
Effects of Chemotherapy on Hematological Parameters and CD4+/CD8+ Ratio in Cats with Mediastinal Lymphoma and Seropositive to Feline Leukemia Virus




Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approvals and Animals
2.2. Measurement of CD4+/CD8+ Ratio
2.3. Statistical Analysis
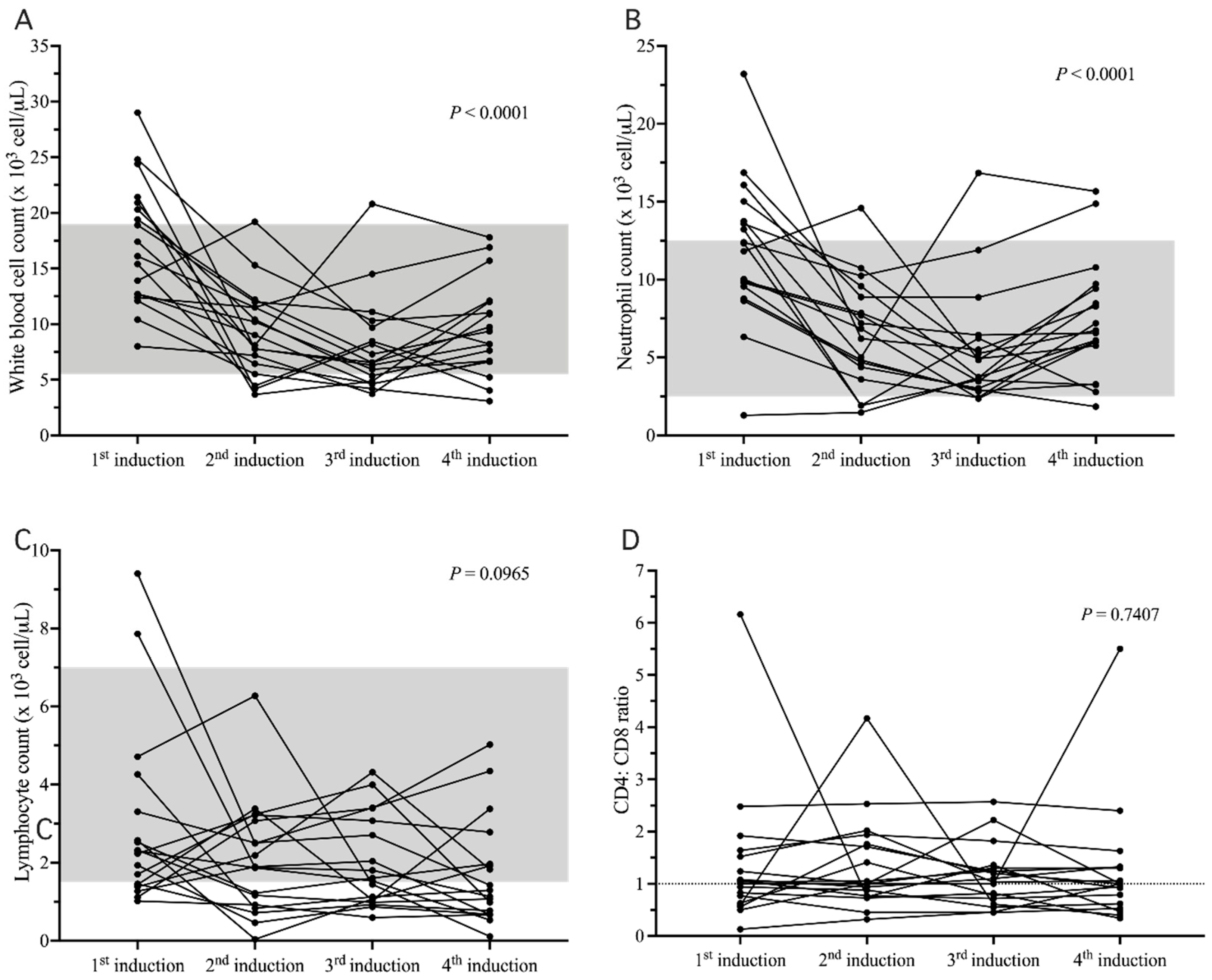
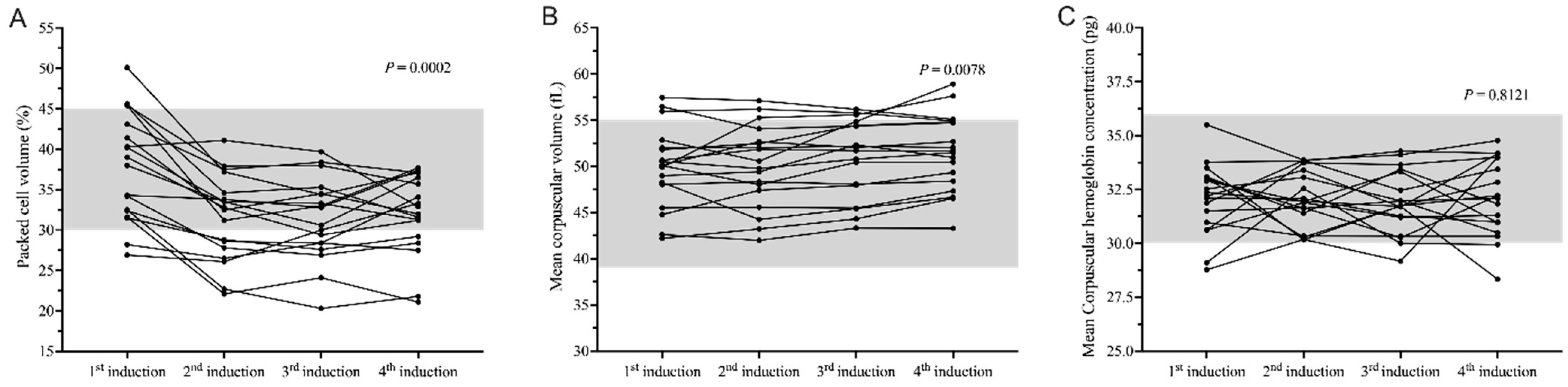
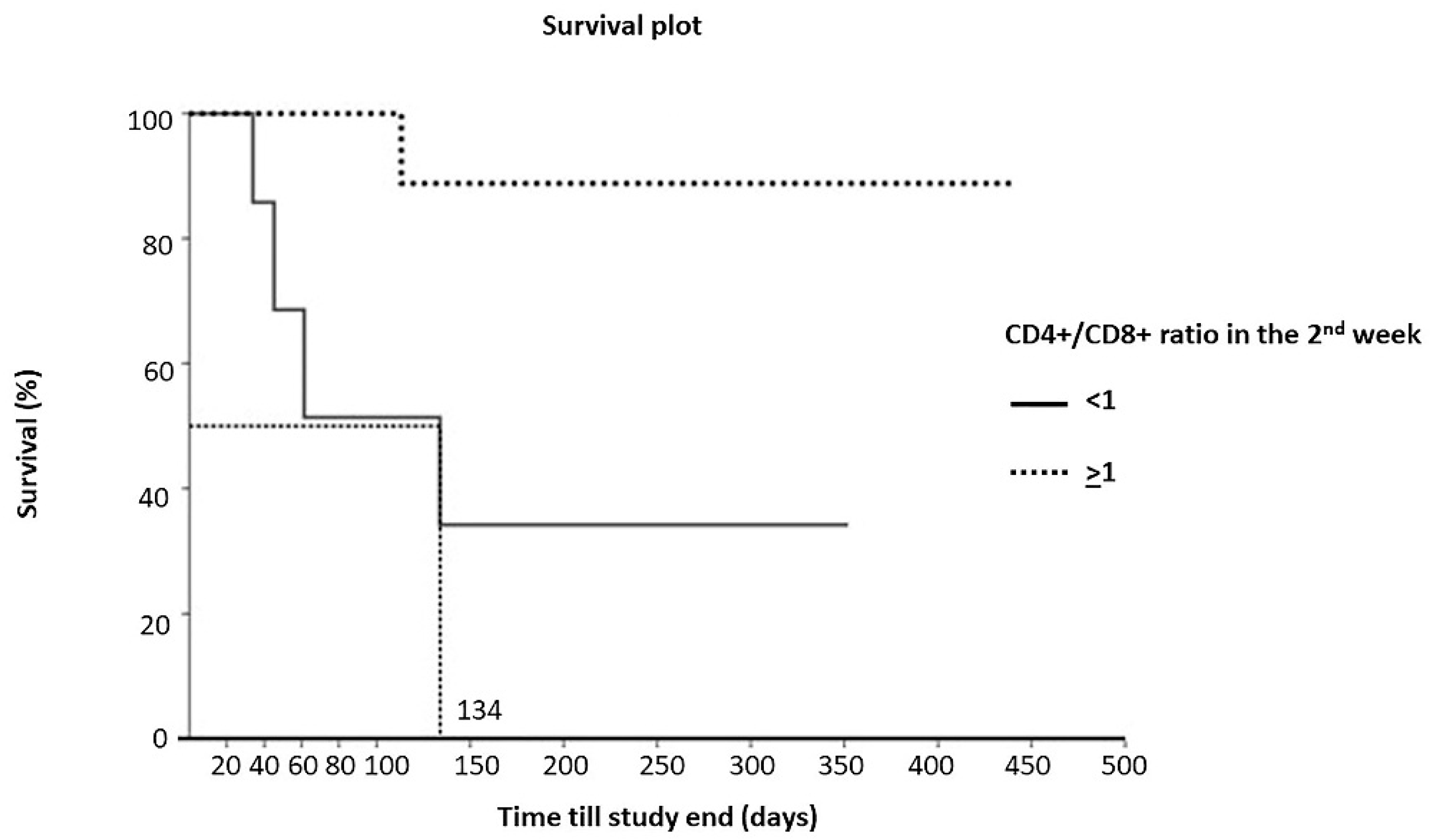
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Collette, S.A.; Allstadt, S.D.; Chon, E.M.; Vernau, W.; Smith, A.N.; Garrett, L.D.; Choy, K.; Rebhun, R.B.; Rodriguez, C.O., Jr.; Skorupski, K.A. Treatment of feline intermediate- to high-grade lymphoma with a modified university of Wisconsin-Madison protocol: 119 cases (2004–2012). Vet. Comp. Oncol. 2016, 14 (Suppl. 1), 136–146. [Google Scholar] [CrossRef]
- Fabrizio, F.; Calam, A.E.; Dobson, J.M.; A Middleton, S.; Murphy, S.; Taylor, S.S.; Schwartz, A.; Stell, A.J. Feline mediastinal lymphoma: A retrospective study of signalment, retroviral status, response to chemotherapy and prognostic indicators. J. Feline Med. Surg. 2013, 16, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Krick, E.L.; Moore, R.H.; Cohen, R.B.; Sorenmo, K.U. Prognostic significance of weight changes during treatment of feline lymphoma. J. Feline Med. Surg. 2011, 13, 976–983. [Google Scholar] [CrossRef]
- Ettinger, S.N. Principles of treatment for feline lymphoma. Clin. Tech. Small Anim. Pract. 2003, 18, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Couto, C.G. Advances in the treatment of the cat with lymphoma in practice. J. Feline Med. Surg. 2000, 2, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Couto, C.G. What is new on feline lymphoma? J. Feline Med. Surg. 2001, 3, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Sukhumavasi, W.; Bellosa, M.L.; Lucio-Forster, A.; Liotta, J.L.; Lee, A.; Pornmingmas, P.; Chungpivat, S.; Mohammed, H.O.; Lorentzen, L.; Dubey, J.; et al. Serological survey of Toxoplasma gondii, Dirofilaria immitis, Feline Immunodeficiency Virus (FIV) and Feline Leukemia Virus (FeLV) infections in pet cats in Bangkok and vicinities, Thailand. Vet. Parasitol. 2012, 188, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Horta, R.S.; Souza, L.M.; Sena, B.V.; Almeida, I.O.; Jaretta, T.A.; Pimenta, M.M.; Reche Junior, A. LOPH: A novel chemotherapeutic protocol for feline high-grade multicentric or mediastinal lymphoma, developed in an area endemic for feline leukemia virus. J. Feline Med. Surg. 2021, 23, 86–97. [Google Scholar] [CrossRef]
- Vail, D.M.; Moore, A.S.; Ogilvie, G.K.; Volk, L.M. Feline Lymphoma (145 Cases): Proliferation Indices, Cluster of Differentiation 3 Immunoreactivity, and Their Association with Prognosis in 90 Cats. J. Vet. Intern. Med. 1998, 12, 349–354. [Google Scholar] [CrossRef] [Green Version]
- Teske, E.; Van Lankveld, A.J.; Rutteman, G.R. Intraperitoneal antineoplastic drug delivery: Experience with a cyclophosphamide, vincristine and prednisolone protocol in cats with malignant lymphoma. Vet. Comp. Oncol. 2012, 12, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Mooney, S.C.; Hayes, A.A.; MacEwen, E.G.; Matus, R.E.; Geary, A.; Shurgot, B.A. Treatment and prognostic factors in lymphoma in cats: 103 cases (1977–1981). J. Am. Vet. Med. Assoc. 1989, 194, 696–702. [Google Scholar]
- Chen, X.; Cao, Z.; Zhang, Y.; Li, J.; Wang, S.; Du, J.; Liao, L. Fuzheng Qingjie Granules Inhibit Growth of Hepatoma Cells via Inducing Mitochondria-Mediated Apoptosis and Enhancing Immune Function. Integr. Cancer Ther. 2017, 16, 329–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, W.Y.; Yee, C.; Greenberg, P.D. Adoptive therapy with CD8+ T cells: It may get by with a little help from its friends. J. Clin. Investig. 2002, 110, 1415–1417. [Google Scholar] [CrossRef]
- Toes, R.E.; Ossendorp, F.; Offringa, R.; Melief, C.J. CD4 T Cells and Their Role in Antitumor Immune Responses. J. Exp. Med. 1999, 189, 753–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pardoll, D.M.; Topalian, S.L. The role of CD4+ T cell responses in antitumor immunity. Curr. Opin. Immunol. 1998, 10, 588–594. [Google Scholar] [CrossRef]
- Wikby, A.; Nilsson, B.-O.; Forsey, R.; Thompson, J.; Strindhall, J.; Löfgren, S.; Ernerudh, J.; Pawelec, G.; Ferguson, F.; Johansson, B. The immune risk phenotype is associated with IL-6 in the terminal decline stage: Findings from the Swedish NONA immune longitudinal study of very late life functioning. Mech. Ageing Dev. 2006, 127, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Novotney, C.; Housman, J.; Davidson, M.G.; Nasisse, M.P.; Jeng, C.-R.; Davis, W.C.; Tompkins, M.B. Lymphocyte population changes in cats naturally infected with feline immunodeficiency virus. AIDS 1990, 4, 1213–1218. [Google Scholar] [CrossRef]
- Pedersen, N.C.; Torten, M.; Rideout, B.; Sparger, E.; Tonachini, T.; Luciw, P.A.; Ackley, C.; Levy, N.; Yamamoto, J. Feline leukemia virus infection as a potentiating cofactor for the primary and secondary stages of experimentally induced feline immunodeficiency virus infection. J. Virol. 1990, 64, 598–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, P.; Normansell, D.E.; Innes, D.J.; Hess, C.E. Lymphocyte subsets in normal bone marrow. Blood 1986, 67, 1600–1606. [Google Scholar] [CrossRef] [Green Version]
- Bofill, M.; Janossy, G.; Lee, C.A.; Macdonald-Burns, D.; Phillips, A.N.; Sabin, C.; Timms, A.; Johnson, M.A.; Kernoff, P.B.A. Laboratory control values for CD4 and CD8 T lymphocytes. Implications for HIV-1 diagnosis. Clin. Exp. Immunol. 1992, 88, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Wahlin, B.E.; Sander, B.; Christensson, B.; Ostenstad, B.; Holte, H.; Brown, P.D.; Sundstrom, C.; Kimby, E. Entourage: The immune microenvironment following follicular lymphoma. Blood Cancer J. 2012, 2, e52. [Google Scholar] [CrossRef] [PubMed]
- Terry, A.; Callanan, J.J.; Fulton, R.; Jarrett, O.; Neil, J.C. Molecular analysis of tumours from feline immunodeficiency virus (FIV)-infected cats: An indirect role for FIV? Int. J. Cancer 1995, 61, 227–232. [Google Scholar] [CrossRef]
- Teske, E.; van Straten, G.; van Noort, R.; Rutteman, G.R. Chemotherapy with cyclophosphamide, vincristine, and prednisolone (COP) in cats with malignant lymphoma: New results with an old protocol. J. Vet. Intern. Med. 2002, 16, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Gomez, A.D.; Collado, V.M.; Miró, G.; Martín, S.; Benítez, L.; Doménech, A. Clinical and Hematological Follow-Up of Long-Term Oral Therapy with Type-I Interferon in Cats Naturally Infected with Feline Leukemia Virus or Feline Immunodeficiency Virus. Animals 2020, 10, 1464. [Google Scholar] [CrossRef] [PubMed]
- Limmer, S.; Eberle, N.; Nerschbach, V.; Nolte, I.; Betz, D. Treatment of feline lymphoma using a 12-week, maintenance-free combination chemotherapy protocol in 26 cats. Vet. Comp. Oncol. 2014, 14 (Suppl. 1), 21–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louwerens, M.; London, C.A.; Pedersen, N.C.; Lyons, L.A. Feline Lymphoma in the Post–Feline Leukemia Virus Era. J. Vet. Intern. Med. 2005, 19, 329. [Google Scholar] [CrossRef]
- Taylor, S.S.; Goodfellow, M.; Browne, W.J.; Walding, B.; Murphy, S.; Tzannes, S.; Gerou-Ferriani, M.; Schwartz, A.; Dobson, J.M. Feline extranodal lymphoma: Response to chemotherapy and survival in 110 cats. J. Small Anim. Pract. 2009, 50, 584–592. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.; Frimberger, A.; Chan, C. Dosage escalation of intravenous cyclophosphamide in cats with cancer. Vet. J. 2018, 242, 39–43. [Google Scholar] [CrossRef]
- Hartmann, K. Clinical Aspects of Feline Retroviruses: A Review. Viruses 2012, 4, 2684–2710. [Google Scholar] [CrossRef] [Green Version]
- Hofmann-Lehmann, R.; Holznagel, E.; Ossent, P.; Lutz, H. Parameters of disease progression in long-term experimental feline retrovirus (feline immunodeficiency virus and feline leukemia virus) infections: Hematology, clinical chemistry, and lymphocyte subsets. Clin. Diagn. Lab. Immunol. 1997, 4, 33–42. [Google Scholar] [CrossRef] [Green Version]
- Doménech, A.; Miró, G.; Collado, V.M.; Ballesteros, N.; Sanjosé, L.; Escolar, E.; Martin, S.; Gomez, A.D. Use of recombinant interferon omega in feline retrovirosis: From theory to practice. Vet. Immunol. Immunopathol. 2011, 143, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Leal, R.O.; Gil, S.; Sepulveda, N.; McGahie, D.; Duarte, A.; Niza, M.; Tavares, L. Monitoring acute phase proteins in retrovirus infected cats undergoing feline interferon-ω therapy. J. Small Anim. Pract. 2013, 55, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Gil, S.; Leal, R.O.; Duarte, A.; McGahie, D.; Sepúlveda, N.; Siborro, I.; Cravo, J.; Cartaxeiro, C.; Tavares, L.M. Relevance of feline interferon omega for clinical improvement and reduction of concurrent viral excretion in retrovirus infected cats from a rescue shelter. Res. Vet. Sci. 2013, 94, 753–763. [Google Scholar] [CrossRef] [PubMed]
- De Mari, K.; Maynard, L.; Sanquer, A.; Lebreux, B.; Eun, H.M. Therapeutic effects of recombinant feline interferon-omega on feline leukemia virus (FeLV)-infected and FeLV/feline immunodeficiency virus (FIV)-coinfected symptomatic cats. J. Vet. Intern. Med. 2004, 18, 477–482. [Google Scholar] [CrossRef]
- Hernberg, M.; Muhonen, T.; Pyrhönen, S. Can the CD4+/CD8+ ratio predict the outcome of interferon-α therapy for renal cell carcinoma? Ann. Oncol. 1997, 8, 71–77. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | |
|---|---|
| Median age (years) | 2.5 |
| Gender | |
| Male | 72.22% (n = 13) |
| Female | 27.78% (n = 5) |
| Breed | |
| Domestic short hair | 100% (n = 18) |
| Viral status | |
| FeLV antigen positive | 100% (n = 18) |
| Tumor anatomic location | |
| Mediastinum | 100% (n = 18) |
| Cytological evaluation | |
| Lymphoblastic lymphoma | 100% (n = 18) |
| Clinical complaint | |
| Dyspnea | 100% (n = 18) |
| Anorexia | 100% (n = 18) |
| Regurgitation | 17% (n = 3) |
| Coughing | 6% (n = 1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaroensong, T.; Piamwaree, J.; Sattasathuchana, P. Effects of Chemotherapy on Hematological Parameters and CD4+/CD8+ Ratio in Cats with Mediastinal Lymphoma and Seropositive to Feline Leukemia Virus. Animals 2022, 12, 223. https://doi.org/10.3390/ani12030223
Jaroensong T, Piamwaree J, Sattasathuchana P. Effects of Chemotherapy on Hematological Parameters and CD4+/CD8+ Ratio in Cats with Mediastinal Lymphoma and Seropositive to Feline Leukemia Virus. Animals. 2022; 12(3):223. https://doi.org/10.3390/ani12030223
Chicago/Turabian StyleJaroensong, Tassanee, Juthaporn Piamwaree, and Panpicha Sattasathuchana. 2022. "Effects of Chemotherapy on Hematological Parameters and CD4+/CD8+ Ratio in Cats with Mediastinal Lymphoma and Seropositive to Feline Leukemia Virus" Animals 12, no. 3: 223. https://doi.org/10.3390/ani12030223