
The Relationship between Physical Activity and Psychosocial Well-Being during and after COVID-19 Lockdown


Abstract
:1. Introduction
2. Physical Activity during and after the Pandemic
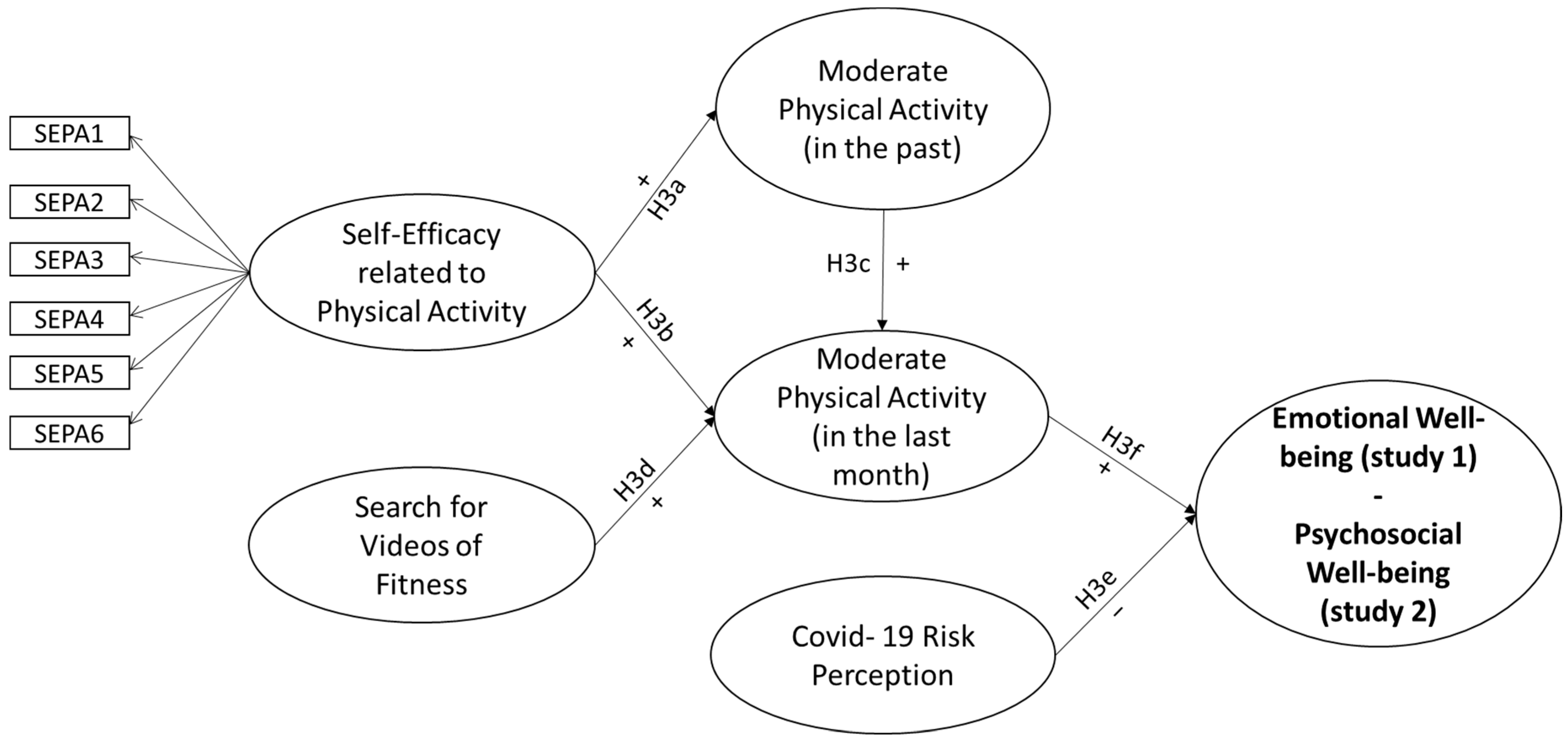
3. Aims and Hypothesis
4. Materials and Methods
4.1. Measures
4.2. Statistical Analysis
4.3. Participants and Procedure of Recruitment
5. Results
5.1. Study 1
5.1.1. Physical Activity before and during Lockdown
5.1.2. Correlations
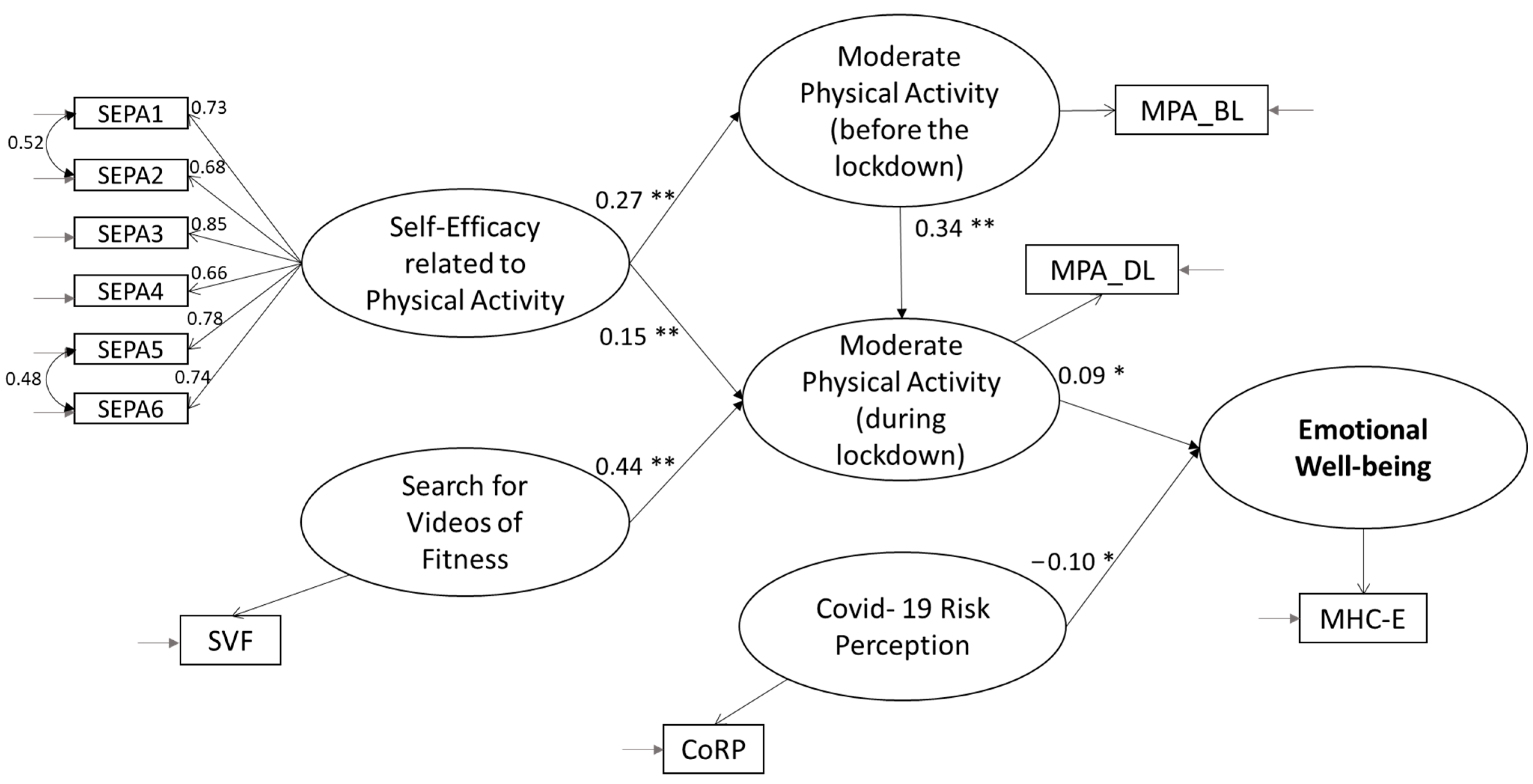
5.1.3. Testing of the Hypothesized Conceptual Model
5.2. Study 2
5.2.1. The Practice of Physical Activities during the Lockdown and after 2 Years
5.2.2. Correlations
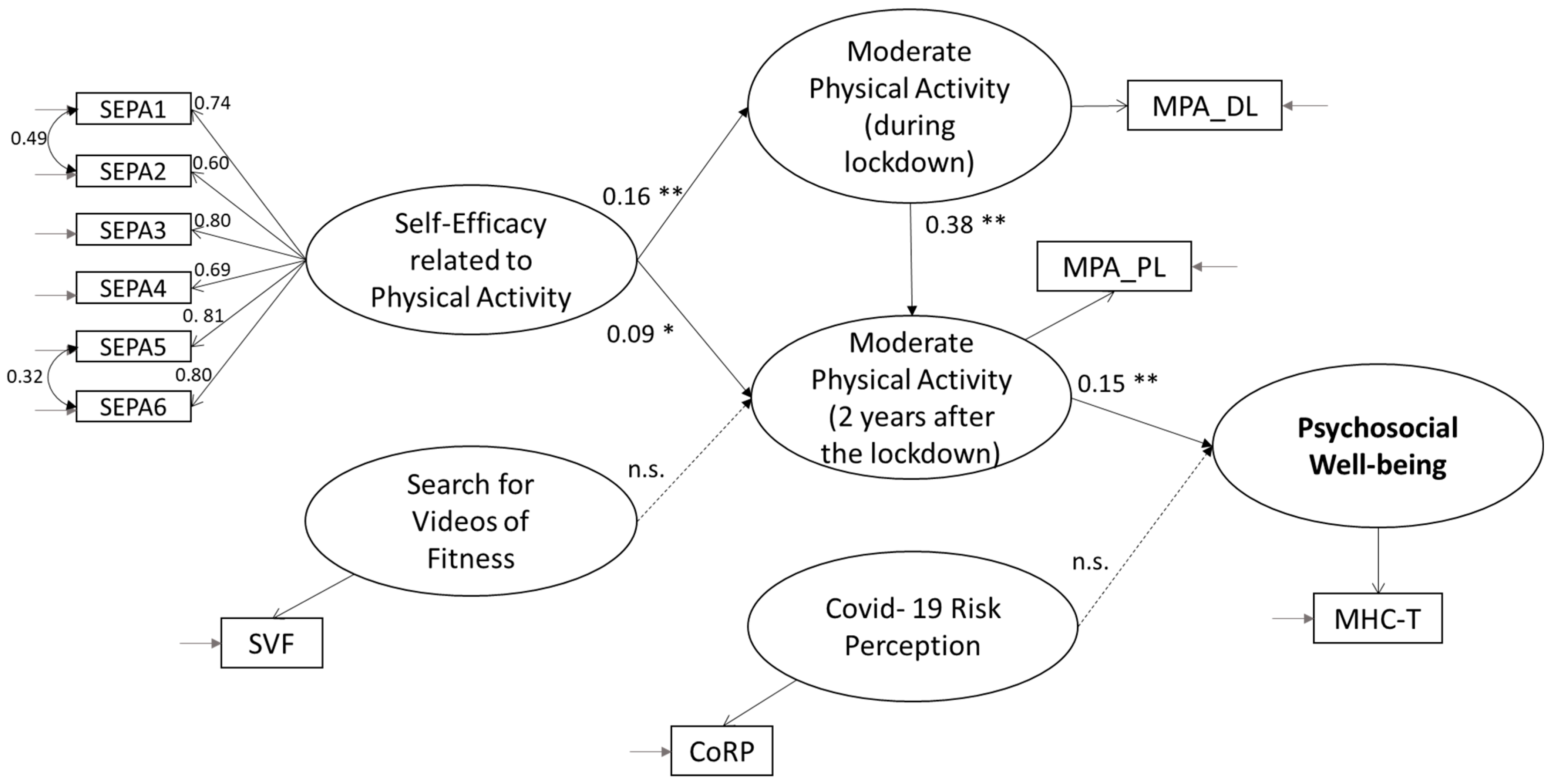
5.2.3. Testing of the Hypothesized Conceptual Model
6. Discussion and Conclusions
Limitations of the Study and Future Research Lines
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Ottawa charter for health promotion. In Proceedings of the First International Conference on Health Promotion, Ottawa, ON, Canada, 21 November 1986. [Google Scholar]
- Petrillo, G. L’approccio bio-psico-sociale alla promozione della salute: Definizioni e caratteristiche. In Psicologia della Salute: Contesti di Applicazione Dell’approccio Bio-Psico-Sociale; Mauri, C., Tinti, A., Eds.; Utet: Torino, Italy, 2006; pp. 3–15. [Google Scholar]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Filadelfia, PA, USA, 2013. [Google Scholar]
- Ryff, C.D.; Keyes, C.L.M. The structure of psychological well-being revisited. J. Pers. Soc. Psychol. 1995, 69, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Ryff, C.D. Psychological well-being in adult life. Curr. Dir. Psychol. Sci. 1995, 4, 99–104. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; De Leon, A.P.; Dunn, A.L.; Deslandes, A.C.; et al. Physical activity and incident depression: A meta-analysis of prospective cohort studies. Am. J. Psychiatry 2018, 175, 631–648. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Stubbs, B.; Meyer, J.; Heissel, A.; Zech, P.; Vancampfort, D.; Rosenbaum, S.; Deenik, J.; Firth, J.; Ward, P.B.; et al. Physical activity protects from incident anxiety: A meta-analysis of prospective cohort studies. Depress. Anxiety 2019, 36, 846–858. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L.M. Promoting and protecting mental health as flourishing: A complementary strategy for improving national mental health. Am. Psychol. 2007, 62, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Ryan, R.M.; Huta, V.; Deci, E.L. Living well: A self-determination theory perspective on eudaimonia. J. Happiness Stud. 2008, 9, 139–170. [Google Scholar] [CrossRef]
- Diener, E.; Suh, E.; Lucas, R.; Smith, H. Subjective well-being: Three decades of progress. Psychol. Bull. 1999, 125, 276–302. [Google Scholar] [CrossRef]
- Ryff, C. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Pers. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Delle Fave, A.; Bassi, M. The contribution of diversity to happiness research. J. Posit. Psychol. 2009, 4, 205–207. [Google Scholar] [CrossRef]
- Keyes, C.L.M. Social well being. Soc. Psychol. Q. 1998, 61, 121–140. [Google Scholar] [CrossRef]
- Keyes, C.L.M. Complete mental health: An agenda for the 21st century. In Flourishing: Positive Psychology and the Life Well-Lived; Keyes, C.L.M., Haidt, J., Eds.; American Psychological Association: Washington, DC, USA, 2003; pp. 293–312. [Google Scholar] [CrossRef]
- Van der Linden, S. Determinants and Measurement of Climate Change Risk Perception, Worry, and Concern. In Oxford Encyclopedia of Climate Change Communication; Nisbet, M.C., Schafer, M., Markowitz, E., Ho, S., O’Neill, S., Thaker, J., Eds.; The Oxford University Press: Oxford, UK, 2017. [Google Scholar] [CrossRef]
- Donizzetti, A.R. La percezione del rischio in adolescenza: Costruzione e validazione di strumenti di rilevazione. Psicol. Salute 2009, 2, 145–162. [Google Scholar] [CrossRef]
- Floyd, D.L.; Prentice-Dunn, S.; Rogers, R.W. A Meta-Analysis of Research on Protection Motivation Theory. J. Appl. Soc. Psychol. 2000, 30, 407–429. [Google Scholar] [CrossRef]
- Wise, T.; Zbozinek, T.D.; Michelini, G.; Hagan, C.C. Changes in Risk Perception and Protective Behavior During the First Week of the COVID-19 Pandemic in the United States. R. Soc. Open Sci. 2020, 7, 200742. [Google Scholar] [CrossRef] [PubMed]
- Davico, C.; Ghiggia, A.; Marcotulli, D.; Ricci, F.; Amianto, F.; Vitiello, B. Psychological Impact of the COVID-19 Pandemic on Adults and Their Children in Italy. Lancet Psychiatry 2020, 12, 572997. [Google Scholar] [CrossRef]
- Chang, M.C.; Park, D. Incidence of post–traumatic stress disorder after coronavirus disease. Healthcare 2020, 8, 373. [Google Scholar] [CrossRef] [PubMed]
- Esmaeilzadeh, S.; Rodriquez-Negro, J.; Pesola, A.J. A Greater Intrinsic, but Not External, Motivation Toward Physical Activity Is Associated with a Lower Sitting Time. Front. Psychol. 2022, 13, 888758. [Google Scholar] [CrossRef] [PubMed]
- Kraut, R. Two conceptions of happiness. Philos. Rev. 1979, 88, 167–197. [Google Scholar] [CrossRef]
- Waterman, A.S.; Schwartz, S.J.; Conti, R. The implications of two conceptions of happiness (hedonic enjoyment and eudaimonia) for the understanding of intrinsic motivation. J. Happiness Stud. 2008, 9, 41–79. [Google Scholar] [CrossRef]
- Lee, D.J.; Sirgy, M.J.; Yu, G.B.; Chalamon, I. The Well-Being Effects of Self-Expressiveness and Hedonic Enjoyment Associated with Physical Exercise. Appl. Res. Qual. 2015, 10, 141–159. [Google Scholar] [CrossRef]
- Fuzhong, L.; Duncan, T.E.; Duncan, S.C.; McAuley, E.; Chaumeton, N.R.; Harmer, P. Enhancing the psychological well-being of elderly individuals through tai chi exercise: A latent growth curve analysis. Struct. Equ. Model. 2001, 8, 53–83. [Google Scholar] [CrossRef]
- Long, B.C.; Van Stavel, R. Effects of exercise training on anxiety: A meta-analysis. J. Appl. Sport Psychol. 1995, 7, 167–189. [Google Scholar] [CrossRef]
- Penedo, F.J.; Dahn, J.R. Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Curr. Opin. Psychiatry 2005, 18, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Stubbe, J.H.; de Moor, M.H.M.; Boomsma, D.I.; de Geus, E.J.C. The association between exercise participation and well-being: A co-twin study. Prev. Med. 2007, 44, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Zuosong, C.; Liu, J. The effects of physical exercise on subjective well being of senior high school students and their psychological mechanism. Acta Psychol. Sin. 2006, 38, 562–575. [Google Scholar]
- Zhang, Z.; Chen, W. A systematic review of measures for psychological well-being in physical activity studies and identification of critical issues. J. Affect. Disord. 2019, 256, 473–485. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.R.; Plotnikoff, R.C.; Lubans, N.J. Review: A systematic review of the impact of physical activity programmes on social and emotional well-being in at-risk youth. Child Adolesc. Ment. Health 2012, 17, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Qin, F.; Song, Y.; Nassis, G.P.; Zhao, L.; Cui, S.; Lai, L.; Wu, Z.; Xu, M.; Qu, C.; Dong, Y.; et al. Prevalence of Insufficient Physical Activity, Sedentary Screen Time and Emotional Well-Being During the Early Days of the 2019 Novel Coronavirus (COVID-19) Outbreak in China: A National Cross-Sectional Study. Lancet 2020, 17, 5170. [Google Scholar] [CrossRef]
- Donaldson, S.J.; Ronan, K.R. The effects of sports participation on young adolescents’ emotional well-being. Adolescence 2006, 41, 369–389. [Google Scholar]
- Steptoe, A.; Butler, N. Sports participation and emotional wellbeing in adolescents. Lancet 1996, 347, 1789–1792. [Google Scholar] [CrossRef]
- Donizzetti, A.R. Aspetti psico-sociali del comportamento sportivo: Un’analisi qualitativa di focus group con giovani adulti. Psicol. Salute 2014, 3, 121–135. [Google Scholar] [CrossRef]
- Kohl, H.W.; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Dwyer, L.M.J.; Allison, K.R.; Makin, S. Internal structure of a measure of self-efficacy in physical activity among high school students. Soc. Sci. Med. 1998, 46, 1175–1182. [Google Scholar] [CrossRef] [PubMed]
- Donizzetti, A.R.; Petrillo, G. Antecedenti dell’attività sportiva in adolescenza: Il ruolo delle intenzioni e delle percezioni di autoefficacia nell’ottica processuale dell’HAPA Model. Psicol. Salute 2007, 3, 71–86. [Google Scholar]
- Donizzetti, A.R. L’attività fisica in adolescenza: Quali effetti benefici per la salute? In Promuovere la Salute nei Contesti Educativi. Comportamenti Salutari e Benessere tra gli Adolescenti; Petrillo, G., Caso, D., Eds.; FrancoAngeli: Milano, Italy, 2008; pp. 116–166. [Google Scholar]
- Joseph, R.P.; Royse, K.E.; Benitez, T.J.; Pekmezi, D.W. Physical activity and quality of life among university students: Exploring self-efficacy, self-esteem, and affect as potential mediators. Qual. Life Res. 2014, 23, 659–667. [Google Scholar] [CrossRef] [PubMed]
- McAuley, E.; Lox, C.; Duncan, T.E. Long-term Maintenance of Exercise, Self-Efficacy, and Physiological Change in Older Adults. J. Gerontol. 1993, 48, P218–P224. [Google Scholar] [CrossRef] [PubMed]
- McAuley, E.; Jacobson, L. Self-efficacy and exercise participation in sedentary adult females. Am. J. Health Promot. 1991, 5, 185–207. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A.; Adams, N. Analysis of self-efficacy theory of behavioral change. Cognit. Ther. Res. 1977, 1, 287–310. [Google Scholar] [CrossRef]
- Aedo, Á.; Ávila, H. Nuevo cuestionario para evaluar la autoeficacia hacia la actividad física en niños. Rev. Panameña Salud Pública 2009, 26, 324–329. [Google Scholar] [CrossRef]
- Ulloa, E.J.; Reynaga-Estrada, P.; Serrano, A.M.; Taylor, J.L.; Acosta, J.M.; Rangel, S.P.; González, J.C. Autoeficacia y actividad física en niños mexicanos con obesidad y sobrepeso. SPORT TK-Rev. EuroAmericana Cienc. Deporte 2013, 2, 69–75. [Google Scholar] [CrossRef]
- Bandura, A. Autoefficacia. Teoria e Applicazioni; Erickson: Trento, Italy, 2000. [Google Scholar]
- British Broadcasting Corporation. Coronavirus: The World in Lockdown in Maps and Charts. 2020. Available online: https://www.bbc.co.uk/news/world-52103747 (accessed on 12 September 2022).
- Jacob, L.; Tully, M.A.; Barnett, Y. The relationship between physical activity and mental health in a sample of the UK public: A cross-sectional study during the implementation of COVID-19 social distancing measures. Ment. Health Phys. Act. 2020, 19, 100345. [Google Scholar] [CrossRef]
- Simpson, R.J.; Katsanis, E. The immunological case for staying active during the COVID-19 pandemic. Brain Behav. Immun. 2020, 87, 6–7. [Google Scholar] [CrossRef] [PubMed]
- Brailovskaia, J.; Cosci, F.; Mansueto, G.; Miragall, M.; Herrero, R.; Baños, R.M.; Krasavtseva, Y.; Kochetkov, Y.; Margraf, J. The association between depression symptoms, psychological burden caused by COVID-19 and physical activity: An investigation in Germany, Italy, Russia, and Spain. Psychiatry Res. 2021, 295, 113596. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Guo, T.; Becker, B.; Yu, Q.; Chen, S.T.; Brendon, S.; Hossain, M.M.; Cunha, P.M.; Soares, F.C.; Veronese, N.; et al. Depression is associated with moderate-intensity physical activity among college students during the COVID-19 pandemic: Differs by activity level, gender and gender role. Psychol. Res. Behav. Manag. 2020, 13, 1123–1134. [Google Scholar] [CrossRef] [PubMed]
- Xiang, M.Q.; Tan, X.M.; Sun, J.; Yang, H.Y.; Zhao, X.P.; Liu, L.; Hou, X.H.; Hu, M. Relationship of physical activity with anxiety and depression symptoms in Chinese college students during the COVID-19 outbreak. Front. Psychol. 2020, 11, 582436. [Google Scholar] [CrossRef] [PubMed]
- Vogel, E.A.; Zhang, J.S.; Peng, K.; Heaney, C.A.; Lu, Y.; Lounsbury, D.; Hsing, A.W.; Prochaska, J.J. Physical activity and stress management during COVID-19: A longitudinal survey study. Psychol. Health 2022, 37, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, M.C.; Devonport, T.J.; Chen-Wilson, C.H.; Nicholls, W.; Cagas, J.Y.; Fernandez-Montalvo, J.; Choi, Y.; Robazza, C. A cross-cultural exploratory study of health behaviors and wellbeing during COVID-19. Front. Psychol. 2021, 11, 608216. [Google Scholar] [CrossRef] [PubMed]
- Cerea, S.; Pecunioso, A.; Casali, N.; Moro, T.; Paoli, A.; Ghisi, M. How COVID-19 lockdown affected physical activity levels and wellbeing: An Italian Survey. Int. J. Sport Exerc. Psychol. 2022, 21, 1054–1069. [Google Scholar] [CrossRef]
- Di Sebastiano, K.M.; Chulak-Bozzer, T.; Vanderloo, L.M.; Faulkner, G. Don’t walk so close to me: Physical distancing and adult physical activity in Canada. Front. Psychol. 2020, 11, 1895. [Google Scholar] [CrossRef]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, J.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Romero-Blanco, C.; Rodríguez-Almagro, J.; Onieva-Zafra, M.D.; Parra-Fernández, M.L.; Prado-Laguna, M.d.C.; Hernández-Martínez, A. Physical Activity and Sedentary Lifestyle in University Students: Changes during Confinement Due to the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6567. [Google Scholar] [CrossRef]
- Lombardo, M.; Guseva, E.; Perrone, M.A.; Müller, A.; Rizzo, G.; Storz, M.A. Changes in eating habits and physical activity after COVID-19 pandemic lockdowns in Italy. Nutrients 2021, 13, 4522. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, E.A.; Lee, C.; Jenkins, M.; Calverley, J.R.; Hodge, K.; Houge Mackenzie, S. Changes in physical activity pre-, during and post-lockdown COVID-19 restrictions in New Zealand and the explanatory role of daily hassles. Front. Psychol. 2021, 12, 642954. [Google Scholar] [CrossRef] [PubMed]
- Bu, F.; Bone, J.K.; Mitchell, J.J.; Steptoe, A.; Fancourt, D. Longitudinal changes in physical activity during and after the first national lockdown due to the COVID-19 pandemic in England. Sci. Rep. 2021, 11, 17723. [Google Scholar] [CrossRef] [PubMed]
- Petrillo, G.; Capone, V.; Caso, D.; Keyes, C. The Mental Health Continuum–Short Form (MHC–SF) as a Measure of Well-Being in the Italian Context. Soc. Indic. Res. 2015, 121, 291–312. [Google Scholar] [CrossRef]
- Caso, D.; Donizzetti, A.R. Le scale di autoefficacia specifiche per la salute: Un contributo alla validazione con il modello di Rasch. Psicol. Salute 2004, 2, 161–176. [Google Scholar]
- Donizzetti, A.R. The effects of physical activity on the psychosocial well-being of Italians during the Coronavirus lockdown. In Proceedings of the 35th Annual Conference of the European Health Psychology Society, Online, 23–27 August 2021. [Google Scholar]
- Capone, V.; Donizzetti, A.R.; Park, M.S.-A. Validation and Psychometric Evaluation of the COVID-19 Risk Perception Scale (CoRP): A New Brief Scale to Measure Individuals’ Risk Perception. Int. J. Ment. Health Addict. 2021, 21, 1320–1333. [Google Scholar] [CrossRef] [PubMed]
- Coakes, J.C.; Ong, C. SPSS Version 18.0 for Windows Analysis without Anguish; John Wiley & Sons, Ltd.: Milton, PA, USA, 2011. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Nunnally, J.C.; Bernstein, I.J. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Hu, L.; Bentler, P. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- McNeish, D.; An, J.; Hancock, G.R. The Thorny Relation between Measurement Quality and Fit Index Cutoffs in Latent Variable Models. J. Pers. Assess. 2018, 100, 43–52. [Google Scholar] [CrossRef]
- Ullman, J.B. Structural Equation Modeling. In Using Multivariate Statistics; Tabachnick, B.G., Fidell, L.S., Eds.; Allyn & Bacon: Needham Heights, MA, USA, 2001; pp. 653–771. [Google Scholar]
- Hewson, C.; Vogel, C.; Laurent, D. Internet Research Methods, 2nd ed.; Sage: London, UK, 2016. [Google Scholar]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during COVID-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef]
- Zaccagni, L.; Toselli, S.; Barbieri, D. Physical activity during COVID-19 lockdown in Italy: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 6416. [Google Scholar] [CrossRef]
- Di Corrado, D.; Magnano, P.; Muzii, B.; Coco, M.; Guarnera, M.; De Lucia, S.; Maldonato, N.M. Effects of social distancing on psychological state and physical activity routines during the COVID-19 pandemic. Sport Sci. Health 2020, 16, 619–624. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Moderate Physical Activity | ||
|---|---|---|
| Before Lockdown | During Lockdown | |
| Never | 25.0% | 25.3% |
| Not every week | 19.0% | 17.2% |
| 1–2 days per week | 25.7% | 20.2% |
| 3–4 days per week | 18.9% | 17.5% |
| 5–6 days per week | 5.2% | 9.0% |
| Every day | 6.2% | 10.8% |
| Total | 100.0% | 100.0% |
| M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Moderate Physical Activity during Lockdown | 3.00 | 1.64 | 1 | |||||||
| 2. Moderate Physical Activity before Lockdown | 2.79 | 1.45 | 0.50 ** | 1 | ||||||
| 3. Well-Being | 3.51 | 1.00 | 0.02 | 0.03 | 1 | |||||
| 4. Emotional Well-Being | 3.75 | 1.18 | 0.09 ** | 0.04 | 0.79 ** | 1 | ||||
| 5. Social Well-Being | 2.71 | 1.16 | −0.05 | −0.02 | 0.84 ** | 0.52 ** | 1 | |||
| 6. Psychological Well-Being | 4.06 | 1.14 | 0.03 | 0.06 | 0.91 ** | 0.66 ** | 0.60 ** | 1 | ||
| 7. Self-Efficacy related to Physical Activity | 3.63 | 0.83 | 0.35 ** | 0.26 ** | −0.07 * | −0.04 | −0.11 ** | −0.02 | 1 | |
| 8. COVID-19 Risk Perception | 3.00 | 1.64 | −0.01 | −0.01 | −0.06 * | −0.10 ** | −0.05 | −0.03 | 0.02 | 1 |
| Moderate Physical Activity | ||
|---|---|---|
| During Lockdown | Two Years after the Lockdown | |
| Never | 21.4% | 26.0% |
| Not every week | 21.2% | 21.0% |
| 1–2 days per week | 29.2% | 21.2% |
| 3–4 days per week | 15.4% | 20.0% |
| 5–6 days per week | 6.2% | 7.7% |
| Every day | 6.6% | 4.1% |
| Total | 100.0% | 100.0% |
| M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Moderate Physical Activity during Lockdown | 2.84 | 1.43 | 1 | |||||||
| 2. Moderate Physical Activity before Lockdown | 2.75 | 1.44 | 0.41 ** | 1 | ||||||
| 3. Well-Being | 3.43 | 0.99 | 0.07 | 0.16 ** | 1 | |||||
| 4. Emotional Well-Being | 3.74 | 1.16 | 0.08 | 0.16 ** | 0.87 ** | 1 | ||||
| 5. Social Well-Being | 2.67 | 1.01 | 0.04 | 0.10 * | 0.85 ** | 0.63 ** | 1 | |||
| 6. Psychological Well-Being | 3.90 | 1.16 | 0.07 | 0.16 ** | 0.93 ** | 0.76 ** | 0.65 ** | 1 | ||
| 7. Self-Efficacy related to Physical Activity | 2.56 | 0.92 | 0.15** | 0.15 ** | −0.13 ** | −0.14 ** | 0.13 ** | 0.08 * | 1 | |
| 8. COVID-19 Risk Perception | 2.82 | 1.00 | −0.09* | −0.14 ** | −0.06 | −0.10 * | 0.01 | −0.06 | −0.05 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donizzetti, A.R. The Relationship between Physical Activity and Psychosocial Well-Being during and after COVID-19 Lockdown. Behav. Sci. 2023, 13, 986. https://doi.org/10.3390/bs13120986
Donizzetti AR. The Relationship between Physical Activity and Psychosocial Well-Being during and after COVID-19 Lockdown. Behavioral Sciences. 2023; 13(12):986. https://doi.org/10.3390/bs13120986
Chicago/Turabian StyleDonizzetti, Anna Rosa. 2023. "The Relationship between Physical Activity and Psychosocial Well-Being during and after COVID-19 Lockdown" Behavioral Sciences 13, no. 12: 986. https://doi.org/10.3390/bs13120986