The Influence of Anaesthetic Drugs on the Laryngeal Motion in Dogs: A Systematic Review

Abstract
:Simple Summary
Abstract
1. Introduction
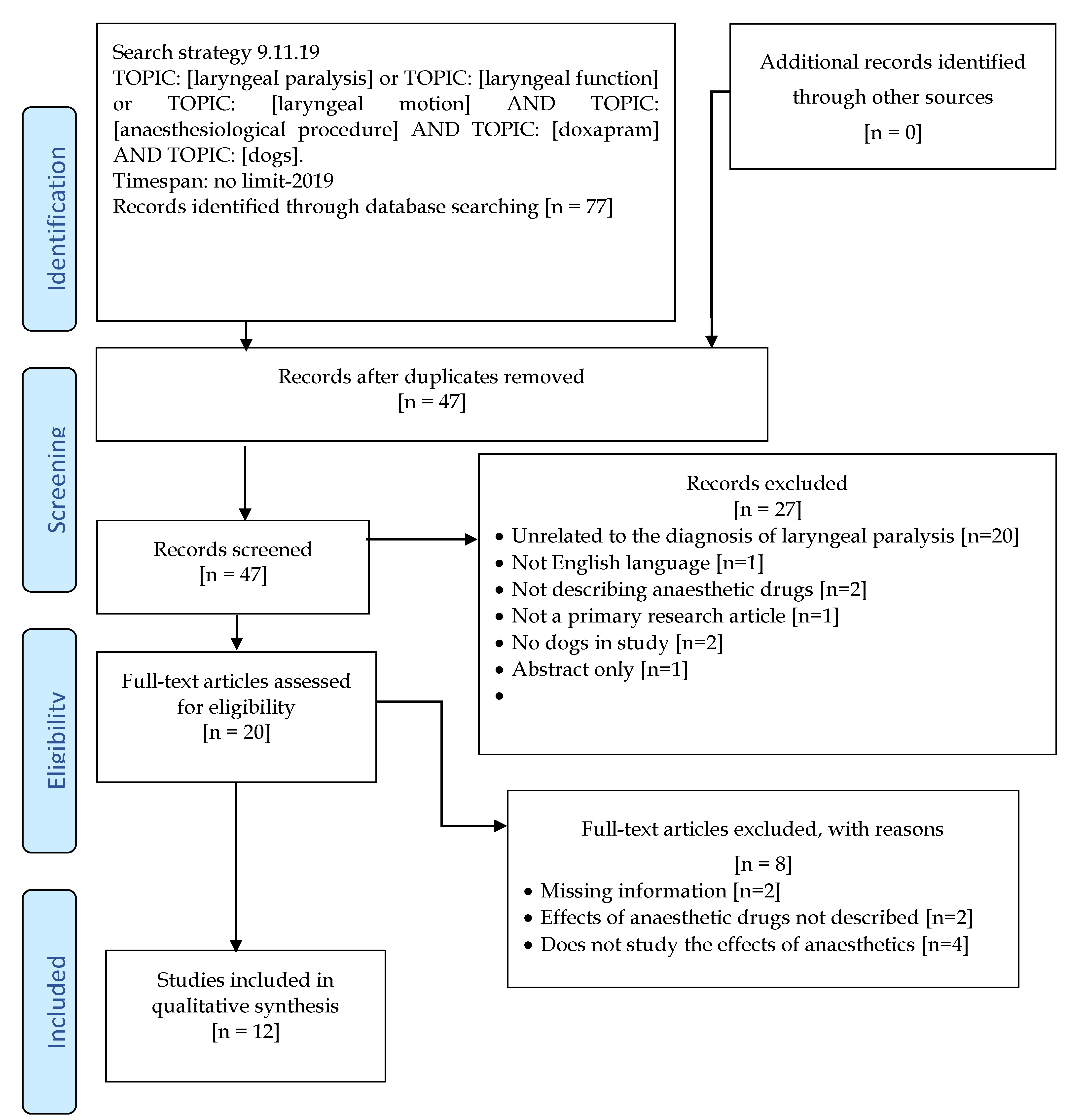
2. Materials and Methods
Assessment of Study Quality and Level of Evidence
3. Results
3.1. Effects of Premedication Drugs and Influence on the Quality of Laryngeal Examination
3.1.1. Dexmedetomidine
3.1.2. Butorphanol
3.1.3. Acepromazine and Butorphanol
3.1.4. Acepromazine and Thiopental, Propofol, Isoflurane
3.1.5. Methadone, Hydromorphone, Oxymorphone
3.2. Effects of Induction Drugs and Influence on the Quality of Laryngeal Examination
3.2.1. Propofol
3.2.2. Alfaxalone
3.2.3. Thiopental
3.2.4. Ketamine-Diazepam
3.2.5. Methohexital
3.2.6. Isoflurane Mask Induction
3.3. Agreement Between Laryngeal Function Assessors
3.4. Respiratory Stimulants
3.4.1. Doxapram
3.4.2. Mechanical Stimulation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- MacPhail, C. Laryngeal disease in dogs and cats. Vet. Clin. Small Anim. Pract. 2014, 44, 19–31. [Google Scholar] [CrossRef]
- Broome, C.; Burbidge, H.; Pfeiffer, D. Prevalence of laryngeal paresis in dogs undergoing general anaesthesia. Aust. Vet. J. 2000, 78, 769–772. [Google Scholar] [CrossRef]
- Rudorf, H.; Barr, F.J.; Lane, J.G. The role of ultrasound in the assessment of laryngeal paralysis in the dog. Vet. Radiol. Ultrasound 2001, 42, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Radlinsky, M.G.; Williams, J.; Frank, P.M.; Cooper, T.C. Comparison of three clinical techniques for the diagnosis of laryngeal paralysis in dogs. Vet. Surg. 2009, 38, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Kitshoff, A.M.; Van Goethem, B.; Stegen, L.; Vandekerckhove, P.; De Rooster, H. Laryngeal paralysis in dogs: An update on recent knowledge. J. S. Afr. Vet. Assoc. 2013, 84, E1–E9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, A.M.; Tobias, K.; Long, C.; Bartges, J.; Harvey, R. Effects of various anesthetic agents on laryngeal motion during laryngoscopy in normal dogs. Vet. Surg. 2004, 33, 102–106. [Google Scholar] [CrossRef]
- DeGroot, W.D.; Tobias, K.M.; Browning, D.C.; Zhu, X. Examination of laryngeal function of healthy dogs by using sedation protocols with dexmedetomidine. Vet. Surg. 2019, 49, 124–130. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Brown, M.B.; Dugat, D.R.; Lyon, S.D.; Nafe, L.A.; Payton, M.E.; Peakheart, S.K.; Salazar, R.S. Comparison of methohexital and propofol as induction agents for evaluation of laryngeal function in healthy dogs. Vet. Surg. 2019, 48, 70–78. [Google Scholar] [CrossRef]
- Labuscagne, S.; Zeiler, G.E.; Dzikiti, B.T. Effects of chemical and mechanical stimulation on laryngeal motion during alfaxalone, thiopentone or propofol anaesthesia in healthy dogs. Vet. Anaesth. Analg. 2019, 46, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Norgate, D.; Ter Haar, G.; Kulendra, N.; Veres-Nyéki, K.O. A comparison of the effect of propofol and alfaxalone on laryngeal motion in nonbrachycephalic and brachycephalic dogs. Vet. Anaesth. Analg. 2018, 45, 729–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radkey, D.I.; Hardie, R.J.; Smith, L.J. Comparison of the effects of alfaxalone and propofol with acepromazine, butorphanol and/or doxapram on laryngeal motion and quality of examination in dogs. Vet. Anaesth. Analg. 2018, 45, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Ambros, B.; Gaunt, M.C.; Duke-Novakovski, T.; Taylor, S.M. Effects of alfaxalone, thiopental, or propofol and diazepam on laryngeal motion in healthy dogs. Can. Vet. J. 2018, 59, 791. [Google Scholar] [PubMed]
- Smalle, T.M.; Hartman, M.J.; Bester, L.; Buck, R.K.; Fosgate, G.T.; Zeiler, G.E. Effects of thiopentone, propofol and alfaxalone on laryngeal motion during oral laryngoscopy in healthy dogs. Vet. Anaesth. Analg. 2017, 44, 427–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKeirnan, K.L.; Gross, M.E.; Rochat, M.; Payton, M. Comparison of propofol and propofol/ketamine anesthesia for evaluation of laryngeal function in healthy dogs. J. Am. Anim. Hosp. Assoc. 2014, 50, 19–26. [Google Scholar] [CrossRef]
- Tobias, K.M.; Jackson, A.M.; Harvey, R.C. Effects of doxapram HCl on laryngeal function of normal dogs and dogs with naturally occurring laryngeal paralysis. Vet. Anaesth. Analg. 2004, 31, 258–263. [Google Scholar] [CrossRef]
- Gross, M.E.; Dodam, J.R.; Pope, E.R.; Jones, B.D. A comparison of thiopental, propofol, and diazepam-ketamine anesthesia for evaluation of laryngeal function in dogs premedicated with butorphanol-glycopyrrolate. J. Am. Anim. Hosp. Assoc. 2002, 38, 503–506. [Google Scholar] [CrossRef]
- Miller, C.J.; McKiernan, B.C.; Pace, J.; Fettman, M.J. The effects of doxapram hydrochloride (Dopram-V) on laryngeal function in healthy dogs. J. Vet. Intern. Med. 2002, 16, 524–528. [Google Scholar] [CrossRef]
- Howick, J. The 2011Oxford Levels of Evidence (Introductory Document). OCEBM (2011) Levels of evidence working group. The oxford levels of evidence, 2 nd. Oxford Centre for Evidence-Based Medicine, Chalmers, I. ed. Oxford Centre for Evidence-Based Medicine. Available online: https://www.cebm.net/index.aspx?o=5653 (accessed on 15 October 2019).
- SIGN. Scottisch Intercollegiate Guidelines Network 50 Methodology Checklist; SIGN: Scotland, UK, 2015; Available online: www.sign.ac.uk/guidelines/fulltext/50/index.html (accessed on 15 October 2019).
- Brodbelt, D.C.; Pfeiffer, D.U.; Young, L.E.; Wood, J.L. Results of the confidential enquiry into perioperative small animal fatalities regarding risk factors for anesthetic-related death in dogs. J. Am. Vet. Med Assoc. 2008, 233, 1096–1104. [Google Scholar] [CrossRef]
- Tzannes, S.; Govendir, M.; Zaki, S.; Miyake, Y.; Packiarajah, P.; Malik, R. The use of sevoflurane in a 2: 1 mixture of nitrous oxide and oxygen for rapid mask induction of anaesthesia in the cat. J. Feline Med. Surg. 2000, 2, 83–90. [Google Scholar] [CrossRef]
- Bednarski, R.; Grimm, K.; Harvey, R.; Lukasik, V.M.; Penn, W.S.; Sargent, B.; Spelts, K. AAHA anesthesia guidelines for dogs and cats. J. Am. Anim. Hosp. Assoc. 2011, 47, 377–385. [Google Scholar] [CrossRef]
- Dani, C.; Bertini, G.; Pezzati, M.; Pratesi, S.; Filippi, L.; Tronchin, M.; Rubaltelli, F.F. Brain hemodynamic effects of doxapram in preterm infants. Neonatology 2006, 89, 69–74. [Google Scholar] [CrossRef]
- Ebihara, S.; Ogawa, H.; Sasaki, H.; Hida, W.; Kikuchi, Y. Doxapram and perception of dyspnea. Chest 2002, 121, 1380–1381. [Google Scholar] [CrossRef] [Green Version]
- Roll, C.; Horsch, S. Effect of doxapram on cerebral blood flow velocity in preterm infants. Neuropediatrics 2004, 35, 126–129. [Google Scholar]
- Arrioja, A. Compendium of Veterinary Products; Ames, I.A., Ed.; North American Compendiums, Iowa State University Press: Ames, IA, USA, 2001. [Google Scholar]
- Franz. Central nervous system stimulants. In Goodman and Gilman’s the Pharmacological Basis of Therapeutics, 7th ed.; Gilman, A.G.G.L., Rall, T.W., Nurad, F., Eds.; Macmillan Publishing Co: New York, NY, USA, 1985; pp. 582–588. [Google Scholar]
- Donald, C.P. Plumb’s Veterinary Drug Handbook: Desk; Iowa State University Press: Ames, IA, USA,, 2001. [Google Scholar]
- Yun, S.A.K.Y. The Effect of Doxapram on Cardiopulmonary Function in Dogs under Total Intravenous Anesthesia with Remifentanil and Propofol. J. Vet. Clin. 2015, 32, 491. [Google Scholar] [CrossRef]
- Greenfield, C.L.; Alsup, J.C.; Hungerford, L.L.; McKiernan, B.C. Bilateral recurrent laryngeal neurectomy as a model for the study of idiopathic canine laryngeal paralysis. Can. Vet. J. 1997, 38, 163. [Google Scholar]
- White, R. Laryngeal paralysis: An introduction. Vet. Q. 1998, 20, S2–S3. [Google Scholar] [CrossRef] [Green Version]
- Monnet. Laryngeal paralysis and devocalization. In Textbook of Small Animal Surgery, 3rd ed.; Slatter, D., Ed.; Saunders: Philadelphia, PA, USA, 2003; pp. 808–813. [Google Scholar]


{kind=link}
| Reference | Journal | Study design | Number of Dogs | Health Status | Group Size | Prospective Power Calculation | Evaluation Method | Assessment of Laryngeal Function | Laryngeal Function Assessed during Inspiratory Cycle | Statistical Analysis |
|---|---|---|---|---|---|---|---|---|---|---|
| Brown et al. (2019) [10] | Veterinary surgery | Prospective, controlled randomised blinded | 40 shelter dogs | Healthy | 10/10/10/10 | Yes | Normalised glottal gap area (NGAA) | Direct visualisation and video from videolaryngoscopy | Yes | ANOVA |
| DeGroot et al. (2019) [7] | Veterinary surgery | Prospective randomised crossover | 8 research dogs | Healthy | 8/8/8/8 | No | Video laryngoscopy, normalised glottal gap area (NGAA) | Still images from videolaryngoscopy | Yes | ANOVA |
| blinded | ||||||||||
| Labuscagne et al. (2019) [11] | Veterinary anaesthesia and analgesia | Prospective randomized crossover | 8 research dogs | Healthy | 8/8/8/8/8/8 | No | Visual subjective | Subjective laryngeal exposure score | Yes | Friedman rank sum test/Wilcoxon rank sum test/ANOVA/ |
| blinded | ||||||||||
| Norgate et al. (2018) [12] | Veterinary anaesthesia and analgesia | Prospective randomized, blinded | 48 client-owned dogs | Healthy brachy-cephalic | 24/24 | No | Video laryngoscopy, visual subjective | Subjective laryngeal exposure score and video from videolaryngoscopy | Yes | Shapiro-Wilk test/ |
| Chi square and Fisher’s exact tests | ||||||||||
| Radkey et al. (2018) [13] | Veterinary anaesthesia and analgesia | Prospective randomized controlled crossover, blinded | 10 research dogs | Healthy | 10/10/10/10 | Yes | Normalised rima glottides surface area (RGSA) | Video and still images from videolaryngoscopy | Yes | Shapiro-Wilk test/ANOVA/Kruskal-Wallis |
| Ambros et al. (2018) [14] | Canadian veterinary journal | Prospective, crossover randomised blinded | 8 client-owned dogs | Healthy | 2008/8/8 | Yes | Normalised glottal gap area (NGAA) | Direct visualisation and still images from videolaryngoscopy | Yes | Kruskal-Wallis |
| Smalle et al. (2017) [15] | Veterinary anaesthesia and analgesia | Prospective randomized crossover, blinded | 6 research dogs | Healthy | 2006/6/6 | No | Visual subjective | Subjective laryngeal exposure score | Yes | Friedman/Mann-Whitney U tests, Spearman |
| McKeirnan et al. (2014) [16] | Journal of the American Animal Hospital Association | Prospective randomized, blinded | 48 shelter dogs | Healthy | 24/24 | No | Visual subjective | Subjective laryngeal exposure score | Yes | T test and Fischer exact test |
| Jackson et al. (2004) [6] | Veterinary surgery | Prospective randomized crossover | 6 dogs | Healthy | 6/6/6/6/6/6/6 | No | Normalised glottal gap area (NGAA) | Video and still images from videolaryngoscopy | Yes | ANOVA/Students t test |
| blinded | ||||||||||
| Tobias et al. (2004) [17] | Veterinary anaesthesia and analgesia | Prospective experimental and clinical | 12 dogs | Healthy/laryngeal paralysis | 6-6 | No | Normalised glottal gap area (NGAA) | Video and still images from videolaryngoscopy | Yes | Wilcoxon rank sum test/t-test/Mann-Whitney test |
| Gross et al. (2002) [18] | Journal of the American Animal Hospital Association | Prospective randomized crossover | 8 dogs | Healthy | 2008/8/8 | No | Visual subjective | Direct visualisation | Yes | ANOVA |
| blinded | ||||||||||
| Miller et al. (2002) [19] | Journal of Veterinary Internal Medicine | Prospective | 30 research dogs | Healthy | 30 | No | Normalised rima glottides surface area (RGSA) | Video and still images from videolaryngoscopy | Yes | Kolmogorov-Smirnov |
| /ANOVA |
| Premedication Agent | Dose | Induction Agent | Timing before Induction | Improved Examination Conditions | Results | Statistical Significance | Reference |
|---|---|---|---|---|---|---|---|
| Dexmedetomidine vs. Butorphanol + dexmedetomidine vs. Hydromorphone + dexmedetomidine | 15 µg kg−1 IV dexmedetomidine 0.3 mg kg−1 IV butorphanol + 7 µg kg−1 IV dexmedetomidine 0.1 mg kg−1 IV hydromorphone + 5 µg kg−1 IV dexmedetomidine | No | To effect | Yes | Normal laryngeal motion with all protocols | No | DeGroot et al. (2019) [7] |
| Acepromazine + methadone | 0.01 mg kg−1 IM acepromazine + 0.2 mg kg−1 IM methadone | Yes–alfaxalone/propofol | 30 min prior to induction | N/D | >75% maintained laryngeal motion | N/D | Norgate et al. (2018) [12] |
| Acepromazine + butorphanol vs. saline (control) | 0.03 mg kg−1 IV acepromazine + 0.2 mg kg−1 IV butorphanol vs. saline (non-premedicated control group) | Yes–alfaxalone/propofol | 5 min prior to induction | Yes | No arytenoid motion in 50% of dogs | Yes | Radkey et al. (2018) [13] |
| Butorphanol | 0.5 mg kg−1 IV butorphanol | Yes–propofol/ketamine | 20 min prior to induction | N/D | N/D | N/A | McKeirnan et al. (2014) [16] |
| good conditions | |||||||
| Butorphanol | 0.5 mg kg−1 IV butorphanol | Yes–thiopental/propofol | 5 min prior to induction | N/D | Laryngeal motion observable | N/A | Gross et al. (2002) [18] |
| Acepromazine + butorphanol | 0.2 mg kg−1 IM acepromazine + 0.4 mg kg−1 IV butorphanol | Yes–mask isoflurane | 20 min prior to induction | N/D | Arytenoid motion maintained | Yes | Jackson et al. (2004) [6] |
| Acepromazine | 0.05 mg kg−1 IM acepromazine | Yes–thiopental | 20 min prior to induction | N/D | Arytenoid motion less than with thiopental alone | Yes | Jackson et al. (2004) [6] |
| Acepromazine + oxymorphone | 0.05 mg kg−1 IM acepromazine + 0.05 mg kg−1 IV oxymorphone | No | 20 min prior to induction | N/D | N/D | N/A | Jackson et al. (2004) [6] |
| Acepromazine + butorphanol | 0.022–0.2 mg kg−1 IM acepromazine + 0.44 mg kg−1 IM butorphanol | Yes–mask isoflurane | 20 min prior to induction | N/D | Laryngeal motion present in all healthy dogs but no motion in dogs with laryngeal paralysis | N/D | Tobias et al. (2004) [17] |
| Acepromazine + butorphanol | 0.05 mg kg−1 SQ acepromazine + 0.22 mg kg−1 IV butorphanol | Yes–propofol | 20 min/5 min prior to induction | N/D | N/D | N/A | Miller et al. (2002) [19] |
| Induction Agent | Dose | Sedation | Titration of Induction | Examination Conditions/Exposure | Results | Statistical Significance | Reference |
|---|---|---|---|---|---|---|---|
| Propofol vs. methohexital vs. saline | 6.8 mg kg−1 IV propofol 7.4 mg kg−1 IV methohexital Control IV (saline control group) | No | To effect | No differences | No differences in laryngeal motion among groups | No | Brown et al. (2019) [10] |
| Alfaxalone + doxapram vs. propofol + doxapram | 1.5 mg kg−1 IV alfaxalone 3.0 mg kg−1 IV propofol 2.5 mg kg−1 IV doxapram | No | To effect | No differences | Alfaxalone-doxapram significantly less arytenoid motions | Yes | Labuscagne et al. (2019) [11] |
| Propofol vs. dexmedetomidine | 6.5 mg kg−1 IV propofol 15 µg kg−1 IV dexmedetomidine | No | To effect | Good except one dog in propofol group | Laryngeal function observed in all except propofol | Yes | DeGroot et al. (2019) [7] |
| Alfaxalone vs. propofol + diazepamvs. thiopental | 2.6 mg kg−1 IV alfaxalone 3.8 mg kg−1 IV propofol + 0.4 mg kg−1 IV diazepam 14.2 mg kg−1 IV thiopental | No | To effect | N/D | No differences in laryngeal motion among groups | No | Ambros et al. (2018) [14] |
| Isoflurane | 3–5% in oxygen (2 L/min) | Yes | To effect | N/D | Active laryngeal motion detected in all healthy dogs but in none of the dogs with suspected laryngeal paralysis | N/A | Tobias et al. (2004) [17] |
| Thiopental vs. propofol vs. ketamine + diazepam vs. acepromazine + thiopental vs. acepromazine + propofol vs. isoflurane | 14 mg kg−1 IV thiopental 5.6 mg kg−1 IV propofol 8.5 mg kg−1 IV ketamine + 0.4 mg kg−1 IV diazepam 0.05 mg kg−1 IM acepromazine + 9.8 mg kg−1 IV thiopental 0.05 mg kg−1 IM acepromazine + 3.7 mg kg−1 IV propofol N/D | Yes | To effect | N/D | After induction: no differences in laryngeal motion among groups. Prior to recovery, thiopental superior motion | No/Yes | Jackson et al. (2004) [6] |
| Propofol vs. thiopental vs. ketamine + diazepam | 3.6 mg kg−1 IV propofol 10.4 mg kg−1 IV thiopental5.6 mg kg−1 IV ketamine + 0.3 mg kg−1 IV diazepam | Yes | To effect | Exposure lower in ketamine/ diazepam | Laryngeal function observed with all protocols. | No | Gross et al. (2002) [18] |
| Propofol | 4.0 mg kg−1 IV propofol | Yes | No | N/D | N/D | N/A | Miller et al. (2002) [19] |
| Respiratory Stimulant | Dose (bolus) /(Titration) | Health Status | Pre-medication | Induction of Anaesthesia | Adverse Effects | Results | Passive or Paradoxical Arytenoid Motion | Statistical Significance | Reference |
|---|---|---|---|---|---|---|---|---|---|
| Doxapram vs. control | 2.2 mg kg−1 IV/saline (control) | Healthy | No | Propofol/methohexital | Exaggerated laryngeal movements | Doxapram improved breathing scores but not laryngeal function | No | No | Brown et al. (2019) [10] |
| Doxapram | 1.0 mg kg−1 IV | Healthy | Dexmedetomidine/Butorphanol/Hydromorphone | Propofol/ dex-medetomidine | No | Doxapram improved laryngeal function in dogs receiving dexmedetomidine. No improvements in the other drug protocols | Yes, prior to doxapram in propofol group | Yes | DeGroot et al. (2019) [7] |
| Doxapram vs. Mechanical stimulation | 2.5 mg kg−1 IV | Healthy | No | Alfaxalone/propofol/thiopental | No | Doxapram more effective in stimulating laryngeal motion. Examination time longest with alfaxalone, despite doxapram | No | Yes | Labuscagne et al. (2019) [11] |
| Doxapram | 0.25 mg kg−1 IV | Healthy | Acepromazine + Butorphanol/ control group | Alfaxalone/propofol | Increased respiratory drive | After doxapram, laryngeal motion present in all healthy dogs with previously lacking laryngeal motion. RGSA was significantly less in ALF before doxapram compared with all other treatments and after doxapram 50% of dogs in alfaxalone no motion | Yes, in dogs with previously good motion | Yes | Radkey et al. (2018) [13] |
| Doxapram | 1 mg kg−1 IV | Healthy | Butorphanol | Propofol/ketamine/propofol | None | Doxapram improved respiratory scores and significantly increased the ability to determine normal laryngeal function | No | Yes | McKeirnan et al. (2014) [16] |
| Doxapram | 2–5 mg kg−1 IV | Healthy | Acepromazine /Butorphanol | Multiple | N/D | N/D | N/D | N/A | Jackson et al. (2004) [6] |
| Doxapram | 1.1 mg kg−1 IV | Healthy and with laryngeal paralysis | Butorphanol/Acepromazine | Isoflurane by mask | Intubation necessary | Healthy dogs differentiated from dogs with laryngeal paralysis with doxapram | Yes, in dogs with laryngeal paralysis | Yes | Tobias et al (2004) [17] |
| Doxapram | 2.2 mg kg−1 | Healthy | Acepromazine + Butorphanol | Propofol | Excitement/awakening | Doxapram increased laryngeal motion in healthy premedicated dogs | No | Yes | Miller et al. (2002) [19] |
| Quality Criterion. | Score | Labuscagne et al. (2019) [11] | Brown et al. (2019) [10] | DeGroot et al. (2019) [7] | Norgate et al. (2018) [12] | Radkey et al. (2018) [13] | Smalle et al. (2017) [15] | Ambros et al. (2018) [14] | McKeirnan et al. (2014) [16] | Tobias et al. (2004) [17] | Jackson et al. (2004) [6] | Gross et al. (2002) [18] | Miller et al. (2002) [19] | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Clear question addressed by study | Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | 0 | / | / | / | / | / | / | / | / | / | / | / | / | |
| Acceptable randomization method | Yes | 1 | 1 | 1 | / | 1 | 1 | 1 | / | 1 | / | 1 | / | / |
| No | 0 | / | / | / | / | / | / | / | / | / | / | / | / | |
| N/R | 0 | / | / | 0 | / | / | / | 0 | / | 0 | / | 0 | 0 | |
| Adequate concealment method | Yes | 1 | 1 | 1 | 1 | / | / | 1 | / | 1 | / | / | / | / |
| No | 0 | / | / | / | / | / | / | / | / | 0 | / | / | / | |
| N/R | 0 | / | / | / | 0 | 0 | / | 0 | / | / | 0 | 0 | 0 | |
| Blinding of assessors | Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | / | 1 | 1 | / |
| No | 0 | / | / | / | / | / | / | / | / | / | / | / | / | |
| N/R | 0 | / | / | / | / | / | / | / | / | 0 | / | / | 0 | |
| Assessment videolaryngoscopy and direct observation | Yes | 2 | / | 2 | / | 2 | / | / | 2 | / | / | / | / | / |
| No | 0 | / | / | / | / | / | / | / | / | / | / | / | / | |
| One only | 1 | 1 | / | 1 | / | 1 | 1 | / | 1 | 1 | 1 | 1 | 1 | |
| Agreement between assessors | Yes | 1 | / | / | / | 1 | / | / | / | / | / | / | / | / |
| No | 0 | / | 0 | / | / | / | / | / | 0 | / | / | / | / | |
| N/R or N/A | 0 | 0 | / | 0 | / | 0 | 0 | 0 | / | 0 | 0 | 0 | 0 | |
| Groups similar at baseline | Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | 0 | / | / | / | / | / | / | / | / | / | / | / | / | |
| Only difference between groups is the anaesthetic drug or doxapram | Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | 0 | / | / | / | / | / | / | / | / | / | / | / | / | |
| Outcomes measurements are standard, valid and reliable | Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | 0 | / | / | / | / | / | / | / | / | / | / | / | / | |
| Intention-to-treat (ITT) | Yes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| No | 0 | / | / | / | / | / | / | / | / | / | / | / | / | |
| Overall bias rating | (++) | |||||||||||||
| (+) | (+) | (++) | (+) | (++) | (+) | (+) | (+) | (+) | (−) | (+) | (+) | (+) | ||
| (−) | ||||||||||||||
| Level of evidence (LoE) | I-V | II | II | II | II | II | II | II | II | III | II | II | III |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ranninger, E.; Kantyka, M.; Bektas, R.N. The Influence of Anaesthetic Drugs on the Laryngeal Motion in Dogs: A Systematic Review. Animals 2020, 10, 530. https://doi.org/10.3390/ani10030530
Ranninger E, Kantyka M, Bektas RN. The Influence of Anaesthetic Drugs on the Laryngeal Motion in Dogs: A Systematic Review. Animals. 2020; 10(3):530. https://doi.org/10.3390/ani10030530
Chicago/Turabian StyleRanninger, Elisabeth, Marta Kantyka, and Rima Nadine Bektas. 2020. "The Influence of Anaesthetic Drugs on the Laryngeal Motion in Dogs: A Systematic Review" Animals 10, no. 3: 530. https://doi.org/10.3390/ani10030530