
Hippocampal Atrophy in Pediatric Transplant Recipients with Human Herpesvirus 6B

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
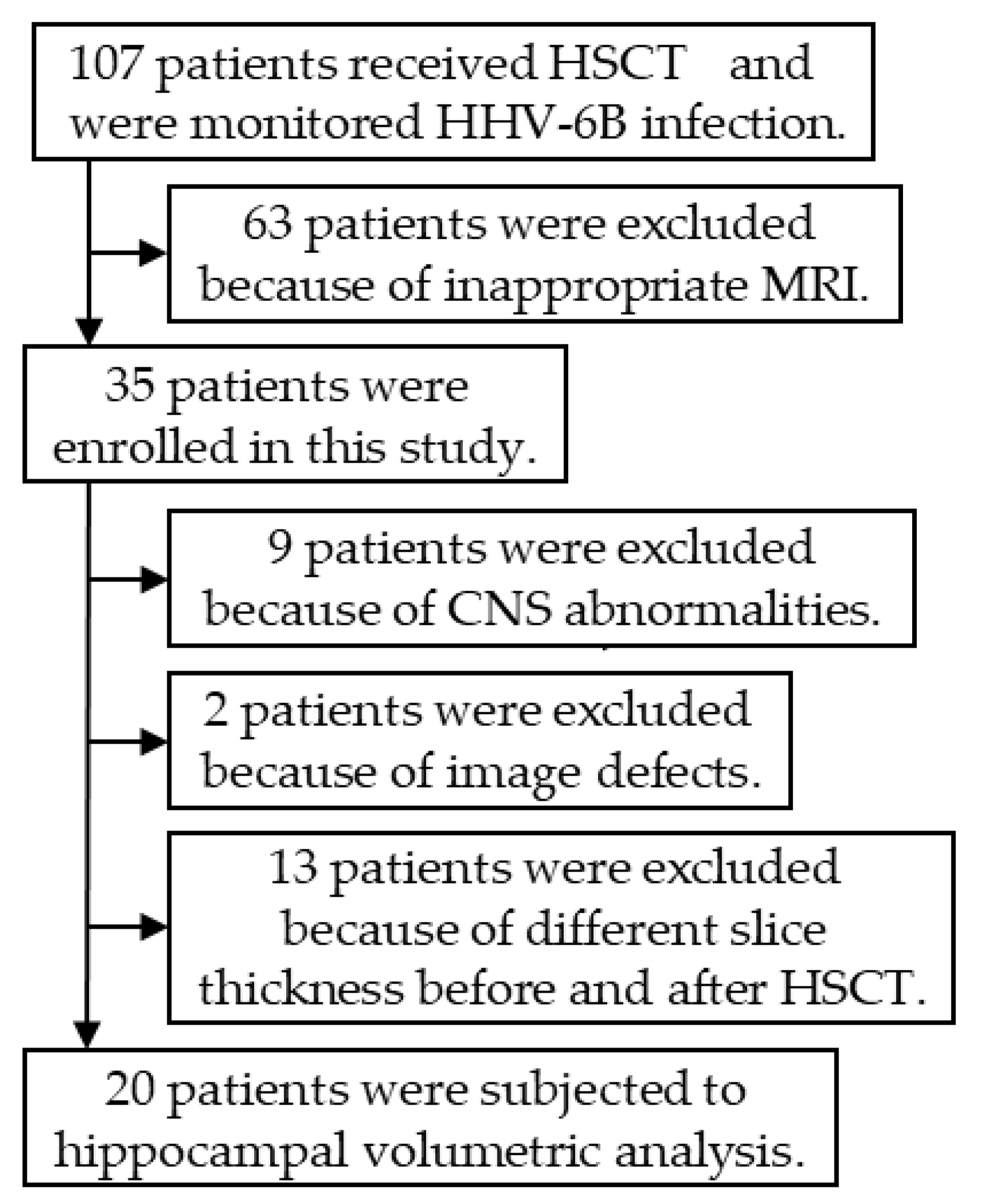
2.1. Patients
2.2. Sample Collection and Definition of HHV-6B Infection
2.3. HHV-6B Isolation
2.4. Real-Time Quantitative PCR Assay for HHV-6
2.5. MRI
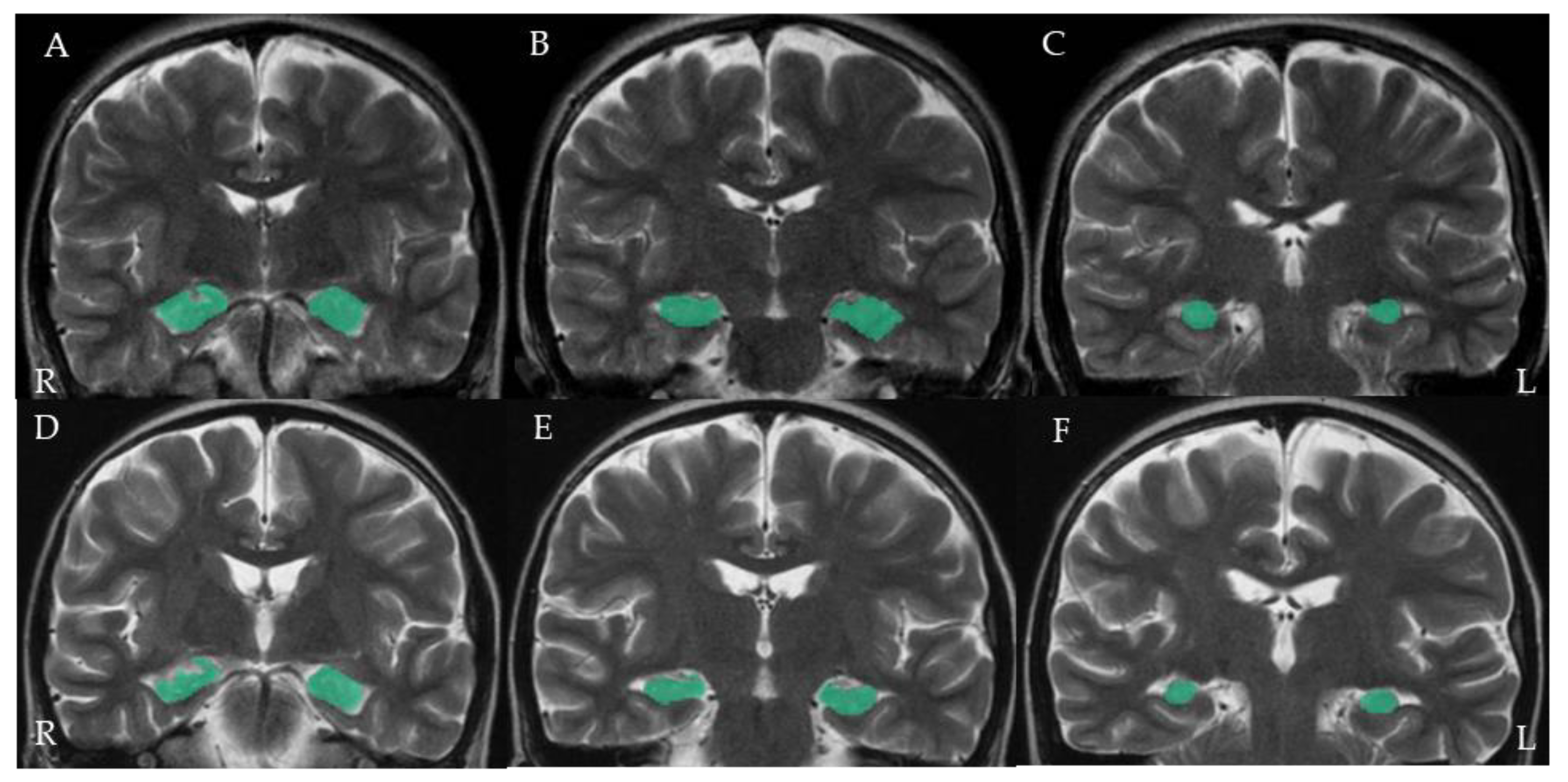
2.6. Hippocampal Volumetric Analysis
2.7. Statistical Analysis
2.8. Ethical Approval
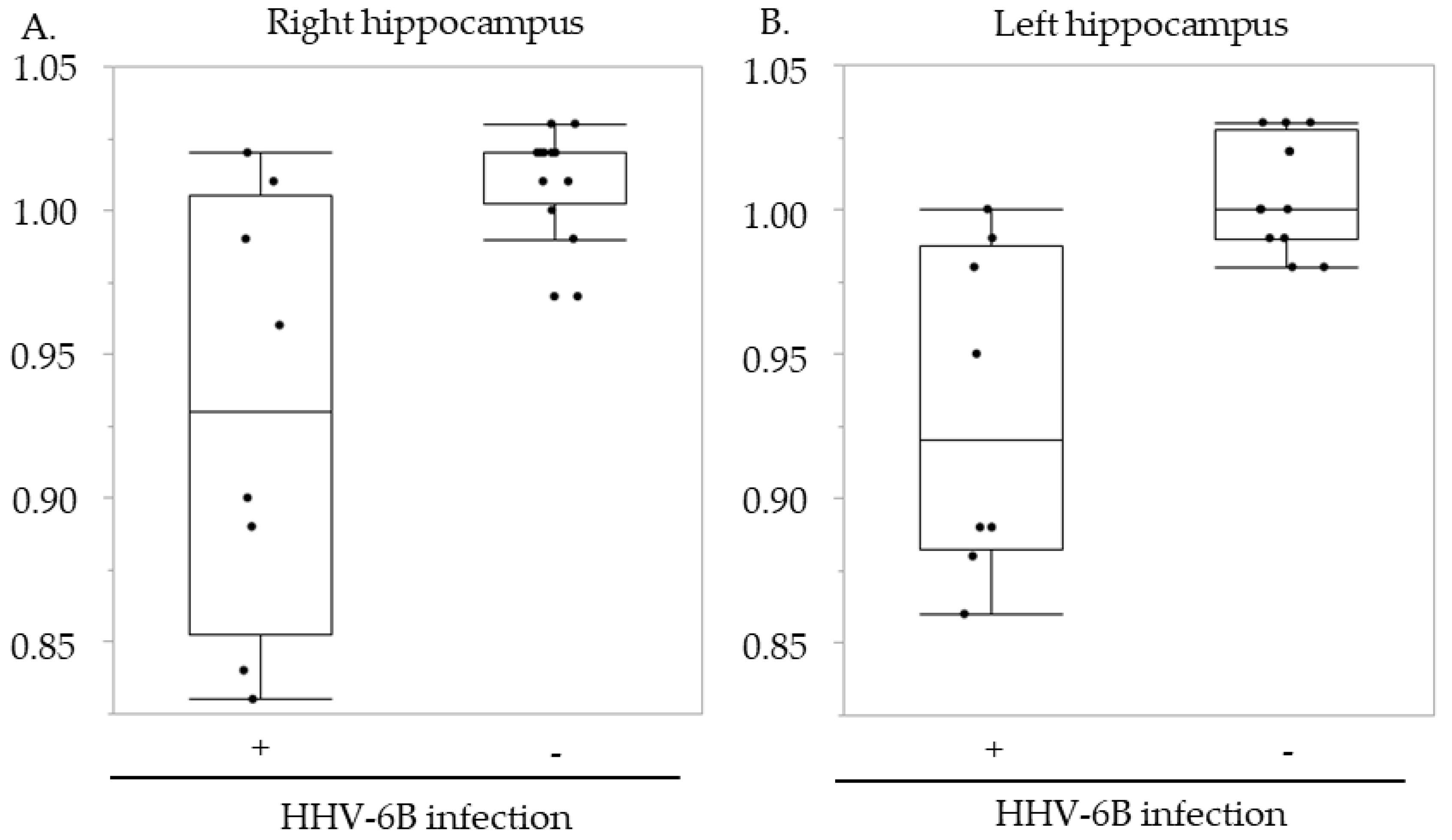
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Yamanishi, K.; Okuno, T.; Shiraki, K.; Takahashi, M.; Kondo, T.; Asano, Y.; Kurata, T. Identification of human herpesvirus-6 as a causal agent for exanthem subitum. Lancet 1988, 1, 1065–1067. [Google Scholar] [CrossRef]
- Hall, C.B.; Long, C.E.; Schnabel, K.C.; Caserta, M.T.; McIntyre, K.M.; Costanzo, M.A.; Knott, A.; Dewhurst, S.; Insel, R.A.; Epstein, L.G. Human herpesvirus-6 infection in children. A prospective study of complications and reactivation. N. Engl. J. Med. 1994, 331, 432–438. [Google Scholar] [CrossRef]
- Caserta, M.T.; Hall, C.B.; Schnabel, K.; Long, C.E.; D’Heron, N. Primary human herpesvirus 7 infection: A comparison of human herpesvirus 7 and human herpesvirus 6 infections in children. J. Pediatr. 1998, 133, 386–389. [Google Scholar] [CrossRef]
- Suga, S.; Suzuki, K.; Ihira, M.; Yoshikawa, T.; Kajita, Y.; Ozaki, T.; Iida, K.; Saito, Y.; Asano, Y. Clinical characteristics of febrile convulsions during primary HHV-6 infection. Arch. Dis. Child. 2000, 82, 62–66. [Google Scholar] [CrossRef]
- Asano, Y.; Yoshikawa, T.; Kajita, Y.; Ogura, R.; Suga, S.; Yazaki, T.; Nakashima, T.; Yamada, A.; Kurata, T. Fatal encephalitis/encephalopathy in primary human herpesvirus-6 infection. Arch. Dis. Child. 1992, 67, 1484–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshikawa, T.; Nakashima, T.; Suga, S.; Asano, Y.; Yazaki, T.; Kimura, H.; Morishima, T.; Kondo, K.; Yamanishi, K. Human herpesvirus-6 DNA in cerebrospinal fluid of a child with exanthem subitum and meningoencephalitis. Pediatrics 1992, 89, 888–890. [Google Scholar] [PubMed]
- Suga, S.; Yoshikawa, T.; Asano, Y.; Kozawa, T.; Nakashima, T.; Kobayashi, I.; Yazaki, T.; Yamamoto, H.; Kajita, Y.; Ozaki, T.; et al. Clinical and virological analyses of 21 infants with exanthem subitum (roseola infantum) and central nervous system complications. Ann. Neurol. 1993, 33, 597–603. [Google Scholar] [CrossRef]
- Yoshikawa, T.; Ohashi, M.; Miyake, F.; Fujita, A.; Usui, C.; Sugata, K.; Suga, S.; Hashimoto, S.; Asano, Y. Exanthem subitum-associated encephalitis: Nationwide survey in Japan. Pediatr. Neurol. 2009, 41, 353–358. [Google Scholar] [CrossRef]
- Saito, Y.; Sharer, L.R.; Dewhurst, S.; Blumberg, B.M.; Hall, C.B.; Epstein, L.G. Cellular localization of human herpesvirus-6 in the brains of children with AIDS encephalopathy. J. Neurovirol. 1995, 1, 30–39. [Google Scholar] [CrossRef]
- Chan, P.K.; Ng, H.K.; Hui, M.; Cheng, A.F. Prevalence and distribution of human herpesvirus 6 variants A and B in adult human brain. J. Med. Virol. 2001, 64, 42–46. [Google Scholar] [CrossRef]
- Cuomo, L.; Trivedi, P.; Cardillo, M.R.; Gagliardi, F.M.; Vecchione, A.; Caruso, R.; Calogero, A.; Frati, L.; Faggioni, A.; Ragona, G. Human herpesvirus 6 infection in neoplastic and normal brain tissue. J. Med. Virol. 2001, 63, 45–51. [Google Scholar] [CrossRef]
- Yoshikawa, T.; Suga, S.; Asano, Y.; Nakashima, T.; Yazaki, T.; Sobue, R.; Hirano, M.; Fukuda, M.; Kojima, S.; Matsuyama, T. Human herpesvirus-6 infection in bone marrow transplantation. Blood 1991, 78, 1381–1384. [Google Scholar] [CrossRef] [Green Version]
- Ljungman, P.; Wang, F.Z.; Clark, D.A.; Emery, V.C.; Remberger, M.; Ringden, O.; Linde, A. High levels of human herpesvirus 6 DNA in peripheral blood leucocytes are correlated to platelet engraftment and disease in allogeneic stem cell transplant patients. Br. J. Haematol. 2000, 111, 774–781. [Google Scholar]
- Zerr, D.M.; Corey, L.; Kim, H.W.; Huang, M.L.; Nguy, L.; Boeckh, M. Clinical outcomes of human herpesvirus 6 reactivation after hematopoietic stem cell transplantation. Clin. Infect. Dis. 2005, 40, 932–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerdemann, U.; Keukens, L.; Keirnan, J.M.; Katari, U.L.; Nguyen, C.T.; de Pagter, A.P.; Ramos, C.A.; Kennedy-Nasser, A.; Gottschalk, S.M.; Heslop, H.E.; et al. Immunotherapeutic strategies to prevent and treat human herpesvirus 6 reactivation after allogeneic stem cell transplantation. Blood 2013, 121, 207–218. [Google Scholar] [CrossRef] [Green Version]
- Verhoeven, D.H.; Claas, E.C.; Jol-van der Zijde, C.M.; Thijssen, J.C.; Lankester, A.C.; Bredius, R.G.; Putter, H.; Kroes, A.C.; Egeler, R.M.; Schilham, M.W.; et al. Reactivation of Human Herpes Virus-6 After Pediatric Stem Cell Transplantation: Risk Factors, Onset, Clinical Symptoms and Association With Severity of Acute Graft-Versus-Host Disease. Pediatr. Infect. Dis. J. 2015, 34, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Hentrich, M.; Oruzio, D.; Jager, G.; Schlemmer, M.; Schleuning, M.; Schiel, X.; Hiddemann, W.; Kolb, H.J. Impact of human herpesvirus-6 after haematopoietic stem cell transplantation. Br. J. Haematol. 2005, 128, 66–72. [Google Scholar] [CrossRef]
- Zerr, D.M.; Boeckh, M.; Delaney, C.; Martin, P.J.; Xie, H.; Adler, A.L.; Huang, M.L.; Corey, L.; Leisenring, W.M. HHV-6 reactivation and associated sequelae after hematopoietic cell transplantation. Biol. Blood Marrow Transplant. 2012, 18, 1700–1708. [Google Scholar] [CrossRef] [Green Version]
- Zerr, D.M. Human Herpesvirus 6B in the Transplant Recipient: When to Worry, When to Act. J. Pediatr. Infect. Dis. Soc. 2018, 7, S75–S78. [Google Scholar] [CrossRef]
- Phan, T.L.; Carlin, K.; Ljungman, P.; Politikos, I.; Boussiotis, V.; Boeckh, M.; Shaffer, M.L.; Zerr, D.M. Human Herpesvirus-6B Reactivation Is a Risk Factor for Grades II to IV Acute Graft-versus-Host Disease after Hematopoietic Stem Cell Transplantation: A Systematic Review and Meta-Analysis. Biol. Blood Marrow Transplant. 2018, 24, 2324–2336. [Google Scholar] [CrossRef] [Green Version]
- Ogata, M.; Kikuchi, H.; Satou, T.; Kawano, R.; Ikewaki, J.; Kohno, K.; Kashima, K.; Ohtsuka, E.; Kadota, J. Human herpesvirus 6 DNA in plasma after allogeneic stem cell transplantation: Incidence and clinical significance. J. Infect. Dis. 2006, 193, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Seeley, W.W.; Marty, F.M.; Holmes, T.M.; Upchurch, K.; Soiffer, R.J.; Antin, J.H.; Baden, L.R.; Bromfield, E.B. Post-transplant acute limbic encephalitis: Clinical features and relationship to HHV6. Neurology 2007, 69, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Vu, T.; Carrum, G.; Hutton, G.; Heslop, H.E.; Brenner, M.K.; Kamble, R. Human herpesvirus-6 encephalitis following allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2007, 39, 705–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogata, M.; Satou, T.; Kadota, J.; Saito, N.; Yoshida, T.; Okumura, H.; Ueki, T.; Nagafuji, K.; Kako, S.; Uoshima, N.; et al. Human herpesvirus 6 (HHV-6) reactivation and HHV-6 encephalitis after allogeneic hematopoietic cell transplantation: A multicenter, prospective study. Clin. Infect. Dis. 2013, 57, 671–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobson, S.; Leibovitch, E.C. Human Herpesvirus 6 as a Viral Trigger in Mesial Temporal Lobe Epilepsy. J. Infect. Dis. 2015, 212, 1011–1013. [Google Scholar] [CrossRef]
- Kawamura, Y.; Nakayama, A.; Kato, T.; Miura, H.; Ishihara, N.; Ihira, M.; Takahashi, Y.; Matsuda, K.; Yoshikawa, T. Pathogenic Role of Human Herpesvirus 6B Infection in Mesial Temporal Lobe Epilepsy. J. Infect. Dis. 2015, 212, 1014–1021. [Google Scholar] [CrossRef] [Green Version]
- Kawamura, Y.; Sugata, K.; Ihira, M.; Mihara, T.; Mutoh, T.; Asano, Y.; Yoshikawa, T. Different characteristics of human herpesvirus 6 encephalitis between primary infection and viral reactivation. J. Clin. Virol. 2011, 51, 12–19. [Google Scholar] [CrossRef]
- Ogata, M.; Fukuda, T.; Teshima, T. Human herpesvirus-6 encephalitis after allogeneic hematopoietic cell transplantation: What we do and do not know. Bone Marrow Transplant. 2015, 50, 1030–1036. [Google Scholar] [CrossRef]
- Ogata, M.; Satou, T.; Kawano, R.; Takakura, S.; Goto, K.; Ikewaki, J.; Kohno, K.; Ikebe, T.; Ando, T.; Miyazaki, Y.; et al. Correlations of HHV-6 viral load and plasma IL-6 concentration with HHV-6 encephalitis in allogeneic stem cell transplant recipients. Bone Marrow Transplant. 2010, 45, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Bhanushali, M.J.; Kranick, S.M.; Freeman, A.F.; Cuellar-Rodriguez, J.M.; Battiwalla, M.; Gea-Banacloche, J.C.; Hickstein, D.D.; Pavletic, S.; Fahle, G.; Nath, A. Human herpes 6 virus encephalitis complicating allogeneic hematopoietic stem cell transplantation. Neurology 2013, 80, 1494–1500. [Google Scholar] [CrossRef] [Green Version]
- Howell, K.B.; Tiedemann, K.; Haeusler, G.; Mackay, M.T.; Kornberg, A.J.; Freeman, J.L.; Harvey, A.S. Symptomatic generalized epilepsy after HHV6 posttransplant acute limbic encephalitis in children. Epilepsia 2012, 53, e122–e126. [Google Scholar] [CrossRef]
- Miura, H.; Kawamura, Y.; Hattori, F.; Tanaka, M.; Kudo, K.; Ihira, M.; Yatsuya, H.; Takahashi, Y.; Kojima, S.; Sakaguchi, H.; et al. Human herpesvirus-6B infection in pediatric allogenic hematopoietic stem cell transplant patients: Risk factors and encephalitis. Transpl. Infect. Dis. 2020, 22, e13203. [Google Scholar] [CrossRef]
- Zerr, D.M.; Fann, J.R.; Breiger, D.; Boeckh, M.; Adler, A.L.; Xie, H.; Delaney, C.; Huang, M.L.; Corey, L.; Leisenring, W.M. HHV-6 reactivation and its effect on delirium and cognitive functioning in hematopoietic cell transplantation recipients. Blood 2011, 117, 5243–5249. [Google Scholar] [CrossRef]
- Asano, Y.; Yoshikawa, T.; Suga, S.; Yazaki, T.; Hata, T.; Nagai, T.; Kajita, Y.; Ozaki, T.; Yoshida, S. Viremia and neutralizing antibody response in infants with exanthem subitum. J. Pediatr. 1989, 114, 535–539. [Google Scholar] [CrossRef]
- Tanaka, N.; Kimura, H.; Hoshino, Y.; Kato, K.; Yoshikawa, T.; Asano, Y.; Horibe, K.; Kojima, S.; Morishima, T. Monitoring four herpesviruses in unrelated cord blood transplantation. Bone Marrow Transplant. 2000, 26, 1193–1197. [Google Scholar] [CrossRef] [Green Version]
- Ihira, M.; Ohta, A.; Sugata, K.; Suga, S.; Asano, Y.; Yoshikawa, T. Loop-mediated isothermal amplification for discriminating between human herpesvirus 6 A and B. J. Virol. Methods 2008, 154, 223–225. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, Y.; Ohashi, M.; Asahito, H.; Takahashi, Y.; Kojima, S.; Yoshikawa, T. Posterior reversible encephalopathy syndrome in a child with post-transplant HHV-6B encephalitis. Bone Marrow Transplant. 2012, 47, 1381–1382. [Google Scholar] [CrossRef] [Green Version]
- Deweer, B.; Lehericy, S.; Pillon, B.; Baulac, M.; Chiras, J.; Marsault, C.; Agid, Y.; Dubois, B. Memory disorders in probable Alzheimer’s disease: The role of hippocampal atrophy as shown with MRI. J. Neurol. Neurosurg. Psychiatry 1995, 58, 590–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurvits, T.V.; Shenton, M.E.; Hokama, H.; Ohta, H.; Lasko, N.B.; Gilbertson, M.W.; Orr, S.P.; Kikinis, R.; Jolesz, F.A.; McCarley, R.W.; et al. Magnetic resonance imaging study of hippocampal volume in chronic, combat-related posttraumatic stress disorder. Biol. Psychiatry 1996, 40, 1091–1099. [Google Scholar] [CrossRef] [Green Version]
- Watson, C.; Jack, C.R., Jr.; Cendes, F. Volumetric Magnetic Resonance Imaging: Clinical Applications and Contributions to the Understanding of Temporal Lobe Epilepsy. JAMA Neurol. 1997, 54, 1521–1531. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.A.; Koo, S.; Guzman Suarez, B.B.; Ho, V.T.; Cutler, C.; Koreth, J.; Armand, P.; Alyea, E.P., 3rd; Baden, L.R.; Antin, J.H.; et al. Cord-blood hematopoietic stem cell transplant confers an increased risk for human herpesvirus-6-associated acute limbic encephalitis: A cohort analysis. Biol. Blood Marrow Transplant. 2012, 18, 1638–1648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, Y.; Thomas, S.; Lee, B.K. Parent-reported prevalence of food allergies in children with autism spectrum disorder: National health interview survey, 2011-2015. Autism Res. 2019, 12, 802–805. [Google Scholar] [CrossRef] [PubMed]
- Mueller, S.G.; Schuff, N.; Yaffe, K.; Madison, C.; Miller, B.; Weiner, M.W. Hippocampal atrophy patterns in mild cognitive impairment and Alzheimer’s disease. Hum. Brain Mapp. 2010, 31, 1339–1347. [Google Scholar] [CrossRef] [Green Version]
- Natsuko, I.; Tsukasa, H.; Masaki, Y.; Naoki, H.; Yuko, Y.; Masanori, N.; Hiroshi, Y.; Nobuhiro, S.; Norio, S.; Hiroyuki, T. HHV-6 encephalitis may complicate the early phase after allogeneic hematopoietic stem cell transplantation: Detection by qualitative multiplex PCR and subsequent quantitative real-time PCR. J. Med. Virol. 2016, 88, 319–323. [Google Scholar] [CrossRef]
- Silva, G.; Martins, C.; Moreira da Silva, N.; Vieira, D.; Costa, D.; Rego, R.; Fonseca, J.; Silva Cunha, J.P. Automated volumetry of hippocampus is useful to confirm unilateral mesial temporal sclerosis in patients with radiologically positive findings. Neuroradiol. J. 2017, 30, 318–323. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | HHV-6B Infection (n = 8) | No HHV-6B Infection (n = 12) | p-Value |
|---|---|---|---|
| Median age (range), years | 10.5 (3–15) | 8.5 (2–14) | 0.416 |
| Sex | 0.158 | ||
| Male | 7 | 6 | |
| Female | 1 | 6 | |
| Underlying disease | 0.112 | ||
| Hematologic malignancy | 5 | 3 | |
| Solid tumor | 2 | 2 | |
| Other | 1 | 7 | |
| Transplant type | 0.450 | ||
| BM | 6 | 10 | |
| PBSC | 1 | 2 | |
| CB | 1 | 0 | |
| Donor allotype | 1.000 | ||
| Related | 4 | 7 | |
| Unrelated | 2 | 3 | |
| TBI | 1.000 | ||
| Yes | 6 | 10 | |
| No | 2 | 2 | |
| Duration between transplant and MRI examination Median (range), days | |||
| Before | −16 (−12 to −57) | −22 (−13 to −35) | 0.129 |
| After | 74 (26 to 153) | 87 (43 to 239) | 0.335 |
| Patient | Age Years/Sex | Underlying Disease | Transplant Type | TBI | CNS Symptoms | HHV-6B DNA in Whole Blood a (Day of Sample b) | Isolation of HHV-6B (Day of Sample b) | Median Duration between Transplant and MRI Examination b before/after | Hippocampal Volume Ratio | |
|---|---|---|---|---|---|---|---|---|---|---|
| Right | Left | |||||||||
| 1 | 12/M | CML | BM | Yes | No | 61,300 (18) | Yes (18) | −16/84 | 0.83 | 0.88 |
| 2 | 5/M | MDS | BM | Yes | No | 104,600 (19) | No | −57/153 | 0.84 | 0.89 |
| 3 | 10/F | AML | BM | Yes | Yes | 44,600 (12) | No | −12/28 | 0.89 | 0.89 |
| 4 | 6/M | Adrenal tumor | PBSC | No | No | 12,200 (18) | No | −16/69 | 0.90 | 0.86 |
| 5 | 3/M | NB | CB | Yes | No | 348,400 (22) | Yes (13) | −15/126 | 0.96 | 0.98 |
| 6 | 15/M | AA | BM | No | No | Not detected | Yes (26) | −16/79 | 0.99 | 0.95 |
| 7 | 15/M | CML | BM | Yes | No | 85,100 (47) | Yes (47) | −16/57 | 1.01 | 0.99 |
| 8 | 11/M | ALL | BM | Yes | Yes | 14,462,400 (17) | No | −21/26 | 1.02 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyake, M.; Kawamura, Y.; Ishihara, N.; Suzuki, S.; Miura, H.; Sakaguchi, Y.; Tanaka, M.; Takahashi, Y.; Kojima, S.; Toyama, H.; et al. Hippocampal Atrophy in Pediatric Transplant Recipients with Human Herpesvirus 6B. Microorganisms 2021, 9, 776. https://doi.org/10.3390/microorganisms9040776
Miyake M, Kawamura Y, Ishihara N, Suzuki S, Miura H, Sakaguchi Y, Tanaka M, Takahashi Y, Kojima S, Toyama H, et al. Hippocampal Atrophy in Pediatric Transplant Recipients with Human Herpesvirus 6B. Microorganisms. 2021; 9(4):776. https://doi.org/10.3390/microorganisms9040776
Chicago/Turabian StyleMiyake, Misa, Yoshiki Kawamura, Naoko Ishihara, Shigetaka Suzuki, Hiroki Miura, Yoko Sakaguchi, Masaharu Tanaka, Yoshiyuki Takahashi, Seiji Kojima, Hiroshi Toyama, and et al. 2021. "Hippocampal Atrophy in Pediatric Transplant Recipients with Human Herpesvirus 6B" Microorganisms 9, no. 4: 776. https://doi.org/10.3390/microorganisms9040776