
The Influence of Emotional Intelligence on Quality of Life in Patients Undergoing Chronic Hemodialysis Focused on Age and Gender
 and
and
Abstract
:1. Introduction
1.1. Chronic Kidney Disease and Its Impact
1.2. Emotional Intelligence
1.3. Quality of Life in Patients Undergoing Chronic Hemodialysis Therapy
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Data Collection
2.4. Variables
2.5. Instruments
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
3.1. Study Sample Characteristics
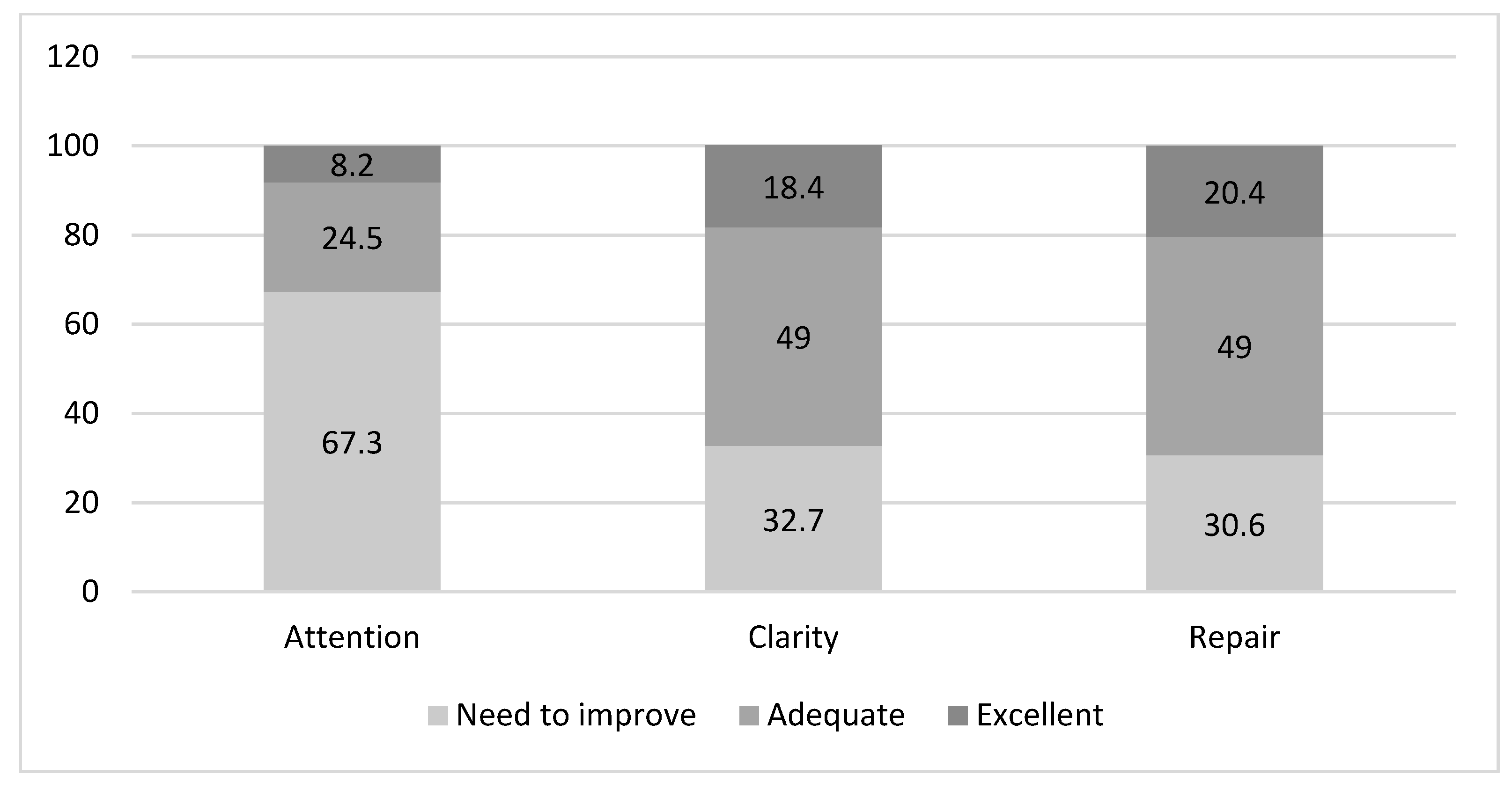
3.2. Emotional Intelligence in Chronic Hemodialysis Patients
3.3. Quality of Life in Chronic Hemodialysis Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HD | hemodialysis |
| TMMS-24 | Trait meta-mood scale |
| KDQOL-SF | kidney disease quality of life—short form questionnaire |
| CDK | chronic kidney disease |
| QL | quality of life |
| EI | emotional intelligence |
| SPSS | Statistical Package for Social Sciences |
| IBM | international business machines corporation |
| IQR | inter quartile range |
| COPD | chronic obstructive pulmonary disease |
References
- Lv, J.C.; Zhang, L.X. Prevalence and Disease Burden of Chronic Kidney Disease. In Renal Fibrosis: Mechanisms and Therapies Advances in Experimental Medicine and Biology; Liu, B.C., Ed.; Springer: Singapore, 2019; pp. 3–15. [Google Scholar]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D.R. Global Prevalence of Chronic Kidney Disease—A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed]
- Eckardt, K.U.; Coresh, J.; Devuyst, O.; Johnson, R.J.; Köttgen, A.; Levey, A.S.; Levin, A. Evolving importance of kidney disease: From subspecialty to global health burden. Lancet 2013, 382, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Thomas, B.; Wulf, S.; Bikbov, B.; Perico, N.; Cortinovis, M.; de Vaccaro, K.C.; Flaxman, A.; Peterson, H.; Delossantos, A.; Haring, D.; et al. Maintenance Dialysis throughout the World in Years 1990 and 2010. J. Am. Soc. Nephrol. 2015, 26, 2621–2633. [Google Scholar] [CrossRef] [PubMed]
- Liyanage, T.; Ninomiya, T.; Jha, V.; Neal, B.; Patrice, H.M.; Okpechi, I.; Zhao, M.-H.; Lv, J.; Garg, A.X.; Knight, J.; et al. World-wide access to treatment for end-stage kidney disease: A systematic review. Lancet 2015, 385, 1975–1982. [Google Scholar] [CrossRef] [PubMed]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, regional, and national burden of chronic kid-ney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef]
- Lee, T.; Flythe, J.E.; Allon, M. Dialysis Care around the World: A Global Perspectives Series. Kidney360 2021, 2, 604–607. [Google Scholar] [CrossRef]
- Pabón-Varela, Y.; Paez-Hernandez, K.S.; Rodriguez-Daza, K.D.; Medina-Atencia, C.E.; López-Tavera, M.; Salcedo-Quintero, L.V. Calidad de vida del adulto con insuficiencia renal crónica, una mirada bibliográfica. Duazary 2015, 12, 157. Available online: https://revistas.unimagdalena.edu.co/index.php/duazary/article/view/1473/922 (accessed on 18 December 2020). [CrossRef]
- Fleishman, T.T.; Dreiher, J.; Shvartzman, P. Pain in Maintenance Hemodialysis Patients: A Multicenter Study. J. Pain. Symptom Manag. 2018, 56, 178–184. [Google Scholar] [CrossRef]
- Grams, M.E.; Yang, W.; Rebholz, C.M.; Wang, X.; Porter, A.C.; Inker, L.A.; Horwitz, E.; Sondheimer, J.H.; Hamm, L.L.; He, J.; et al. Risks of Adverse Events in Advanced CKD: The Chronic Renal Insufficiency Cohort (CRIC) Study. Am. J. Kidney Dis. 2017, 70, 337–346. [Google Scholar] [CrossRef]
- Perl, J.; Karaboyas, A.; Morgenstern, H.; Sen, A.; Rayner, H.C.; Vanholder, R.C.; Combe, C.; Hasegawa, T.; Finkelstein, F.O.; Lopes, A.A.; et al. Association between changes in quality of life and mortality in hemodialysis patients: Results from the DOPPS. Nephrol. Dial. Transplant. 2017, 32, 521–527. Available online: https://academic.oup.com/ndt/article/32/3/521/3060597 (accessed on 23 December 2020). [CrossRef] [PubMed]
- Fernández-Berrocal, P.; Extremera, N. Emotional intelligence: A theoretical and empirical review of its first 15 years of history. Psycothema 2006, 18, 7–12. [Google Scholar]
- O’Connor, P.J.; Hill, A.; Kaya, M.; Martin, B. The Measurement of Emotional Intelligence: A Critical Review of the Literature and Recommendations for Researchers and Practitioners. Front. Psychol. 2019, 10, 1116. [Google Scholar] [CrossRef] [PubMed]
- Salovey, P.; Mayer, J.D.; Goldman, S.; Turvey, C.; Palfai, T.P. Emotional attention, clarity and repair: Exploring emotional intelligence using the Trait Meta-Mood Scale. In Emotion, Disclosure, and Health; Pennebaker, J.W., Ed.; American Psychology Association: Washington, DC, USA, 1995; pp. 125–154. [Google Scholar]
- Mayer, J.D.; Salovey, P.; Caruso, D. Models of emotional intelligence. In Handbook of Intelligence; R. J. S. Cambridge University Press: Cambridge, UK, 2000; pp. 396–420. [Google Scholar]
- Guil, R.; Ruiz-González, P.; Merchán-Clavellino, A.; Morales-Sánchez, L.; Zayas, A.; Gómez-Molinero, R. Breast Cancer and Resil-ience: The Controversial Role of Perceived Emotional Intelligence. Front. Psychol. 2020, 11, 595713. [Google Scholar] [CrossRef] [PubMed]
- Caruso, D.R.; Mayer, J.D.; Bryan, V.; Phillips, K.G.; Salovey, P. Measuring emotional and personal intelligence. In Positive Psychological Assessment: A Handbook of Models and Measures; Gallagher, M.W., Lopez, S.J., Eds.; American Psychological Association: Washington, DC, USA, 2019; pp. 233–245. [Google Scholar]
- Sarrionandia, A.; Mikolajczak, M. A meta-analysis of the possible behavioural and biological variables linking trait emotional intelligence to health. Health Psychol. Rev. 2019, 14, 220–244. [Google Scholar] [CrossRef] [PubMed]
- Moradi, F.; Tourani, S.; Ziapour, A.; Abbas, J.; Hematti, M.; Moghadam, E.J.; Aghili, A.; Soroush, A. Emotional Intelligence and Quality of Life in El-derly Diabetic Patients. Int. Q. Community Health Educ. 2021, 42, 15–20. [Google Scholar] [CrossRef]
- Martins, A.; Ramalho, N.; Morin, E. A comprehensive meta-analysis of the relationship between Emotional Intelligence and health. Pers. Individ. Differ. 2010, 49, 554–564. [Google Scholar] [CrossRef]
- Kret, M.; De Gelder, B. A review on sex differences in processing emotional signals. Neuropsychologia 2012, 50, 1211–1221. [Google Scholar] [CrossRef]
- Hines, M. Neuroscience and Sex/Gender: Looking Back and Forward. J. Neurosci. 2020, 40, 37–43. [Google Scholar] [CrossRef]
- Joel, D.; Berman, Z.; Tavor, I.; Wexler, N.; Gaber, O.; Stein, Y.; Shefi, N.; Pool, J.; Urchs, S.; Margulies, D.S.; et al. Sex beyond the genitalia: The human brain mosaic. Proc. Natl. Acad. Sci. USA 2015, 112, 15468–15473. [Google Scholar] [CrossRef]
- Shahnavazi, M.; Yekta, Z.P.; Rigi, F.; Yekaninejad, M.S. The Relationship between Emotional Intelligence and Quality of life among University Teachers. Int. J. Med. Res. Health Sci. 2016, 5, 564–570. [Google Scholar]
- Shahnavazi, M.; Parsa-Yekta, Z.; Yekaninejad, M.S.; Amaniyan, S.; Griffiths, P.; Vaismoradi, M. The effect of the emotional intelli-gence education programme on quality of life in haemodialysis patients. Appl. Nurs. Res. 2018, 39, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Jesus, N.M.; Souza, G.F.D.; Mendes-Rodrigues, C.; Almeida, O.P.D.; Rodrigues, D.D.M.; Cunha, C.M. Quality of life of individ-uals with chronic kidney disease on dialysis. J. Bras. Nefrol. 2019, 41, 364–374. [Google Scholar] [CrossRef] [PubMed]
- The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Jassal, S.V.; Karaboyas, A.; Comment, L.A.; Bieber, B.A.; Morgenstern, H.; Sen, A.; Gillespie, B.W.; De Sequera, P.; Marshall, M.R.; Fukuhara, S.; et al. Functional Dependence and Mortality in the International Dialysis Outcomes and Practice Patterns Study (DOPPS). Am. J. Kidney Dis. 2016, 67, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Perales-Montilla, C.M.; Duschek, S.; Reyes-del Paso, G.A. Influencia de los factores emocionales sobre el informe de síntomas somáticos en pacientes en hemodiálisis crónica: Relevancia de la ansiedad. Nefrologia 2013, 33, 816–825. [Google Scholar] [PubMed]
- Palmer, S.; Vecchio, M.; Craig, J.C.; Tonelli, M.; Johnson, D.W.; Nicolucci, A.; Pellegrini, F.; Saglimbene, V.; Logroscino, G.; Fishbane, S.; et al. Prevalence of depression in chronic kidney disease: Systematic review and meta-analysis of observational studies. Kidney Int. 2013, 84, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, K.L. Patient Experience Assessment is a Requisite for Quality Evaluation: A Discussion of the In-Center Hemo-dialysis Consumer Assessment of Health Care Providers and Systems (ICH CAHPS) Survey. Semin. Dial. 2016, 29, 135–143. [Google Scholar] [CrossRef]
- Kliger, A.S. Quality measures for dialysis: Time for a balanced scorecard. Clin. J. Am. Soc. Nephrol. 2016, 11, 363–368. [Google Scholar] [CrossRef]
- Chuasuwan, A.; Pooripussarakul, S.; Thakkinstian, A.; Ingsathit, A.; Pattanaprateep, O. Comparisons of quality of life between patients underwent peritoneal dialysis and hemodialysis: A systematic review and meta-analysis. Health Qual. Life Outcomes 2020, 18, 191. [Google Scholar] [CrossRef]
- Watson, R. Quantitative Research|Western Sydney University ResearchDirect. Nurs. Stand. 2015, 29, 44–48. Available online: https://researchdirect.westernsydney.edu.au/islandora/object/uws:34764 (accessed on 23 December 2020). [CrossRef] [PubMed]
- Fernández-Berrocal, P.; Extremera, N.; Ramos, N. Validity and reliability of the Spanish modified version of the Traït Me-ta-Mood Scale. Psychol Rep. 2004, 94, 751–755. [Google Scholar] [CrossRef] [PubMed]
- Angulo, R.; Albarracín, A.P. Validez y Confiabilidad de la Escala Rasgo de Metaconocimiento Emocional (TMMS-24) en Pro-fesores Universitarios. Rev. Lebret. 2018, 10, 61–72. Available online: http://revistas.ustabuca.edu.co/index.php/LEBRET/article/view/2197/1684 (accessed on 23 December 2020).
- Hays, R.D.; Kallich, J.D.; Mapes, D.L.; Coons, S.J.; Carter, W.B. Development of the kidney disease quality of life (KDQOL) instrument. Qual Life Res. 1994, 3, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.; Prieto, L.A.J. La versión española del SF-36 Health Survey (Cuestionario de Salud SF-36): Un instrumento para la medida de los resultados clínicos [The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): An in-strument for measuring clinical resu. Med. Clin. 1995, 104, 771–776. [Google Scholar]
- Hays, R.D.; Kallich, J.D.; Mapes, D.L.; Coons, S.J.; Naseem, A.; Carter, W. Kidney Disease Quality of Life Short Forma (KDQOL-SFtm), version 1.3. A Manual for Use and Scoring; RAND: Santa Monica, CA, USA, 1997. [Google Scholar]
- Pabon-Varela, Y.; Saray Paez-Hernandez, K.; Dayanna Rodriguez-Daza, K.; Eustralia Medina-Atencia, C.; Lopez-Tavera, M.; Vanessa Salcedo-Quintero, L. Adult’s life quality with chronic kidney disease, a bibliographic view. Rev. Duazary. 2015, 12, 7. [Google Scholar]
- Joseph, D.L.; Newman, D.A. Emotional Intelligence: An Integrative Meta-Analysis and Cascading Model. J. Appl. Psychol. 2010, 95, 54–78. [Google Scholar] [CrossRef] [PubMed]
- Milivojevic, V.; Sinha, R.; Morgan, P.T.; Sofuoglu, M.; Fox, H.C. Effects of endogenous and exogenous progesterone on emo-tional intelligence in cocaine-dependent men and women who also abuse alcohol. Hum. Psychopharmacol. Clin. Exp. 2014, 29, 589–598. [Google Scholar] [CrossRef]
- Pardeller, S.; Frajo-Apor, B.; Kemmler, G.; Hofer, A. Emotional Intelligence and cognitive abilities—Associations and sex differ-ences. Psychol. Health Med. 2018, 22, 1001–1010. [Google Scholar] [CrossRef]
- MacCann, C.; Joseph, D.L.; Newman, D.A.; Roberts, R.D. Emotional intelligence is a second-stratum factor of intelligence: Evidence from hierarchical and bifactor models. Emotion 2014, 14, 358–374. [Google Scholar] [CrossRef]
- Fischer, A.H.; Kret, M.E.; Broekens, J. Gender differences in emotion perception and self-reported emotional intelligence: A test of the emotion sensitivity hypothesis. PLoS ONE 2021, 13, e0190712. [Google Scholar] [CrossRef]
- Guil, R.; Gómez-Molinero, R.; Merchán-Clavellino, A.; Gil-Olarte, P. Lights and Shadows of Trait Emotional Intelligence: Its Mediating Role in the Relationship Between Negative Affect and State Anxiety in University Students. Front. Psychol. 2021, 11, 615010. [Google Scholar] [CrossRef] [PubMed]
- Mcguire, C.L. Preparing Future Healthcare Professionals: The Relationship Between Resilience Emotional Intelligence, and Age. Ph.D. Thesis, Abilene Christian University, Abilene, TX, USA, 2021. [Google Scholar]
- Abbasabad Arabi, H.; Bastani, F.; Navab, E.; Haghani, H. Investigating quality of life and its relationship with emotional intelligence (EQ) in elderly with diabetes. Iran. J. Psychiatry Clin. Psychol. 2015, 21, 215–224. [Google Scholar]
- Ghasemi, F.; Yarahmadi, F.; Forooghi, S. The effects of emotional intelligence training on anxiety in hemodialysis patients. J. Nurs. Midwifery Sci. 2015, 2, 8. [Google Scholar] [CrossRef]
- Mokhatri-Hesari, P.; Montazeri, A. Health-related quality of life in breast cancer patients: Review of reviews from 2008 to 2018. Health Qual Life Outcomes 2020, 18, 338. [Google Scholar] [CrossRef] [PubMed]
- Muflih, S.; Alzoubi, K.H.; Al-Azzam, S.; Al-Husein, B. Depression symptoms and quality of life in patients receiving renal replacement therapy in Jordan: A cross-sectional study. Ann. Med. Surg. 2021, 66, 102384. [Google Scholar] [CrossRef] [PubMed]
- Yapa, H.E.; Purtell, L.; Chambers, S.; Bonner, A. The Relationship Between Chronic Kidney Disease, Symptoms and Health-Related Quality of Life: A Systematic Review. J. Ren. Care 2020, 46, 74–84. [Google Scholar] [CrossRef] [PubMed]
- National Kidney Foundation. KDOQI clinical practice guideline for hemodialysis adequacy: 2015 update. Am. J. Kidney Dis. 2015, 66, 884–930. [Google Scholar] [CrossRef]
- Yalcin, B.M.; Karahan, T.F.; Ozcelik, M.; Igde, F.A. The Effects of an Emotional Intelligence Program on the Quality of Life and Well-Being of Patients with Type 2 Diabetes Mellitus. Diabetes Educ. 2008, 34, 1013–1024. [Google Scholar] [CrossRef]
- Baudry, A.-S.; Lelorain, S.; Mahieuxe, M.; Christophe, V. Impact of emotional competence on supportive care needs, anxiety and depression symptoms of cancer patients: A multiple mediation model. Support. Care Cancer 2018, 26, 223–230. [Google Scholar] [CrossRef]
- Benzo, R.P.; Kirsch, J.L.; Dulohery, M.M.; Abascal-Bolado, B. Emotional Intelligence: A Novel Outcome Associated with Wellbeing and Self-Management in Chronic Obstructive Pulmonary Disease. Ann. Am. Thorac. Soc. 2016, 13, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Chazot, C. Sustainability and environmental impact of on-line hemodiafiltration. Semin. Dial. 2022, 35, 446–448. [Google Scholar] [CrossRef]
- Blankestijn, P.J.; Bruchfeld, A.; Cozzolino, M.; Fliser, D.; Fouque, D.; Gansevoort, R.; Goumenos, D.; A Massy, Z.; Rychlık, I.; Soler, M.J.; et al. Nephrology: Achieving sustainability. Nephrol. Dial. Transplant. 2020, 35, 2030–2033. [Google Scholar] [CrossRef] [PubMed]
- Dinescu, A. Advance Care Planning. Clin. Geriatr. Med. 2021, 37, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.; Haywood, K.; Fitzpatrick, R. Impact of patient-reported outcome measures on routine practice: A structured review. J. Evaluation Clin. Pr. 2006, 12, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Rubio, R.; Palacios, B.; Varela, L.; Fernández, R.; Correa, S.C.; Estupiñan, M.F.; Calvo, E.; José, N.; Muñoz, M.R.; Yun, S.; et al. Quality of life and disease experience in patients with heart failure with reduced ejection fraction in Spain: A mixed-methods study. BMJ Open 2021, 11, e053216. [Google Scholar] [CrossRef]
- Churruca, K.; Pomare, C.; Ellis, L.A.; Long, J.C.; Henderson, S.B.; Murphy, L.E.D.; Leahy, C.J.; Braithwaite, J. Patient-reported outcome measures (PROMs): A review of generic and condition-specific measures and a discussion of trends and issues. Health Expect. 2021, 24, 1015–1024. [Google Scholar] [CrossRef]
- Delhom, I.; Satorres, E.; Meléndez, J.C. Emotional intelligence intervention in older adults to improve adaptation and reduce negative mood. Int. Psychogeriatr. 2022, 34, 79–89. [Google Scholar] [CrossRef]
- Varo, C.; Amoretti, S.; Sparacino, G.; Jiménez, E.; Solé, B.; Bonnin, C.D.M.; Montejo, L.; Serra, M.; Torrent, C.; Salagre, E.; et al. Emotional intelligence: A comparison between patients after first episode mania and those suffering from chronic bipolar disorder type I. Psychol. Med. 2023, 53, 3065–3076. [Google Scholar] [CrossRef]
- Teques, A.P.; Carrera, G.B.; Ribeiro, J.P.; Teques, P.; Ramón, G.L. The importance of emotional intelligence and meaning in life in psycho-oncology. Psycho Oncol. 2016, 25, 324–331. [Google Scholar] [CrossRef]
- Pérez-Fernández, A.; Fernández-Berrocal, P.; Gutiérrez-Cobo, M.J. The Relationship Between Emotional Intelligence and Dia-betes Management: A Systematic Review. Front Psychol. 2021, 12, 754362. [Google Scholar] [CrossRef]
- Ashby, D.; Borman, N.; Burton, J.; Corbett, R.; Davenport, A.; Farrington, K.; Flowers, K.; Fotheringham, J.; Andrea Fox, R.N.; Franklin, G.; et al. Renal Association Clinical Practice Guideline on Haemodialysis. BMC Nephrol. 2019, 20, 379. [Google Scholar] [CrossRef]
- Coelho, J.; Sampaio, F.; Teixeira, S.; Parola, V.; Sequeira, C.; Fortuño, M.L.; Merino, J.R. A relação de ajuda como intervenção de enfermagem: Uma scoping review. Rev. Port. Enferm. Saúde Ment. 2020, 23, 63–72. [Google Scholar] [CrossRef]
- Kidney Disease Improving Global Outcomes (KDIGO) Guideline. Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. Suppl. 2013, 1, 1–150. [Google Scholar]



{kind=link}
{kind=link}
| Global n: 138 | Men n: 89 | Women n: 49 | p | |
|---|---|---|---|---|
| Age (SD) | 65.2 (15.5) | 65.2 (15) | 65.3 (16.4) | 0.964 |
| Education level | ||||
| Primary Secondary University | 106 (76.8) 25 (18.1) 7 (5.1) | 67 (75.3) 17 (19.1) 5 (5.6) | 39 (79.6) 8 (16.3) 2 (4.1) | 0.836 |
| Living situation | ||||
| Alone With family Nursing home | 18 (13) 118 (85.6) 2 (1.4) | 8 (9) 80 (90) 1 (1) | 10 (20.4) 38 (77.6) 1 (2) | 0.142 |
| Clinical characteristics | ||||
| Pain (Visual Analogue scale) | 3.6 (3) | 3.1 (2.9) | 4.4 (3.1) | 0.015 |
| Hemodialysis time (months) | 55.2 (56.5) | 54.4 (60.7) | 56.5 (48.5) | 0.831 |
| Male | Female | |||
|---|---|---|---|---|
| Mean (Standard Deviation) | Median (Interquartile) | Mean (Standard Deviation) | Median (Interquartile) | |
| Attention | 23.8 (7.466) | 24.00 [17–30] | 22.29 (8.319) | 21.00 [16.50–29.50] |
| Clarity | 28.80 (7.478) | 27.00 [24–36] | 26.59 (8.178) | 25.00 [23.00–31.50] |
| Repair | 27.29 (7.271) | 29.00 [22–33] | 27.35 (8.268) | 28.00 [20.50–34.00] |
| Physical Function | Physical Role | Pain | General Health | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | p | Mean | p | Mean | p | Mean | p | |
| Gender | ||||||||
| Male Female | 52.13 (28.56) 46.00 (30.12) | 0.120 | 42.97 (40.41) 44.38 (38.94) | 0.422 | 57.27 (31.94) 53.62 (31.89) | 0.261 | 37.58 (20.74) 36.83 (20.45) | 0.419 |
| Age | ||||||||
| 25–45 | 75.52 (17.15) | <0.001 | 56.57 (38.94) | 0.305 | 62.76 (27.87) | 0.207 | 39.73 (17.27) | 0.166 |
| 46–65 | 57.16 (27.14) | 41.89 (38.66) | 61.28 (31.70) | 42.02 (20.29) | ||||
| >65 | 40.79 (27.99) | 41.15 (40.51) | 52.01 (32.52) | 34.63 (21.15) | ||||
| Living situation | ||||||||
| Alone | 57.22 (32.86) | 0.199 | 38.88 (39.50) | 0.478 | 55.13 (33.06) | 0.242 | 38.88 (16.58) | 0.348 |
| With family | 48.38 (28.53) | 43.64 (40.19) | 55.46 (31.69) | 36.73 (21.09) | ||||
| Nursing homes | 77.50 (10.60) | 75.00 (0.00) | 93.75 (8.83) | 57.50 (17.67) | ||||
| Level of education | ||||||||
| Primary | 46.32 (29.09) | 0.027 | 39.85 (39.30) | 0.122 | 53.58 (31.50) | 0.160 | 36.42 (20.39) | 0.604 |
| Secondary | 61.80 (27.07) | 53.00 (39.07) | 60.80 (30.10) | 39.60 (22.68) | ||||
| University | 62.85 (25.79) | 64.28 (45.31) | 75.00 (39.55) | 42.85 (15.77) | ||||
| Emotional Wellbeing | Emotional Role | Social Function | Vitality | |||||
|---|---|---|---|---|---|---|---|---|
| Mean | p | Mean | p | Mean | p | Mean | p | |
| Gender | ||||||||
| Male | 64.51 (23.00) | 0.235 | 76.40 (37.42) | 0.045 | 66.03 (27.39) | 0.173 | 49.32 (24.27) | 0.187 |
| Female | 61.38 (26.52) | 64.11 (45.33) | 61.22 (30.85) | 45.30 (27.22) | ||||
| Age | ||||||||
| 25–45 | 68.42 (24.54) | 0.463 | 73.68 (39.40) | 0.916 | 71.44 (30.22) | 0.447 | 60.26 (22.20) | 0.038 |
| 46–65 | 65.18 (23.41) | 73.87 (38.59) | 65.20 (24.49) | 49.72 (23.83) | ||||
| >65 | 61.43 (24.63) | 70.83 (42.27) | 62.28 (30.04) | 44.20 (25.93) | ||||
| Living situation | ||||||||
| Alone | 62.00 (23.61) | 0.679 | 79.62 (34.56) | 0.693 | 65.97 (26.36) | 0.964 | 44.44 (26.00) | 0.537 |
| With family | 63.37 (24.58) | 70.97 (41.64) | 64.11 (29.14) | 48.13 (25.41) | ||||
| Nursing homes | 78.00 (2.82) | 66.66 (47.14) | 62.50 (35.35) | 65.00 (07.07) | ||||
| Level of education | ||||||||
| Primary | 60.83 (24.17) | 0.036 | 69.26 (41.77) | 0.346 | 61.93 (28.23) | 0.182 | 46.41 (25.78) | 0.143 |
| Secondary | 69.19 (24.11) | 81.33 (36.10) | 71.00 (29.69) | 49.20 (23.34) | ||||
| University | 81.71 (15.45) | 80.95 (37.79) | 76.78 (28.34) | 65.71 (20.70) | ||||
| Coefficients | ||||||
|---|---|---|---|---|---|---|
| Non Standardized Coefficients | Standardized Coefficients | t | Sig. | 95.0% CI for B | ||
| B | Std. Error | β | ||||
| Constant | 80.449 | 76.904 | 1.046 | 0.299 | −72.511 to 233.409 | |
| Age | 0.590 | 0.744 | 0.087 | 0.793 | 0.430 | −0.890 to 2.070 |
| Level of education | 10.405 | 19.832 | 0.058 | 0.525 | 0.601 | −29.041 to 49.850 |
| Attention | −1.762 | 1.659 | −0.128 | −1.062 | 0.291 | −5.062 to 1.538 |
| Clarity | −0.253 | 2.057 | −0.018 | −0.123 | 0.903 | −4.345 to 3.839 |
| Repair | 3.805 | 2.200 | 0.270 | 1.730 | 0.087 | −0.570 to 8.180 |
| Coefficients | ||||||
|---|---|---|---|---|---|---|
| Non Standardized Coefficients | Standardized Coefficients | t | Sig. | 95.0% CI for B | ||
| B | Std. Error | β | ||||
| Constant | 242.504 | 96.294 | 2.518 | 0.016 | 48.309 to 436.699 | |
| Age | −1.666 | 0.866 | −0.266 | −1.923 | 0.061 | −3.414 to 0.081 |
| Level of education | −6.354 | 27.897 | −0.032 | −0.228 | 0.821 | −62.614 to 49.905 |
| Attention | −3.730 | 1.816 | −0.301 | −2.055 | 0.046 | −7.392 to −0.069 |
| Clarity | −2.004 | 2.085 | −0.159 | −0.961 | 0.342 | −6.209 to 2.201 |
| Repair | 7.163 | 2.025 | 0.574 | 3.538 | <0.001 | 3.080 to 11.247 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masià-Plana, A.; Sitjar-Suñer, M.; Mantas-Jiménez, S.; Suñer-Soler, R. The Influence of Emotional Intelligence on Quality of Life in Patients Undergoing Chronic Hemodialysis Focused on Age and Gender. Behav. Sci. 2024, 14, 220. https://doi.org/10.3390/bs14030220
Masià-Plana A, Sitjar-Suñer M, Mantas-Jiménez S, Suñer-Soler R. The Influence of Emotional Intelligence on Quality of Life in Patients Undergoing Chronic Hemodialysis Focused on Age and Gender. Behavioral Sciences. 2024; 14(3):220. https://doi.org/10.3390/bs14030220
Chicago/Turabian StyleMasià-Plana, Afra, Miquel Sitjar-Suñer, Susana Mantas-Jiménez, and Rosa Suñer-Soler. 2024. "The Influence of Emotional Intelligence on Quality of Life in Patients Undergoing Chronic Hemodialysis Focused on Age and Gender" Behavioral Sciences 14, no. 3: 220. https://doi.org/10.3390/bs14030220