1. Introduction
Urine is formed in the kidneys, and it flows through the renal pelvis and the ureter to the bladder with the help of hydrodynamic pressure and peristalsis [
1,
2]. If a focal or segmental lesion develops in the ureter, a urinary disturbance can occur. This disturbance can be relieved through a urinary diversion, such as with a percutaneous nephrostomy using a drainage tube [
3]. Another way to solve the problem is to use ureter stents. Currently, plastic stents made of polyurethane are commonly used along with metallic stents [
4,
5,
6,
7,
8]. A double-J stent is a plastic stent and it consists of a shaft with coils on both ends, with multiple side holes [
9,
10]. It is used in the upper urinary system in cases of ureteral stenosis or occlusion caused by a ureter stone or extrinsic tumor. The placement of a double-J stent in the extrinsic tumor involving the ureter does not guarantee effective urine flow as the tumor compression of the stent often makes fluid drainage outside the stent impossible, and the use of a double-J stent in the tumor can result in stent failure in many cases [
11]. In contrast, the placement of a double-J stent in the case of a ureter stone is effective in maintaining urine flow as urine flow is allowed through and around the stent.
In a clinical setting, the 5-, 6-, 7-, and 8-Fr double-J stents are used for ureter stones before and after lithotripsy. The selection of size depends on the clinician’s experience based on the possible urine flow rate through the stent. Brewer et al. [
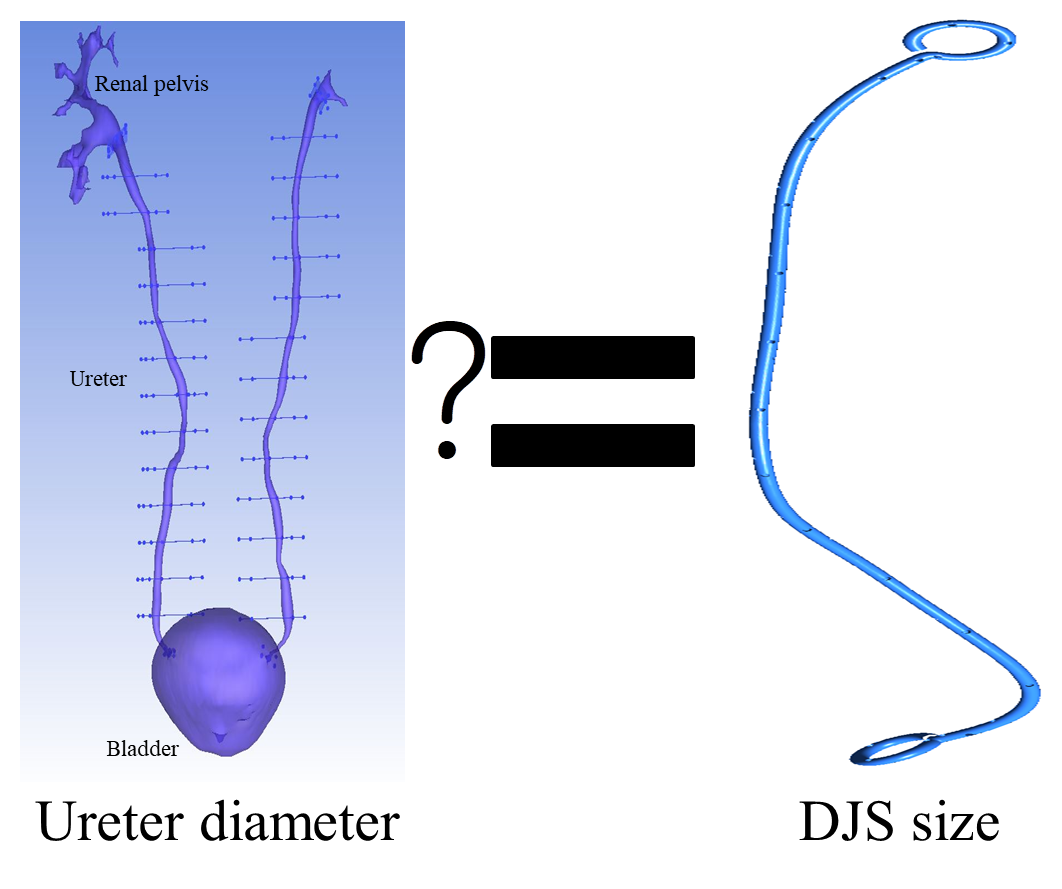
12] reported that luminal flow is directly proportional to the internal diameter of the stent, and extraluminal flow does not correlate with the external diameter of the stent once a 7-Fr size is reached although it is proportional to the external diameter. In this study, we investigated which size of double-J stent is better at achieving an acceptable urine flow through the stented ureter using computational fluid dynamics (CFD) to determine the total flow, the sum of luminal and extraluminal flow. We developed a curved ureter model based on human anatomy [
13]. Sixty-four CFD models of the combinations of two different gauge ureters (4.57-mm diameter and 5.39-mm diameter) with four levels of ureteral stenosis (0%, 33%, 52%, and 74%) and different sizes of double-J stents with different numbers of side holes were used for the numerical analysis of urine flow in stenotic and stented ureters.
2. Materials and Methods
A CFD model for the numerical analysis was composed of a ureter connected to a renal pelvis and a bladder, and a double-J stent (
Figure 1). The ureter was made based on the two-dimensional axial computed tomography image data of human anatomies, including the kidney, ureter, and bladder, of 19 males into 15 equal sections perpendicular to the direction in which the patient was lying (z-axis), as shown in
Figure 1. The beginning and end points of the ureter were separated into the cross-section of the renal pelvis and the ureter and that of the ureter and the bladder.
Figure 1 shows the ureter shape of each section of Patient 1. The area of each separated cross-section was measured to calculate the diameter when the cross-section was assumed to be circular. This method was repeated for 18 additional patients. S. 1-1’ is segment 1-1’. The mean diameter of each section from the 19 patients are shown in
Table 1. The STDEVP function calculated the standard deviation based on the entire population given as arguments [
14]. The standard deviation is a measure of how widely the values are dispersed from the average value. The distance between the center points of each cross-section was measured similarly to the method mentioned above.
Table 2 presents the measured distance for Patient 1. S. 1-2 is the distance between segments 1-1’ and 2-2’. Similarly, measurements were made on the x, y, and z axes between sections of the other 18 patients. According to the measured information, a ureter model was constructed by averaging the data of the ureteral lengths and diameters from the patients. The model was curved and 226.21-mm long, and the proximal end of the ureter was connected to the renal pelvis, which has a conical shape. The distal end of the ureter was connected to the bladder, which has a dome shape. The base of the renal pelvis and the bladder was round and 40 mm in diameter. The height of the renal pelvis and bladder was 15.5 mm. The ureter was tubular and 4.57 mm in diameter. Another ureter model was made with a 5.39-mm ureter diameter in view of the 8-Fr stents. A double-J stent (DJS) model inserted into the ureter using the ureteral data collected from the patients was developed using SolidWorks software (Dassault Systèmes SE, Vélizy-Villacoublay, France) and ICEM CFD software (version 16.2; Ansys, Inc., Canonsburg, PA, USA). The DJS model was based on the Cook Medical stent (Cook Group Inc., Bloomington, IN, USA). This DJS model consists of two coils with a J-shape and a shaft. The shaft has several side holes that provide a flow diversion from the stent to the ureter or vice versa, and the coiled ends have various side holes which play a role in urine flow in and out of the stent in the kidney and the bladder, as shown in
Figure 2.
The DJS model included a shaft in the middle that was as long as the ureter, at 226.21 mm. It had two coils in the ends that were round and 10 mm in diameter. The sizes of the stents were 5, 6, 7, and 8 Fr with inner diameters of 0.67, 1, 1.33, and 1.67 mm, respectively, and outer diameters of 1.67, 2, 2.33, and 2.67 mm, respectively, with multiple side holes in the shaft and coils. The side holes and end holes in the coils were called ports to differentiate them from the side holes in the shaft. Two different types of stents were made, differentiated by the number and position of the side holes in the shaft. The first type was a stent with 22 side holes placed at a 1-cm intervals and at a 90° angular position. The other was a stent with 45 side holes placed at a 0.5-cm intervals and at a 90° angular position. The number of ports in each coil was five, including four side holes and one end hole. The diameter of the side holes and ports, except the end holes, was 1 mm, and the diameter of the end holes in the coils depended on the diameter of the stent.The ureter and the stent were combined, and thus the axis of the ureter was shared with that of the stent, meaning that the ureter and the stent had the same axis. The stent was located in the center of the ureter. A concentric stenosis was made in the middle of the ureter, and it was 15 mm long.
The degrees of stenosis in the ureter were 0%, 33%, 52%, and 74% in area, as shown in
Figure 3.
Stenosis in the ureter can occur not only in the middle position, but anywhere in the narrow diameter of the ureter [
15]. This study assumed the same location and size of stenosis to extend the results of the study to cases in which a previous stenosis occurred, to compare and analyze the effects on the DJS size [
16].
The combination of two different curved tubular ureters (4.57 and 5.39 mm), eight different types of stents (5–8 Fr, each with 22 or 45 side holes), and four different degrees of stenosis in the ureter (0%, 33%, 52%, and 74%) resulted in 64 different stented ureter CFD models for numerical analysis.
Table 3 shows the details of the eight different models in a certain diameter ureter with a certain size of double-J stent. In two models with a 4.57-mm ureter, 8-Fr stent, and 74% stenosis (Cases 7 and 8), no space was found between the inner ureter wall and the outer stent wall.
The mesh generation of the ureter-inserted DJS geometry was conducted using ICEM CFD software. The prism and tetrahedron grid types were used to make the mesh because of the complex shape of the model. The unconstructed grid systems of the ureter-inserted DJS are shown in
Figure 4. The total grid elements and node range of the model were 9.579 × 10
6–13.53 × 10
6 elements and 3.049 × 106–19.52 × 106 nodes, respectively. To check the mesh sensitivity, a mesh independency test was performed for Case 1 (tubular type, 4.57 mm, 5-Fr size, without ureteral stenosis), as shown in
Figure 5.
The governing equations for fluid flow and the boundary conditions for numerical analysis in a previous study [
16] were also used here. The continuity and momentum equations are as follows:
where
ρ,
u,
η, and
p are the density, velocity vector, viscosity, and pressure, respectively. The governing equations were discretized using the finite volume method with CFX 16.2 software (Ansys Inc.) [
17]. The boundary condition and the urine viscosity used in the study were the same as in the previous study [
16]. Urine is considered an incompressible and Newtonian fluid. If urine is stagnant in one place for a long time, its viscosity and physical properties will change [
18]. However, this study focused on urine flow through the DJS and did not consider the change in the physical properties of urine in stagnant situations. Here, we investigated the flow rates and patterns in the urinary system. The flow inside the stent is called the luminal flow, and the flow outside of the stent in the ureter is called the extraluminal flow, as shown in
Figure 6. The total flow rate is the sum of the luminal and extraluminal flow rates. The luminal, extraluminal, and total flow rates along the ureter were measured. In addition, the flow patterns around the ports and side holes, especially in the mid-ureter, were analyzed. In subsequent studies, an in vitro experiment was conducted to verify the validity of the simulation results, and a good match was found [
19].
3. Results
The total flow rate in the 5-Fr double-J stents was 23–63 mL/h in the 4.57-mm ureter and 43–147 mL/h in the 5.39-mm ureter, and in the 6-Fr double-J stents the flow rate was 20–47 mL/h in the 4.57-mm ureter and 36–116 mL/h in the 5.39-mm ureter (
Figure 7). The total flow rate in the 7-Fr double-J stents was 17–35 mL/h in the 4.57-mm ureter and 29–92 mL/h in the 5.39-mm ureter, and in the 8-Fr double-J stents the flow rate was 16–26 mL/h in the 4.57-mm ureter and 26–71 mL/h in the 5.39-mm ureter.
The total flow rate in the stented ureters with 5-Fr double-J stents was greater than that in the stented ureters with the other sizes of double-J stents.
The total flow rate decreased with the increase in the size of the stents. The total flow rate in the stented ureters without any ureteral stenosis was greater than that in the stented ureters with ureteral stenosis. The total flow rate decreased with the increase in the severity of the stenosis. The 4.57-mm ureter with an 8-Fr double-J stent and 74% ureteral stenosis did not exhibit an extraluminal flow rate because of the lack of space between the inner ureter wall and the outer stent wall, that is, the absence of extraluminal space. In this case, the luminal flow rate was the total flow rate. The luminal flow rate around the ureteral stenosis in the mid-ureter was different from that in the proximal and distal ureter (
Figure 8 and
Figure 9).
The luminal flow formed through the fifth port in the renal pelvis and the first side hole in the proximal ureter was maintained in the proximal ureter. The luminal flow rate increased before the stenosis because of the increase in the luminal flow through the side holes before the stenosis. Then, it decreased after the stenosis because of the decrease in the luminal flow through the side holes after the stenosis. However, the luminal flow rate was maintained in the distal ureter.
The luminal flow rate was greater when the size of the stent was larger. When a ureteral stenosis became more severe, the luminal flow rate in the proximal and distal ureter decreased and that in the mid-ureter increased. The luminal flow rate in the 5-Fr double-J stents reached 1.2 mL/h in the 4.57-mm ureter and 1.2 mL/h in the 5.39-mm ureter, and in the 6-Fr double-J stents the flow rate reached 5.9 mL/h in the 4.57-mm ureter and 6.1 mL/h in the 5.39-mm ureter. The luminal flow rate in the 7-Fr double-J stents reached 11.4 mL/h in the 4.57-mm ureter and 14.7 mL/h in the 5.39-mm ureter, and in the 8-Fr double-J stents the flow rate reached 16 mL/h in the 4.57-mm ureter and 24 mL/h in the 5.39-mm ureter.
The extraluminal flow rate was greater than the luminal flow rate in the proximal and distal ureter (
Figure 10 and
Figure 11). In the mid-ureter, the luminal flow rate was greater than the extraluminal flow rate when the ureteral stenosis was 74% and the size of the double-J stent was 8 Fr. However, in the remaining cases, the extraluminal flow rate was greater than the luminal flow rate.
No significant flow into or out of the stent was found except for the first and last side holes in the proximal and distal ureter. The inflow and outflow to the stent were demonstrated before and after the stenosis. Around a ureteral stenosis, the flows into and out of a stent before and after the stenosis were shown.
4. Discussion
A double-J stent is used along with metallic stents in ureteral stenosis or occlusion [
4,
5,
6,
7,
8]. The goal in using a double-J stent is to obtain a route for urine flow and to achieve a sufficient and acceptable urine flow through the stented ureter. The indwelling pigtail ureteral stent has proven its efficacy in maintaining ureteral patency in many cases, and it is widely used as an adjunct to extracorporeal shock wave lithotripsy. Here, we limited the study to cases of ureter stones. Although malignant ureteral obstruction is treated with a double-J stent, the patency rate has been poor [
20].
Normal urine flow through the ureter is formed with the help of peristalsis and hydrodynamic forces [
1,
2]. Peristalsis occurs about five to six times per minute in a normal condition, but it is affected by physical changes in the ureter or by the placement of a double-J stent. Initially, peristalsis can be activated to overcome a limited urine output to the bladder, but as time goes on, the frequency of peristalsis may lessen and finally zero-out [
21,
22,
23]. This condition is a great obstacle in maintaining urine flow through the ureter.
The critical evaluation for the clinical application of a double-J stent should be whether the stent could get a sufficient and acceptable urine flow through a stented ureter and which stent size is the best in achieving this. No fluid dynamics studies have been conducted yet on the proper size in the application of a double-J stent.
There is a question of whether we could achieve a sufficient urine flow through a stented ureter with only a luminal flow. The peak values of the luminal flow rates in this study were 16 mL/h and 24 mL/h in the 4.57 mm and 5.39 mm ureters, respectively, obtained with a 74% ureteral stenosis and an 8-Fr double-J stent. The urine output over 24 h was 384 mL and 576 mL with the peak flow values, which were not sufficient or acceptable urine flows in normal daily living. Achieving the goal in the clinical application of a double-J stent is difficult with only a luminal flow.
The extraluminal flow was greater than the luminal flow in mild ureteral stenosis, and it was devoted to the total flow rate even in severe stenosis, in which the luminal flow rate was greater than the extraluminal flow. In severe ureteral stenosis, achieving a sufficient and acceptable total urine flow is difficult with a high luminal flow and a low extraluminal flow. The total flow rate in the 4.57-mm ureter with a 74% ureteral stenosis was 16–23 mL/h and in the 5.39-mm ureter with 74% ureteral stenosis the flow rate was 26–43 mL/h. The urine output over 24 h was 384–552 mL and 624–1032 mL. Achieving a sufficient urine flow through a stented ureter in severe ureteral stenosis is not easy.
In mild ureteral stenosis or no stenosis, achieving a sufficient and acceptable urine flow was relatively easy through a stented ureter, especially with a smaller-sized double-J stent. In the 4.57-mm ureter, the peak total flow rates with 5-, 6-, 7-, and 8-Fr double-J stents were 63, 47, 35, and 26 mL/h, respectively, and the urine output totals over 24 h were 1512, 1128, 840, and 624 mL, respectively. In the 5.39-mm ureter, the peak total flow rates with 5-, 6-, 7-, and 8-Fr double-J stents were 147, 116, 92, and 71 mL/h, respectively, and the urine output totals over 24 h were 3528, 2784, 2208, and 1704 mL, respectively.
Brewer et al. [
12] reported correlation between inner and outer diameters of the ureter stent and urine flow in the stented ureter in an in vivo study. Our study showed similar results, direct proportion, in luminal flow, but partially different results, inverse proportion, in extraluminal flow. In their study, the stent smaller than or equal to 7 Fr showed a direct proportion and the stent bigger than 7 Fr showed an inverse proportion. Our study supports their study findings regarding a decrease in extraluminal flow with bigger ureteral stents.
Ramsay et al. [
24] examined the effects of a double-J stent on an unobstructed ureter and found that the practical in vitro flow capabilities of stents did not seem to theoretically apply in vivo due to increased urine flow around the stent secondary to dilatation of the ureteral lumen in response to the stent and that the stenting could limit urinary drainage. This result means that the double-J stent itself could be one of the obstacles causing insufficient urinary drainage, even though the stent is widely used for relieving disturbances in urinary drainage due to a ureteral stenosis.
Here, we performed the simulation with solid ureter and solid stent models differently from that of the human body. This study also has some limitations. First, we did not consider peristalsis or passive ureteral dilatation in the CFD analysis and thus did not perform the fluid structure interaction (FSI) simulation. Second, the tubular ureter model used in the study had a discrepancy with an uneven or undulated ureter in humans. Third, the results could be different if there had been more than a single site of stenosis. Further studies using the FSI simulation or an undilated ureter model based on the human anatomy could elaborate on the current study. Moreover, in vitro or in vivo studies could help to verify the findings of this study.















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}