
Metaplastic Carcinoma of the Breast: Case Series of a Single Institute and Review of the Literature

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Follow-Up and Definitions
2.2. Statistical Analysis
3. Results
3.1. Search Strategy
3.2. Baseline Characteristics
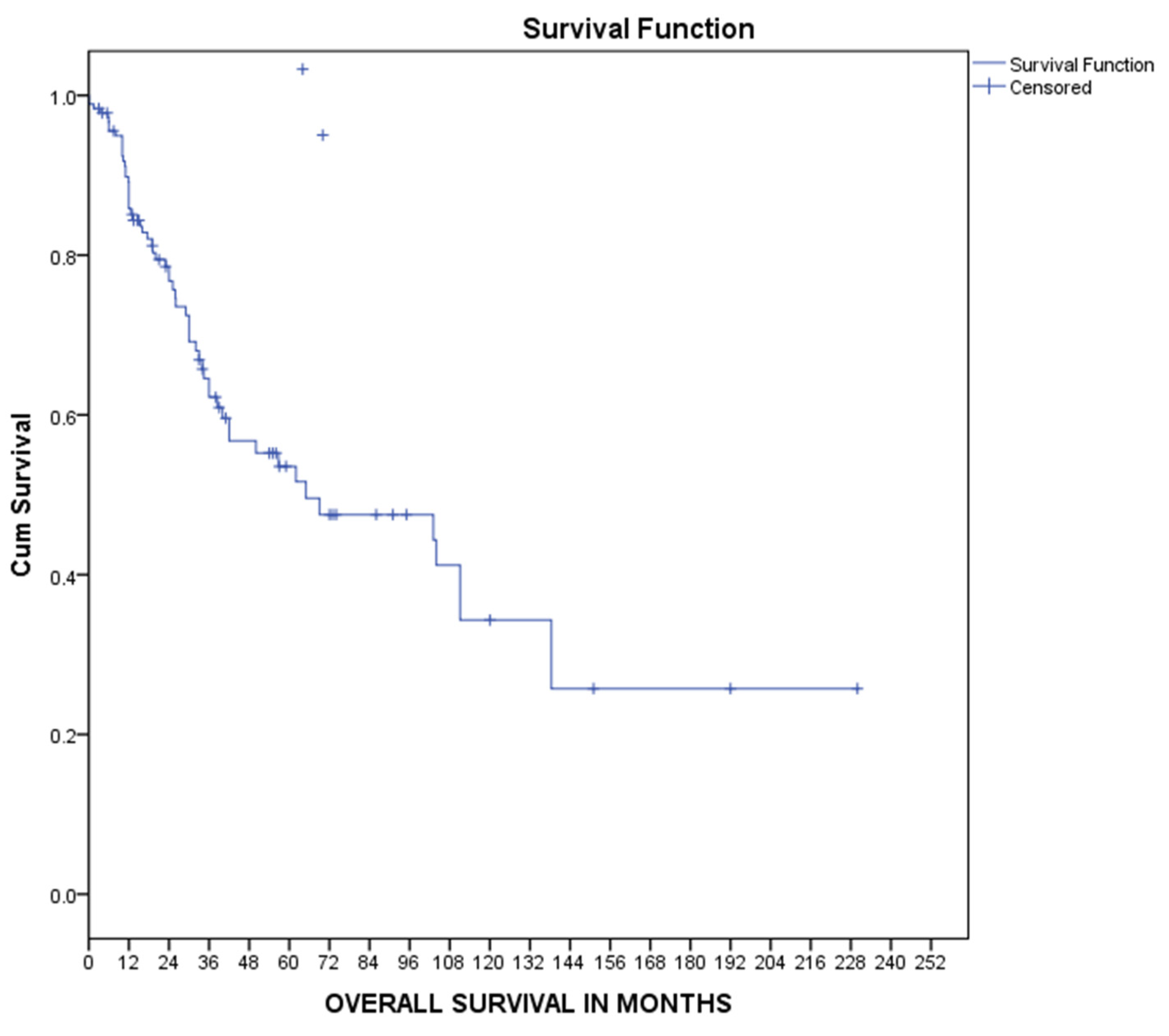
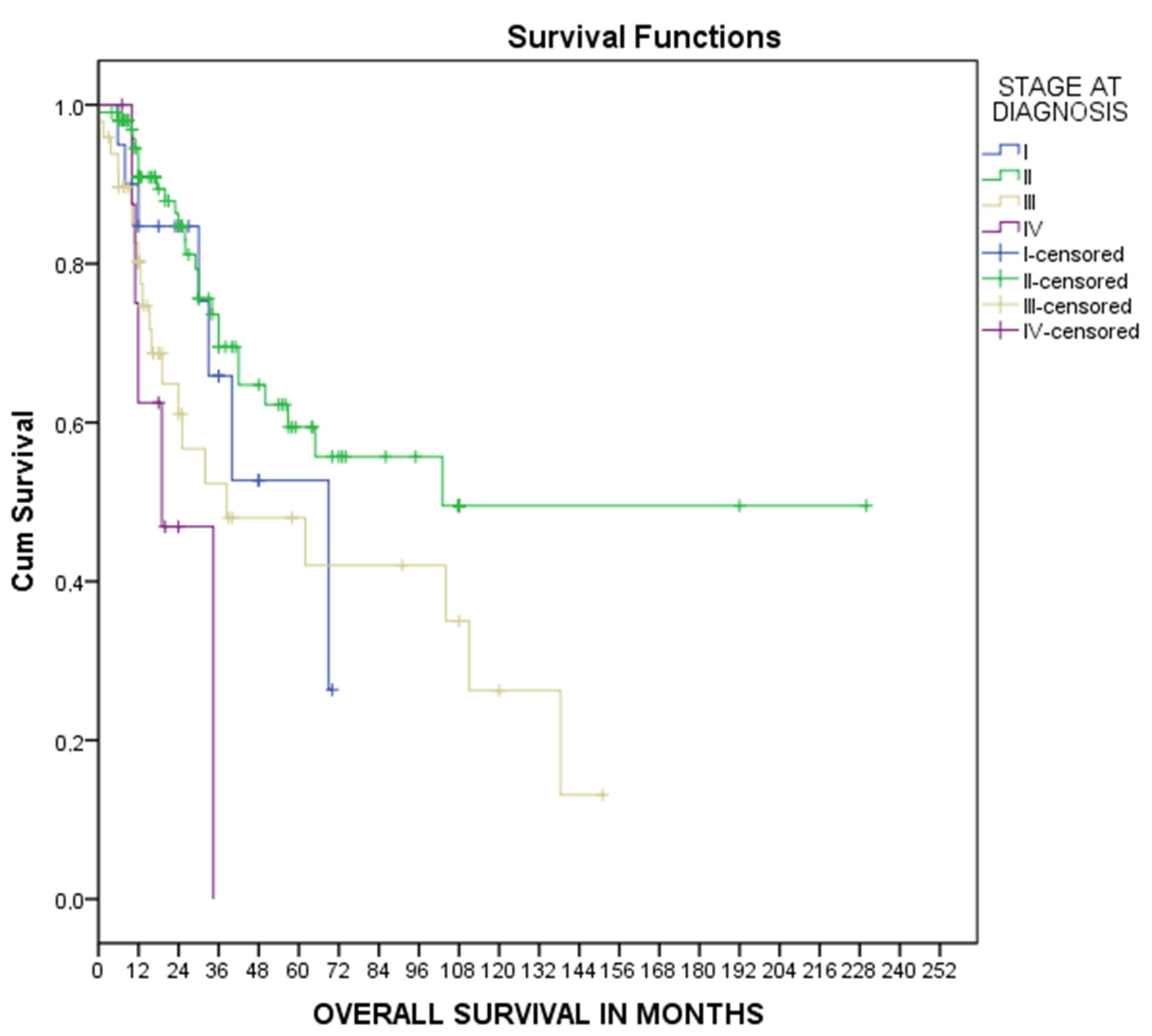
3.3. Overall Survival
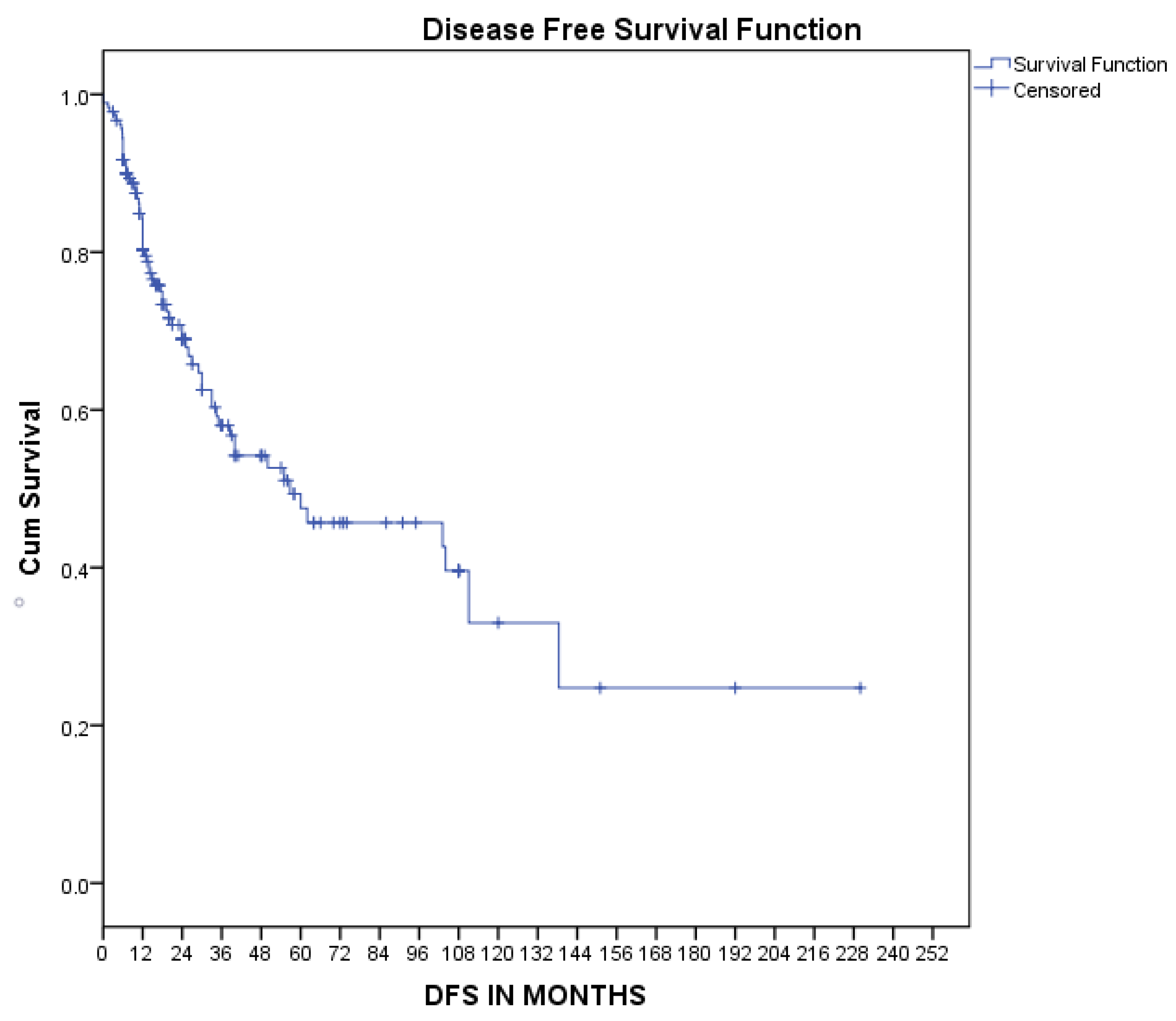
3.4. Disease-Free Survival
4. Discussion
4.1. Classification of MpBC
4.2. Carcinogenesis
4.3. Genetic Mutations on MpBC
4.4. Clinicopathological Features
4.5. Diagnosis of MpBC
4.6. Histopathology
4.7. Treatment
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Yersal, O.; Barutca, S. Biological subtypes of breast cancer: Prognostic and therapeutic implications. World J. Clin. Oncol. 2014, 5, 412–424. [Google Scholar] [CrossRef]
- Denduluri, N.; Somerfield, M.R.; Chavez-MacGregor, M.; Comander, A.H.; Dayao, Z.; Eisen, A.; Freedman, R.A.; Gopalakrishnan, R.; Graff, S.L.; Hassett, M.J.; et al. Selection of Optimal Adjuvant Chemotherapy and Targeted Therapy for Early Breast Cancer: ASCO Guideline Update. J. Clin. Oncol. 2021, 39, 685–693. [Google Scholar] [CrossRef]
- Giordano, S.H.; Temin, S.; Chandarlapaty, S.; Crews, J.R.; Esteva, F.; Kirshner, J.J.; Krop, I.E.; Levinson, J.; Lin, N.U.; Modi, S.; et al. Systemic Therapy for Patients with Advanced Human Epidermal Growth Factor Receptor 2–Positive Breast Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 2736–2740. [Google Scholar] [CrossRef]
- Korde, L.A.; Somerfield, M.R.; Carey, L.A.; Crews, J.R.; Denduluri, N.; Hwang, E.S.; Khan, S.A.; Loibl, S.; Morris, E.A.; Perez, A.; et al. Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline. J. Clin. Oncol. 2021, 39, 1485–1505. [Google Scholar] [CrossRef]
- Tray, N.; Taff, J.; Adams, S. Therapeutic landscape of metaplastic breast cancer. Cancer Treat. Rev. 2019, 79, 101888. [Google Scholar] [CrossRef]
- Pezzi, C.M.; Patel-Parekh, L.; Cole, K.; Franko, J.; Klimberg, V.S.; Bland, K. Characteristics and Treatment of Metaplastic Breast Cancer: Analysis of 892 Cases from the National Cancer Data Base. Ann. Surg. Oncol. 2007, 14, 166–173. [Google Scholar] [CrossRef]
- Jung, S.-Y.; Kim, H.Y.; Nam, B.-H.; Min, S.Y.; Lee, S.J.; Park, C.; Kwon, Y.; Kim, E.-A.; Ko, K.L.; Shin, K.H.; et al. Worse prognosis of metaplastic breast cancer patients than other patients with triple-negative breast cancer. Breast Cancer Res. Treat. 2010, 120, 627–637. [Google Scholar] [CrossRef]
- Bian, T.; Lin, Q.; Wu, Z.; Cui, C.; Qi, C.; Li, L.; Su, X. Metaplastic carcinoma of the breast: Imaging and pathological features. Oncol. Lett. 2016, 12, 3975–3980. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Acar, T.; Acar, N.; Sezgin, G.; Gokova, M.B.; Kucukzeybek, B.B.; Haciyanli, M. What should be treatment approach in metaplastic breast cancer? A report of 5 cases. North. Clin. Istanb. 2018, 5, 365–369. [Google Scholar] [CrossRef]
- M’hamdi, H.A.; Abbad, F.; Rais, H.; Asmouki, H.; Soumani, A.; Khouchani, M.; Belbaraka, R. Rare variant of metaplastic carcinoma of the breast: A case report and review of the literature. J. Med. Case Rep. 2018, 12, 43. [Google Scholar] [CrossRef]
- Amini, A.; Kakkis, J.; Reitherman, R.; Ibarra, J.; Sanati, H. Near-complete pathological response with preoperative chemotherapy in a patient with metaplastic breast carcinoma. Anti-Cancer Drugs 2013, 24, 765–768. [Google Scholar] [CrossRef]
- Anand, M.; Deshmukh, S.D. Metaplastic carcinoma of the breast with rhabdo-myosarcomatous element. Indian J. Med. Paediatr. Oncol. 2014, 35, 117–118. [Google Scholar] [CrossRef]
- Babahabib, M.A.; Chennana, A.; Hachi, A.; Kouach, J.; Moussaoui, D.; Dhayni, M. Metaplastic breast cancer: Report of a case. Pan Afr. Med. J. 2014, 19, 268. [Google Scholar] [CrossRef]
- Bataillon, G.; Collet, J.-F.; Voillemot, N.; Menet, E.; Vincent-Salomon, A.; Klijanienko, J. Fine-Needle Aspiration of Low-Grade Adenosquamous Carcinomas of the Breast: A Report of Three New Cases. Acta Cytol. 2014, 58, 427–431. [Google Scholar] [CrossRef]
- Baum, J.E.; Sung, K.-J.; Tran, H.; Song, W.; Ginter, P.S. Mammary Epithelial-Myoepithelial Carcinoma: Report of a Case with HRAS and PIK3CA Mutations by Next-Generation Sequencing. Int. J. Surg. Pathol. 2019, 27, 441–445. [Google Scholar] [CrossRef]
- Bergeron, A.; Desmoulins, I.; Beltjens, F.; Causeret, S.; Charon-Barra, C.; Martin, E.; Richard, C.; Boidot, R.; Arnould, L. An exceptional metaplastic lobular breast carcinoma diagnosed through exome sequencing. J. Clin. Pathol. 2020, 73, 597–601. [Google Scholar] [CrossRef]
- Bhosale, S.; Kshirsagar, A.; Sulhyan, S.; Jagtap, S.; Nikam, Y. Metaplastic Carcinoma with Predominant Chondrosarcoma of the Right Breast. Case Rep. Oncol. 2010, 3, 277–281. [Google Scholar] [CrossRef]
- Jagtap, S.V.; Bhosale, S.J.; Kshirsagar, A.Y.; Sulhyan, S.R.; Sulhyan, S.R. Matrix-producing metaplastic breast carcinoma—A rare malignancy. Am. J. Case Rep. 2013, 14, 213–215. [Google Scholar] [CrossRef]
- Bigotti, G.; Di Filippo, S.; Di Filippo, F.; Perri, P.; Coli, A. An unusual case of metaplastic breast carcinoma following neoadjuvant chemotherapy. Pathol. Int. 2012, 62, 72–74. [Google Scholar] [CrossRef]
- Brown-Glaberman, U.; Graham, A.; Stopeck, A. A Case of Metaplastic Carcinoma of the Breast Responsive to Chemotherapy with Ifosfamide and Etoposide: Improved Antitumor Response by Targeting Sarcomatous Features. Breast J. 2010, 16, 663–665. [Google Scholar] [CrossRef]
- Carlucci, M.; Iacobellis, M.; Colonna, F.; Marseglia, M.; Gambarotti, M.; Giardina, C.; Bisceglia, M. Metaplastic carcinoma of the breast with dominant squamous and sebaceous differentiation in the primary tumor and osteochondroid metaplasia in a distant metastasis: Report of a case with review of sebaceous differentiation in breast tumors. Int. J. Surg. Pathol. 2012, 20, 284–296. [Google Scholar] [CrossRef]
- Cha, N.; Wang, S.; Lv, M.; Wang, D.-W.; Zhang, X.-J.; Zheng, M.; Tian, L.-X. Breast Metaplastic Squamous Cell Carcinoma Diagnosed with Fine Needle and Core Biopsy: A Case Study. Am. J. Case Rep. 2018, 19, 203–206. [Google Scholar] [CrossRef]
- Chen, I.C.; Lin, C.H.; Huang, C.S.; Lien, H.C.; Hsu, C.; Kuo, W.H.; Lu, Y.S.; Cheng, A.L. Lack of efficacy to systemic chemotherapy for treatment of metaplastic carcinoma of the breast in the modern era. Breast Cancer Res. Treat. 2011, 130, 345–351. [Google Scholar] [CrossRef]
- Chien, T.-J.; Chou, J.-M.; Chang, T.-A.; Lin, C.-P. Successful treatment of biphasic metaplastic sarcomatoid carcinoma of the breast by evaluation of immunohistochemical markers. Hematol./Oncol. Stem Cell Ther. 2010, 3, 89–93. [Google Scholar] [CrossRef]
- Chuthapisith, S.; Warnnissorn, M.; Amornpinyokiat, N.; Pradniwat, K.; Angsusinha, T. Metaplastic carcinoma of the breast with transformation from adenosquamous carcinoma to osteosarcomatoid and spindle cell morphology. Oncol. Lett. 2013, 6, 728–732. [Google Scholar] [CrossRef]
- Conrad, C.; Miller, D.L.; Kaiser, C.; Jauch, K.-W.; Nieß, H.; Huss, R. Spindle Cell Metaplastic Breast Carcinoma with Leiomyoid Differentiation: A Case Report. Breast Care 2011, 6, 230–233. [Google Scholar] [CrossRef]
- Djomehri, S.I.; Gonzalez, M.E.; Leprevost, F.D.V.; Tekula, S.R.; Chang, H.-Y.; White, M.J.; Cimino-Mathews, A.; Burman, B.; Basrur, V.; Argani, P.; et al. Quantitative proteomic landscape of metaplastic breast carcinoma pathological subtypes and their relationship to triple-negative tumors. Nat. Commun. 2020, 11, 1723. [Google Scholar] [CrossRef]
- Gafumbegete, E.; Fahl, U.; Weinhardt, R.; Respondek, M.; Elsharkawy, A.E. Primary osteosarcoma of the breast after complete resection of a metaplastic ossification: A case report. J. Med. Case Rep. 2016, 10, 231. [Google Scholar] [CrossRef]
- Ghilli, M.; Mariniello, D.M.; Fanelli, G.; Cascione, F.; Fontana, A.; Cristaudo, A.; Cilotti, A.; Caligo, A.M.; Manca, G.; Colizzi, L.; et al. Carcinosarcoma of the Breast: An Aggressive Subtype of Metaplastic Cancer. Report of a Rare Case in a Young BRCA-1 Mutated Woman. Clin. Breast Cancer 2017, 17, e31–e35. [Google Scholar] [CrossRef]
- Ghosh, M. Metaplastic Carcinoma Breast: A Clinical Analysis of Nine Cases. J. Clin. Diagn. Res. 2017, 11, XR01–XR03. [Google Scholar] [CrossRef]
- Gultekin, M.; Eren, G.; Babacan, T.; Yildiz, F.; Altundag, K.; Guler, N.; Ozisik, Y.; Yazici, G.; Hurmuz, P.; Gurkaynak, M. Metaplastic Breast Carcinoma: A Heterogeneous Disease. Asian Pac. J. Cancer Prev. 2014, 15, 2851–2856. [Google Scholar] [CrossRef]
- Hasdemir, O.; Tokgöz, S.; Köybaşioğlu, F.; Karabacak, H.; Yücesoy, C.; Imamoğlu, G. Clinicopathological features of metaplastic breast carcinoma. Adv. Clin. Exp. Med. 2018, 27, 509–513. [Google Scholar] [CrossRef]
- Ilhan, E.; Vardar, E.; Ozkok, G.; Sezgin, A.; Sahin, S.; Teker, K.; Postaci, H.; Yildirim, M. A Rare Tumour of the Breast: Carcinosarcoma. J. Clin. Med. Res. 2010, 2, 96–98. [Google Scholar] [CrossRef]
- Kang, Y.; Kang, S.; Li, Q.; Zheng, X. Mixed epithelial and mesenchymal metaplastic carcinoma (carcinosarcoma) of the breast: A case report. Eur. J. Med. Res. 2014, 19, 14. [Google Scholar] [CrossRef]
- Kashyap, R.; Chakkalakkoombil, S.V.; Toi, P.C.; Satheesan, D. Metaplastic breast carcinoma with osseous differentiation presenting as calcified breast mass—Radio-pathological correlation. Breast J. 2020, 26, 1825–1827. [Google Scholar] [CrossRef]
- Kim, I.; Rajamanickam, V.; Bernard, B.; Chun, B.; Wu, Y.; Martel, M.; Sun, Z.; Redmond, W.L.; Sanchez, K.; Basho, R.; et al. A Case Series of Metastatic Metaplastic Breast Carcinoma Treated with Anti-PD-1 Therapy. Front. Oncol. 2021, 11, 635237. [Google Scholar] [CrossRef]
- Kito, K.; Maeda, T.; Ninomiya, K.; Sugita, A.; Sagawa, T.; Matsuoka, K.; Kinoshita, K.; Hyodo, N.; Morita, N.; Furuya, K. HER2-Positive Metaplastic Spindle Cell Carcinoma Associated with Synchronous Bilateral Apocrine Carcinoma of the Breast. Case Rep. Pathol. 2014, 2014, 310829. [Google Scholar] [CrossRef]
- Lai, Y.-C.; Hsu, C.-Y.; Chou, Y.-H.; Tiu, C.-M.; Tseng, L.-M.; Wang, H.-K.; Chiou, H.-J. Sonographic presentations of metaplastic breast cancers. J. Chin. Med. Assoc. 2012, 75, 589–594. [Google Scholar] [CrossRef]
- Leite, C.; Dias, N.; Oliveira, D.; Pinto, R.M.; Vaz, F.C. Metaplastic breast cancer with chondroid differentiation—Case report and literature review. J. Surg. Case Rep. 2021, 2021, rjab113. [Google Scholar] [CrossRef]
- Li, K.; Kang, H.; Wang, Y.; Hai, T.; Wang, B. Development of ipsilateral chest wall spindle cell carcinoma in a patient with invasive ductal breast carcinoma during postoperative adjuvant therapy: A case report. Medicine 2018, 97, e0739. [Google Scholar] [CrossRef]
- Li, S.; Wei, Q.-Z. Metaplastic carcinoma of the right breast and simultaneous giant ovarian teratoma: A case report. Chin. J. Cancer 2012, 31, 500–504. [Google Scholar] [CrossRef]
- Liu, C.H.; Chang, C.; Sy, E.; Lai, H.-W.; Kuo, Y.-L. Metaplastic breast carcinoma with multiple muscle metastasis: A case report. Medicine 2015, 94, e662. [Google Scholar] [CrossRef]
- Liu, L.-Y.; Sheng, S.-H.; Zhang, Z.-Y.; Xu, J.-H. A case of matrix-producing carcinoma of the breast with micoglandular adenosis and review of literature. Int. J. Clin. Exp. Pathol. 2015, 8, 8568–8572. [Google Scholar]
- Luo, K.; Wang, X. Bone in the breast: A case report of a metaplastic breast cancer with osseous differentiation. Radiol. Case Rep. 2021, 16, 136–139. [Google Scholar] [CrossRef]
- Miglietta, L.; Vanella, P.; Rezzo, R.; Carli, F.; Spina, B. A 37-Year-Old Woman with Spindle Cells Metaplastic Breast Carcinoma: A Case Characterized by Very Aggressive Clinical Behavior. Breast J. 2010, 16, 315–317. [Google Scholar] [CrossRef]
- Mitra, B.; Pal, M.; Debnath, S.; Paul, B.; Saha, T.N.; Maiti, A. Primary squamous cell carcinoma of breast with ipsilateral axillary lymph node metastasis: An unusual case. Int. J. Surg. Case Rep. 2011, 2, 194–197. [Google Scholar] [CrossRef]
- Murukutla, S.; Bhatt, V.; Vivekanandarajah, A.; Coomer, C.; Gupta, S. Triple negative mixed metaplastic breast carcinoma with squamous and spindle cells in an 84-year-old woman: A rare entity with unclear management strategy and poor prognosis. BMJ Case Rep. 2012, 2012, bcr1020115044. [Google Scholar] [CrossRef]
- Nahleh, Z.; Ebrahim, V.; Guerrero, R.; Gaur, S.; Ayyappan, A.; Padilla, O. Spindle cell carcinoma of the breast: A case report and discussion. Breast Dis. 2011, 33, 115–119. [Google Scholar] [CrossRef]
- Nonnis, R.; Paliogiannis, P.; Giangrande, D.; Marras, V.; Trignano, M. Low-Grade Fibromatosis-Like Spindle Cell Metaplastic Carcinoma of the Breast: A Case Report and Literature Review. Clin. Breast Cancer 2012, 12, 147–150. [Google Scholar] [CrossRef]
- Ogiya, A.; Takahashi, K.; Sato, M.; Kubo, Y.; Nishikawa, N.; Kikutani, M.; Tadokoro, Y.; Tanaka, K.; Uematsu, T.; Watanabe, J.; et al. Metastatic breast carcinoma of the abdominal wall muscle: A case report. Breast Cancer 2015, 22, 206–209. [Google Scholar] [CrossRef]
- Rajan, R.; Abdullah, N.; Abdullah, N.M.A.; Kassim, A.Y.M. Metaplastic breast carcinoma with upper limb gangrene. Breast Cancer Targets Ther. 2017, 2017, 297–299. [Google Scholar] [CrossRef]
- Rashid, M.U.; Shah, M.A.; Azhar, R.; Syed, A.A.; Amin, A.; Hamann, U. A deleterious BRCA1 mutation in a young Pakistani woman with metaplastic breast carcinoma. Pathol.-Res. Pract. 2011, 207, 583–586. [Google Scholar] [CrossRef]
- Rossi, L.; Paglicci, C.; Caprio, G.; Barberi, S.; Ranieri, E.; Zancla, S.; Rengo, M.; Pagni, P. Matrix-Producing Carcinoma of the Breast: A Case Report. Case Rep. Oncol. 2013, 6, 245–249. [Google Scholar] [CrossRef]
- Seo, T.; Noguchi, E.; Yoshida, M.; Mori, T.; Tanioka, M.; Sudo, K.; Shimomura, A.; Yonemori, K.; Fujiwara, Y.; Tamura, K. Response to Dabrafenib and Trametinib of a Patient with Metaplastic Breast Carcinoma Harboring a BRAF V600E Mutation. Case Rep. Oncol. Med. 2020, 2020, 2518383. [Google Scholar] [CrossRef]
- Shruti, S.; Siraj, F. Matrix-producing metaplastic breast carcinoma—A rare tumor with heterologous elements. Ger. Med. Sci. 2017, 15, Doc17. [Google Scholar] [CrossRef]
- Shui, R.; Bi, R.; Cheng, Y.; Lu, H.; Wang, J.; Yang, W. Matrix-producing carcinoma of the breast in the Chinese population: A clinicopathological study of 13 cases. Pathol. Int. 2011, 61, 415–422. [Google Scholar] [CrossRef]
- Shui, R.; Li, A.; Yang, F.; Zhou, X.; Yu, B.; Xu, X.; Yang, W. Primary squamous cell carcinoma of the breast with unusual basal-HER2 phenotype. Int. J. Clin. Exp. Pathol. 2014, 7, 5203–5209. [Google Scholar]
- Singal, R.; Dalal, A.K.; Dalal, U.; Attri, A.K.; Gupta, S.; Gupta, N. Giant sarcomatoid carcinoma of the breast—A rare case report. Maedica 2011, 6, 201–203. [Google Scholar]
- Sinha, U.; Jha, C.K.; Bharti, S.; Singh, A.; Sinha, R.; Kumar, P. Densely calcified metaplastic carcinoma of breast: An undescribed mammographic feature. Breast J. 2020, 26, 1031–1032. [Google Scholar] [CrossRef]
- Takuwa, H.; Ueno, T.; Ishiguro, H.; Mikami, Y.; Kanao, S.; Takada, M.; Sugie, T.; Toi, M. A case of metaplastic breast cancer that showed a good response to platinum-based preoperative chemotherapy. Breast Cancer 2014, 21, 504–507. [Google Scholar] [CrossRef]
- Tampaki, E.C.; Tampakis, A.; Agrogiannis, G.; Kavantzas, N.; Kontzoglou, K.; Kouraklis, G. A Case of Positive Mixed Epithelial/Mesenchymal Metaplastic Breast Carcinoma (Carcinosarcoma). Towards Novel Therapeutic Targets: Case Report. Onkologie 2013, 36, 506–509. [Google Scholar] [CrossRef]
- Tang, H.; Liu, F.; Li, H.; Huang, X.; Zhao, T. Pleomorphic carcinoma of breast: A case report and review of literature. Int. J. Clin. Exp. Pathol. 2014, 7, 5215–5220. [Google Scholar]
- Tomasicchio, G.; Rizzi, A.; Stucci, L.; Moschetta, M.; Giliberti, G.; Punzo, C. Metaplastic squamous cell breast cancer: A case report and treatment strategy during COVID-19 pandemic. Int. J. Surg. Case Rep. 2021, 79, 405–408. [Google Scholar] [CrossRef]
- Tot, T.; De La Parra, J.J.B.; Bergkvist, L. Metaplastic Carcinoma of the Breast with Neuroectodermal Stromal Component. Pathol. Res. Int. 2011, 2011, 191274. [Google Scholar] [CrossRef]
- Toumi, Z.; Bullen, C.; Tang, A.C.S.; Dalal, N.; Ellenbogen, S. Metaplastic breast carcinoma: A case report and systematic review of the literature. Pathol. Int. 2011, 61, 582–588. [Google Scholar] [CrossRef]
- Tsilimigras, I.D.; Ntanasis-Stathopoulos, I.; Schizas, D.; Bakopoulos, A.; Moris, D.; Stanc, G.-M.; Tentolouris, A.; Nassar, S.; Salla, C. Combined Use of Mammography and FNA Eliminates Pitfalls in the Management of Metaplastic Breast Carcinoma. In Vivo 2017, 31, 737–740. [Google Scholar] [CrossRef]
- Twadell, S.; Schilling, K.; Gleckman, A.; McDonald, K.-A. Imaging characteristics of metaplastic breast cancer with osteoblastic differentiation. BMJ Case Rep. 2020, 13, e235050. [Google Scholar] [CrossRef]
- Victoor, J.; Bourgain, C.; Borght, S.V.; Bempt, I.V.; De Rop, C.; Floris, G. Fibromatosis-like metaplastic carcinoma: A case report and review of the literature. Diagn. Pathol. 2020, 15, 20. [Google Scholar] [CrossRef]
- Wu, H.-B.; Zhang, A.-L.; Wang, W.; Li, H. Expression of hormone receptors in low-grade adenosquamous carcinoma of the breast: A case report. Medicine 2017, 96, e8785. [Google Scholar] [CrossRef]
- Yahaya, J.; Mremi, A. Metaplastic carcinoma of breast: A report of two cases. Oxf. Med. Case Rep. 2020, 2020, omaa070. [Google Scholar] [CrossRef]
- Yang, M.-H.; Chen, I.-C.; Lu, Y.-S. PI3K inhibitor provides durable response in metastatic metaplastic carcinoma of the breast: A hidden gem in the BELLE-4 study. J. Formos. Med. Assoc. 2019, 118, 1333–1338. [Google Scholar] [CrossRef]
- Zhang, L.; Comertpay, S.; Shimizu, D.; DeMay, R.M.; Carbone, M.; Honda, S.A.; Eaves, J.M.M. Axillary Metaplastic Breast Carcinoma with Ipsilateral Pectoral Invasive Ductal Carcinoma: An Unusual Presentation. Case Rep. Oncol. Med. 2014, 2014, 938509. [Google Scholar] [CrossRef]
- Zhu, H.; Li, K.; Dong, D.-D.; Fu, J.; Liu, D.-D.; Wang, L.; Xu, G.; Song, L.-H. Spindle cell metaplastic carcinoma of breast: A clinicopathological and immunohistochemical analysis. Asia-Pac. J. Clin. Oncol. 2017, 13, e72–e78. [Google Scholar] [CrossRef]
- Mao, J.; Hu, J.; Zhang, Y.; Shen, J.; Dong, F.; Zhang, X.; Ming, J.; Huang, T.; Run, X. Single Hormone Receptor-Positive Metaplastic Breast Cancer: Similar Outcome as Triple-Negative Subtype. Front. Endocrinol. 2021, 12, 628939. [Google Scholar] [CrossRef]
- Gradishar, W.J.; Anderson, B.O.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Blair, S.L.; Burstein, H.J.; Dang, C.; Elias, A.D.; et al. Breast Cancer, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 452–478. [Google Scholar] [CrossRef]
- Sinn, H.P.; Kreipe, H. A Brief Overview of the WHO Classification of Breast Tumors, 4th Edition, Focusing on Issues and Updates from the 3rd Edition. Breast Care 2013, 8, 149–154. [Google Scholar] [CrossRef]
- Yamaguchi, R.; Horii, R.; Maeda, I.; Suga, S.; Makita, M.; Iwase, T.; Oguchi, M.; Ito, Y.; Akiyama, F. Clinicopathologic study of 53 metaplastic breast carcinomas: Their elements and prognostic implications. Hum. Pathol. 2010, 41, 679–685. [Google Scholar] [CrossRef]
- Wang, M.; He, X.; Chang, Y.; Sun, G.; Thabane, L. A sensitivity and specificity comparison of fine needle aspiration cytology and core needle biopsy in evaluation of suspicious breast lesions: A systematic review and meta-analysis. Breast 2017, 31, 157–166. [Google Scholar] [CrossRef]
- Alan, O.; Telli, T.A.; Ercelep, O.; Hasanov, R.; Simsek, E.T.; Mutis, A.; Ones, T.; Kaya, H.; Yumuk, P.F. A case of primary squamous cell carcinoma of the breast with pathologic complete response after neoadjuvant chemotherapy. Curr. Probl. Cancer 2019, 43, 308–311. [Google Scholar] [CrossRef]
- Hennessy, B.T.; Giordano, S.H.; Broglio, K.; Duan, Z.; Trent, J.; Buchholz, T.A.; Babiera, G.; Hortobagyi, G.N.; Valero, V. Biphasic metaplastic sarcomatoid carcinoma of the breast. Ann. Oncol. 2006, 17, 605–613. [Google Scholar] [CrossRef]
- Schmid, P.; Cortes, J.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2020, 382, 810–821. [Google Scholar] [CrossRef]
- Joneja, U.; Vranic, S.; Swensen, J.; Feldman, R.; Chen, W.; Kimbrough, J.; Xiao, N.; Reddy, S.; Palazzo, J.; Gatalica, Z. Comprehensive profiling of metaplastic breast carcinomas reveals frequent overexpression of programmed death-ligand 1. J. Clin. Pathol. 2017, 70, 255–259. [Google Scholar] [CrossRef]
- Tray, N.; Taff, J.; Singh, B.; Suh, J.; Ngo, N.; Kwa, M.; Troxel, A.B.; Chae, Y.K.; Kurzrock, R.; Patel, S.P.; et al. Metaplastic breast cancers: Genomic profiling, mutational burden and tumor-infiltrating lymphocytes. Breast 2019, 44, 29–32. [Google Scholar] [CrossRef]
- Tung, N.M.; Zakalik, D.; Somerfield, M.R.; for the Hereditary Breast Cancer Guideline Expert Panel. Adjuvant PARP Inhibitors in Patients with High-Risk Early-Stage HER2-Negative Breast Cancer and Germline BRCA Mutations: ASCO Hereditary Breast Cancer Guideline Rapid Recommendation Update. J. Clin. Oncol. 2021, 39, 2959–2961. [Google Scholar] [CrossRef]
- Henneman, L.; van Miltenburg, M.H.; Michalak, E.M.; Braumuller, T.M.; Jaspers, J.E.; Drenth, A.P.; de Korte-Grimmerink, R.; Gogola, E.; Szuhai, K.; Schlicker, A.; et al. Selective resistance to the PARP inhibitor olaparib in a mouse model for BRCA1-deficient metaplastic breast cancer. Proc. Natl. Acad. Sci. USA 2015, 112, 8409–8414. [Google Scholar] [CrossRef]
- Hu, J.; Zhang, H.; Dong, F.; Zhang, X.; Wang, S.; Ming, J.; Huang, T. Metaplastic breast cancer: Treatment and prognosis by molecular subtype. Transl. Oncol. 2021, 14, 101054. [Google Scholar] [CrossRef]
- Basho, R.K.; Yam, C.; Gilcrease, M.; Murthy, R.K.; Helgason, T.; Karp, D.D.; Meric-Bernstam, F.; Hess, K.R.; Valero, V.; Albarracin, C.; et al. Comparative Effectiveness of an mTOR-Based Systemic Therapy Regimen in Advanced, Metaplastic and Nonmetaplastic Triple-Negative Breast Cancer. Oncologist 2018, 23, 1300–1309. [Google Scholar] [CrossRef]
- Lan, T.; Lu, Y.; Zheng, R.; Shao, X.; Luo, H.; He, J.; Yang, H.; Xu, H.; Wang, X.; Hu, Z. The Role of Adjuvant Chemotherapy in Metaplastic Breast Carcinoma: A Competing Risk Analysis of the SEER Database. Front. Oncol. 2021, 11, 572230. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (years), mean (SD) | 55 (14.7) |
| TNM stage, n (%) | |
| I | 20 (9.8) |
| II | 120 (58.5) |
| III | 52(25.4) |
| IV | 13 (6.3) |
| ER > 1% n/N (%) | 19/180 (10.6) |
| PR > 1% n/N (%) | 18/180 (10) |
| HER2 enriched n/N (%) | 17/191 (8.9) |
| Ki 67 > 15% n/N (%) | 32/40 (68.4) |
| Surgery n/N (%) | 186/189 (98.4) |
| Chemotherapy n/N (%) | 152/176 (86.4) |
| Radiation n/N (%) | 88/154 (57.1) |
| Univariate Cox Regression | Multivariate Cox Regression | |||||
|---|---|---|---|---|---|---|
| Patient Characteristic | HR | 95% CI | p | HR | 95% CI | p |
| Age | 1 | 0.99–1.03 | 0.4 | 1 | 0.96–1.02 | 0.73 |
| TNM stage | 1.6 | 1.13–2.36 | 0.01 | 1.5 | 1.04–2.28 | 0.03 |
| ER > 1% | 1 | 0.43–2.35 | 0.99 | |||
| PR > 1% | 1 | 0.43–2.35 | 0.99 | |||
| HER2 enriched | 0.58 | 0.21–1.61 | 0.3 | |||
| Triple-negative phenotype | 1.08 | 0.57–2.05 | 0.82 | |||
| Histology * | 1.14 | 0.90–1.45 | 0.28 | |||
| Ki 67 > 15% | 0.87 | 0.32–2.38 | 0.79 | |||
| Surgery | 0.06 | 0.02–0.2 | <0.001 | 0.11 | 0.02–0.54 | 0.01 |
| Chemotherapy | 0.68 | 0.32–1.38 | 0.23 | |||
| Radiation | 1.02 | 0.63–2.28 | 0.58 | |||
| Univariate Cox Regression | Multivariate Cox Regression | |||||
|---|---|---|---|---|---|---|
| Patient Characteristic | HR | 95% CI | p | HR | 95% CI | p |
| Age | 1.01 | 0.99–1.04 | 1.17 | 1.01 | 0.98–1.03 | 0.59 |
| TNM stage | 1.3 | 0.85–2 | 0.23 | 1.36 | 0.84–2.21 | 0.21 |
| ER > 1% | 0.42 | 0.11–1.73 | 0.23 | |||
| PR > 1% | 0.69 | 0.21–2.24 | 0.53 | |||
| HER2 enriched | 0.41 | 0.1–1.7 | 0.22 | |||
| Triple-negative phenotype | 2.08 | 0.81–5.33 | 0.13 | |||
| Histology * | 1.15 | 0.90–1.46 | 0.26 | |||
| Ki 67 > 15% | 0.82 | 0.31–2.18 | 0.69 | |||
| Surgery | 0.05 | 0.01–0.23 | <0.001 | 0.17 | 0.98–1.03 | 0.06 |
| Chemotherapy | 0.45 | 0.21–0.94 | 0.03 | 0.19 | 0.23–1.34 | 0.55 |
| Radiation | 1.72 | 0.87–3.4 | 0.12 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papatheodoridi, A.; Papamattheou, E.; Marinopoulos, S.; Ntanasis-Stathopoulos, I.; Dimitrakakis, C.; Giannos, A.; Kaparelou, M.; Liontos, M.; Dimopoulos, M.-A.; Zagouri, F. Metaplastic Carcinoma of the Breast: Case Series of a Single Institute and Review of the Literature. Med. Sci. 2023, 11, 35. https://doi.org/10.3390/medsci11020035
Papatheodoridi A, Papamattheou E, Marinopoulos S, Ntanasis-Stathopoulos I, Dimitrakakis C, Giannos A, Kaparelou M, Liontos M, Dimopoulos M-A, Zagouri F. Metaplastic Carcinoma of the Breast: Case Series of a Single Institute and Review of the Literature. Medical Sciences. 2023; 11(2):35. https://doi.org/10.3390/medsci11020035
Chicago/Turabian StylePapatheodoridi, Alkistis, Eleni Papamattheou, Spyridon Marinopoulos, Ioannis Ntanasis-Stathopoulos, Constantine Dimitrakakis, Aris Giannos, Maria Kaparelou, Michalis Liontos, Meletios-Athanasios Dimopoulos, and Flora Zagouri. 2023. "Metaplastic Carcinoma of the Breast: Case Series of a Single Institute and Review of the Literature" Medical Sciences 11, no. 2: 35. https://doi.org/10.3390/medsci11020035