An Innovative Bioceramic Bone Graft Substitute for Bone Defect Treatment: In Vivo Evaluation of Bone Healing

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Material Characterizations
2.3. Animal Study
2.4. Histological Analysis
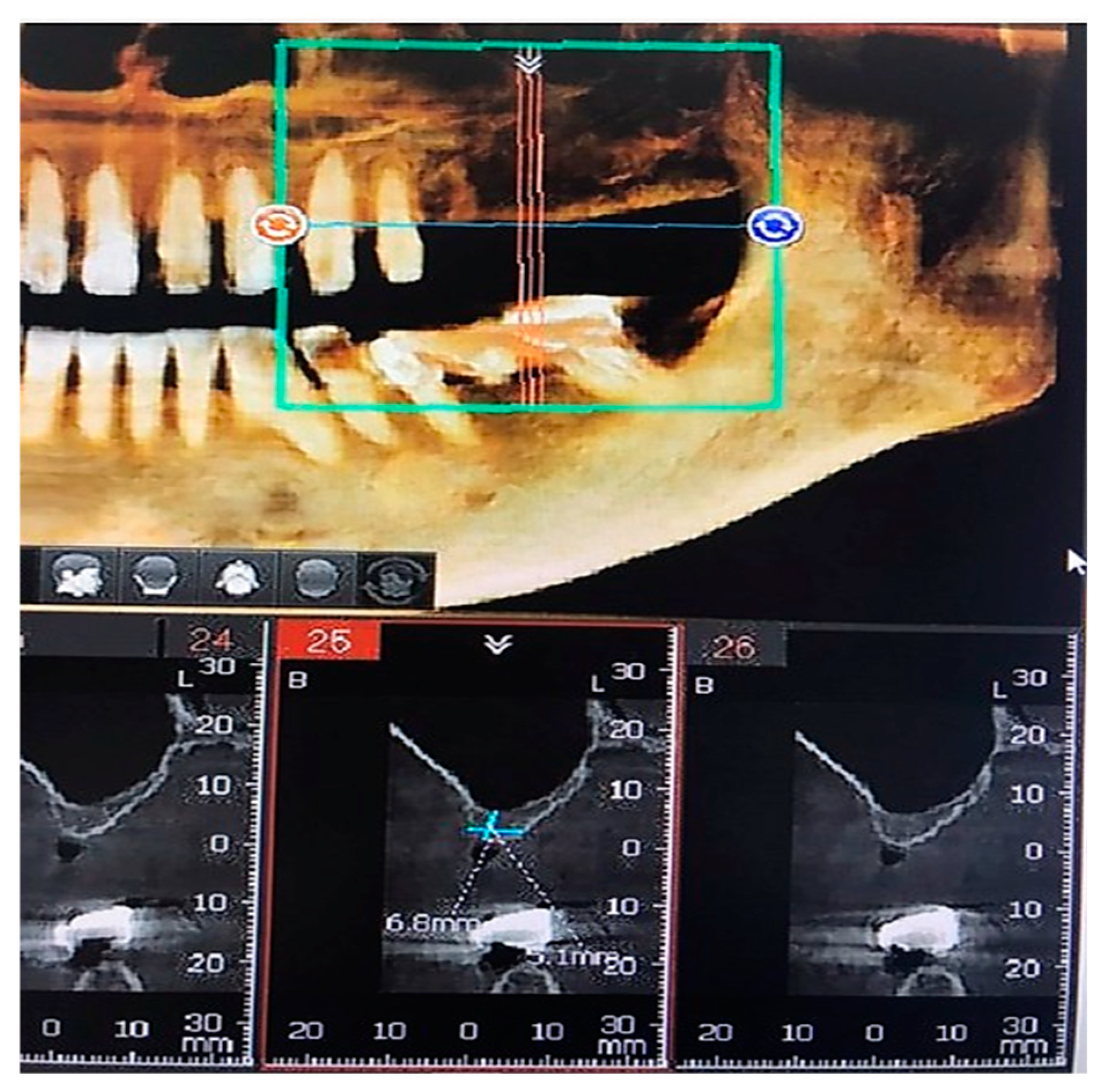
2.5. Bone Defect Treatment Analysis in Patient with Height Bone Loss in the Posterior Maxillary
3. Results and Discussion
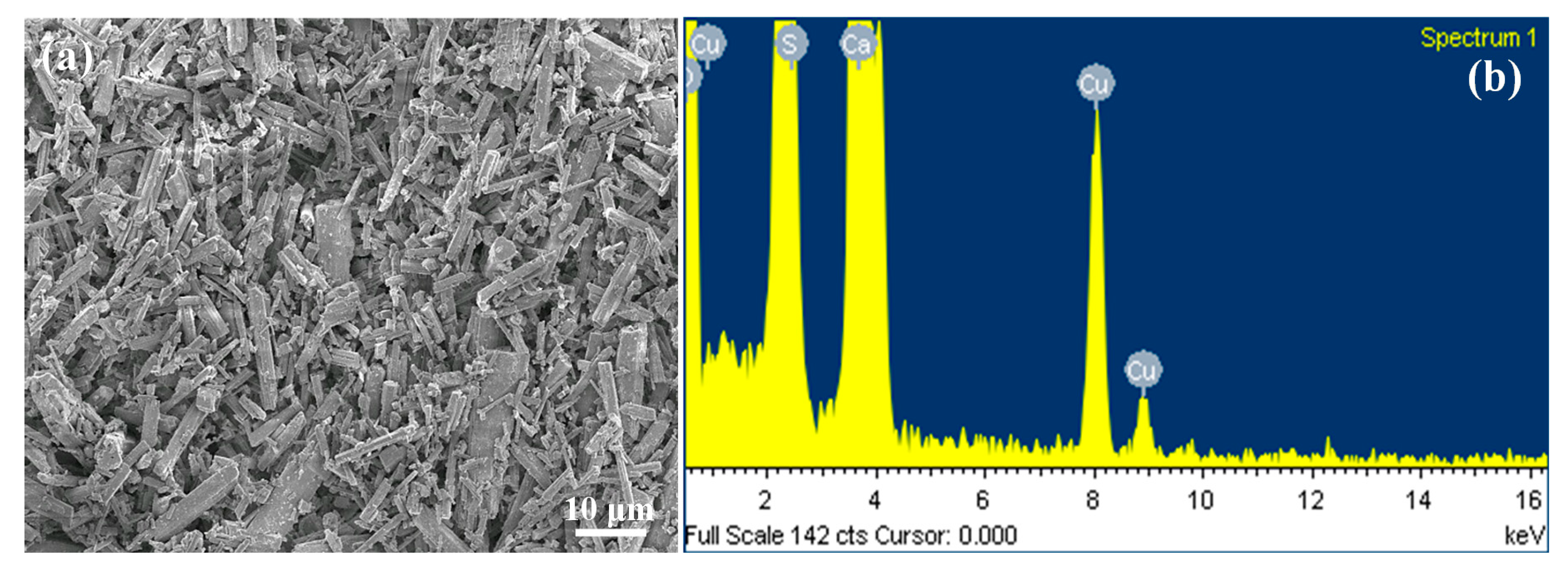
3.1. Morphology of the Innovate α-CSH Bioceramic
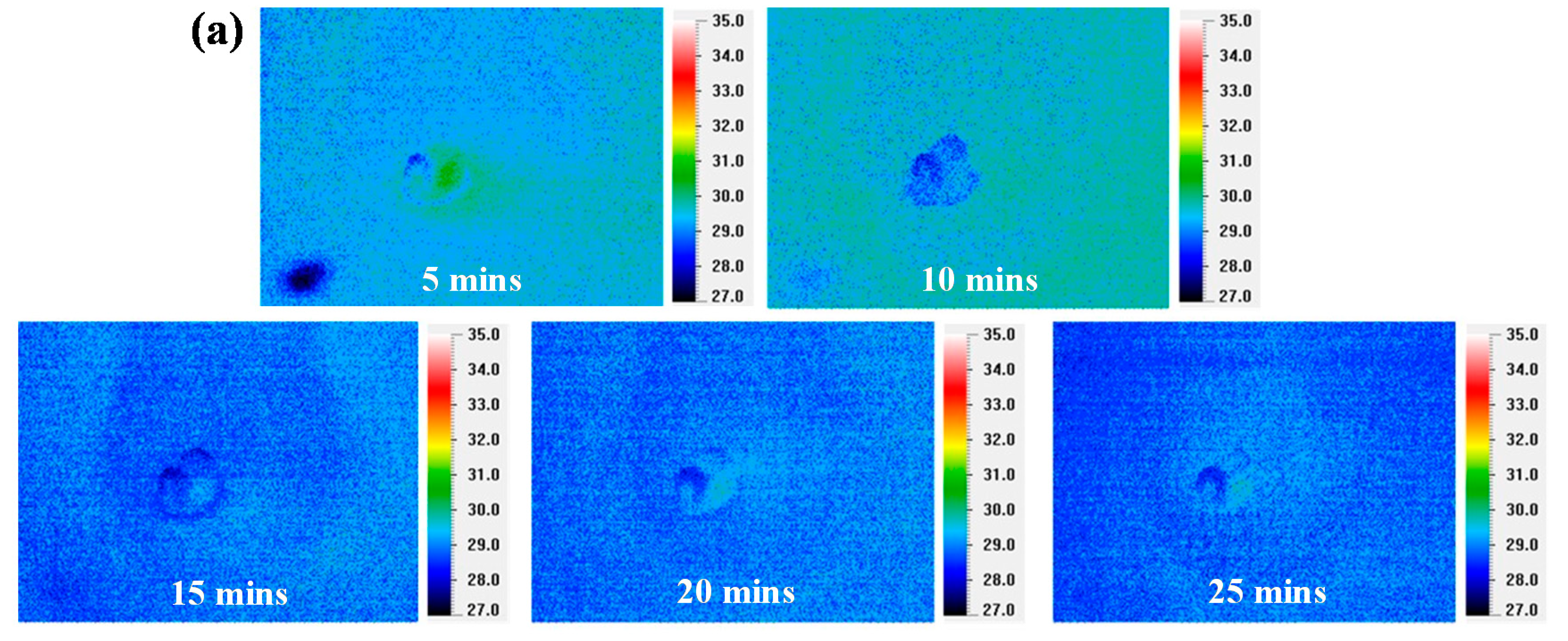
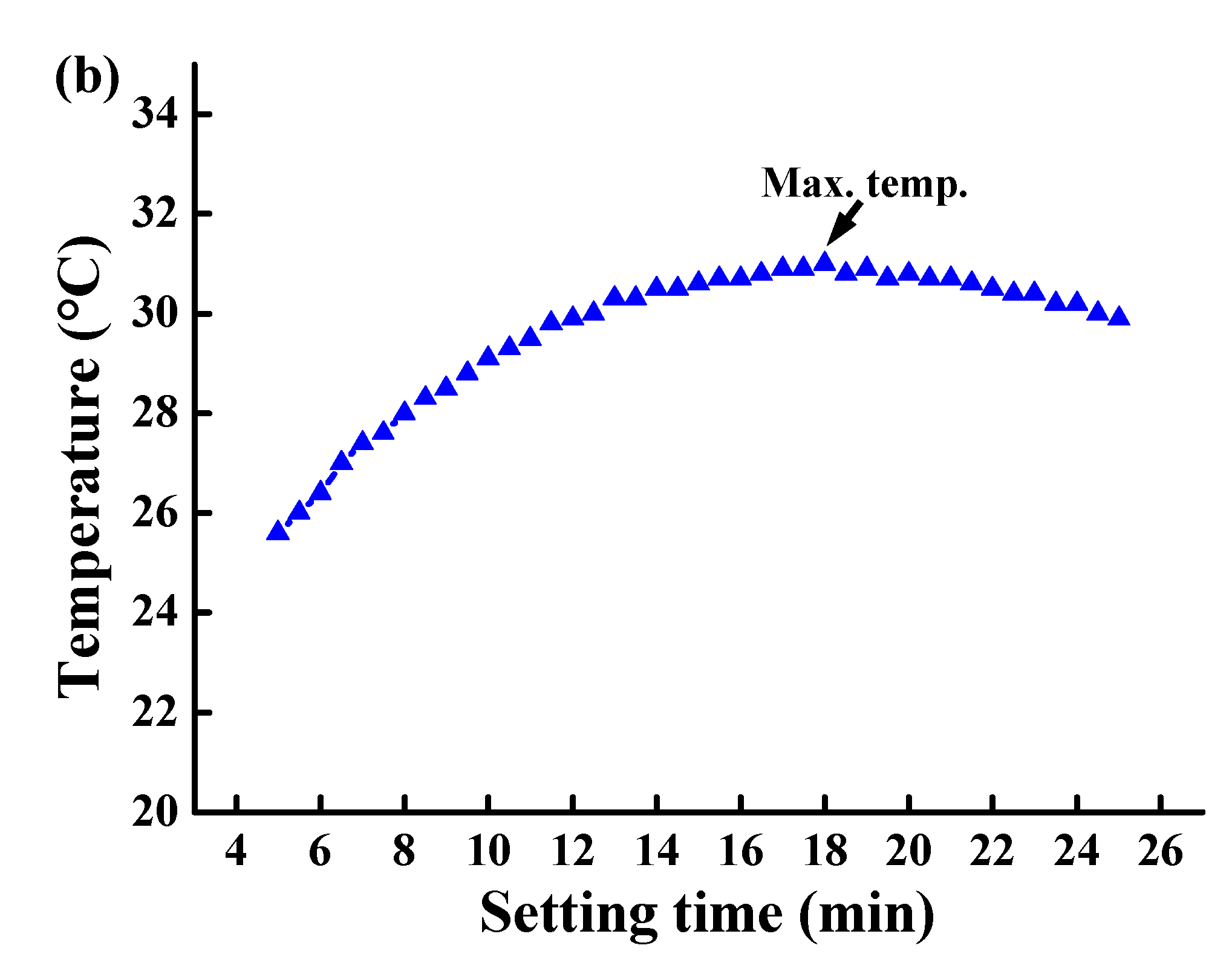
3.2. Thermal Observation in the Setting Process
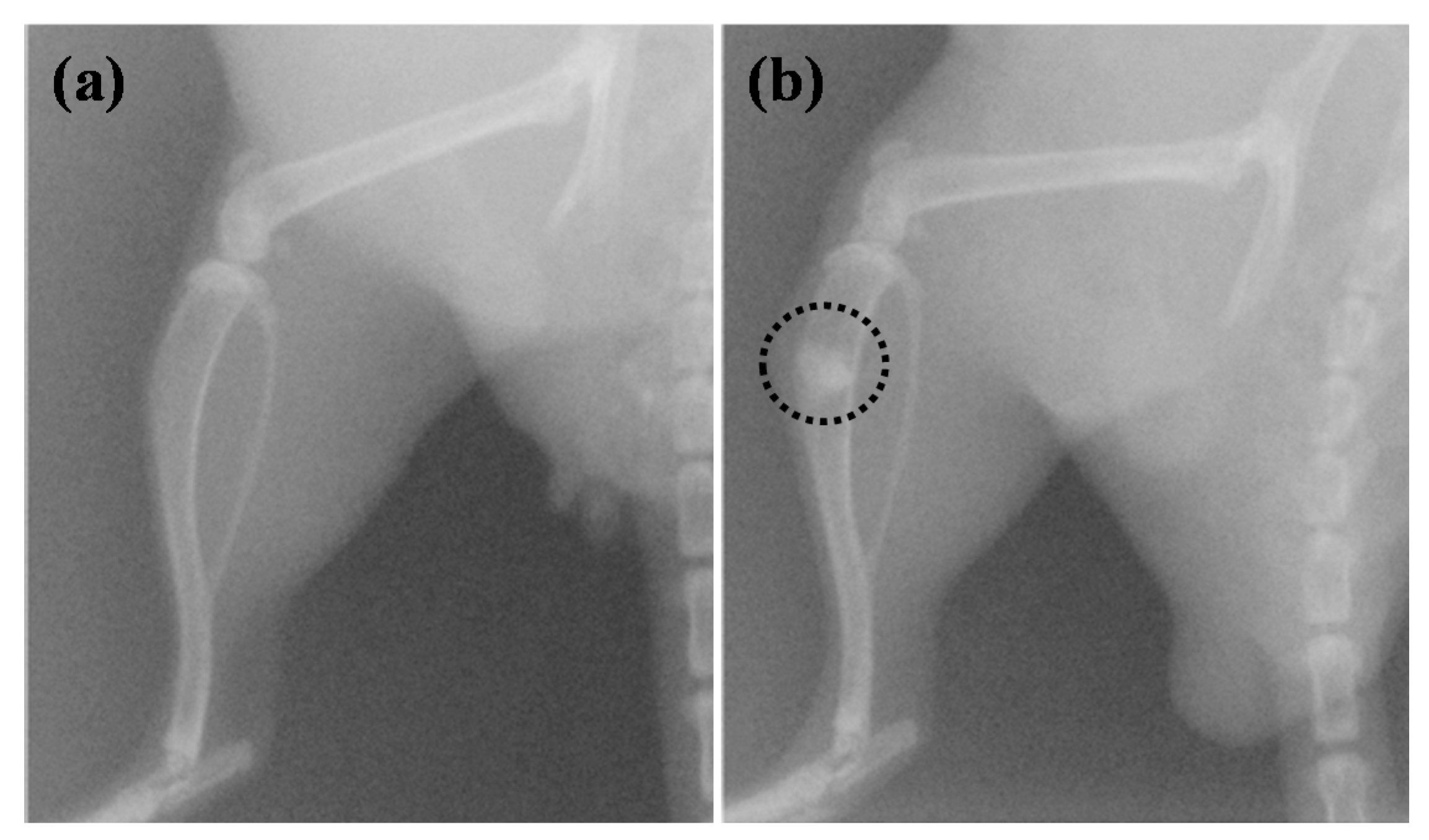
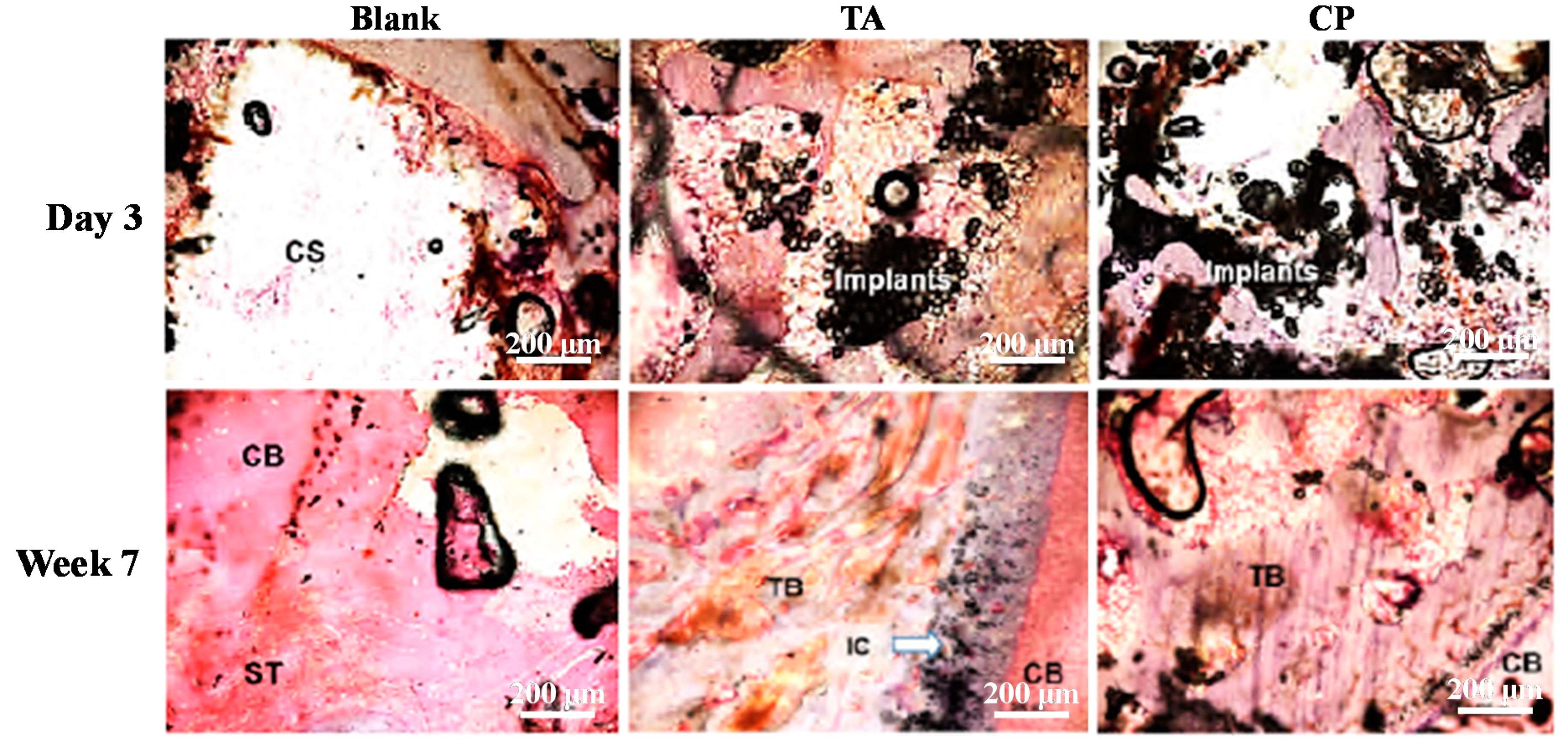
3.3. Bone Healing and Regeneration Characteristic of the Materials in the Animal Study
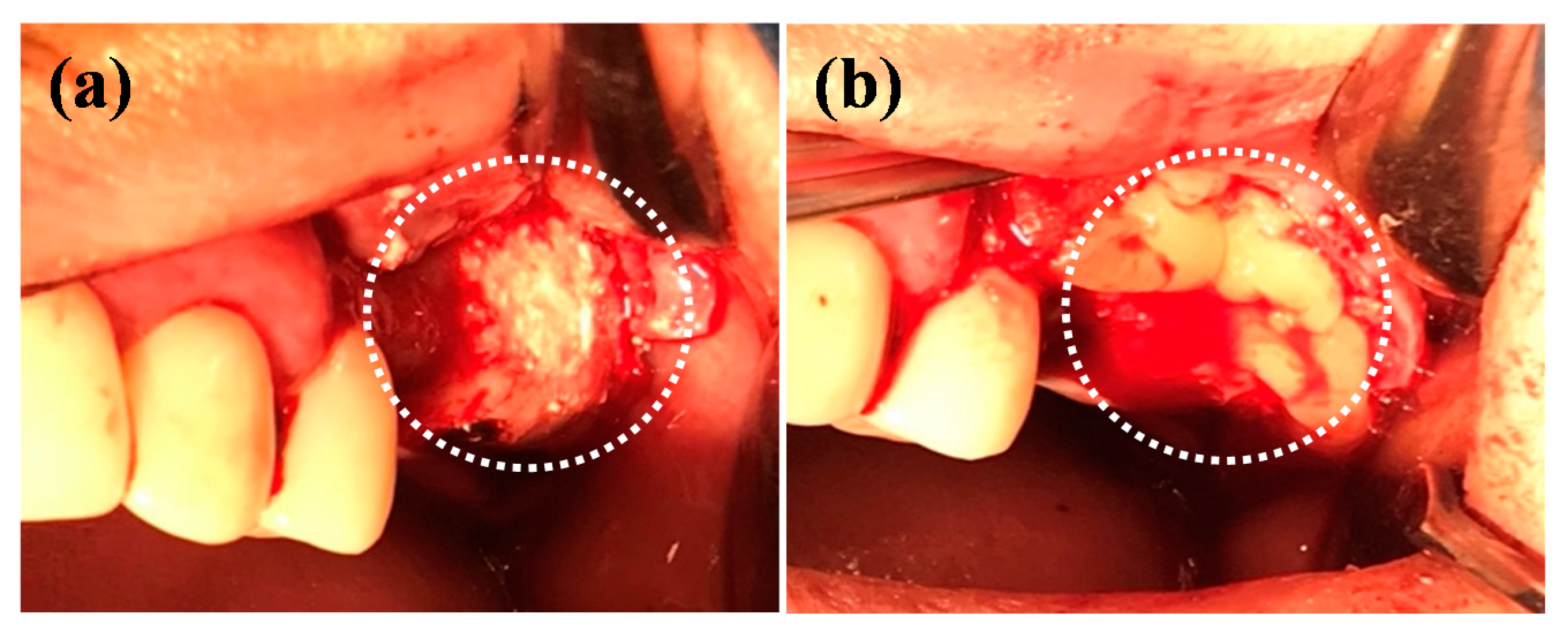
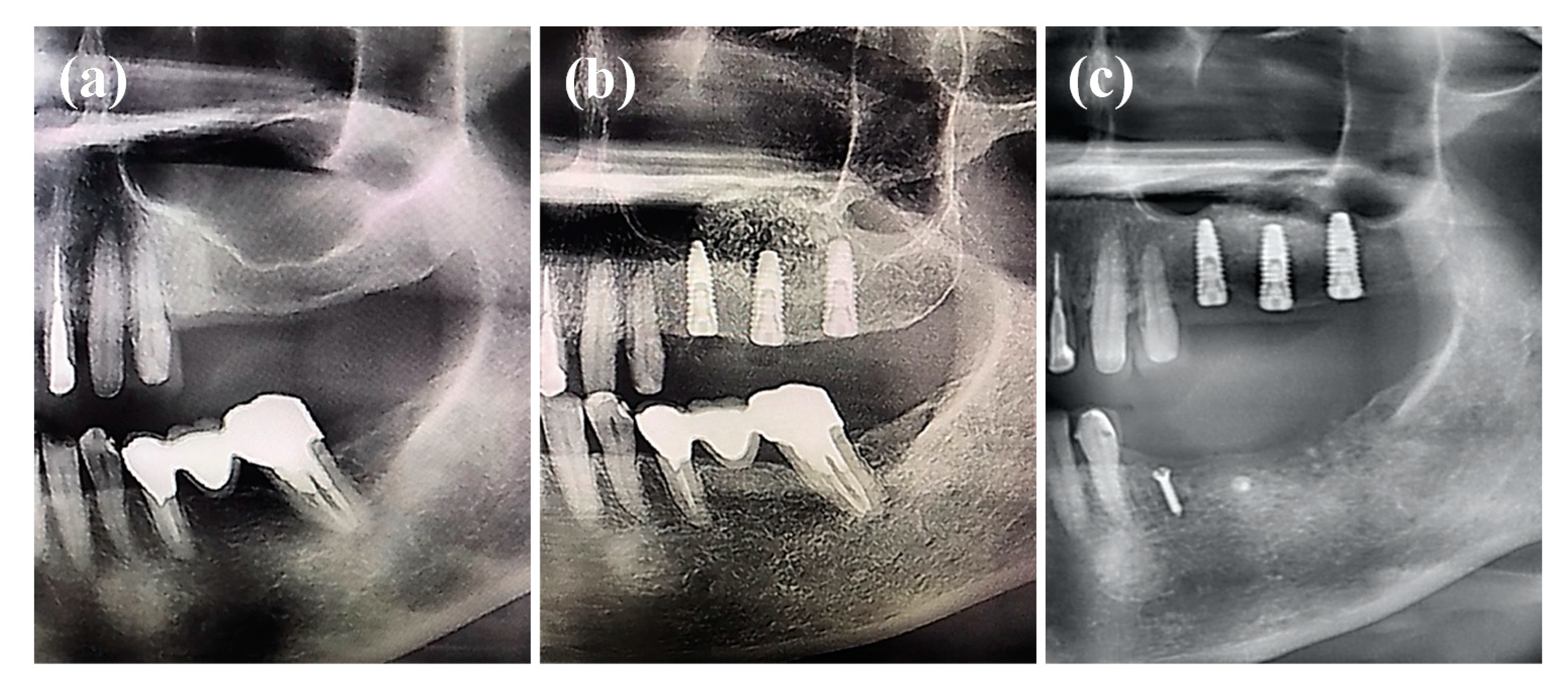
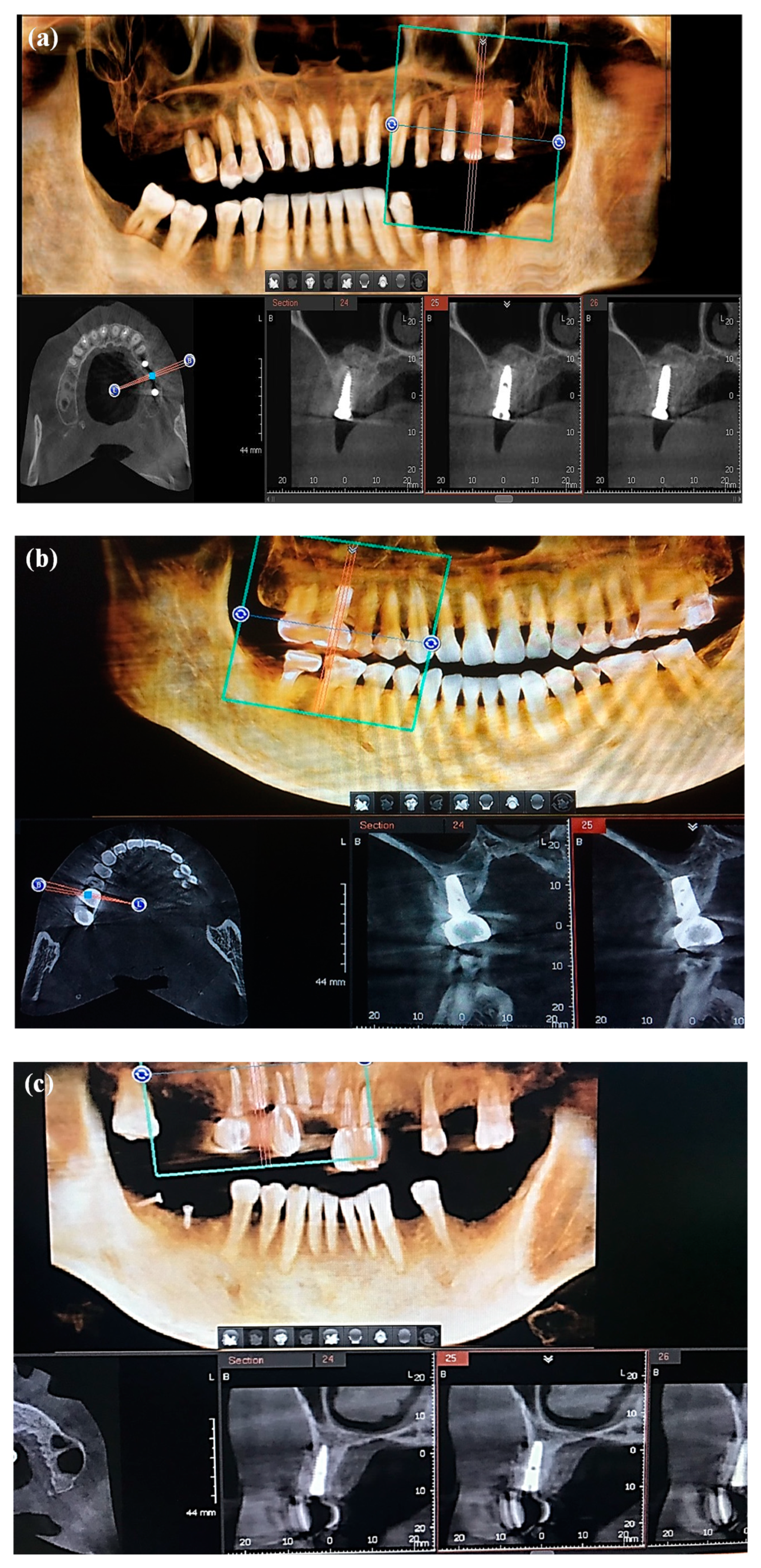
3.4. Bone Healing and Regeneration Characteristisc of the Materials in the Clinical Application
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Smrke, D.; Roman, P.; Veselko, M.; Gubi, B. Treatment of bone defects—allogenic platelet gel and autologous bone technique. Regenerat. Med. Tissue Eng. 2013. [Google Scholar] [CrossRef] [Green Version]
- Wiese, A.; Pape, H.C. Bone defects caused by high-energy injuries, bone loss, infected nonunions, and nonunions. Orthop. Clin. North Am. 2010, 41, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Titsinides, S.; Agrogiannis, G.; Karatzas, T. Bone grafting materials in dentoalveolar reconstruction: A comprehensive review. Jpn. Dent. Sci. Rev. 2019, 55, 26–32. [Google Scholar] [CrossRef]
- Fernandez de Grado, G.; Keller, L.; Idoux-Gillet, Y.; Wagner, Q.; Musset, A.-M.; Benkirane-Jessel, N.; Bornert, F.; Offner, D. Bone substitutes: A review of their characteristics, clinical use, and perspectives for large bone defects management. J. Tissue Eng. 2018, 9, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, V.; Helder, M.N.; Bravenboer, N.; Ten Bruggenkate, C.M.; Jin, J.; Klein-Nulend, J.; Schulten, E. Bone tissue regeneration in the oral and maxillofacial region: A review on the application of stem cells and new strategies to improve vascularization. Stem Cells Int. 2019, 2019, 6279721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfotawi, R.; Ayoub, A. reconstruction of maxillofacial bone defects: Contemporary methods and future techniques. Am. J. Adv. Med. Sci. 2014, 2, 10. [Google Scholar]
- Gjerde, C.; Mustafa, K.; Hellem, S.; Rojewski, M.; Gjengedal, H.; Yassin, M.A.; Feng, X.; Skaale, S.; Berge, T.; Rosen, A.; et al. Cell therapy induced regeneration of severely atrophied mandibular bone in a clinical trial. Stem Cell Res. Ther. 2018, 9, 213. [Google Scholar] [CrossRef] [PubMed]
- Kheirallah, M.; Almeshaly, H. Bone graft substitutes for bone defect regeneration. A collective review. Int. J. Dent. Oral Sci. 2016, 247–255. [Google Scholar] [CrossRef]
- Haugen, H.J.; Lyngstadaas, S.P.; Rossi, F.; Perale, G. Bone grafts: Which is the ideal biomaterial? J. Clin. Periodontol. 2019, 46 (Suppl. 21), 92–102. [Google Scholar] [CrossRef]
- Khodakaram-Tafti, A.; Mehrabani, D.; Shaterzadeh-Yazdi, H.; Zamiri, B.; Omidi, M. Tissue engineering in maxillary bone defects. World J. Plast. Surg. 2018, 7, 9. [Google Scholar]
- Faverani, L.P.; Ramalho-Ferreira, G.; Santos, P.H.; Rocha, E.P.; Garcia Junior, I.R.; Pastori, C.M.; Assuncao, W.G. Surgical techniques for maxillary bone grafting-Literature review. Rev. Col. Bras. Cir. 2014, 41, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz, A.D.; Peixoto, G.A.; Aguiar, M.F.; Camargo, G.; Homs, N. Surgeons’ Performance determining the amount of graft material for sinus floor augmentation using tomography. Braz. Dent. J. 2017, 28, 385–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khojasteh, A.; Esmaeelinejad, M.; Aghdashi, F. Regenerative techniques in oral and maxillofacial bone grafting. In A Textbook of Advanced Oral and Maxillofacial Surgery; IntechOpen: London, UK, 2015; Volume 2. [Google Scholar] [CrossRef]
- Vieira, J.S.; Brandao-Filho, E.M.; Deliberador, F.R.; Zielak, J.C.; Giovanini, A.F.; Deliberador, T.M. Dental implant placement with simultaneous anterior maxillary reconstruction with block and particulate fresh frozen allograft bone: A case report with 24-month follow-up data. Case Rep. Surg. 2017, 2017, 1565973. [Google Scholar] [CrossRef] [PubMed]
- Rivara, F.; Negri, M.; Lumetti, S.; Parisi, L.; Toffoli, A.; Calciolari, E.; Manfredi, E.; Macaluso, G.M. Maxillary sinus floor augmentation using an equine-derived graft material: Preliminary results in 17 patients. Biomed. Res. Int. 2017, 2017, 9164156. [Google Scholar] [CrossRef] [Green Version]
- Turri, A.; Dahlin, C. Comparative maxillary bone-defect healing by calcium-sulphate or deproteinized bovine bone particles and extra cellular matrix membranes in a guided bone regeneration setting: An experimental study in rabbits. Clin. Oral Implants Res. 2015, 26, 501–506. [Google Scholar] [CrossRef]
- Monje, A.; Urban, I.A.; Miron, R.J.; Caballe-Serrano, J.; Buser, D.; Wang, H.L. Morphologic patterns of the atrophic posterior maxilla and clinical implications for bone regenerative therapy. Int J. Periodont. Restorat. Dent. 2017, 37, e279–e289. [Google Scholar] [CrossRef] [Green Version]
- Kashani, H.; Dasmah, A.; Mokhtari, R.; Dahlin, C. Sinus-lift by use of hemihydrate-calcium sulphate: A prospective clinical, radiographical, histological study of implant integration in the posterior maxilla. EC Dent. Sci. 2017, 15, 10. [Google Scholar]
- Suleiman, M.S.; Hasouni, M.K. Effect of β-calcium sulphate hemihydrate on mandible healing in dog (radiographical assessment using Image-J Program). Iraqi J. Vet. Sci. 2014, 28, 10. [Google Scholar] [CrossRef]
- Pillai, S.; Ganapathy, D. Bone substitutes for sinus lift. J. Pharm. Sci. Res. 2016, 8, 6. [Google Scholar]
- Silva, L.D.; de Lima, V.N.; Faverani, L.P.; de Mendonca, M.R.; Okamoto, R.; Pellizzer, E.P. Maxillary sinus lift surgery-with or without graft material? A systematic review. Int. J. Oral Maxillofac. Surg. 2016, 45, 1570–1576. [Google Scholar] [CrossRef] [Green Version]
- Yousefi, A.M. A review of calcium phosphate cements and acrylic bone cements as injectable materials for bone repair and implant fixation. J. Appl. Biomater. Funct. Mater. 2019, 17, 2280800019872594. [Google Scholar] [CrossRef]
- Yashavantha, K.C.; Nalini, K.B.; Jagdish Menon, D.K.P.; Banerji, B.H. Calcium sulfate as bone graft substitute in the treatment of osseous bone defects, a prospective study. J. Clin. Diagn. Res. 2013, 7, 2926–2928. [Google Scholar] [CrossRef]
- McCall, T.A.; Brokaw, D.S.; Jelen, B.A.; Scheid, D.K.; Scharfenberger, A.V.; Maar, D.C.; Green, J.M.; Shipps, M.R.; Stone, M.B.; Musapatika, D.; et al. Treatment of large segmental bone defects with reamer-irrigator-aspirator bone graft: Technique and case series. Orthop. Clin. North. Am. 2010, 41, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Meng, Z.L.; Wu, Z.Q.; Shen, B.X.; Li, H.B.; Bian, Y.Y.; Zeng, L.; Fu, J.; Peng, L. Reconstruction of large segmental bone defects in rabbit using the Masquelet technique with alpha-calcium sulfate hemihydrate. J. Orthop. Surg. Res. 2019, 14, 192. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Qin, C.H.; Ma, Y.F.; Wang, L.; Yu, B. Possibility of one-stage surgery to reconstruct bone defects using the modified Masquelet technique with degradable calcium sulfate as a cement spacer: A case report and hypothesis. Biomed. Rep. 2016, 4, 374–378. [Google Scholar] [CrossRef] [Green Version]
- Sakkas, A.; Wilde, F.; Heufelder, M.; Winter, K.; Schramm, A. Autogenous bone grafts in oral implantology-is it still a “gold standard”? A consecutive review of 279 patients with 456 clinical procedures. Int. J. Implant. Dent. 2017, 3, 23. [Google Scholar] [CrossRef]
- Salamanca, E.; Hsu, C.C.; Huang, H.M.; Teng, N.C.; Lin, C.T.; Pan, Y.H.; Chang, W.J. Bone regeneration using a porcine bone substitute collagen composite in vitro and in vivo. Sci. Rep. 2018, 8, 984. [Google Scholar] [CrossRef] [Green Version]
- Maghaireh, H.; Hussain, I. Localized maxillary ridge augmentation using onlay technique with a xenograft block for dental implant placement: A case series. Smile Dent. J. 2012, 7, 6. [Google Scholar]
- Ortiz-Vigon, A.; Suarez, I.; Martinez-Villa, S.; Sanz-Martin, I.; Bollain, J.; Sanz, M. Safety and performance of a novel collagenated xenogeneic bone block for lateral alveolar crest augmentation for staged implant placement. Clin. Oral Implants Res. 2018, 29, 36–45. [Google Scholar] [CrossRef]
- Scarano, A.; Carinci, F.; Assenza, B.; Piattelli, M.; Murmura, G.; Piattelli, A. Vertical ridge augmentation of atrophic posterior mandible using an inlay technique with a xenograft without miniscrews and miniplates: Case series. Clin. Oral Implants Res. 2011, 22, 1125–1130. [Google Scholar] [CrossRef]
- Zafar, M.J.; Zhu, D.; Zhang, Z. 3D Printing of bioceramics for bone tissue engineering. Materials 2019, 12, 3361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Favvas, E.P.; Stefanopoulos, K.L.; Vordos, N.C.; Drosos, G.I.; Mitropoulos, A.C. Structural characterization of calcium sulfate bone graft substitute cements. Mater. Res. 2016, 19, 1108–1113. [Google Scholar] [CrossRef] [Green Version]
- Thomas, M.V.; Puleo, D.A. Calcium sulfate: Properties and clinical applications. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 88, 597–610. [Google Scholar] [CrossRef] [PubMed]
- Al-Haddad, A.; Che Ab Aziz, Z.A. Bioceramic-based root canal sealers: A review. Int. J. Biomater. 2016, 2016, 9753210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarano, A.; Quaranta, A.; Feregalli, B.; Di Cristinzi, A.; Carinci, F.; Lauritano, D. Haemostasis control in dental extraction with calcium sulphate: A case series. Eur. J. Inflamm. 2012, 10, 5. [Google Scholar]
- Scarano, A.; Sinjari, B.; Murmura, G.; Mijiritsky, E.; Iaculli, F.; Mortellaro, C.; Tete, S. Hemostasis control in dental extractions in patients receiving oral anticoagulant therapy: An approach with calcium sulfate. J. Craniofac. Surg. 2014, 25, 843–846. [Google Scholar] [CrossRef]
- Jang, Y.; Kim, H.; Roh, B.D.; Kim, E. Biologic response of local hemostatic agents used in endodontic microsurgery. Restorat. Dent. Endodont. 2014, 39, 79–88. [Google Scholar] [CrossRef] [Green Version]
- Menendez Nieto, I.; Cervera Ballester, J.; Penarrocha Diago, M.; Penarrocha Oltra, D. New perspectives in periapical surgery: Hemostasis. J. Oral Sci. Rehabilit. 2018, 4, 4. [Google Scholar]
- Ou, K.-L.; Hou, P.-J.; Huang, B.-H.; Chou, H.-H.; Yang, T.-S.; Huang, C.-F.; Ueno, T. Bone healing and regeneration potential in rabbit cortical defects using an innovative bioceramic bone graft substitute. Appl. Sci. 2020, 10, 6239. [Google Scholar] [CrossRef]
- Hsu, H.-J.; Waris, R.A.; Ruslin, M.; Lin, Y.-H.; Chen, C.-S.; Ou, K.-L. An innovative α-calcium sulfate hemihydrate bioceramic as a potential bone graft substitute. J. Am. Ceram. Soc. 2017, 101, 419–427. [Google Scholar] [CrossRef]
- Dunne, N.; Ormsby, R.W. MWCNT Used in Orthopaedic Bone Cements; IntechOpen: London, UK, 2011. [Google Scholar]
- Liptakova, T.; Lelovics, H.; Necas, L. Variations of temperature of acrylic bone cements prepared by hand and vacuum mixing during their polymerization. Acta Bioeng. Biomech. 2009, 11, 5. [Google Scholar]
- Abu Zeid, S.T.; Mokeem Saleh, A.A.; Khafagi, M.G.E.-D.; Abou Neel, E.A. Setting reaction of new bioceramic root canal sealers. Spectrosc. Lett. 2018, 51, 426–430. [Google Scholar] [CrossRef]
- Gupta, A.; Kumar, P. Assessment of the histological state of the healing wound. Plast. Aesthet. Res. 2015, 2, 239–242. [Google Scholar] [CrossRef] [Green Version]
- Sculean, A.; Stavropoulos, A.; Bosshardt, D.D. Self-regenerative capacity of intra-oral bone defects. J. Clin. Periodontol. 2019, 46 (Suppl. 21), 70–81. [Google Scholar] [CrossRef] [Green Version]
- Hori, M.; Kaneko, K.; Harada, D.; Nakanishi, K.; Tanaka, T.; Ishii, T.; Tanaka, H. Treatment planning in a case of restoration of the maxilla and mandible using osseointegrated with four types of bone graft. J. Oral Sci. 2003, 45, 6. [Google Scholar] [CrossRef] [Green Version]
- Pirpir, C.; Yilmaz, O.; Candirli, C.; Balaban, E. Evaluation of effectiveness of concentrated growth factor on osseointegration. Int. J. Implant. Dent. 2017, 3, 7. [Google Scholar] [CrossRef] [Green Version]
- Tabatabaei, F.; Aghamohammadi, Z.; Tayebi, L. In vitro and in vivo effects of concentrated growth factor on cells and tissues. J. Biomed. Mater. Res. A 2020, 108, 1338–1350. [Google Scholar] [CrossRef]
- Begum, M.; Reddy, J.T.; Kumar, K.V.S.; Naik, P.M. Concentrated growth factor (CGF) in alveolar bone grafting procedures: Dilemma or a reality? A detailed review. Glob. J. Med. Res. 2019, 19, 6. [Google Scholar]
- Kumar, Y.P. Role of CGF (Concentrated Growth Factor) in periodontal regeneration. J. Dent. Health Oral Dis. Ther. 2018, 9, 350–352. [Google Scholar] [CrossRef] [Green Version]
- Crespi, R.; Vinci, R.; Cappare, P.; Gherlone, E.; Romanos, G.E. Calvarial versus iliac crest for autologous bone graft material for a sinus lift procedure: A histomorphometric study. Int. J. Oral Maxillofac. Implants 2007, 22, 6. [Google Scholar]
- Moraschini, V.; Mourão, C.F.d.A.B.; Machado, R.C.d.M.; Nascimento, J.R.B.; Javid, K.; Calasans-Maia, M.D.; Cardarelli, A.; Montemezzi, P.; Calasans-Maia, J.d.A. Does platelet-rich fibrin decrease dimensional changes and improve postoperative comfort in post-extraction sockets? An overview of systematic reviews. Appl. Sci. 2020, 10. [Google Scholar] [CrossRef]
- Dimitriou, R.; Mataliotakis, G.I.; Angoules, A.G.; Kanakaris, N.K.; Giannoudis, P.V. Complications following autologous bone graft harvesting from the iliac crest and using the RIA: A systematic review. Injury 2011, 42 (Suppl. 2), S3–S15. [Google Scholar] [CrossRef] [PubMed]
- Saha, A.; Shah, S.; Waknis, P.; Bhujbal, P.; Aher, S.; Vaswani, V. Comparison of minimally invasive versus conventional open harvesting technique for iliac bone graft in secondary alveolar bone grafting in cleft palate patients: A systematic review. J. Korean Assoc. Oral Maxillofac. Surg. 2019, 45, 241–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Sun, X.; Yu, J.; Wang, J.; Zhai, P.; Chen, S.; Liu, M.; Zhou, Y. Platelet-rich fibrin as a bone graft material in oral and maxillofacial bone regeneration: Classification and summary for better application. Biomed. Res. Int. 2019, 2019, 3295756. [Google Scholar] [CrossRef]
- Wang, W.; Yeung, K.W.K. Bone grafts and biomaterials substitutes for bone defect repair: A review. Bioact. Mater. 2017, 2, 224–247. [Google Scholar] [CrossRef]
- Borrelli, J., Jr.; Prickett, W.D.; Ricci, W.M. Treatment of nonunions and osseous defects with bone graft and calcium sulfate. Clin. Orthop. Relat. Res. 2003, 411, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Szponder, T.; Mytnik, E.; Jaegermann, Z. Use of calcium sulfate as a biomaterial in the treatment of bone fractures in rabbits–preliminary studies. Bull. Vet. Inst. Pulawy 2013, 57, 119–122. [Google Scholar] [CrossRef] [Green Version]
- Yang, B.C.; Lee, J.W.; Ju, C.P.; Chern Lin, J.H. Physical/chemical properties and resorption behavior of a newly developed Ca/P/S-based bone substitute material. Materials 2020, 13, 3458. [Google Scholar] [CrossRef]
- Lei, D.; Zhanzhong, M.; Huaikuo, Y.; Lei, X.; Gongbo, Y. Treatment of Distal Radius Bone Defects with Injectable Calcium Sulphate Cement, Bone Grafting; IntechOpen: London, UK, 2012. [Google Scholar]
- Mukherji, A.; Rath, S. Calcium sulfate in periodontics: A time tested versatile alloplast. J. Sci. Soc. 2016, 43, 18. [Google Scholar] [CrossRef]
- Menendez, L.R.; Mirzayan, R.; Samimi, B.; Lindberg, A.W.; Allison, D.C. A comparison of mineral bone graft substitutes for bone defects. Oncol. Hematol. Rev. 2011, 7, 38–49. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Pi, B.; Wang, J.-N.; Zhu, X.-S.; Yang, H.-L. Preparation and properties of calcium sulfate bone cement incorporated with silk fibroin and Sema3A-loaded chitosan microspheres. Front. Mater. Sci. 2015, 9, 51–65. [Google Scholar] [CrossRef]
- Hesaraki, S.; Moztarzadeh, F.; Nemati, R.; Nezafati, N. Preparation and characterization of calcium sulfate-biomimetic apatite nanocomposites for controlled release of antibiotics. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 91, 651–661. [Google Scholar] [CrossRef] [PubMed]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Syam, S.; Cho, Y.-C.; Liu, C.-M.; Huang, M.-S.; Lan, W.-C.; Huang, B.-H.; Ueno, T.; Tsai, C.-H.; Saito, T.; Chen, M.-S.; et al. An Innovative Bioceramic Bone Graft Substitute for Bone Defect Treatment: In Vivo Evaluation of Bone Healing. Appl. Sci. 2020, 10, 8303. https://doi.org/10.3390/app10228303
Syam S, Cho Y-C, Liu C-M, Huang M-S, Lan W-C, Huang B-H, Ueno T, Tsai C-H, Saito T, Chen M-S, et al. An Innovative Bioceramic Bone Graft Substitute for Bone Defect Treatment: In Vivo Evaluation of Bone Healing. Applied Sciences. 2020; 10(22):8303. https://doi.org/10.3390/app10228303
Chicago/Turabian StyleSyam, Syamsiah, Yung-Chieh Cho, Chung-Ming Liu, Mao-Suan Huang, Wen-Chien Lan, Bai-Hung Huang, Takaaki Ueno, Chi-Hsun Tsai, Takashi Saito, May-Show Chen, and et al. 2020. "An Innovative Bioceramic Bone Graft Substitute for Bone Defect Treatment: In Vivo Evaluation of Bone Healing" Applied Sciences 10, no. 22: 8303. https://doi.org/10.3390/app10228303