Patient-Specific Surgical Implant Using Cavity-Filled Approach for Precise and Functional Mandible Reconstruction

 , , , and
, , , and
Abstract
:1. Introduction
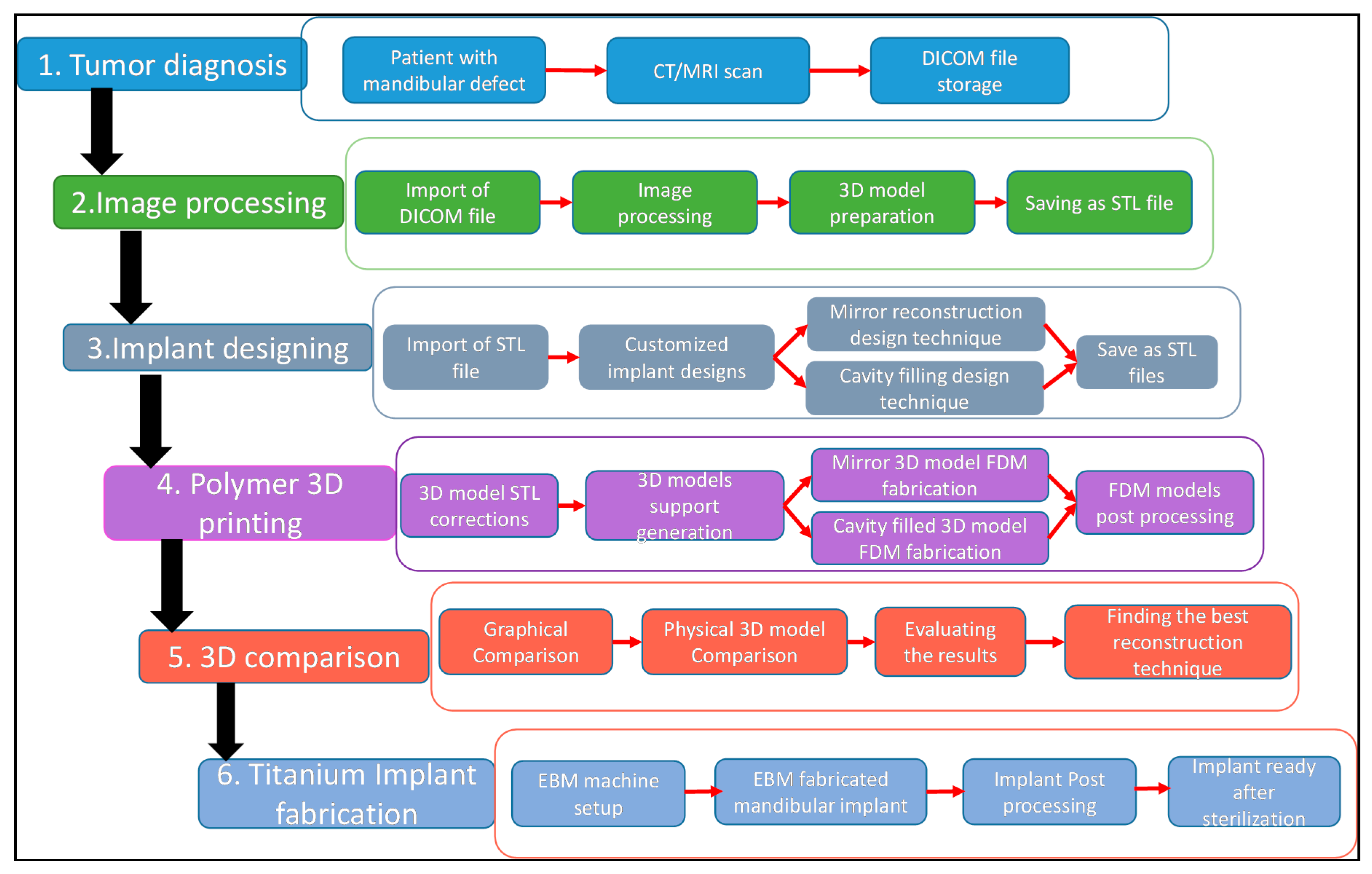
2. Proposed Methodology
2.1. Tumor Diagnosis
2.2. Image Acquisition and Processing
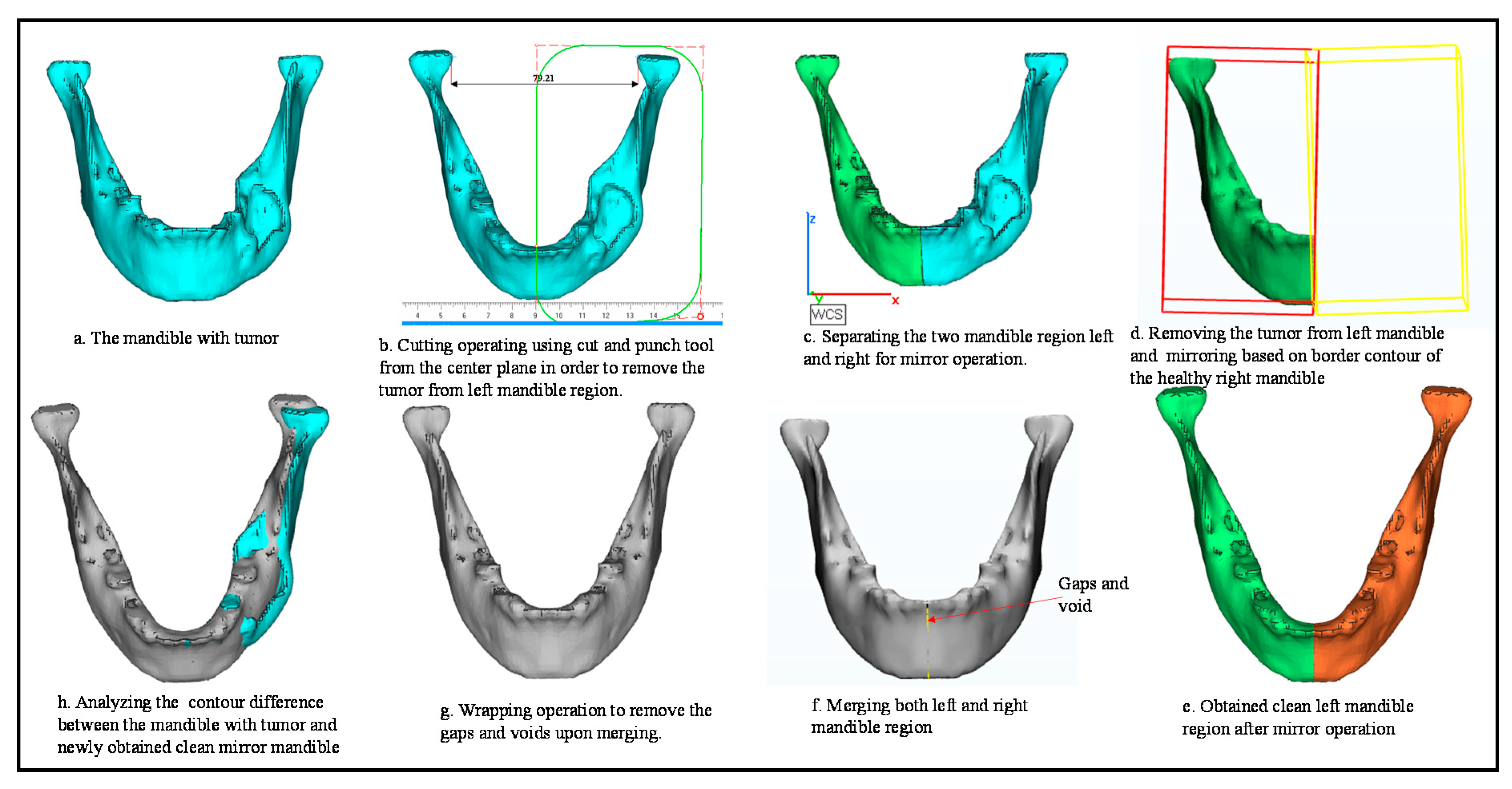
2.3. Custom Implant Design
3. 3D Printing
3.1. STL Corrections and Support Generations
3.2. FDM Fabrication
4. Accuracy Assessment
5. Results
6. EBM Fabrication
7. Discussion
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Statement
References
- Torroni, A.; Marianetti, T.; Romandini, M.; Gasparini, G.; Cervelli, D.; Pelo, S. Mandibular Reconstruction with Different Techniques. J. Craniofacial Surg. 2015, 26, 885–890. [Google Scholar] [CrossRef] [PubMed]
- Kumar, B.P.; Venkatesh, V.; Kumar, K.A.J.; Yadav, B.Y.; Mohan, S.R. Mandibular Reconstruction: Overview. J. Maxillofac. Oral Surg. 2016, 15, 425–441. [Google Scholar] [CrossRef] [PubMed]
- Zeller, A.; Neuhaus, M.T.; Weissbach, L.V.M.; Rana, M.; Dhawan, A.; Eckstein, F.M.; Gellrich, N.C.; Zimmerer, R.M. Patient-Specific Mandibular Reconstruction Plates Increase Accuracy and Long-Term Stability in Immediate Alloplastic Reconstruction of Segmental Mandibular Defects. J. Maxillofac. Oral Surg. 2020. [Google Scholar] [CrossRef]
- Parthasarathy, J. 3D modeling, custom implants and its future perspectives in craniofacial surgery. Ann. Maxillofac. Surg. 2013, 4, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Bowers, C.A.; McMullin, J.H.; Brimley, C.; Etherington, L.; Siddiqi, F.A.; Riva-Cambrin, J. Minimizing bone gaps when using custom pediatric cranial implants is associated with implant success. J. Neurosurg. Pediatrics 2015, 16, 439–444. [Google Scholar] [CrossRef] [Green Version]
- Cassoni, A.; Brauner, E.; Pucci, R.; Terenzi, V.; Mangini, N.; Battisti, A.; Monaca, M.D.; Ciolfi, A.; Laudoni, F.; Di Carlo, S.; et al. Head and Neck Osteosarcoma—The Ongoing Challenge about Reconstruction and Dental Rehabilitation. Cancers 2020, 12, 1948. [Google Scholar] [CrossRef]
- Meyer-Marcotty, P.; Alpers, G.W.; Gerdes, A.B.M.; Stellzig-Eisenhauer, A. Impact of facial asymmetry in visual perception: A 3-dimensional data analysis. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 168.e1–168.e8. [Google Scholar] [CrossRef]
- Metzler, P.; Geiger, E.J.; Alcon, A.; Ma, X.; Steinbacher, D.M. Three-dimensional virtual surgery accuracy for free fibula mandibular reconstruction: Planned versus actual results. J. Oral Maxillofac. Surg. 2014, 72, 2601–2612. [Google Scholar] [CrossRef]
- Alasseri, N.; Alasraj, A. Patient-specific implants for maxillofacial defects: Challenges and solutions. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 15. [Google Scholar] [CrossRef]
- Huotilainen, E.; Jaanimets, R.; Valášek, J.; Marcián, P.; Salmi, M.; Tuomi, J.; Mäkitie, A.; Wolff, J. Inaccuracies in additive manufactured medical skull models caused by the DICOM to STL conversion process. J. Craniomaxillofac. Surg. 2014, 42, e259–e265. [Google Scholar] [CrossRef]
- Davim, J.P. Additive and Subtractive Manufacturing: Emergent Technologies; Walter de Gruyter GmbH & Co KG: Berlin, Germany, 2020. [Google Scholar]
- Boyette, J.R.; Pemberton, J.D.; Bonilla-Velez, J. Management of orbital fractures: Challenges and solutions. Clin. Ophthalmol. 2015, 9, 2127–2137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goormans, F.; Sun, Y.; Bila, M.; Schoenaers, J.; Geusens, J.; Lübbers, h.-t.; Coucke, W.; Politis, C. Accuracy of computer-assisted mandibular reconstructions with free fibula flap: Results of a single-center series. Oral Oncol. 2019, 97, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Lancellotta, V.; Pagano, S.; Tagliaferri, L.; Piergentini, M.; Ricci, A.; Montecchiani, S.; Saldi, S.; Chierchini, S.; Chierchini, S.; Cianetti, S.; et al. Individual 3-dimensional printed mold for treating hard palate carcinoma with brachytherapy: A clinical report. J. Prosthet. Dent. 2019, 121, 690–693. [Google Scholar] [CrossRef] [PubMed]
- Pagano, S.; Moretti, M.; Marsili, R.; Ricci, A.; Barraco, G.; Cianetti, S. Evaluation of the Accuracy of Four Digital Methods by Linear and Volumetric Analysis of Dental Impressions. Materials 2019, 12, 1958. [Google Scholar] [CrossRef] [Green Version]
- Kirke, D.N.; Owen, R.P.; Carrao, V.; Miles, B.A.; Kass, J.I. Using 3D computer planning for complex reconstruction of mandibular defects. Cancers Head Neck 2016, 1, 17. [Google Scholar] [CrossRef] [Green Version]
- Bartier, S.; Mazzaschi, O.; Benichou, L.; Sauvaget, E. Computer-assisted versus traditional technique in fibular free-flap mandibular reconstruction: A CT symmetry study. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2020. [Google Scholar] [CrossRef]
- Mascha, F.; Winter, K.; Pietzka, S.; Heufelder, M.; Schramm, A.; Wilde, F. Accuracy of computer-assisted mandibular reconstructions using patient-specific implants in combination with CAD/CAM fabricated transfer keys. J. Cranio-Maxillofac. Surg. 2017, 45, 1884–1897. [Google Scholar] [CrossRef]
- Yang, W.-F.; Zang, C.-Y.; Choi, W.S.; Zhu, W.-Y.; Li, D.T.S.; Chen, X.-S.; Du, R.; Su, Y.-X. A novel ‘surgeon-dominated’ approach to the design of 3D-printed patient-specific surgical plates in mandibular reconstruction: A proof-of-concept study. Int. J. Oral Maxillofac. Surg. 2020, 49, 13–21. [Google Scholar] [CrossRef]
- Davies, J.C.; Chan, H.H.L.; Jozaghi, Y.; Goldstein, D.P.; Irish, J.C. Analysis of simulated mandibular reconstruction using a segmental mirroring technique. J. Craniomaxillofac. Surg. 2019, 47, 468–472. [Google Scholar] [CrossRef]
- Mahendru, S.; Jain, R.; Aggarwal, A.; Aulakh, H.S.; Jain, A.; Khazanchi, R.K.; Sarin, D. CAD-CAM vs conventional technique for mandibular reconstruction with free fibula flap: A comparison of outcomes. Surg. Oncol. 2020, 34, 284–291. [Google Scholar] [CrossRef]
- Darwich, K.; Ismail, M.B.; Al-Mozaiek, M.Y.A.-S.; Alhelwani, A. Reconstruction of mandible using a computer-designed 3D-printed patient-specific titanium implant: A case report. Oral Maxillofac. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Linares, O.C.; Bianchi, J.; Raveli, D.; Neto, J.B.; Hamann, B. Mandible and skull segmentation in cone beam computed tomography using super-voxels and graph clustering. Vis. Comput. 2019, 35, 1461–1474. [Google Scholar] [CrossRef] [Green Version]
- Qiu, B.; Guo, J.; Kraeima, J.; Glas, H.H.; Borra, R.J.H.; Witjes, M.J.H.; van Ooijen, P.M.A. Automatic segmentation of the mandible from computed tomography scans for 3D virtual surgical planning using the convolutional neural network. Phys. Med. Biol. 2019, 64, 175020. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, A.J.; Parvin, M.; Bashiri, S. Innovative use of a stereolithographic model together with the mirror image technique to reconstruct a defect in mandibular continuity. Br. J. Oral Maxillofac. Surg. 2018, 56, 887–889. [Google Scholar] [CrossRef]
- Lin, H.; Zhu, P.; Lin, Q.; Huang, X.; Xu, Y.; Yang, X. Comprehensive Analysis of Mandibular Residual Asymmetry after Bilateral Sagittal Split Ramus Osteotomy Correction of Menton Point Deviation. PLoS ONE 2016, 11, e0161601. [Google Scholar] [CrossRef]
- Moiduddin, K.; Darwish, S.; Al-Ahmari, A.; ElWatidy, S.; Mohammad, A.; Ameen, W. Structural and mechanical characterization of custom design cranial implant created using additive manufacturing. Electron. J. Biotechnol. 2017, 29, 22–31. [Google Scholar] [CrossRef]
- Hatamleh, M.M.; Bhamrah, G.; Ryba, F.; Mack, G.; Huppa, C. Simultaneous Computer-Aided Design/Computer-Aided Manufacture Bimaxillary Orthognathic Surgery and Mandibular Reconstruction Using Selective-Laser Sintered Titanium Implant. J. Craniofacial Surg. 2016, 27, 1810–1814. [Google Scholar] [CrossRef]
- Scolozzi, P. Maxillofacial reconstruction using polyetheretherketone patient-specific implants by ‘mirroring’ computational planning. Aesthetic Plast. Surg. 2012, 36, 660–665. [Google Scholar] [CrossRef] [Green Version]
- Neyman, J.; Pearson, E.S.; Pearson, K. On the problem of the most efficient tests of statistical hypotheses. Philos. Trans. Royal Soc. Lond. Ser. A 1933, 231, 289–337. [Google Scholar] [CrossRef] [Green Version]
- Giudice, A.L.; Ronsivalle, V.; Grippaudo, C.; Lucchese, A.; Muraglie, S.; Lagraere, M.O.; Isola, G. One Step before 3D Printing—Evaluation of Imaging Software Accuracy for 3-Dimensional Analysis of the Mandible: A Comparative Study Using a Surface-to-Surface Matching Technique. Materials 2020, 13, 2798. [Google Scholar] [CrossRef]
- Mian, S.H.; Mannan, M.A.; Al-Ahmari, A.M. The influence of surface topology on the quality of the point cloud data acquired with laser line scanning probe. Sens. Rev. 2014, 34, 255–265. [Google Scholar] [CrossRef]
- Hague, R.J.M.; Reeves, P.E. Rapid Prototyping, Tooling and Manufacturing; iSmithers Rapra Publishing: Shropshire, UK, 2000. [Google Scholar]
- Material Properties of ABS-Acrylonitrile-Butadlene-Styrene. Dielectric Manufacturing. Available online: https://dielectricmfg.com/knowledge-base/abs/ (accessed on 31 January 2020).
- Oropallo, W.; Piegl, L.A. Ten challenges in 3D printing. Eng. Comput. 2016, 32, 135–148. [Google Scholar] [CrossRef]
- Umer, U.; Ameen, W.; Abidi, M.H.; Moiduddin, K.; Alkhalefah, H.; Alkahtani, M.; Al-Ahmari, A. Modeling the Effect of Different Support Structures in Electron Beam Melting of Titanium Alloy Using Finite Element Models. Metals 2019, 9, 806. [Google Scholar] [CrossRef] [Green Version]
- About Arcam. GE Additive. Available online: https://www.ge.com/additive/who-we-are/about-arcam (accessed on 4 March 2020).
- Calignano, F. Design optimization of supports for overhanging structures in aluminum and titanium alloys by selective laser melting. Mater. Des. 2014, 64, 203–213. [Google Scholar] [CrossRef]
- Martinez-Marquez, D.; Mirnajafizadeh, A.; Carty, C.P.; Stewart, R.A. Application of quality by design for 3D printed bone prostheses and scaffolds. PLoS ONE 2018, 13. [Google Scholar] [CrossRef]
- Adel, E.-N.K.; John, C.K.C.; Jennifer, G.; Takashi, T.; Pieter, J.S. WHO Classification of Head and Neck Tumours, 4th ed.; International Agency for Research on Cancer (IACR): Lyon, France, 2017; Volume 9. [Google Scholar]
- Tekkeşin, M.S.; Wright, J. The World Health Organization Classification of Odontogenic Lesions: A Summary of the Changes of the 2017 (4th) Edition. Turk. J. Pathol. 2013, 34. [Google Scholar] [CrossRef]
- Dunfee, B.L.; Sakai, O.; Pistey, R.; Gohel, A. Radiologic and Pathologic Characteristics of Benign and Malignant Lesions of the Mandible. RadioGraphics 2006, 26, 1751–1768. [Google Scholar] [CrossRef]
- Shah, J. Cancer of the Head and Neck, Mandible Reconstruction. Cancer Head Neck 2013, 19, 355–375. [Google Scholar]
- Essig, H.; Rana, M.; Kokemueller, H.; von See, C.; Ruecker, M.; Tavassol, F.; Gellrich, N.-C. Pre-operative planning for mandibular reconstruction—A full digital planning workflow resulting in a patient specific reconstruction. Head Neck Oncol. 2011, 3, 45. [Google Scholar] [CrossRef] [Green Version]
- Jardini, A.L.; Larosa, M.A.; Filho, R.M.; de Carvalho Zavaglia, C.A.; Bernardes, L.F.; Lambert, C.S.; Calderoni, D.R.; Kharmandayan, P. Cranial reconstruction: 3D biomodel and custom-built implant created using additive manufacturing. J. Cranio-Maxillofac. Surg. 2014, 42, 1877–1884. [Google Scholar] [CrossRef]
- White, T.D.; Folkens, P.A. Chapter 7-SKULL. In The Human Bone Manual; White, T.D., Folkens, P.A., Eds.; Academic Press: San Diego, CA, USA, 2005; pp. 75–126. [Google Scholar]
- Ferrario, V.F.; Sforza, C.; Ciusa, V.; Dellavia, C.; Tartaglia, G.M. The effect of sex and age on facial asymmetry in healthy subjects: A cross-sectional study from adolescence to mid-adulthood. J. Oral Maxillofac. Surg. 2001, 59, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Yáñez-Vico, R.M.; Iglesias-Linares, A.; Torres-Lagares, D.; Gutiérrez-Pérez, J.L.; Solano-Reina, E. Three-dimensional evaluation of craniofacial asymmetry: An analysis using computed tomography. Clin. Oral Investig. 2011, 15, 729–736. [Google Scholar] [CrossRef] [PubMed]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Number | Mode (R-T) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Scanned (Resected)- Scanned (Mirror) | STL (Resected)- STL (Mirror) | Scanned (Resected)- Scanned (Cavity-Filled) | STL (Resected)- STL (Cavity-Filled) | |||||||||
| RMS | Average | RMS | Average | RMS | Average | RMS | Average | |||||
| Negative | Positive | Negative | Positive | Negative | Positive | Negative | Positive | |||||
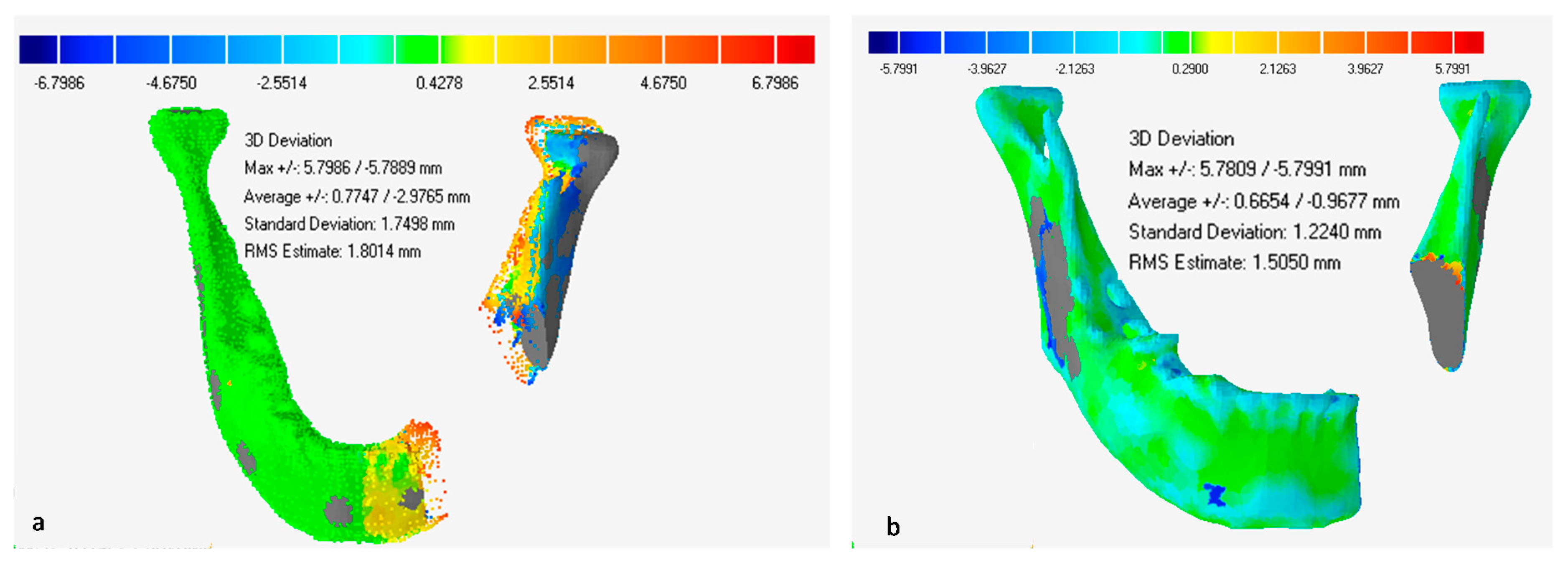
| 1 | 1.2695 | −0.8676 | 0.7432 | 1.8014 | −2.9765 | 0.7747 | 1.1021 | −0.5386 | 0.5192 | 1.5050 | −0.9677 | 0.6654 |
| 2 | 1.2690 | −0.8672 | 0.7434 | 1.8017 | −2.9760 | 0.7753 | 1.1011 | −0.5390 | 0.5198 | 1.5047 | −0.9680 | 0.6650 |
| 3 | 1.2672 | −0.8693 | 0.7432 | 1.8031 | −2.9762 | 0.7730 | 1.1014 | −0.5397 | 0.5196 | 1.5054 | −0.9671 | 0.6655 |
| 4 | 1.2664 | −0.8690 | 0.7424 | 1.8025 | −2.9769 | 0.7742 | 1.1023 | −0.5389 | 0.5193 | 1.5046 | −0.9670 | 0.6652 |
| 5 | 1.2692 | −0.8678 | 0.7483 | 1.8004 | −2.9779 | 0.7758 | 1.1028 | −0.5399 | 0.5190 | 1.5044 | −0.9679 | 0.6649 |
| Mean | 1.2683 | −0.8682 | 0.7441 | 1.8018 | −2.9767 | 0.7746 | 1.1019 | −0.5392 | 0.5194 | 1.5048 | −0.9675 | 0.6652 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moiduddin, K.; Mian, S.H.; Ameen, W.; Alkindi, M.; Ramalingam, S.; Alghamdi, O. Patient-Specific Surgical Implant Using Cavity-Filled Approach for Precise and Functional Mandible Reconstruction. Appl. Sci. 2020, 10, 6030. https://doi.org/10.3390/app10176030
Moiduddin K, Mian SH, Ameen W, Alkindi M, Ramalingam S, Alghamdi O. Patient-Specific Surgical Implant Using Cavity-Filled Approach for Precise and Functional Mandible Reconstruction. Applied Sciences. 2020; 10(17):6030. https://doi.org/10.3390/app10176030
Chicago/Turabian StyleMoiduddin, Khaja, Syed Hammad Mian, Wadea Ameen, Mohammed Alkindi, Sundar Ramalingam, and Osama Alghamdi. 2020. "Patient-Specific Surgical Implant Using Cavity-Filled Approach for Precise and Functional Mandible Reconstruction" Applied Sciences 10, no. 17: 6030. https://doi.org/10.3390/app10176030