Effect of Fiber-Reinforced Composite and Elastic Post on the Fracture Resistance of Premolars with Root Canal Treatment—An In Vitro Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Experimental Procedure
2.3. Restorations Procedure
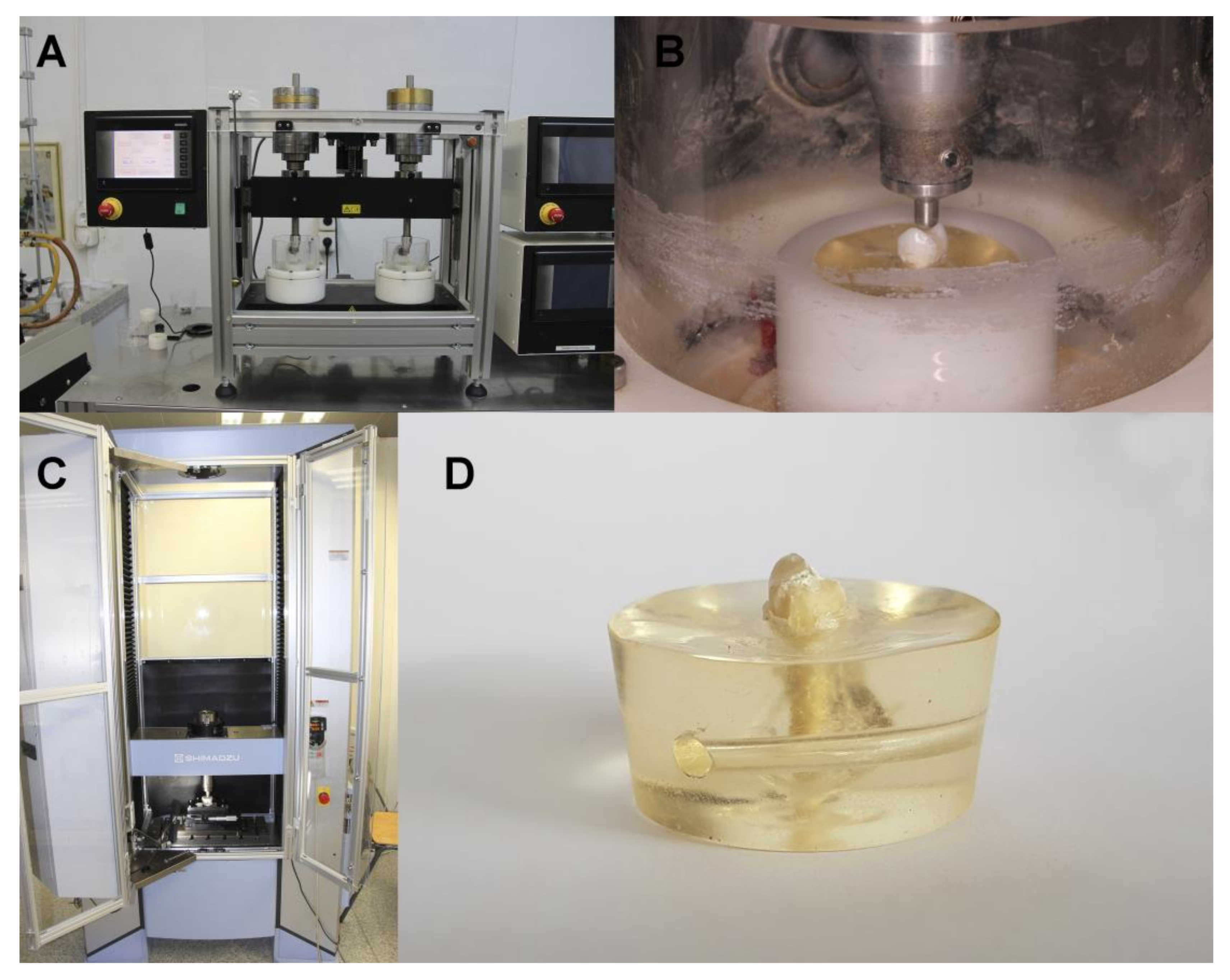
2.4. Thermal and Mechanical Cycling Fatigue
2.5. Fracture Load Test
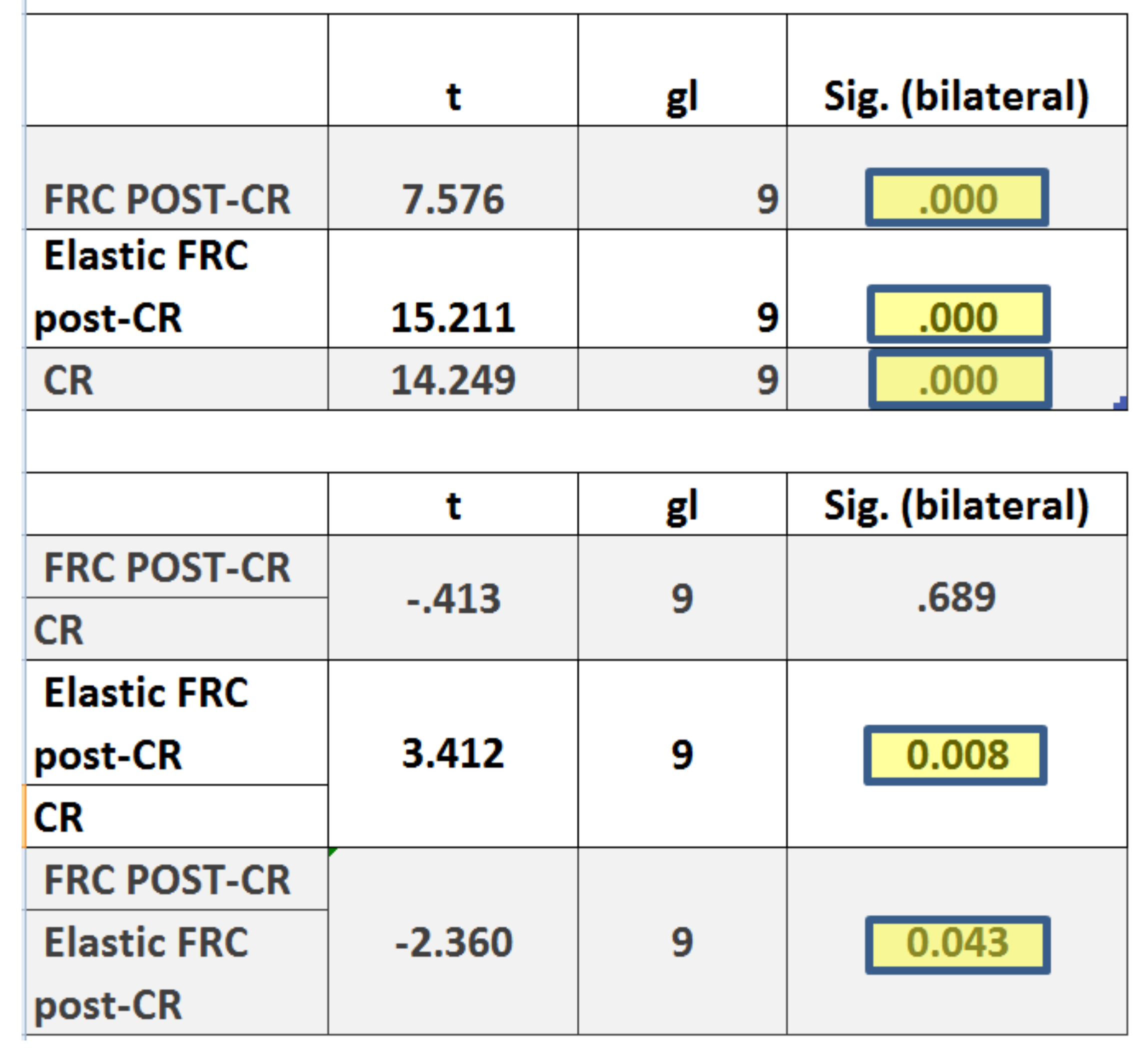
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- -
- The use of elastic FRC post increase the fracture resistance of endodontically treated single-rooted upper first premolar teeth versus FRC post and only CR core. Besides, the restoration using FRC core resin also presents greater resistance to fracture than when they are restored with composite resin (CR).
- -
- The use of fiber-reinforced composites both in the core restoration and inside the root canal can help to reduce the potential risk of fracture associated to endodontically teeth.
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ausiello, P.; Apicella, A.; Davidson, C.; Rengo, S. 3D-finite element analyses of cusp movements in a human upper premolar, restored with adhesive resin-based composites. J. Biomech. 2001, 34, 1269–1277. [Google Scholar] [CrossRef]
- Dietschi, D.; Duc, O.; Krejci, I.; Sadan, A. Biomechanical considerations for the restoration of endodontically treated teeth: A systematic review of the literature—Part 1. Composition and micro- and macrostructure alterations. Quintessence Int. 2007, 38, 733–743. [Google Scholar] [PubMed]
- Goodacre, C.J.; Spolnik, K.J. The Prosthodontic Management of endodontically treated teeth: A literature review. Part I. Success and failure data, treatment concepts. J. Prosthodont. 1994, 3, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Dietschi, D.; Duc, O.; Krejci, I.; Sadan, A. Biomechanical considerations for the restoration of endodontically treated teeth: A systematic review of the literature, Part II (Evaluation of fatigue behavior, interfaces, and in vivo studies). Quintessence Int. 2008, 39, 117–129. [Google Scholar] [PubMed]
- Tamse, A.; Zilburg, I.; Halpern, J. Vertical root fractures in adjacent maxillary premolars: An endodontic-prosthetic perplexity. Int. Endod. J. 1998, 31, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Sorrentino, R.; Monticelli, F.; Goracci, C.; Zarone, F.; Tay, F.R.; García-Godoy, F.; Ferrari, M. Effect of post-retained composite restorations and amount of coronal residual structure on the fracture resistance of endodontically-treated teeth. Am. J. Dent. 2007, 20, 269–274. [Google Scholar] [PubMed]
- Peroz, I.; Blankenstein, F.; Lange, K.-P.; Naumann, M. Restoring endodontically treated teeth with posts and cores—A review. Quintessence Int. 2005, 36, 737–746. [Google Scholar]
- Saritha, M.K.; Paul, U.; Keswani, K.; Jhamb, A.; Mhatre, S.H.; Sahoo, P.K. Comparative evaluation of fracture resistance of different post systems. J. Int. Soc. Prev. Community Dent. 2017, 7, 356–359. [Google Scholar] [CrossRef]
- Da Rocha, D.M.; Tribst, J.P.; Ausiello, P.; Piva, A.M.D.O.D.; Da Rocha, M.C.; Di Nicoló, R.; Borges, A.L.S. Effect of the restorative technique on load-bearing capacity, cusp deflection, and stress distribution of endodontically-treated premolars with MOD restoration. Restor. Dent. Endod. 2019, 44, e33. [Google Scholar] [CrossRef]
- Taha, N.A.; Palamara, J.E.; Messer, H.H. Cuspal deflection, strain and microleakage of endodontically treated premolar teeth restored with direct resin composites. J. Dent. 2009, 37, 724–730. [Google Scholar] [CrossRef]
- Signore, A.; Benedicenti, S.; Covani, U.; Ravera, G. A 4-to 6-year retrospective clinical study of cracked teeth restored with bonded indirect resin composite onlays. Int. J. Prosthodont. 2007, 20, 609–616. [Google Scholar] [CrossRef]
- Pereira, R.; Bicalho, A.; Franco, S.; Tantbirojn, D.; Versluis, A.; Soares, C.J.; Tantbirojin, D. Effect of restorative protocol on cuspal strain and residual stress in endodontically treated molars. Oper. Dent. 2016, 41, 23–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarow, M.; Vadini, M.; Chojnacka-Brozek, A.; Szczeklik, K.; Milewski, G.; Biferi, V.; D’Arcangelo, C.; De Angelis, F. Effect of fiber posts on stress distribution of endodontically treated upper premolars: Finite element analysis. Nanomaterials 2020, 10, 1708. [Google Scholar] [CrossRef] [PubMed]
- Ausiello, P.; Ciaramella, S.; Garcia-Godoy, F.; Martorelli, M.; Sorrentino, R.; Gloria, A. Stress distribution of bulk-fill resin composite in class II restorations. Am. J. Dent. 2017, 30, 227–232. [Google Scholar]
- Mortazavi, V.; Fathi, M.; Katiraei, N.; Shahnaseri, S.; Badrian, H.; Khalighinejad, N. Fracture resistance of structurally compromised and normal endodontically treated teeth restored with different post systems: An in vitro study. Dent. Res. J. 2012, 9, 185–191. [Google Scholar] [CrossRef]
- Gloria, A.; Maietta, S.; Martorelli, M.; Lanzotti, A.; Watts, D.; Ausiello, P. FE analysis of conceptual hybrid composite endodontic post designs in anterior teeth. Dent. Mater. 2018, 34, 1063–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ausiello, P.; Gloria, A.; Maietta, S.; Watts, D.C.; Martorelli, M. Stress distributions for hybrid composite endodontic post designs with and without a ferrule: FEA study. Polymers 2020, 12, 1836. [Google Scholar] [CrossRef]
- Vadavadagi, S.V.; Dhananjaya, K.M.; Yadahalli, R.P.; Lahari, M.; Shetty, S.R.; Bhavana, B. Comparison of different post systems for fracture resistance: An in vitro study. J. Contemp. Dent. Pract. 2017, 18, 205–208. [Google Scholar] [CrossRef] [Green Version]
- Saker, S.; Özcan, M. Retentive strength of fiber-reinforced composite posts with composite resin cores: Effect of remaining coronal structure and root canal dentin conditioning protocols. J. Prosthet. Dent. 2015, 114, 856–861. [Google Scholar] [CrossRef] [Green Version]
- Schneider, S.W. A comparison of canal preparations in straight and curved root canals. Oral Surg. Oral Med. Oral Pathol. 1971, 32, 271–275. [Google Scholar] [CrossRef]
- Fráter, M.; Forster, A.; Jantyik, Á.; Braunitzer, G.; Nagy, K.; Grandini, S. In vitro fracture resistance of premolar teeth restored with fibre-reinforced composite posts using a single or a multi-post technique. Aust. Endod. J. 2017, 43, 16–22. [Google Scholar]
- Pottmaier, L.; Linhares, L.A.; Baratieri, L.; Vieira, L.C. Evaluation of the fracture resistance of premolars with extensive and medium cavity preparations restored with direct restoring systems. Indian J. Dent. Res. 2018, 29, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Nothdurft, F.P.; Seidel, E.; Gebhart, F.; Naumann, M.; Motter, P.; Pospiech, P. The fracture behavior of premolar teeth with class II cavities restored by both direct composite restorations and endodontic post systems. J. Dent. 2008, 36, 444–449. [Google Scholar] [CrossRef] [PubMed]
- Bolay, Ş.; Ozturk, E.; Tuncel, B.; Ertan, A. Fracture resistance of endodontically treated teeth restored with or without post systems. J. Dent. Sci. 2012, 7, 148–153. [Google Scholar] [CrossRef] [Green Version]
- Rocca, G.T.; Saratti, C.M.; Poncet, A.; Feilzer, A.J.; Krejci, I. The influence of FRCs reinforcement on marginal adaptation of CAD/CAM composite resin endocrowns after simulated fatigue loading. Odontology 2016, 104, 220–232. [Google Scholar] [CrossRef]
- Mohammadi, N.; Kahnamoii, M.A.; Yeganeh, P.K.; Navimipour, E.J. Effect of fiber post and cusp coverage on fracture resistance of endodontically treated maxillary premolars directly restored with composite resin. J. Endod. 2009, 35, 1428–1432. [Google Scholar] [CrossRef] [PubMed]
- Xie, K.X.; Wang, X.Y.; Gao, X.J.; Yuan, C.Y.; Li, J.X.; Chu, C.H. Fracture resistance of root filled premolar teeth restored with direct composite resin with or without cuspcoverage. Int. Endod. J. 2012, 45, 524–529. [Google Scholar] [CrossRef]
- Hannig, C.; Westphal, C.; Becker, K.; Attin, T. Fracture resistance of endodontically treated maxillary premolars restored with CAD/CAM ceramic inlays. J. Prosthet. Dent. 2005, 94, 342–349. [Google Scholar] [CrossRef]
- Göktürk, H.; Karaarslan, E.Ş.; Tekin, E.; Hologlu, B.; Sarıkaya, I. The effect of the different restorations on fracture resistance of root-filled premolars. BMC Oral Health 2018, 18, 196. [Google Scholar]
- Moezizadeh, M.; Shokripour, M. Effect of fiber orientation and type of restorative material on fracture strength of the tooth. J. Conserv. Dent. 2011, 14, 341–345. [Google Scholar] [CrossRef] [Green Version]
- Scotti, N.; Forniglia, A.; Tempesta, R.M.; Comba, A.; Saratti, C.M.; Pasqualini, D.; Alovisi, M.; Berutti, E.; Nicola, S.; Alberto, F.; et al. Effects of fiber-glass-reinforced composite restorations on fracture resistance and failure mode of endodontically treated molars. J. Dent. 2016, 53, 82–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scotti, N.; Scansetti, M.; Rota, R.; Pera, F.; Pasqualini, D.; Berutti, E. The effect of the post length and cusp coverage on the cycling and static load of endodontically treated maxillary premolars. Clin. Oral Investig. 2011, 15, 923–929. [Google Scholar] [CrossRef] [PubMed]
- López-Suárez, C.; Castillo-Oyagüe, R.; Rodríguez-Alonso, V.; Lynch, C.D.; Suárez-García, M.-J. Fracture load of metal-ceramic, monolithic, and bi-layered zirconia-based posterior fixed dental prostheses after thermo-mechanical cycling. J. Dent. 2018, 73, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Augstin-Panadero, R.; Fons-Font, A.; Rodríguez, J.L.R.; Granell-Ruiz, M.; Del Rio-Highsmith, J.; Ruiz, M.F.S. Zirconia versus metal: A preliminary comparative analysis of ceramic veneer behavior. Int. J. Prosthodont. 2012, 25, 294–300. [Google Scholar] [PubMed]
- Lopez-Suarez, C.; Tobar, C.; Sola-Ruiz, M.F.; Pelaez, J.; Suarez, M.J. Effect of thermomechanical and static loading on the load to fracture of metal-ceramic, monolithic and veneered zirconia posterior fixed partial dentures. J. Prosthodont. 2019, 28, 171–178. [Google Scholar] [CrossRef]
- Quinn, J.B.; Quinn, G.D. A practical and systematic review of Weibull statistics for reporting strengths of dental materials. Dent. Mater. 2010, 26, 135–147. [Google Scholar] [CrossRef] [Green Version]
- Ausiello, P.; Ciaramella, S.; Martorelli, M.; Lanzotti, A.; Gloria, A.; Watts, D.C. CAD-FE modeling and analysis of class II restorations incorporating resin-composite, glass ionomer and glass ceramic materials. Dent. Mater. 2017, 33, 1456–1465. [Google Scholar] [CrossRef] [Green Version]
- Coelho, C.S.D.M.; Biffi, J.C.G.; Da Silva, G.R.; Abrahão, A.; Campos, R.E.; Soares, C.J. Finite element analysis of weakened roots restored with composite resin and posts. Dent. Mater. J. 2009, 28, 671–678. [Google Scholar] [CrossRef] [Green Version]
- Falakaloğlu, S.; Adıgüzel, Ö.; Özdemir, G. Root canal reconstruction using biological dentin posts: A 3D finite element analysis. J. Dent. Res. Dent. Clin. Dent. Prospect. 2019, 13, 274–280. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | Elastic Modulus |
|---|---|
| (GPa) | |
| Dentin | 14–18.6 |
| Enamel | 80 |
| Periodontal Ligament | 0.05 |
| Compact Bone | 13.8 |
| Medullar Bone | 0.345 |
| Material/Manufacture | Classification | Elastic Modulus (GPa) |
|---|---|---|
| Gradia Core Self-Etching Bond®, GC Europe, Leuven, Belgium | Dual-cure one-step self-etch adhesive system | 4.5 |
| Fiber Post® 0.8 mm, GC Europe, Leuven, Belgium | Conventional glass Fiber Reinforced Composite posts | 24 |
| EverStick Post® 0.9 mm, GC Europe, Leuven, Belgium | Elastic Fiber Reinforced Composite posts | 13–16 |
| Gradia Core®, GC Europe, Leuven, Belgium | Dual-cure Composite Resin core material | 10.8 |
| Everx X Posterior®, GC Europe, Leuven, Belgium | Fiber Reinforced Composite resin lightcured | 14.6 |
| Group | n | Mean | SD | Minimum | Maximum |
|---|---|---|---|---|---|
| Conventional FRC post-CR Core | 10 | 2420 * | 1010 | 1190 | 4010 |
| Elastic FRC post-CR Core | 10 | 3510 | 730 | 2010 | 4230 |
| Conventional FRC post-FRC CR | 10 | 3620 | 470 | 2800 | 4020 |
| Elastic FRC post-FRC CR | 10 | 3520 | 730 | 2070 | 4020 |
| CR Core | 10 | 2560 * | 570 | 1690 | 3400 |
| FRC CR | 10 | 3040 | 1080 | 1310 | 4070 |
| Control: intact teeth without MOD cavity, nor endodontic treatment nor restorations | 10 | 3290 | 830 | 1830 | 4930 |
| m = Weibull Shape (β) | σ0 = Weibull Scale (η) | |||||||
|---|---|---|---|---|---|---|---|---|
| Estimate | St Error | Lower | Upper | Estimate | St Error | Lower | Upper | |
| Conventional FRC Post-CR Core | 27.410 | 0.6686 | 16.992 | 44.213 | 27.270 | 0.3333 | 21.461 | 34.651 |
| Elastic FRC post-CR Core | 70.055 | 19.508 | 40.589 | 120.914 | 37.789 | 0.1774 | 34.468 | 41.431 |
| Conventional FRC Post-FRC CR | 106.744 | 29.247 | 62.390 | 182.628 | 38.129 | 0.1184 | 35.878 | 40.521 |
| Elastic FRC Post-FRC CR | 72.262 | 20.690 | 41.228 | 126.655 | 37.814 | 0.1718 | 34.592 | 41.336 |
| CR Core (Gradia Core) | 56.240 | 14.407 | 34.040 | 92.917 | 27.773 | 0.1645 | 24.729 | 31.191 |
| FRC CR (Ever-X) | 35.211 | 0.9514 | 20.735 | 59.795 | 33.993 | 0.3202 | 28.263 | 40.884 |
| Control | 44.830 | 10.508 | 28.317 | 70.974 | 35.997 | 0.2687 | 31.099 | 41.667 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mena-Álvarez, J.; Agustín-Panadero, R.; Zubizarreta-Macho, A. Effect of Fiber-Reinforced Composite and Elastic Post on the Fracture Resistance of Premolars with Root Canal Treatment—An In Vitro Pilot Study. Appl. Sci. 2020, 10, 7616. https://doi.org/10.3390/app10217616
Mena-Álvarez J, Agustín-Panadero R, Zubizarreta-Macho A. Effect of Fiber-Reinforced Composite and Elastic Post on the Fracture Resistance of Premolars with Root Canal Treatment—An In Vitro Pilot Study. Applied Sciences. 2020; 10(21):7616. https://doi.org/10.3390/app10217616
Chicago/Turabian StyleMena-Álvarez, Jesús, Rubén Agustín-Panadero, and Alvaro Zubizarreta-Macho. 2020. "Effect of Fiber-Reinforced Composite and Elastic Post on the Fracture Resistance of Premolars with Root Canal Treatment—An In Vitro Pilot Study" Applied Sciences 10, no. 21: 7616. https://doi.org/10.3390/app10217616