1. Introduction
Canine apocrine gland adenocarcinoma of the anal sac (AGASAC) is a malignant epithelial tumour arising from the glands of the anal sac [
1,
2]. A genetic and breed predisposition for English Cocker Spaniels has been identified; however, sporadic disease occurs across all breeds [
3,
4]. Metastasis is frequent, often affecting the locoregional lymph nodes. Distant spread occurs widely and can involve the abdominal and thoracic viscera and bone [
2,
5,
6,
7]. Paraneoplastic hypercalcaemia, through the effect of tumour-produced parathyroid-hormone-related polypeptide [
8,
9,
10], is present in 25–51% of dogs at diagnosis and can result in life-threatening complications [
5]. Reported metastatic rates at diagnosis and overall survival times are variable, ranging from 26% [
11] to 79% [
5], and 212 days [
2] to 1237 days [
11], respectively, depending upon the clinical stage and treatment received [
2,
5,
12,
13,
14,
15,
16,
17,
18,
19]. Multimodal therapy involving two or more treatment modalities, including surgery, radiation therapy, and/or medical therapy, is typically recommended. Surgery is considered the basis of treatment for non-metastatic AGASAC and AGASAC with regional lymph node metastasis [
2,
12,
20,
21]. Radiotherapy and a range of medical agents have been used both as adjuvant or palliative therapy [
2,
13,
14,
15,
20,
22,
23,
24,
25,
26,
27,
28]. Successful management of the primary tumour and metastatic lesions can lead to prolonged survival ranging from 713 to 1035 days [
14,
18,
21,
24], in comparison with patients managed solely medically, which has a reported median survival time of 212 days [
2]. However, there are contrasting reports on the effect of treatment protocols on outcomes of AGASAC patients [
2,
5,
15,
19,
22,
23], and as yet, a consensus therapeutic approach has not been defined.
Several clinical and histological factors have been suggested as indicators of poor survival or reduced progression-free interval (PFI). Primary tumour size has the greatest volume of evidence, with larger tumours associated with shorter survival times [
2,
7,
15]. Lymph node involvement and distant metastasis have also been reported to have prognostic relevance [
2,
5,
7,
15,
19]. The influence of hypercalcaemia on survival is ambiguous, with evidence both for and against an association [
2,
5,
7,
29]. Studies investigating clinical factors as indicators of PFI are less numerous; however, tumour size, lymph node metastasis [
15], sublumbar lymphadenopathy [
19], and hypercalcaemia [
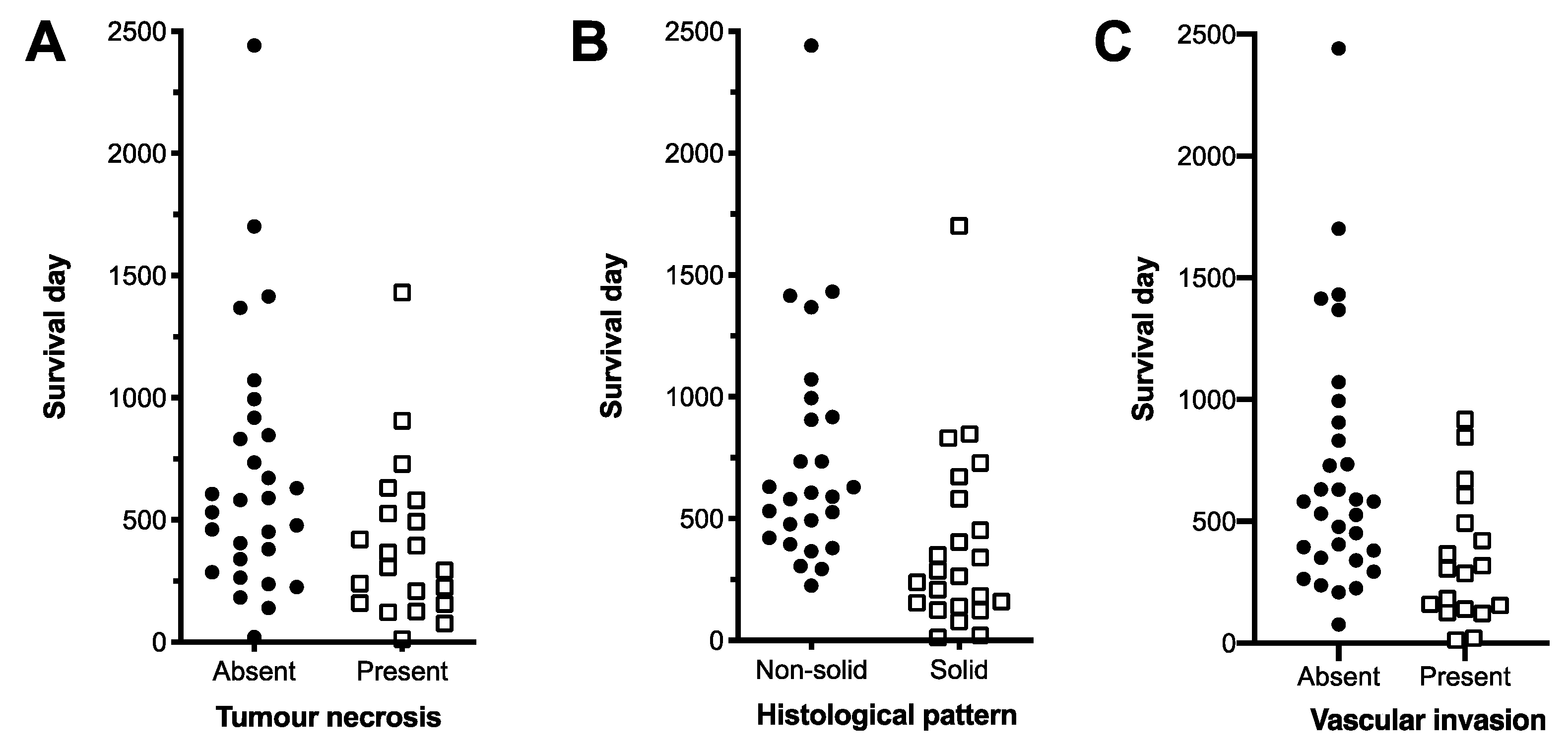
29] have been associated with a decrease in median PFI (MPFI). The histological variables of necrosis, solid tumour pattern, vascular invasion and peripheral infiltration, when considered in isolation, have been associated with decreased overall survival [
11,
16,
30]. Previous studies have found no association between mitotic count and survival and/or metastasis at presentation [
16,
31]. The role of the proliferation marker Ki67 in predicting the progression of AGASAC cases has not been clearly defined; however, studies so far have found no association between per cent of Ki67 immunolabelling within the primary tumour and metastatic lymph nodes with overall median survival time (MST) [
17,
30].
In this study, multivariate models optimised for stability were used to establish clinical and histopathological risk factors of decreased survival and PFI in AGASAC patients. Our aim was to provide clinicians treating dogs with AGASAC with replicable algorithms using readily available clinical and pathological data to generate estimated survival times and relative prognosis for the purpose of informing treatment decisions. Guiding that aim were two hypotheses. Firstly, as our case population employed predominant use of CT imaging for patient staging that allowed precise surgical planning for primary and metastatic disease, we hypothesised that surgery would benefit AGASAC patients irrespective of clinically defined disease stage. Secondly, we also hypothesised that histological features associated with decreased survival have additive risk and that the presence of more than one such feature has greater predictive power for decreased survival than a single variable alone.
4. Discussion
This study identifies clinical and histopathological features of 81 AGASAC patients that were independent risk factors for decreased survival or PFI. In this paper, we focused on creating a stringent statistical methodology, similar to that used in human oncology, to produce robust results that maximised translational relevance [
37]. Careful consideration was given to the number of variables that could be robustly evaluated with the dataset, and variable selection followed recommendations for human medical fields [
38].
Tumour diameter over 2 cm, lymph node diameter grouped into three tiers by the thresholds of 1.6 cm and 5 cm, and surgical management and/or use of radiotherapy were identified as independent clinical variables associated with survival, irrespective of tumour stage. Tumour diameter over 1.3 cm and presence of distant metastasis were identified as independent clinical variables associated with shorter progression-free intervals. Histological evidence of necrosis, solid histological pattern, and vascular invasion were independent histological variables associated with survival. These data were used to create algorithms based on clinical features and treatment options, or histological features, that significantly influence survival, in order to deliver more accurate estimates of individual survival times. The clinical algorithm utilised staging information, whilst the histological algorithm utilised information from primary tumour tissue. This distinction acknowledges that some AGASAC cases are initially cytologically diagnosed, resulting in clinical staging preceding surgical excision, or that histopathology may be unavailable in cases not managed with surgery. Conversely, in some situations, surgical removal/sampling with histopathology may occur in the absence of full clinical staging.
This paper is the first to use a multivariate model stratified by clinical stage to investigate the effect of clinical parameters on survival. It has been postulated that some effect of tumour size and lymph node size upon survival is often, in part, related to a potential association between larger tumour or lymph node size and increased stage of disease [
7,
17]. However, in this study, tumour and lymph node size are consistent independent risk factors of decreased survival irrespective of tumour stage. A tumour diameter of 2 cm was identified as the optimum threshold in this study. Previously reported thresholds of tumour size with prognostic value were a diameter of 2.5 cm [
7,
23] and a volume of 10 cm
2 (approximate diameter of 3.6 cm) [
2]. For studies that use unstandardised methods of determining threshold points, this level of concordance is encouraging. For lymph node size, a two-tier threshold of 1.6 cm and 5 cm was the most discriminatory in these data. The higher threshold of 5 cm is similar to the 4.5 cm threshold previously reported [
7], but our data also identified an additional threshold of 1.6 cm, below which cases exhibit a trend for long survival times. Dogs with large primary or lymph node tumour volume, irrespective of distant metastatic disease, can have urofaecal obstruction that may progress to death or euthanasia [
5]. In this study, the majority of cases with symptoms of urofeacal obstruction had a tumour diameter over 2 cm and/or lymph node diameter over 5 cm, respectively. We hypothesise that the mass effect of locoregional disease and its sequelae contribute to the association of tumour and lymph node size and survival in our study.
Successful management of the primary tumour and metastatic lesions, primarily through surgery, can lead to improved survival [
2,
12,
20,
21]. Our study demonstrates that locoregional management with surgery and/or radiotherapy can result in significantly longer MST for patients with nodal or distant metastasis when compared to those treated with medical treatment alone or with no treatment. At the study institution, surgery was the predominant form of aggressive locoregional control and was widely offered to patients due to limited access to radiotherapy geographically. This afforded a unique opportunity to assess surgery as a tool for early debulking therapy and interventional palliation of advanced-stage patients that may have otherwise undergone more conservative non-surgical treatment if radiotherapy was readily available. It also explored the impact of locoregional therapy in survival for those patients with distant metastasis when medical management was insufficient to acutely alleviate obstructive symptoms. Our extensive use of CT imaging supported surgical planning, and in our patients, surgery was shown to be safe and effective with a low surgical mortality rate (3%). Tumour or lymph node size was not correlated to the type of treatment received, and therefore, the volume of local disease did not influence patient management. The uncoupling of the clinical stage from the patient outcome is similar to that observed in canine thyroid carcinoma, where distant metastasis has not been a reliable determinant of survival [
39,
40].
The prognostic relevance of tumour and lymph node size is recognised in the current clinical grading system [
7], but suggested treatment options are stage-dependent. We suggest an alternative algorithm that places less importance on distant metastasis and instead focuses on the extent, as measured by size, of locoregional disease and its proposed treatment. By using a cumulative score, the algorithm also allows the treatment type to mitigate the effects of presenting tumour and lymph node size, further underscoring the benefits of locoregional control regardless of the original tumour and lymph node size.
In our study population, the incidence of hypercalcaemia was 23%. This study identified a positive association between hypercalcaemia and lymph node size, suggesting that the presence of hypercalcaemia may be related to metastatic volume. Differential expression of parathyroid-hormone-related polypeptide between primary and metastatic lesions has been documented in human mammary carcinoma [
41,
42] and may suggest a potential mechanism for the association in AGASAC cases. Hypercalcaemia can result in renal damage and other complications, potentially affecting mortality. However, similar to a previous study [
15], we found no significant association with survival. It is generally expected that tumour remission will result in the resolution of paraneoplastic hypercalcaemia, and the majority of hypercalcaemic patients in this study were managed surgically, either alone or with adjunctive treatments. We hypothesise that aggressive locoregional management in this study contributed to reducing hypercalcaemia and its sequelae and may explain why hypercalcaemia was not found to be a significant risk factor in this study.
Our study identified tumour size and the presence of distant metastasis as independent significant risk factors in the first PFI. Tumours over 1.3 cm had an almost six-fold increase in the relative risk of a decreased PFI, compared to tumours equal to or less than 1.3 cm. These data are supportive of previously published results in which tumour size influenced the first PFI [
15]. The effect of distant metastasis as an independent risk factor for decreased first PFI could be due to the presence of circulating and pre-metastatic seeding of neoplastic cells. Additionally, cases with distant metastasis may be more likely to have an increased frequency of re-examination, and therefore may experience earlier detection of disease progression.
With regard to histopathological features, we identified necrosis, a solid histological pattern, and vascular invasion as independent risk factors of poor survival in multivariate analysis. A solid histological pattern has previously been found to correlate with poor survival on univariate analysis. [
11,
16,
30] Our findings support the hypothesis that loss of the original glandular tissue architecture suggests a loss of cellular differentiation and a more aggressive biological behaviour. Previous evidence also supports an association between decreased survival and the presence of necrosis or vascular invasion [
16,
30]. We evaluated our hypothesis that two or more of these factors was a more discriminating threshold to differentiate between less favourable and favourable survival times. To achieve this, we combined the independently significant variables into an algorithm based on the presence of two or more of the independently significant variables. Confirming our hypothesis, the algorithm was able to stratify cases into two groups with a significantly different MST and hazard ratio. Using the methodology applied here, Ki67% was not found to be useful in predicting overall survival, a finding consistent with studies [
17,
30]. Furthermore, Ki67% and the mitotic count showed no correlation in our data.
A limitation of our study is that the retrospective nature resulted in varied patient management, an output of diverse clinical, financial, and ethical considerations. The statistical approach was designed to accommodate this variability, but a subsequent multi-centre study using standardised protocols would be useful to further investigate the findings presented here.


 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}