J. Anatomy of the Temporal Bone with Surgical Implications; Lea & Febiger: Philadelphia, PA, USA, 1986. [Google Scholar]
- Badr-El-Dine, M.; James, A.L.; Panetti, G.; Marchioni, D.; Presutti, L.; Nogueira, J.F. Instrumentation and technologies in endoscopic ear surgery. Otolaryngol. Clin. N. Am. 2013, 46, 211–225. [Google Scholar] [CrossRef]
- Kozin, E.D.; Kiringoda, R.; Lee, D.J. Incorporating Endoscopic Ear Surgery into Your Clinical Practice. Otolaryngol. Clin. N. Am. 2016, 49, 1237–1251. [Google Scholar] [CrossRef] [PubMed]
- Mijovic, T.; Lea, J. Training and education in endoscopic ear surgery. Curr. Otorhinolaryngol. Rep. 2015, 3, 193–199. [Google Scholar] [CrossRef]
- Alicandri-Ciufelli, M.; Molinari, G.; Beckmann, S.; Caversaccio, M.; Presutti, L.; Anschuetz, L. Epinephrine Use in Endoscopic Ear Surgery: Quantitative Safety Assessment. ORL 2019. [Google Scholar] [CrossRef]
- Zhang, Y.; Bai, Y.; Chen, M.; Zhou, Y.; Yu, X.; Zhou, H.; Chen, G. The safety and efficiency of intravenous administration of tranexamic acid in coronary artery bypass grafting (CABG): A meta-analysis of 28 randomized controlled trials. BMC Anesthesiol. 2019, 19, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, G.; Chen, G.; Huang, Q.; Huang, Z.; Alexander, P.G.; Lin, H.; Xu, H.; Zhou, Z.; Pei, F. The efficacy and safety of tranexamic acid for reducing blood loss following simultaneous bilateral total knee arthroplasty: A multicenter retrospective study. BMC Musculoskelet. Disord. 2019, 20, 325. [Google Scholar] [CrossRef] [Green Version]
- Ping, W.D.; Zhao, Q.M.; Sun, H.F.; Lu, H.S.; Li, F. Role of tranexamic acid in nasal surgery: A systemic review and meta-analysis of randomized control trial. Medicine 2019, 98, e15202. [Google Scholar] [CrossRef]
- Gilroy, A.M.; MacPherson, B.R.; Ross, L.M.; Broman, J.; Josephson, A. Atlas of Anatomy; Thieme Stuttgart: Stuttgart, Germany, 2008. [Google Scholar]
- Tomazic, P.V.; Hammer, G.P.; Gerstenberger, C.; Koele, W.; Stammberger, H. Heat development at nasal endoscopes’ tips: Danger of tissue damage? A laboratory study. Laryngoscope 2012, 122, 1670–1673. [Google Scholar] [CrossRef]
- Nelson, J.J.; Goyal, P. Temperature variations of nasal endoscopes. Laryngoscope 2011, 121, 273–278. [Google Scholar] [CrossRef] [PubMed]
- MacKeith, S.A.; Frampton, S.; Pothier, D.D. Thermal properties of operative endoscopes used in otorhinolaryngology. J. Laryngol. Otol. 2008, 122, 711–714. [Google Scholar] [CrossRef] [PubMed]
- Kozin, E.D.; Lehmann, A.; Carter, M.; Hight, E.; Cohen, M.; Nakajima, H.H.; Lee, D.J. Thermal effects of endoscopy in a human temporal bone model: Implications for endoscopic ear surgery. Laryngoscope 2014, 124, E332–E339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aksoy, F.; Dogan, R.; Ozturan, O.; Eren, S.B.; Veyseller, B.; Gedik, O. Thermal effects of cold light sources used in otologic surgery. Eur. Arch. Otorhinolaryngol. 2015, 272, 2679–2687. [Google Scholar] [CrossRef]
- Bottrill, I.; Perrault, D.F., Jr.; Poe, D. In vitro and in vivo determination of the thermal effect of middle ear endoscopy. Laryngoscope 1996, 106, 213–216. [Google Scholar] [CrossRef]
- Craig, J.; Goyal, P. Insulating and cooling effects of nasal endoscope sheaths and irrigation. Int. Forum Allergy Rhinol. 2014, 4, 759–762. [Google Scholar] [CrossRef]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Kang, J.M.; Song, H.-Y.; Kang, W.S.; Park, J.-H.; Chung, J.W. Self-Expandable Retainer for Endoscopic Visualization in the External Auditory Canal: Proof of Concept in Human Cadavers. Appl. Sci. 2020, 10, 1877. https://doi.org/10.3390/app10051877
Kim Y, Kang JM, Song H-Y, Kang WS, Park J-H, Chung JW. Self-Expandable Retainer for Endoscopic Visualization in the External Auditory Canal: Proof of Concept in Human Cadavers. Applied Sciences. 2020; 10(5):1877. https://doi.org/10.3390/app10051877
Chicago/Turabian StyleKim, Yehree, Jeon Min Kang, Ho-Young Song, Woo Seok Kang, Jung-Hoon Park, and Jong Woo Chung. 2020. "Self-Expandable Retainer for Endoscopic Visualization in the External Auditory Canal: Proof of Concept in Human Cadavers" Applied Sciences 10, no. 5: 1877. https://doi.org/10.3390/app10051877