
Immunohistochemical and Molecular Genetic Analysis of Canine Digital Mast Cell Tumours
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Histopathology
2.2. Immunohistochemistry
2.3. Screening for Mutations in Exons 8, 9, 11 and 14 of c-kit
2.4. Statistical Analysis
3. Results
3.1. Case Description
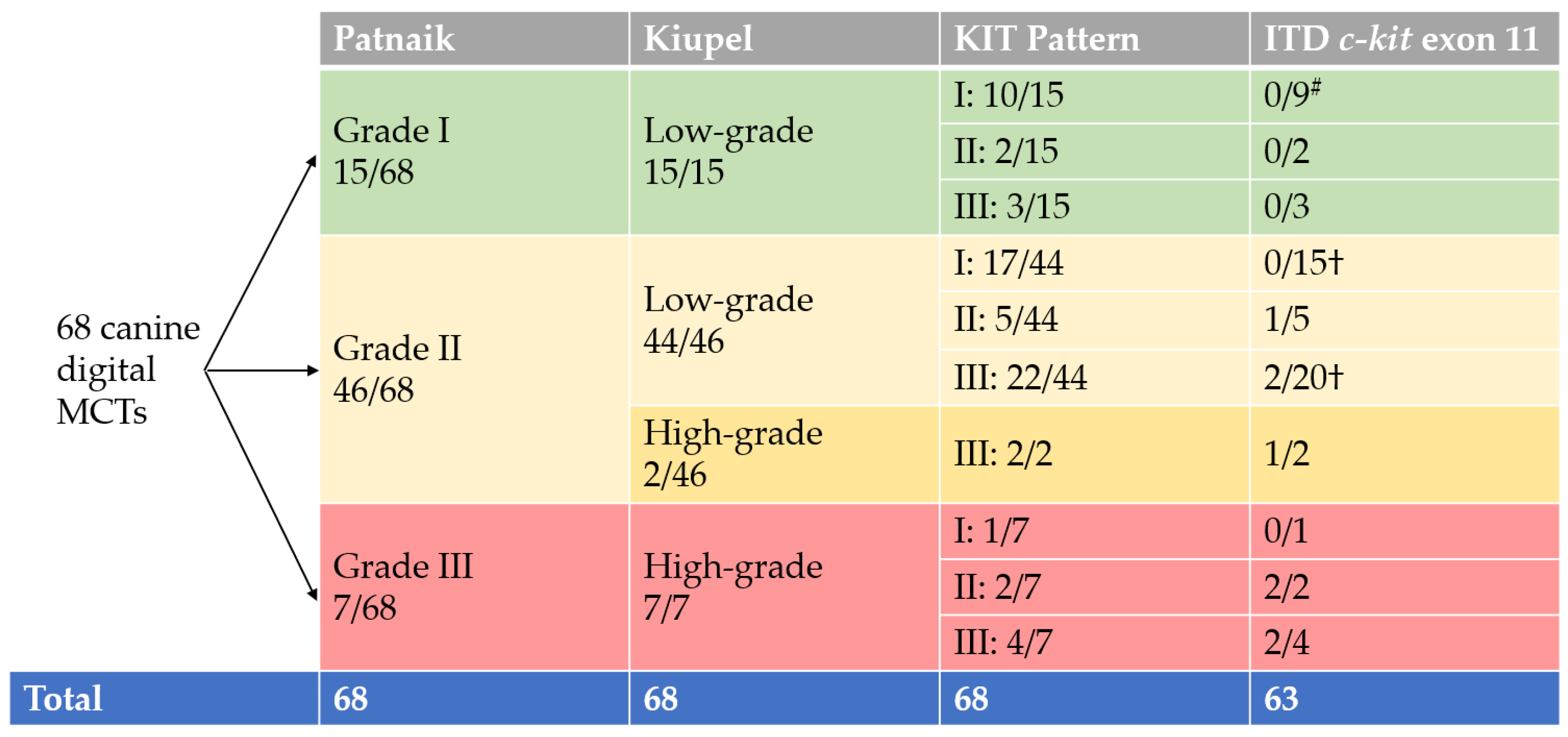
3.2. Grading and Pathological Findings
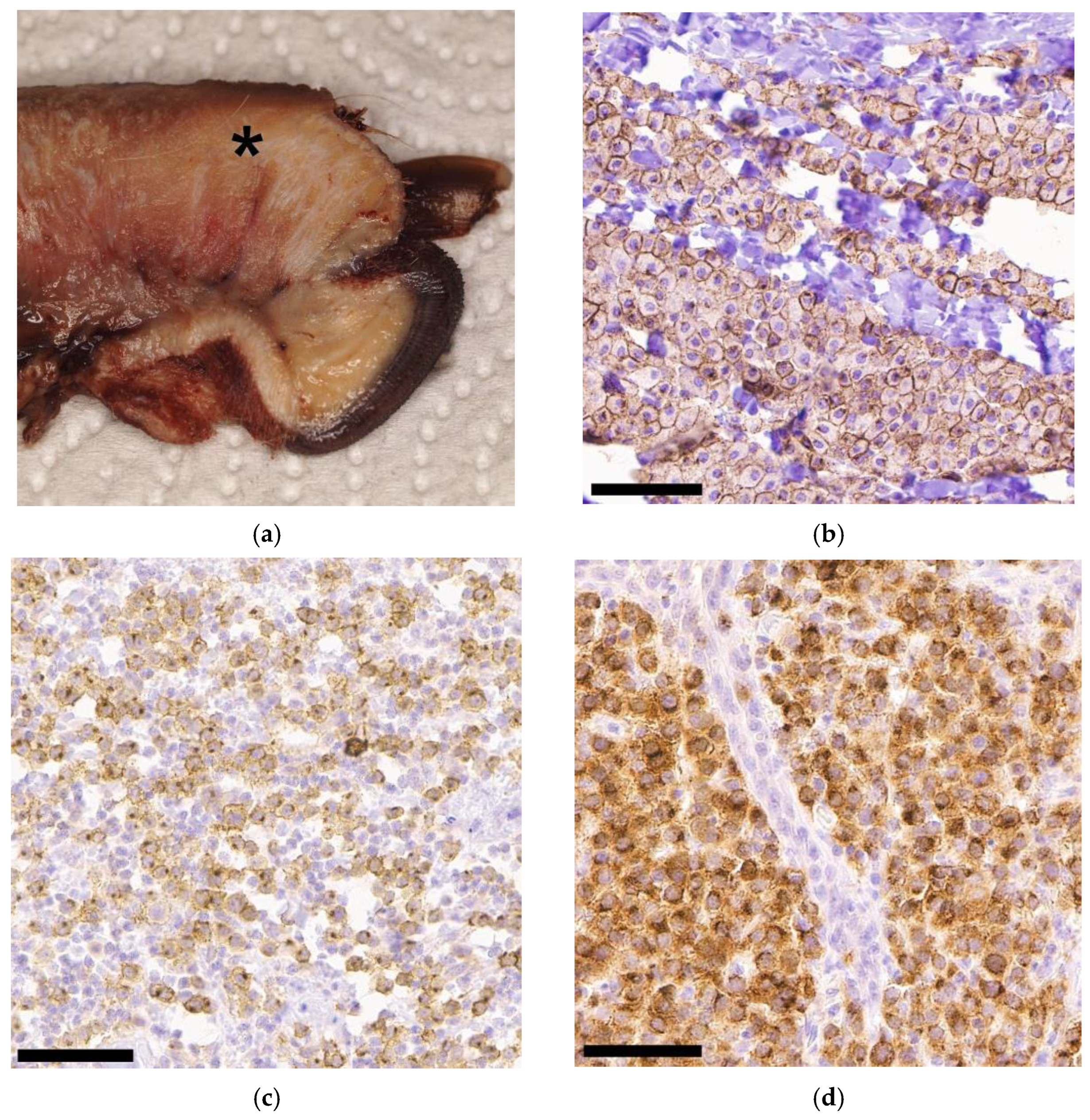
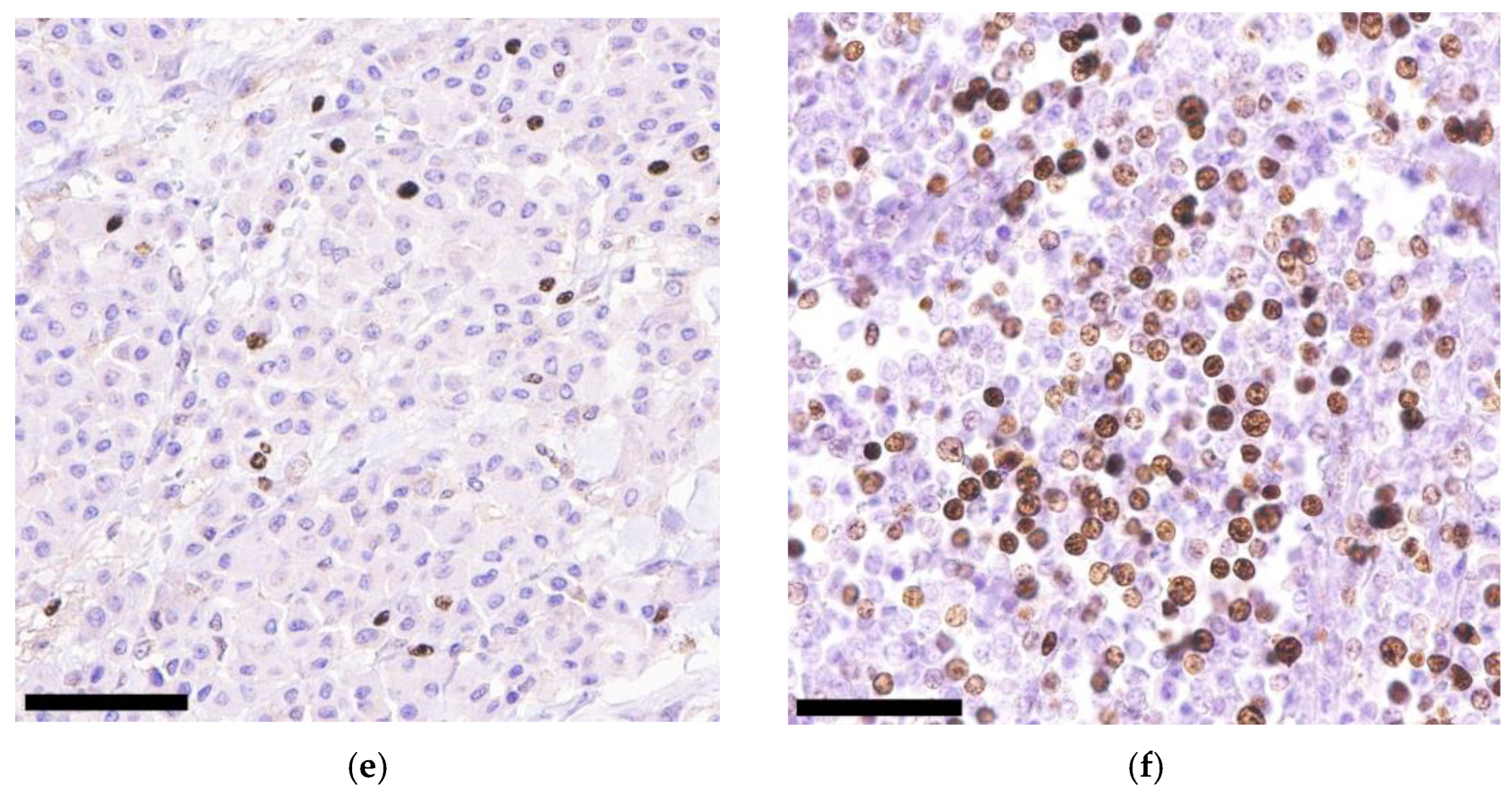
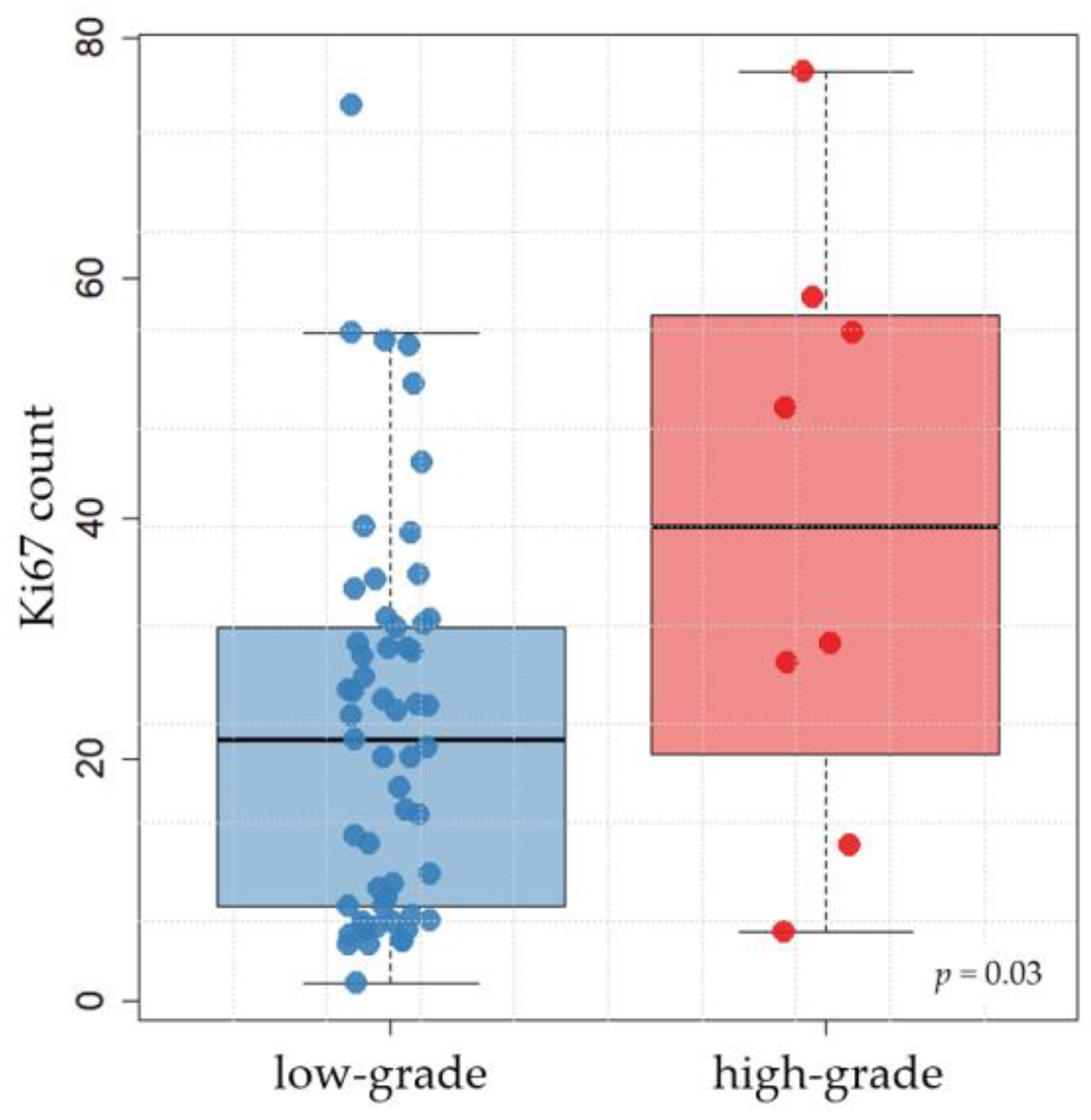
3.3. Immunohistochemical KIT and Ki67 Expression
3.4. c-kit Mutation Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bostock, D.E. Neoplasms of the skin and subcutaneous tissues in dogs and cats. Br. Vet. J. 1986, 142, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Tamlin, V.S.; Bottema, C.D.K.; Peaston, A.E. Comparative aspects of mast cell neoplasia in animals and the role of KIT in prognosis and treatment. Vet. Med. Sci. 2020, 6, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Aupperle-Lellbach, H.; Grassinger, J.M.; Floren, A.; Törner, K.; Beitzinger, C.; Loesenbeck, G.; Müller, T. Tumour Incidence in Dogs in Germany: A Retrospective Analysis of 109,616 Histopathological Diagnoses (2014–2019). J. Comp. Pathol. 2022, 198, 33–55. [Google Scholar] [CrossRef] [PubMed]
- Śmiech, A.; Łopuszyński, W.; Ślaska, B.; Bulak, K.; Jasik, A. Occurrence and Distribution of Canine Cutaneous Mast Cell Tumour Characteristics Among Predisposed Breeds. J. Vet. Res. 2019, 63, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Blackwood, L.; Murphy, S.; Buracco, P.; de Vos, J.P.; de Fornel-Thibaud, P.; Hirschberger, J.; Kessler, M.; Pastor, J.; Ponce, F.; Savary-Bataille, K.; et al. European consensus document on mast cell tumours in dogs and cats. Vet. Comp. Oncol. 2012, 10, e1–e29. [Google Scholar] [CrossRef] [PubMed]
- Welle, M.M.; Bley, C.R.; Howard, J.; Rüfenacht, S. Canine mast cell tumours: A review of the pathogenesis, clinical features, pathology and treatment. Vet. Dermatol. 2008, 19, 321–339. [Google Scholar] [CrossRef]
- Pierini, A.; Lubas, G.; Gori, E.; Binanti, D.; Millanta, F.; Marchetti, V. Epidemiology of Breed-Related Mast Cell Tumour Occurrence and Prognostic Significance of Clinical Features in a Defined Population of Dogs in West-Central Italy. Vet. Sci. 2019, 6, 53. [Google Scholar] [CrossRef]
- Patnaik, A.K.; Ehler, W.J.; MacEwen, E.G. Canine cutaneous mast cell tumor: Morphologic grading and survival time in 83 dogs. Vet. Pathol. 1984, 21, 469–474. [Google Scholar] [CrossRef]
- Rigas, K.; Biasoli, D.; Polton, G.; Finotello, R.; Murphy, S.; Di Palma, S.; Starkey, M.; Verganti, S. Mast cell tumours in dogs less than 12 months of age: A multi-institutional retrospective study. J. Small Anim. Pract. 2020, 61, 449–457. [Google Scholar] [CrossRef]
- Kiupel, M.; Webster, J.D.; Bailey, K.L.; Best, S.; DeLay, J.; Detrisac, C.J.; Fitzgerald, S.D.; Gamble, D.; Ginn, P.E.; Goldschmidt, M.H.; et al. Proposal of a 2-tier histologic grading system for canine cutaneous mast cell tumors to more accurately predict biological behavior. Vet. Pathol. 2011, 48, 147–155. [Google Scholar] [CrossRef]
- Northrup, N.C.; Harmon, B.G.; Gieger, T.L.; Brown, C.A.; Carmichael, K.P.; Garcia, A.; Latimer, K.S.; Munday, J.S.; Rakich, P.M.; Richey, L.J.; et al. Variation among pathologists in histologic grading of canine cutaneous mast cell tumors. J. Vet. Diagn. Investig. 2005, 17, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Avallone, G.; Rasotto, R.; Chambers, J.K.; Miller, A.D.; Behling-Kelly, E.; Monti, P.; Berlato, D.; Valenti, P.; Roccabianca, P. Review of Histological Grading Systems in Veterinary Medicine. Vet. Pathol. 2021, 58, 809–828. [Google Scholar] [CrossRef] [PubMed]
- Freytag, J.O.; Queiroz, M.R.; Govoni, V.M.; Pereira, I.V.A.; Pulz, L.H.; de Francisco Strefezzi, R.; Queiroga, F.L.; Cogliati, B. Prognostic value of immunohistochemical markers in canine cutaneous mast cell tumours: A systematic review and meta-analysis. Vet. Comp. Oncol. 2021, 19, 529–540. [Google Scholar] [CrossRef] [PubMed]
- Scholzen, T.; Gerdes, J. The Ki-67 protein: From the known and the unknown. J. Cell Physiol. 2000, 182, 311–322. [Google Scholar] [CrossRef]
- Esteban-Villarrubia, J.; Soto-Castillo, J.J.; Pozas, J.; San Román-Gil, M.; Orejana-Martín, I.; Torres-Jiménez, J.; Carrato, A.; Alonso-Gordoa, T.; Molina-Cerrillo, J. Tyrosine Kinase Receptors in Oncology. Int. J. Mol. Sci. 2020, 21, 8529. [Google Scholar] [CrossRef]
- Preziosi, R.; Morini, M.; Sarli, G. Expression of the KIT protein (CD117) in primary cutaneous mast cell tumors of the dog. J. Vet. Diagn. Investig. 2004, 16, 554–561. [Google Scholar] [CrossRef]
- Da Gil Costa, R.M.; Matos, E.; Rema, A.; Lopes, C.; Pires, M.A.; Gärtner, F. CD117 immunoexpression in canine mast cell tumours: Correlations with pathological variables and proliferation markers. BMC Vet. Res. 2007, 3, 19. [Google Scholar] [CrossRef]
- London, C.A. Tyrosine kinase inhibitors in veterinary medicine. Top. Companion Anim. Med. 2009, 24, 106–112. [Google Scholar] [CrossRef]
- London, C.A.; Malpas, P.B.; Wood-Follis, S.L.; Boucher, J.F.; Rusk, A.W.; Rosenberg, M.P.; Henry, C.J.; Mitchener, K.L.; Klein, M.K.; Hintermeister, J.G.; et al. Multi-center, placebo-controlled, double-blind, randomized study of oral toceranib phosphate (SU11654), a receptor tyrosine kinase inhibitor, for the treatment of dogs with recurrent (either local or distant) mast cell tumor following surgical excision. Clin. Cancer Res. 2009, 15, 3856–3865. [Google Scholar] [CrossRef]
- Hahn, K.A.; Ogilvie, G.; Oglivie, G.; Rusk, T.; Devauchelle, P.; Leblanc, A.; Legendre, A.; Powers, B.; Leventhal, P.S.; Kinet, J.-P.; et al. Masitinib is safe and effective for the treatment of canine mast cell tumors. J. Vet. Intern. Med. 2008, 22, 1301–1309. [Google Scholar] [CrossRef]
- Webster, J.D.; Yuzbasiyan-Gurkan, V.; Kaneene, J.B.; Miller, R.; Resau, J.H.; Kiupel, M. The role of c-KIT in tumorigenesis: Evaluation in canine cutaneous mast cell tumors. Neoplasia 2006, 8, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Vozdova, M.; Kubickova, S.; Fictum, P.; Cernohorska, H.; Fröhlich, J.; Rubes, J. Mutation and methylation status of KIT and TP53 in canine cutaneous and subcutaneous mast cell tumours. Vet. Comp. Oncol. 2020, 18, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Vozdova, M.; Kubickova, S.; Pal, K.; Fröhlich, J.; Fictum, P.; Rubes, J. Recurrent gene mutations detected in canine mast cell tumours by next generation sequencing. Vet. Comp. Oncol. 2020, 18, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Vozdova, M.; Kubickova, S.; Fictum, P.; Fröhlich, J.; Jelinek, F.; Rubes, J. Prevalence and prognostic value of c-kit and TP53 mutations in canine mast cell tumours. Vet. J. 2019, 247, 71–74. [Google Scholar] [CrossRef]
- Nakano, Y.; Kobayashi, M.; Bonkobara, M.; Takanosu, M. Identification of a secondary mutation in the KIT kinase domain correlated with imatinib-resistance in a canine mast cell tumor. Vet. Immunol. Immunopathol. 2017, 188, 84–88. [Google Scholar] [CrossRef]
- Brocks, B.A.W.; Bertram, C.A.; Bartel, A.; Kirpensteijn, J.; Collins-Webb, A.; Catlin, C.; Thaiwong, T.; Kiupel, M. Internal Tandem Duplication of Exon 8 of c-kit Is Associated with Longer Total Survival in Canine Cutaneous Mast Cell Tumors. Vet. Pathol. 2021, 58, 315–324. [Google Scholar] [CrossRef]
- Gentilini, F.; Turba, M.E.; Dally, C.; Takanosu, M.; Kurita, S.; Bonkobara, M. The secondary KIT mutation p.Ala510Val in a cutaneous mast cell tumour carrying the activating mutation p.Asn508Ile confers resistance to masitinib in dogs. BMC Vet. Res. 2020, 16, 64. [Google Scholar] [CrossRef]
- Mochizuki, H.; Thomas, R.; Moroff, S.; Breen, M. Genomic profiling of canine mast cell tumors identifies DNA copy number aberrations associated with KIT mutations and high histological grade. Chromosome Res. 2017, 25, 129–143. [Google Scholar] [CrossRef]
- Tamlin, V.S.; Bottema, C.D.K.; Woolford, L.; Dobson, E.C.; Kessell, A.E.; Peaston, A.E. Canine mast cell tumours part I: Clinical and survival outcomes. Vet. Med. Sci. 2022, 8, 1409–1420. [Google Scholar] [CrossRef]
- Webster, J.D.; Yuzbasiyan-Gurkan, V.; Miller, R.A.; Kaneene, J.B.; Kiupel, M. Cellular proliferation in canine cutaneous mast cell tumors: Associations with c-KIT and its role in prognostication. Vet. Pathol. 2007, 44, 298–308. [Google Scholar] [CrossRef]
- Bae, S.; Milovancev, M.; Bartels, C.; Irvin, V.L.; Tuohy, J.L.; Townsend, K.L.; Leeper, H. Histologically low-grade, yet biologically high-grade, canine cutaneous mast cell tumours: A systematic review and meta-analysis of individual participant data. Vet. Comp. Oncol. 2020, 18, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Kiupel, M.; Webster, J.D.; Miller, R.A.; Kaneene, J.B. Impact of tumour depth, tumour location and multiple synchronous masses on the prognosis of canine cutaneous mast cell tumours. J. Vet. Med. A Physiol. Pathol. Clin. Med. 2005, 52, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Marino, D.J.; Matthiesen, D.T.; Stefanacci, J.D.; Moroff, S.D. Evaluation of dogs with digit masses: 117 cases (1981–1991). J. Am. Vet. Med. Assoc. 1995, 207, 726–728. [Google Scholar] [PubMed]
- Wobeser, B.K.; Kidney, B.A.; Powers, B.E.; Withrow, S.J.; Mayer, M.N.; Spinato, M.T.; Allen, A.L. Diagnoses and clinical outcomes associated with surgically amputated canine digits submitted to multiple veterinary diagnostic laboratories. Vet. Pathol. 2007, 44, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Grassinger, J.M.; Floren, A.; Müller, T.; Cerezo-Echevarria, A.; Beitzinger, C.; Conrad, D.; Törner, K.; Staudacher, M.; Aupperle-Lellbach, H. Digital Lesions in Dogs: A Statistical Breed Analysis of 2912 Cases. Vet. Sci. 2021, 8, 136. [Google Scholar] [CrossRef]
- Conrad, D.; Kehl, A.; Beitzinger, C.; Metzler, T.; Steiger, K.; Pfarr, N.; Fischer, K.; Klopfleisch, R.; Aupperle-Lellbach, H. Molecular Genetic Investigation of Digital Melanoma in Dogs. Vet. Sci. 2022, 9, 56. [Google Scholar] [CrossRef] [PubMed]
- Meuten, D.J.; Moore, F.M.; Donovan, T.A.; Bertram, C.A.; Klopfleisch, R.; Foster, R.A.; Smedley, R.C.; Dark, M.J.; Milovancev, M.; Stromberg, P.; et al. International Guidelines for Veterinary Tumor Pathology: A Call to Action. Vet. Pathol. 2021, 58, 766–794. [Google Scholar] [CrossRef]
- Abrams, B.E.; Putterman, A.B.; Ruple, A.; Wavreille, V.; Selmic, L.E. Variability in tumor margin reporting for soft tissue sarcoma and cutaneous mast cell tumors in dogs: A systematic review. Vet. Surg. 2021, 50, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Karbe, G.T.; Davis, E.; Runge, J.J.; Brown, D.C.; Holt, D.E. Evaluation of scar revision after inadequate primary excision of cutaneous mast cell tumors in 85 dogs (2000–2013). Vet. Surg. 2021, 50, 807–815. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Heinze, G.; Ploner, M.; Jiricka, L. Logistf: Firth’s Bias-Reduced Logistic Regression. R Package Version 1.24.1. 2022. Available online: https://CRAN.R-project.org/package=logistf (accessed on 11 March 2023).
- Venables, W.N.; Ripley, B.D. Modern Applied Statistics with S, 4th ed.; Springer: New York, NY, USA, 2002; ISBN 0-387-95457-0. [Google Scholar]
- Zemke, D.; Yamini, B.; Yuzbasiyan-Gurkan, V. Mutations in the juxtamembrane domain of c-KIT are associated with higher grade mast cell tumors in dogs. Vet. Pathol. 2002, 39, 529–535. [Google Scholar] [CrossRef]
- Horta, R.S.; Lavalle, G.E.; Monteiro, L.N.; Souza, M.C.C.; Cassali, G.D.; Araújo, R.B. Assessment of Canine Mast Cell Tumor Mortality Risk Based on Clinical, Histologic, Immunohistochemical, and Molecular Features. Vet. Pathol. 2018, 55, 212–223. [Google Scholar] [CrossRef] [PubMed]
- McNiel, E.A.; Prink, A.L.; O’Brien, T.D. Evaluation of risk and clinical outcome of mast cell tumours in pug dogs. Vet. Comp. Oncol. 2006, 4, 2–8. [Google Scholar] [CrossRef]
- Reynolds, B.D.; Thomson, M.J.; O’Connell, K.; Morgan, E.J.; Gummow, B. Patient and tumour factors influencing canine mast cell tumour histological grade and mitotic index. Vet. Comp. Oncol. 2019, 17, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Biasoli, D.; Compston-Garnett, L.; Ricketts, S.L.; Birand, Z.; Courtay-Cahen, C.; Fineberg, E.; Arendt, M.; Boerkamp, K.; Melin, M.; Koltookian, M.; et al. A synonymous germline variant in a gene encoding a cell adhesion molecule is associated with cutaneous mast cell tumour development in Labrador and Golden Retrievers. PLoS Genet. 2019, 15, e1007967. [Google Scholar] [CrossRef] [PubMed]
- Stefanello, D.; Buracco, P.; Sabattini, S.; Finotello, R.; Giudice, C.; Grieco, V.; Iussich, S.; Tursi, M.; Scase, T.; Di Palma, S.; et al. Comparison of 2- and 3-category histologic grading systems for predicting the presence of metastasis at the time of initial evaluation in dogs with cutaneous mast cell tumors: 386 cases (2009–2014). J. Am. Vet. Med. Assoc. 2015, 246, 765–769. [Google Scholar] [CrossRef]
- Cruz, V.S.; Borges, J.C.A.; Nepomuceno, L.L.; Gonçalves, P.A.M.; Prado, Y.C.L.; Bianchi, C.; Fioravanti, M.C.S.; Araújo, E.G. Histological classification and expression of markers of canine mast cell tumors. Vet. World 2020, 13, 1627–1634. [Google Scholar] [CrossRef]
- de Nardi, A.B.; Dos Santos Horta, R.; Fonseca-Alves, C.E.; de Paiva, F.N.; Linhares, L.C.M.; Firmo, B.F.; Ruiz Sueiro, F.A.; de Oliveira, K.D.; Lourenço, S.V.; de Francisco Strefezzi, R.; et al. Diagnosis, Prognosis and Treatment of Canine Cutaneous and Subcutaneous Mast Cell Tumors. Cells 2022, 11, 618. [Google Scholar] [CrossRef]
- Thamm, D.H.; Weishaar, K.M.; Charles, J.B.; Ehrhart, E.J. Phosphorylated KIT as a predictor of outcome in canine mast cell tumours treated with toceranib phosphate or vinblastine. Vet. Comp. Oncol. 2020, 18, 169–175. [Google Scholar] [CrossRef]
- Romansik, E.M.; Reilly, C.M.; Kass, P.H.; Moore, P.F.; London, C.A. Mitotic index is predictive for survival for canine cutaneous mast cell tumors. Vet. Pathol. 2007, 44, 335–341. [Google Scholar] [CrossRef]
- Giantin, M.; Vascellari, M.; Morello, E.M.; Capello, K.; Vercelli, A.; Granato, A.; Lopparelli, R.M.; Nassuato, C.; Carminato, A.; Martano, M.; et al. c-KIT messenger RNA and protein expression and mutations in canine cutaneous mast cell tumors: Correlations with post-surgical prognosis. J. Vet. Diagn. Investig. 2012, 24, 116–126. [Google Scholar] [CrossRef]
- Chen, P.; Marconato, L.; Sabattini, S.; Kiupel, M. Mutations in Exons 8 and 11 of c-kit Gene in Canine Subcutaneous Mast Cell Tumors and Their Association with Cell Proliferation. Vet. Sci. 2022, 9, 493. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antigen | Species | Supplier | Dilution | Pre-Treatment |
|---|---|---|---|---|
| KIT/CD117 | rabbit | Dako 1 (#A4502) | 1:150 | EDTA buffer |
| Ki67 | mouse | Dako 1 (#M7240) | 1:200 | EDTA buffer |
| c-kit Exon | Primer | Sequence |
|---|---|---|
| 8 | Forward Reverse | 5′-GGT GAG GTG TTC CAG CAG TC-3′ 5′-CCT TCC CTC GTG CAC ATT A-3′ |
| 9 | Forward Reverse | 5′-ACT CGT CTC TGT CAC CGT CTG GAA-3′ 5′-ATG GCA GGC AGA GCC TAA ACA TCC-3′ |
| 11 | Forward Reverse | 5′-CCC ATG TAT GAA GTA CAG TGG AAG-3′ 5′-GTT CCC TAA AGT CAT TGT TAC ACG-3′ |
| 14 | Forward Reverse | 5′-AGC CTG CTA AGT ATT TGC CTT ATC AAT-3′ 5′-TGG CAC CTC GAA GTA CCT CTG T-3′ |
| Parameter | ITD c-kit Exon 11 |
|---|---|
| Patnaik grading | p = 0.002 |
| Kiupel grading | p < 0.001 |
| Mitotic count | p < 0.001 |
| Ki67 count | p = 0.006 |
| KIT pattern | p = 0.018 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conrad, D.; Kehl, A.; Müller, T.; Klopfleisch, R.; Aupperle-Lellbach, H. Immunohistochemical and Molecular Genetic Analysis of Canine Digital Mast Cell Tumours. Animals 2023, 13, 1694. https://doi.org/10.3390/ani13101694
Conrad D, Kehl A, Müller T, Klopfleisch R, Aupperle-Lellbach H. Immunohistochemical and Molecular Genetic Analysis of Canine Digital Mast Cell Tumours. Animals. 2023; 13(10):1694. https://doi.org/10.3390/ani13101694
Chicago/Turabian StyleConrad, David, Alexandra Kehl, Tobias Müller, Robert Klopfleisch, and Heike Aupperle-Lellbach. 2023. "Immunohistochemical and Molecular Genetic Analysis of Canine Digital Mast Cell Tumours" Animals 13, no. 10: 1694. https://doi.org/10.3390/ani13101694