
The Role of Alexithymia and Impulsivity in Male Victims and Perpetrators of Intimate Partner Violence

Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedure
2.2. Sample Size Calculation
2.3. Participants
2.4. Measures
2.4.1. Toronto Alexithymia Scale 20 (TAS-20)
2.4.2. Barratt Impulsiveness Scale (BIS-11)
2.5. Statistical Analyses
3. Results
3.1. Preliminary Analyses: Controlling Model Assumptions
3.2. Preliminary Analyses: Assessment of General Alexithymia Levels among Groups
3.3. Profile Analysis: Parallelism
3.4. Profile Analysis: Level Equality—Between-Group Differences
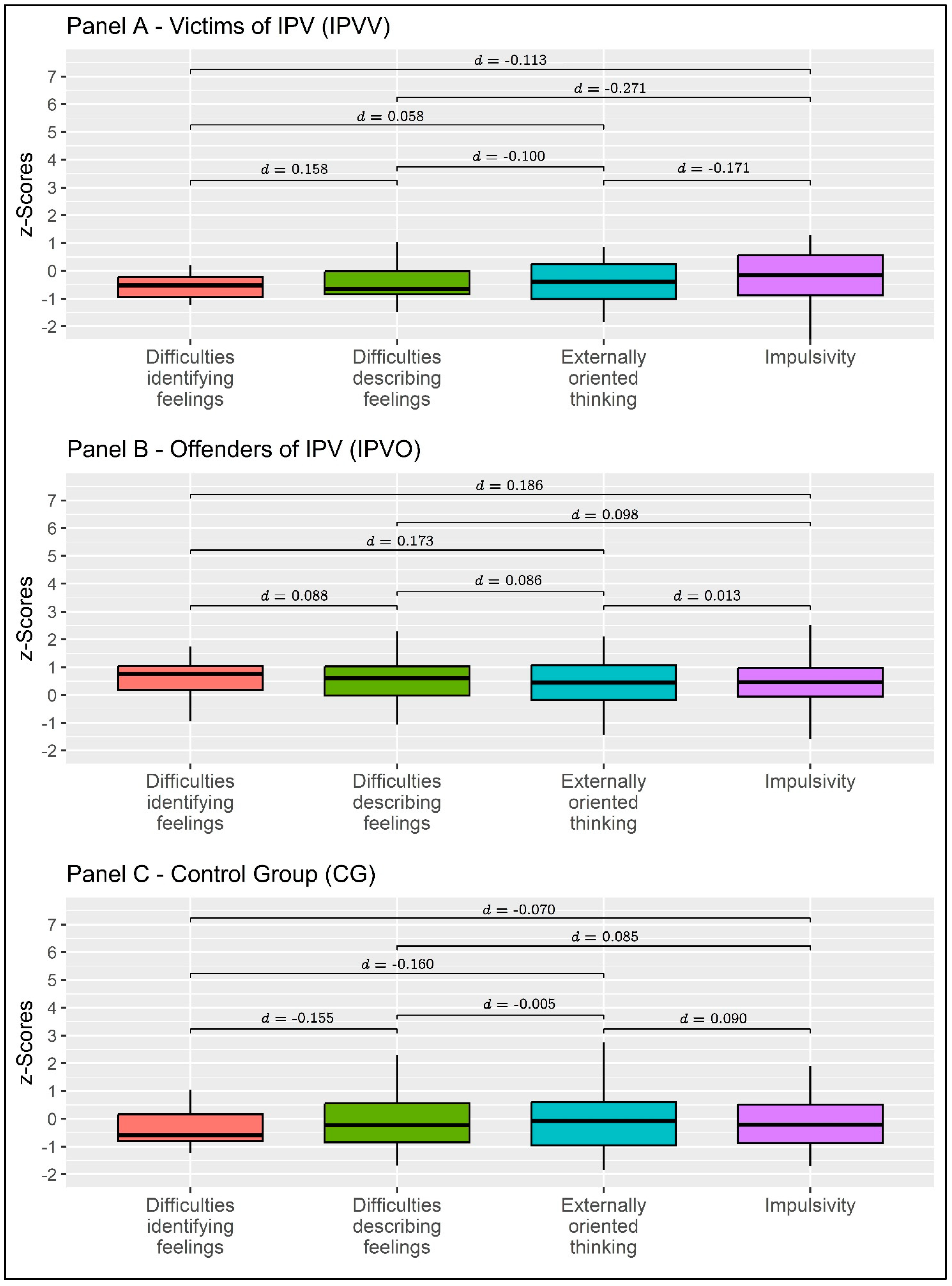
3.5. Profile Analysis: Flatness—Within-Group Differences
4. Discussion
4.1. Implications for Practice
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krug, G.E.; Dahlberg, L.L.; Mercy, A.J.; Zwi, B.A.; Lozano, R. World Report on Violence and Health; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- WHO. Global, Regional and National Prevalence Estimates for Intimate Partner Violence against Women and Global and Regional Prevalence Estimates for Non-Partner Sexual Violence against Women; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Taccini, F.; Rossi, A.A.; Mannarini, S. Women’s EmotionS, Trauma and EmpowErMent (W-ES.T.EEM) study protocol: A psychoeducational support intervention for victims of domestic violence—A randomised controlled trial. BMJ Open 2022, 12, e060672. [Google Scholar] [CrossRef] [PubMed]
- Taccini, F.; Rossi, A.A.; Mannarini, S. Intergenerational Transmission of Relational Styles: Current Considerations. Front. Psychol. 2021, 12, 672961. [Google Scholar] [CrossRef] [PubMed]
- Mannarini, S.; Balottin, L.; Munari, C.; Gatta, M. Assessing conflict management in the couple: The definition of a latent dimension. Fam. J. 2017, 25, 13–22. [Google Scholar] [CrossRef]
- Taccini, F.; Mannarini, S. An Attempt to Conceptualize the Phenomenon of Stigma toward Intimate Partner Violence Survivors: A Systematic Review. Behav. Sci. 2023, 13, 194. [Google Scholar] [CrossRef] [PubMed]
- Kolbe, V.; Büttner, A. Domestic Violence Against Men-Prevalence and Risk Factors. Dtsch. Arztebl. Int. 2020, 117, 534–541. [Google Scholar] [CrossRef] [PubMed]
- Trombetta, T.; Rollè, L. Intimate Partner Violence Perpetration Among Sexual Minority People and Associated Factors: A Systematic Review of Quantitative Studies. Sex. Res. Soc. Policy 2022. [Google Scholar] [CrossRef]
- Mannarini, S.; Taccini, F.; Rossi, A.A. Women and violence: Alexithymia, relational competence and styles, and satisfaction with life: A comparative profile analysis. Behav. Sci. 2021, 11, 147. [Google Scholar] [CrossRef]
- Tharp, A.T.; DeGue, S.; Valle, L.A.; Brookmeyer, K.A.; Massetti, G.M.; Matjasko, J.L. A systematic qualitative review of risk and protective factors for sexual violence perpetration. Trauma Violence Abus. 2013, 14, 133–167. [Google Scholar] [CrossRef]
- Bagby, R.M.; Parker, J.D.; Taylor, G.J. The twenty-item Toronto Alexithymia Scale—I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- Strickland, J.; Parry, C.L.; Allan, M.M.; Allan, A. Alexithymia among Perpetrators of Violent Offences in Australia: Implications for Rehabilitation. Aust. Psychol. 2017, 52, 230–237. [Google Scholar] [CrossRef]
- Mannarini, S.; Balottin, L.; Palmieri, A.; Carotenuto, F. Emotion regulation and parental bonding in families of adolescents with internalizing and externalizing symptoms. Front. Psychol. 2018, 9, 1493. [Google Scholar] [CrossRef] [PubMed]
- Hornsveld, R.H.J.; Kraaimaat, F.W. Alexithymia in Dutch violent forensic psychiatric outpatients. Psychol. Crime Law 2012, 18, 833–846. [Google Scholar] [CrossRef]
- Craparo, G.; Gori, A.; Petruccelli, I.; Cannella, V.; Simonelli, C. Intimate partner violence: Relationships between alexithymia, depression, attachment styles, and coping strategies of battered women. J. Sex. Med. 2014, 11, 1484–1494. [Google Scholar] [CrossRef]
- Yelsma, P. Affective Orientations of Perpetrators, Victims, and Functional Spouses. J. Interpers. Violence 2016, 11, 141–161. [Google Scholar] [CrossRef]
- Anuk, D.; Bahadır, G. The association of experience of violence and somatization, depression, and alexithymia: A sample of women with medically unexplained symptoms in Turkey. Arch. Women’s Ment. Health 2018, 21, 93–103. [Google Scholar] [CrossRef]
- Signorelli, M.; Fusar-Poli, L.; Arcidiacono, E.; Caponnetto, P.; Aguglia, E. Depression, PTSD and alexithymia in victims of intimate partner violence: A case-control study. Arc. Clin. Psychiatr. 2020, 47, 45–50. [Google Scholar] [CrossRef]
- De Rick, A.; Vanheule, S. Alexithymia and DSM-IV personality disorder traits in alcoholic inpatients: A study of the relation between both constructs. Personal. Individ. Differ. 2007, 43, 119–129. [Google Scholar] [CrossRef]
- Zimmermann, G. Delinquency in male adolescents: The role of alexithymia and family structure. J. Adolesc. 2006, 29, 321–332. [Google Scholar] [CrossRef]
- Lumley, M.A.; Neely, L.C.; Burger, A.J. The assessment of alexithymia in medical settings: Implications for understanding and treating health problems. J. Pers. Assess. 2007, 89, 230–246. [Google Scholar] [CrossRef]
- Shishido, H.; Gaher, R.M.; Simons, J.S. I don’t know how I feel, therefore I act: Alexithymia, urgency, and alcohol problems. Addict. Behav. 2013, 38, 2014–2017. [Google Scholar] [CrossRef]
- Herman, A.M.; Pilcher, N.; Duka, T. Deter the emotions: Alexithymia, impulsivity and their relationship to binge drinking. Addict. Behav. Rep. 2020, 12, 100308. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Zhu, Z.; Zhang, W.; Chen, Y.; Zhen, S. Trait impulsivity components correlate differently with proactive and reactive control. PLoS ONE 2017, 12, e0176102. [Google Scholar] [CrossRef] [PubMed]
- Stanford, M.S.; Mathias, C.W.; Dougherty, D.M.; Lake, S.L.; Anderson, N.E.; Patton, J.H. Fifty years of the Barratt Impulsiveness Scale: An update and review. Personal. Individ. Differ. 2009, 47, 385–395. [Google Scholar] [CrossRef]
- Moeller, F.G.; Barratt, E.S.; Dougherty, D.M.; Schmitz, J.M.; Swann, A.C. Psychiatric aspects of impulsivity. Am. J. Psychiatry 2001, 158, 1783–1793. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.; Zabala, C.; Del-Monte, J.; Graziani, P.; Aizpurua, E.; Barry, T.J.; Ricarte, J. Examining the relationships between impulsivity, aggression, and recidivism for prisoners with antisocial personality disorder. Aggress. Violent Behav. 2019, 49, 101314. [Google Scholar] [CrossRef]
- Lawrence, K.A.; Allen, J.S.; Chanen, A.M. Impulsivity in borderline personality disorder: Reward-based decision-making and its relationship to emotional distress. J. Personal. Disord. 2010, 24, 786–799. [Google Scholar] [CrossRef] [PubMed]
- Swogger, M.T.; Walsh, Z.; Kosson, D.S. Domestic violence and psychopathic traits: Distinguishing the antisocial batterer from other antisocial offenders. Aggress. Behav. 2007, 33, 253–260. [Google Scholar] [CrossRef]
- Dolan, M.; Anderson, I.M.; Deakin, J.F.W. Relationship between 5-HT function and impulsivity and aggression in male offenders with personality disorders. Br. J. Psychiatry 2001, 178, 352–359. [Google Scholar] [CrossRef]
- Stanford, M.S.; Houston, R.J.; Baldridge, R.M. Comparison of impulsive and premeditated perpetrators of intimate partner violence. Behav. Sci. Law 2008, 26, 709–722. [Google Scholar] [CrossRef]
- Helfritz, L.E.; Stanford, M.S.; Conklin, S.M.; Greve, K.W.; Villemarette-Pittman, N.R.; Houston, R.J. Usefulness of Self-Report Instruments in Assessing Men Accused of Domestic Violence. Psychol. Rec. 2006, 56, 171–180. [Google Scholar] [CrossRef]
- Tharp, A.T.; Schumacher, J.A.; Samper, R.E.; McLeish, A.C.; Coffey, S.F. Relative Importance of Emotional Dysregulation, Hostility, and Impulsiveness in Predicting Intimate Partner Violence Perpetrated by Men in Alcohol Treatment. Psychol. Women Q. 2013, 37, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Di Piazza, L.; Kowal, C.; Hodiaumont, F.; Blavier, A. Intimate partner violence: Perseverance vs Dropout from treatment programs targeting male batterers. In Proceedings of the Annual Meeting of the Belgian Association for Psychological Science, Anvers, Belgium, 24 May 2016. [Google Scholar]
- Stuart, G.L.; Holtzworth-Munroe, A. Testing a Theoretical Model of the Relationship Between Impulsivity, Mediating Variables, and Husband Violence. J. Fam. Violence 2005, 20, 291–303. [Google Scholar] [CrossRef]
- Molero Jurado, M.D.M.; Pérez-Fuentes, M.D.C.; Simón Márquez, M.D.M.; Barragán Martín, A.B.; Sisto, M.; Gázquez Linares, J.J. Relationship Between Impulsivity, Sensation-Seeking, and Drug Use in Aggressors and Victims of Violence. Front. Psychol. 2020, 11, 600055. [Google Scholar] [CrossRef] [PubMed]
- Mullet, N.; Hawkins, L.G.; Tuliao, A.P.; Snyder, H.; Holyoak, D.; McGuire, K.C.; Earl, A.K.; McChargue, D. Early Trauma and Later Sexual Victimization in College Women: A Multiple Mediation Examination of Alexithymia, Impulsivity, and Alcohol Use. J. Interpers. Violence 2022, 37, Np18194–Np18214. [Google Scholar] [CrossRef] [PubMed]
- Messman-Moore, T.L.; Ward, R.M.; Zerubavel, N. The role of substance use and emotion dysregulation in predicting risk for incapacitated sexual revictimization in women: Results of a prospective investigation. Psychol. Addict. Behav. 2013, 27, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Bulut, O.; Desjardins, C.D. Profile Analysis of Multivariate Data: A Brief Introduction to the ProfileR Package; University of Minnesota: Minneapolis, MN, USA, 2020; pp. 1–16. [Google Scholar] [CrossRef]
- Schmit, M.K.; Oller, M.L.; Tapia-Fuselier, J.L.; Schmit, E.L. A Holistic Client Functioning Profile Comparison of People with Serious Mental Illness. J. Couns. Dev. 2020, 98, 3–16. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics; Pearson: Harlow, UK, 2014. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- Pillai, K.C.S. Some New Test Criteria in Multivariate Analysis. Ann. Math. Statist. 1955, 26, 117–121. [Google Scholar] [CrossRef]
- Eid, M.; Gollwitzer, M.; Schmitt, M. Statistik und Forschungsmethoden, 5th ed.; Beltz: Basel, Switzerland, 2017. [Google Scholar]
- Bressi, C.; Taylor, G.; Parker, J.; Bressi, S.; Brambilla, V.; Aguglia, E.; Allegranti, I.; Bongiorno, A.; Giberti, F.; Bucca, M.; et al. Cross validation of the factor structure of the 20-item Toronto Alexithymia Scale: An Italian multicenter study. J. Psychosom. Res. 1996, 41, 551–559. [Google Scholar] [CrossRef]
- Leshem, R.; van Lieshout, P.H.H.M.; Ben-David, S.; Ben-David, B.M. Does emotion matter? The role of alexithymia in violent recidivism: A systematic literature review. Crim. Behav. Ment. Health 2019, 29, 94–110. [Google Scholar] [CrossRef]
- Fossati, A.; Di Ceglie, A.; Acquarini, E.; Barratt, E.S. Psychometric properties of an Italian version of the Barratt Impulsiveness Scale-11 (BIS-11) in nonclinical subjects. J. Clin. Psychol. 2001, 57, 815–828. [Google Scholar] [CrossRef] [PubMed]
- Patton, J.H.; Stanford, M.S.; Barratt, E.S. Factor structure of the barratt impulsiveness scale. J. Clin. Psychol. 1995, 51, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D. esvis: Visualization and Estimation of Effect Sizes; Version 0.3.1; 2020. Available online: https://github.com/datalorax/esvis (accessed on 27 April 2023).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Revelle, W. psych: Procedures for Personality and Psychological Research; Northwestern University: Evanston, IL, USA, 2018. [Google Scholar]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Rossi, A.A.; Pietrabissa, G.; Tagliagambe, A.; Scuderi, A.; Montecchiani, L.; Castelnuovo, G.; Mannarini, S.; Dalla Ragione, L. Many facets of eating disorders: Profiling key psychological features of anorexia nervosa and binge eating disorder. Behav. Sci. 2023, 13, 276. [Google Scholar] [CrossRef]
- Bulut, O.; Davison, M.L.; Rodriguez, M.C. Estimating Between-Person and Within-Person Subscore Reliability with Profile Analysis. Multivar. Behav. Res. 2017, 52, 86–104. [Google Scholar] [CrossRef] [PubMed]
- Bulut, O.; Desjardins, C.D. profileR: Profile Analysis of Multivariate Data in R; R package version 0.3-5; 2018. Available online: https://cran.r-project.org/web/packages/profileR/index.html (accessed on 27 April 2023).
- Davison, M.L.; Davenport, E.C.J. Identifying criterion-related patterns of predictor scores using multiple regression. Psychol. Methods 2002, 7, 468–484. [Google Scholar] [CrossRef] [PubMed]
- Schmit, M.K.; Watson, J.C.; Schmit, E.L. Using Profile Analysis in Counseling Outcome Research. Couns. Outcome Res. Eval. 2019, 10, 94–105. [Google Scholar] [CrossRef]
- Watkins, M.W.; Glutting, J.J.; Youngstrom, E.A. Issues in Subtest Profile Analysis. In Contemporary Intellectual Assessment: Theories, Tests, and Issues; The Guilford Press: New York, NY, USA, 2005; pp. 251–268. [Google Scholar]
- Howell, D.C. Statistical Methods for Psychology; Wadsworth, Cengage Learning: Belmont, CA, USA, 2013. [Google Scholar]
- Pond Jr, R.S.; Kashdan, T.B.; DeWall, C.N.; Savostyanova, A.; Lambert, N.M.; Fincham, F.D. Emotion differentiation moderates aggressive tendencies in angry people: A daily diary analysis. Emotion 2012, 12, 326–337. [Google Scholar] [CrossRef]
- Garofalo, C.; Velotti, P.; Zavattini, G.C. Emotion regulation and aggression: The incremental contribution of alexithymia, impulsivity, and emotion dysregulation facets. Psychol. Violence 2018, 8, 470–483. [Google Scholar] [CrossRef]
- Romero-Martínez, Á.; Lila, M.; Martínez, M.; Pedrón-Rico, V.; Moya-Albiol, L. Improvements in Empathy and Cognitive Flexibility after Court-Mandated Intervention Program in Intimate Partner Violence Perpetrators: The Role of Alcohol Abuse. Int. J. Env. Res. Public Health 2016, 13, 394. [Google Scholar] [CrossRef]
- Louth, S.M.; Hare, R.D.; Linden, W. Psychopathy and alexithymia in female offenders. Can. J. Behav. Sci./Rev. Can. Des Sci. Du Comport. 1998, 30, 91–98. [Google Scholar] [CrossRef]
- Zarei, J.; Besharat, M.a. Alexithymia and interpersonal problems. Procedia -Soc. Behav. Sci. 2010, 5, 619–622. [Google Scholar] [CrossRef]
- Valdespino, A.; Antezana, L.; Ghane, M.; Richey, J.A. Alexithymia as a Transdiagnostic Precursor to Empathy Abnormalities: The Functional Role of the Insula. Front Psychol 2017, 8, 2234. [Google Scholar] [CrossRef] [PubMed]
- Walker, L. Battered woman syndrome: Empirical findings. Ann. NY Acad. Sci. 2006, 1087, 142–157. [Google Scholar] [CrossRef] [PubMed]
- Fossati, A.; Acquarini, E.; Feeney, J.A.; Borroni, S.; Grazioli, F.; Giarolli, L.E.; Franciosi, G.; Maffei, C. Alexithymia and attachment insecurities in impulsive aggression. Attach. Hum. Dev. 2009, 11, 165–182. [Google Scholar] [CrossRef]
- Bateman, A.; Fonagy, P. Mentalization-based treatment. Psychoanal. Inq. 2013, 33, 595–613. [Google Scholar] [CrossRef]
- Cameron, K.; Ogrodniczuk, J.; Hadjipavlou, G. Changes in Alexithymia Following Psychological Intervention: A Review. Harv. Rev. Psychiatry 2014, 22, 162–178. [Google Scholar] [CrossRef]
- Mannarini, S. A method for the definition of a self-awareness behavior dimension with clinical subjects: A latent trait analysis. Behav. Res. Methods 2009, 41, 1029–1037. [Google Scholar] [CrossRef]
- Shorey, R.C.; Brasfield, H.; Febres, J.; Stuart, G.L. The association between impulsivity, trait anger, and the perpetration of intimate partner and general violence among women arrested for domestic violence. J. Interpers. Violence 2011, 26, 2681–2697. [Google Scholar] [CrossRef]
- Mannarini, S.; Boffo, M.; Balottin, L. Beliefs about the patient’s role in the psychotherapeutic relationship: A latent trait perspective. TPM Test Psychom. Methodol. Appl. Psychol. 2013, 20, 277–294. [Google Scholar] [CrossRef]
- Wang, X.; Cheng, Z. Cross-Sectional Studies: Strengths, Weaknesses, and Recommendations. Chest 2020, 158, S65–S71. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Descriptive Statistics | Correlations | Collinearity | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | Sk | K | 1 | 2 | 3 | 4 | 5 | T | VIF | ||
| 1 | TAS-20 | 46.62 | 13.576 | 0.391 | −0.696 | - | - | - | ||||
| 2 | DIF | 15.66 | 7.051 | 0.698 | −0.311 | 0.896 *** | - | 0.407 | 2.460 | |||
| 3 | DDF | 13.09 | 4.781 | 0.399 | −0.546 | 0.856 *** | 0.723 *** | - | 0.462 | 2.164 | ||
| 4 | EOT | 17.87 | 4.787 | 0.185 | −0.338 | 0.681 *** | 0.347 ** | 0.363 ** | - | 0.847 | 1.181 | |
| 5 | BIS-11 | 59.53 | 9.700 | −0.030 | −0.341 | 0.530 *** | 0.548 *** | 0.433 *** | 0.264 * | - | 0.692 | 1.445 |
| IPVV | IPVP | CG | IPVV vs. IPVP | IPVP vs. CG | IPVV vs. CG | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | t | d | t | d | t | d | ||
| 1 | DIF | 13.33 | 6.621 | 19.16 | 5.640 | 14.37 | 7.472 | −2.946 * | −0.872 | 2.649 * | 0.717 | −0.544 | −0.155 |
| 2 | DDF | 10.86 | 3.229 | 15.08 | 4.349 | 13.00 | 5.408 | −3.136 ** | −0.928 | 1.689 * | 0.457 | −1.656 | −0.471 |
| 3 | EOT | 16.05 | 3.827 | 19.48 | 4.473 | 17.80 | 5.288 | −2.489 * | −0.737 | 1.332 | 0.361 | −1.322 | −0.376 |
| 4 | BIS-11 | 57.29 | 10.061 | 62.68 | 10.007 | 58.47 | 8.792 | −1.907 | −0.564 | 1.628 | 0.441 | −0.434 | −0.124 |
| IPVV | IPVP | CG | |||||
|---|---|---|---|---|---|---|---|
| t | d | t | d | t | d | ||
| DIF | DDF | 0.595 | 0.158 | 0.447 | 0.088 | −0.767 | −0.155 |
| EOT | 0.219 | 0.058 | 0.884 | 0.173 | −0.790 | −0.160 | |
| BIS-11 | −0.426 | −0.113 | 0.948 | 0.186 | −0.346 | −0.070 | |
| DDF | EOT | −0.376 | −0.100 | 0.437 | 0.086 | −0.023 | −0.005 |
| BIS-11 | −1.020 | −0.271 | 0.501 | 0.098 | 0.421 | 0.085 | |
| EOT | BIS-11 | −0.644 | −0.171 | 0.064 | 0.013 | 0.444 | 0.090 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mannarini, S.; Taccini, F.; Rossi, A.A. The Role of Alexithymia and Impulsivity in Male Victims and Perpetrators of Intimate Partner Violence. Behav. Sci. 2023, 13, 402. https://doi.org/10.3390/bs13050402
Mannarini S, Taccini F, Rossi AA. The Role of Alexithymia and Impulsivity in Male Victims and Perpetrators of Intimate Partner Violence. Behavioral Sciences. 2023; 13(5):402. https://doi.org/10.3390/bs13050402
Chicago/Turabian StyleMannarini, Stefania, Federica Taccini, and Alessandro Alberto Rossi. 2023. "The Role of Alexithymia and Impulsivity in Male Victims and Perpetrators of Intimate Partner Violence" Behavioral Sciences 13, no. 5: 402. https://doi.org/10.3390/bs13050402