Custom-Made Horizontal and Vertical Maxillary Augmentation with Smartbone® On Demand™: A Seven-Year Follow-Up Case

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
2.1. Methods
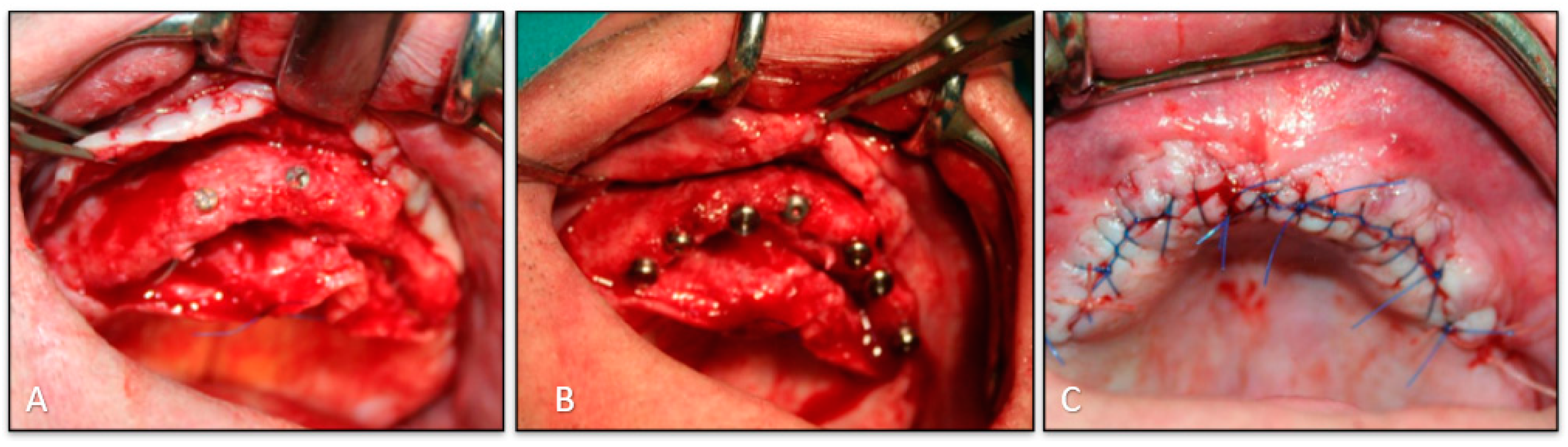
2.2. Surgical Phase
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Consent to Participate
References
- Belleggia, F.; Pozzi, A.; Rocci, M.; Barlattani, A.; Gargari, M. Piezoelectric surgery in mandibular split crest technique with immediate implant placement: A case report. Oral Implantol. (Rome) 2008, 1, 116–123. [Google Scholar]
- Chiapasco, M.; Abati, S.; Romeo, E.; Vogel, G. Clinical outcome of autogenous bone blocks or guided tissue regeneration with e-PTFE membranes for the reconstruction of narrow edentulous ridges. Clin. Oral Implants Res. 1999, 10, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, R.A.; Leventis, M.D.; Rohrer, M.D.; Prasad, H.S. Bone grafting: History, rationale, and selection of materials and techniques. Compend. Contin. Educ. Dent. 2014, 35 (Suppl. S4), 1–6. [Google Scholar] [PubMed]
- Kim, Y.K.; Kim, S.G.; Byeon, J.H.; Lee, H.J.; Um, I.U.; Lim, S.C.; Kim, S.Y. Development of a novel bone grafting material using autogenous teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, 496–503. [Google Scholar] [CrossRef]
- Block, M.S.; Kent, J.N. Sinus augmentation for dental implants: The use of autogenous bone. J. Oral Maxillofac. Surg. 1997, 55, 1281–1286. [Google Scholar] [CrossRef]
- Haugen, H.J.; Lyngstadaas, S.P.; Rossi, F.; Perale, G. Bone grafts: Which is the ideal biomaterial? J. Clin. Periodontol. 2019, 90, 1–11. [Google Scholar] [CrossRef]
- He, J.; Genetos, D.C.; Leach, J.K. Osteogenesis and trophic factor secretion are influenced by the composition of hydroxyapatite/poly(lactide-co-glycolide) composite scaffolds. Tissue Eng. Part A 2010, 16, 127–137. [Google Scholar] [CrossRef] [Green Version]
- Kane, R.J.; Roeder, R.K. Effects of hydroxyapatite reinforcement on the architecture and mechanical properties of freeze-dried collagen scaffolds. J. Mech. Behav. Biomed. Mater. 2012, 7, 41–49. [Google Scholar] [CrossRef]
- Jeong, S.I.; Lee, A.Y.; Shin, H. Electrospun gelatin/poly(L-lactide-co-ε-caprolactone) nanofibers for mechanically functional tissue-engineering scaffolds. J. Biomater. Sci. Polym. Ed. 2008, 19, 339–357. [Google Scholar] [CrossRef]
- Isikli, C.; Hasirci, V.; Hasirci, N. Development of porous chitosan–gelatin/ hydroxyapatite composite scaffolds for hard tissue-engineering applications. J. Tissue Eng. Regen. Med. 2012, 6, 135–143. [Google Scholar] [CrossRef]
- Salgado, A.J.; Coutinho, O.P.; Reis, R.L. Bone tissue engineering: State of the art and future trends. Macromol. Biosci. 2004, 4, 743–765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhumiratana, S.; Vunjak-Novakovic, G. Concise review: Personalized human bone grafts for reconstructing head and face. Stem Cells Transl. Med. 2012, 1, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Bauer, T.W.; Muschler, G.F. Bone graft materials. An overview of the basic science. Clin. Orthop. Relat. Res. 2000, 371, 10–27. [Google Scholar] [CrossRef]
- Cingolani, A.; Grottoli, C.F.; Esposito, R.; Villa, T.; Rossi, F.; Perale, G. Improving Bovine Bone Mechanical Characteristics for the Development of Xenohybrid Bone Grafts. Curr. Pharm. Biotechnol. 2018, 19, 1005. [Google Scholar] [CrossRef]
- Grottoli, C.; Ferracini, R.; Compagno, M.; Tombolesi, A.; Rampado, O.; Pilone, L.; Bistolfi, A.; Borrè, A.; Cingolani, A.; Perale, G. A Radiological Approach to Evaluate Bone Graft Integration in Reconstructive Surgeries. Appl. Sci. 2019, 9, 1469. [Google Scholar] [CrossRef] [Green Version]
- Facciuto, E.; Grottoli, C.F.; Mattarocci, M.; Illiano, F.; Compagno, M.; Ferrari, R.; Perale, G. Three-Dimensional Craniofacial Bone Reconstruction With SmartBone on Demand. J. Craniofac. Surg. 2019, 30, 739. [Google Scholar] [CrossRef]
- Secondo, F.; Grottoli, C.F.; Zollino, I.; Perale, G.; Lauritano, D. Positioning of a contextual implant along with a sinus lift anchored with a block of heterologous bone. Oral Implantol. (Rome) 2017, 4, 457. [Google Scholar] [CrossRef]
- Stacchi, C.; Lombardi, T.; Ottonelli, R.; Berton, F.; Perinetti, G.; Traini, T. New bone formation after transcrestal sinus floor elevation was influenced by sinus cavity dimensions: A prospective histologic and histomorphometric study. Clin. Oral Implants Res. 2018, 29, 465. [Google Scholar] [CrossRef]
- Mandelli, F.; Perale, G.; Danti, S.; D’Alessandro, D.; Ghensi, P. Clinical and histological evaluation of socket preservation using SmartBone®, a novel heterologous bone substitute: A case series study. Oral Implantol. (Rome) 2018, 11, 87. [Google Scholar]
- Cingolani, A.; Casalini, T.; Caimi, S.; Klaue, A.; Sponchioni, M.; Rossi, F.; Perale, G. A methodologic approach for the selection of bio-resorbable polymers in the development of medical devices: The case of poly (L-lactide-co-ε-caprolactone). Polymers (Basel) 2018, 10, 851. [Google Scholar] [CrossRef] [Green Version]
- Cristalli, M.P.; La Monaca, G.; Pranno, N.; Annibali, S.; Iezzi, G.; Vozza, I. Xeno-Hybrid Composite Scaffold Manufactured with CAD/CAM Technology for Horizontal Bone-Augmentation in Edentulous Atrophic Maxilla: A Short Communication. Appl. Sci. 2020, 10, 2659. [Google Scholar] [CrossRef] [Green Version]
- Abuelnaga, M.; Elbokle, N.; Khashaba, M. Evaluation of custom made xenogenic bone grafts in mandibular alveolar ridge augmentation versus particulate bone graft with titanium mesh. Egypt. J. Oral Maxillof. Surg. 2018, 9, 62–73. [Google Scholar] [CrossRef] [Green Version]
- Albanese, M.; Zotti, F.; Lanaro, L.; Trojan, D.; Paolin, A.; Montagner, G.; Iannielli, A.; Rodella, L.F.; Nocini, P.F. Fresh-frozen homologous bone in sinus lifting: Histological and radiological analysis. Minerva Stomatol. 2019, 68, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Rocha, L.R.S.; Aloise, A.C.; Oliveira, R.M.; Teixeira, M.L.; Pelegrine, A.A.; Macedo, L.G.S. Long-term Retrospective Study of Implants Placed after Sinus Floor Augmentation with Fresh-frozen homologous block. Contemp. Clin. Dent. 2017, 8, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Pecora, G.; Piattelli, M.; Piattelli, A. Osseointegration in a sinus augmented with bovine porous bone mineral: Histological results in an implant retrieved 4 years after insertion. A case report. J. Periodontol. 2004, 75, 1161–1166. [Google Scholar] [CrossRef] [PubMed]












Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Messo, E.; Grottoli, C.F.; Perale, G.; Hirsch, J.-M. Custom-Made Horizontal and Vertical Maxillary Augmentation with Smartbone® On Demand™: A Seven-Year Follow-Up Case. Appl. Sci. 2020, 10, 8039. https://doi.org/10.3390/app10228039
Messo E, Grottoli CF, Perale G, Hirsch J-M. Custom-Made Horizontal and Vertical Maxillary Augmentation with Smartbone® On Demand™: A Seven-Year Follow-Up Case. Applied Sciences. 2020; 10(22):8039. https://doi.org/10.3390/app10228039
Chicago/Turabian StyleMesso, Elias, Carlo F. Grottoli, Giuseppe Perale, and Jan-Michaél Hirsch. 2020. "Custom-Made Horizontal and Vertical Maxillary Augmentation with Smartbone® On Demand™: A Seven-Year Follow-Up Case" Applied Sciences 10, no. 22: 8039. https://doi.org/10.3390/app10228039