Risk of Hepatitis E among Persons Who Inject Drugs in Hong Kong: A Qualitative and Quantitative Serological Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Controls
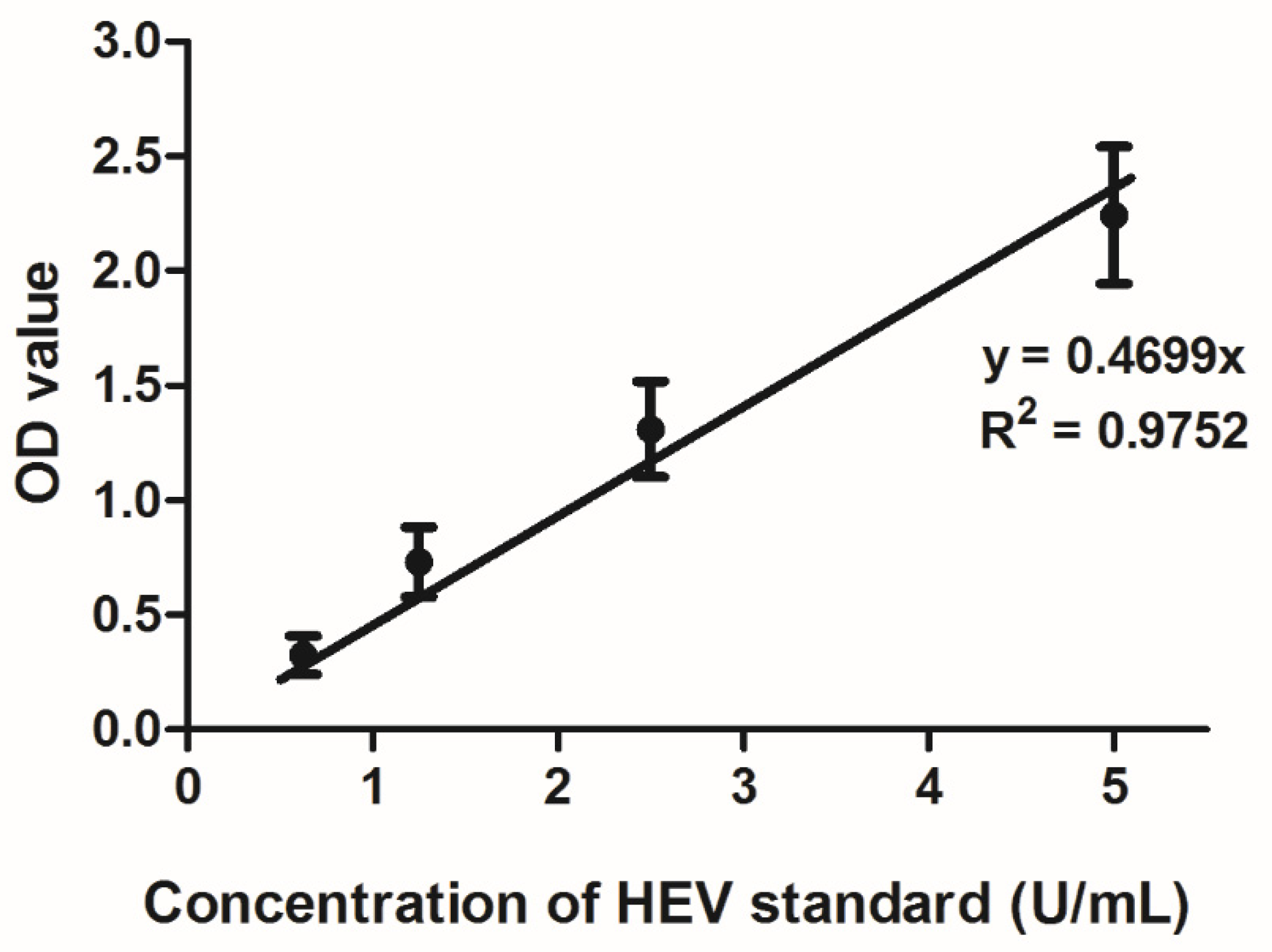
2.2. Hepatitis E Serology
2.3. Hepatitis E Nucleic Acid Detection
2.4. Statistical Analysis
3. Results
3.1. Characteristics of PWIDs and Organ Donors
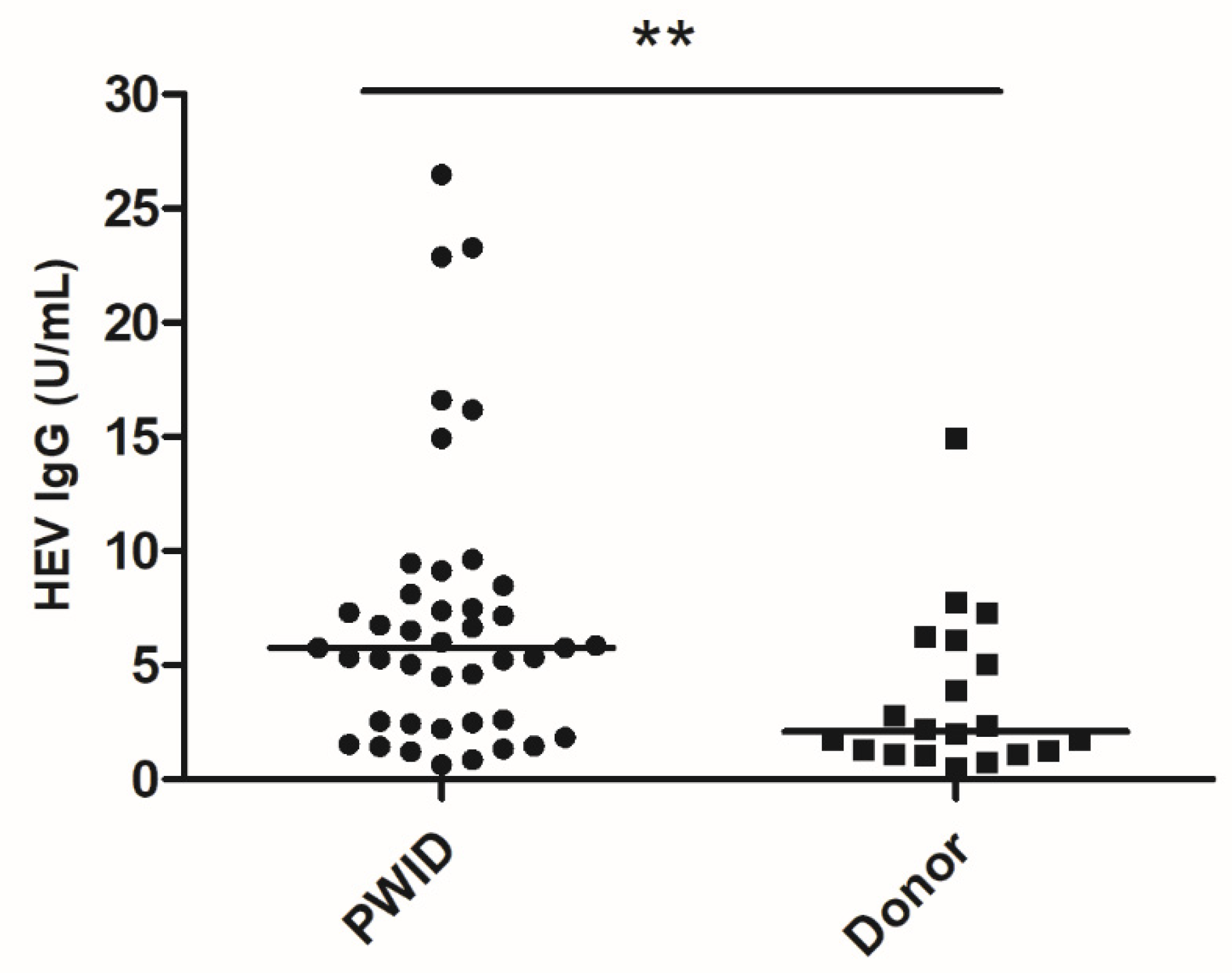
3.2. HEV IgG Quantitation
3.3. Bivariable and Multiple Regression Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rein, D.B.; Stevens, G.A.; Theaker, J.; Wittenborn, J.S.; Wiersma, S.T. The global burden of hepatitis E virus genotypes 1 and 2 in 2005. Hepatology 2012, 55, 988–997. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.B.; Simmonds, P.; International Committee on Taxonomy of Viruses Hepeviridae Study Group; Jameel, S.; Emerson, S.U.; Harrison, T.J.; Meng, X.J.; Okamoto, H.; Van der Poel, W.H.; Purdy, M.A. Consensus proposals for classification of the family Hepeviridae. J. Gen. Virol. 2014, 95, 2223–2232. [Google Scholar] [CrossRef] [PubMed]
- Sridhar, S.; Lo, S.K.; Xing, F.; Yang, J.; Ye, H.; Chan, J.F.; Teng, J.L.; Huang, C.; Yip, C.C.; Lau, S.K.; et al. Clinical characteristics and molecular epidemiology of hepatitis E in Shenzhen, China: A shift toward foodborne transmission of hepatitis E virus infection. Emerg. Microbes Infect. 2017, 6, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisano, M.B.; Martinez-Wassaf, M.G.; Mirazo, S.; Fantilli, A.; Arbiza, J.; Debes, J.D.; Re, V.E. Hepatitis E virus in South America: The current scenario. Liver Int. 2018, 38, 1536–1546. [Google Scholar] [CrossRef] [Green Version]
- Lapa, D.; Capobianchi, M.R.; Garbuglia, A.R. Epidemiology of Hepatitis E Virus in European Countries. Int. J. Mol. Sci. 2015, 16, 25711–25743. [Google Scholar] [CrossRef] [Green Version]
- Sridhar, S.; Yip, C.C.Y.; Wu, S. Rat Hepatitis E Virus as Cause of Persistent Hepatitis after Liver Transplant. Emerg. Infect. Dis. 2018, 24, 2241. [Google Scholar] [CrossRef] [Green Version]
- Sridhar, S.; Yip, C.C.; Wu, S.; Chew, N.F.; Leung, K.H.; Chan, J.F.; Zhao, P.S.; Chan, W.M.; Poon, R.W.; Tsoi, H.W.; et al. Transmission of rat hepatitis E virus infection to humans in Hong Kong: A clinical and epidemiological analysis. Hepatology 2020. [Google Scholar] [CrossRef]
- Hewitt, P.E.; Ijaz, S.; Brailsford, S.R.; Brett, R.; Dicks, S.; Haywood, B.; Kennedy, I.T.; Kitchen, A.; Patel, P.; Poh, J.; et al. Hepatitis E virus in blood components: A prevalence and transmission study in southeast England. Lancet 2014, 384, 1766–1773. [Google Scholar] [CrossRef] [Green Version]
- Sridhar, S.; Cheng, V.C.; Wong, S.C.; Yip, C.C.; Wu, S.; Lo, A.W.; Leung, K.H.; Mak, W.W.; Cai, J.P.; Li, X.; et al. Donor-Derived Genotype 4 Hepatitis E Virus Infection, Hong Kong, China, 2018. Emerg. Infect. Dis. 2019, 25, 425. [Google Scholar] [CrossRef]
- Goel, A.; Vijay, H.J.; Katiyar, H.; Aggarwal, R. Prevalence of hepatitis E viraemia among blood donors: A systematic review. Vox Sang. 2020, 115, 120–132. [Google Scholar] [CrossRef]
- Domanovic, D.; Tedder, R.; Blumel, J.; Zaaijer, H.; Gallian, P.; Niederhauser, C.; Sauleda Oliveras, S.; O’Riordan, J.; Boland, F.; Harritshoj, L.; et al. Hepatitis E and blood donation safety in selected European countries: A shift to screening? Eurosurveill 2017, 22, 30514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- British Transplantation Guidelines. Guidelines for Hepatitis E and Solid Organ Transplantation. Available online: https://bts.org.uk/wp-content/uploads/2017/05/BTS-HEV-Guideline-CONSULTATION_DRAFT.pdf (accessed on 8 September 2018).
- Yrondi, A.; Salles, J.; Peron, J.M.; Sporer, M.; Taib, S.; Gallini, A.; Noilhan, C.; Dimeglio, C.; Entajan, F.; Crequy, M.; et al. The Prevalence of Hepatitis E in a Patient Cohort Presenting With Addictive Injection Behavior. Front. Psychiatry 2019, 10, 832. [Google Scholar] [CrossRef] [PubMed]
- Mellgren, A.; Karlsson, M.; Karlsson, M.; Lagging, M.; Wejstal, R.; Norder, H. High seroprevalence against hepatitis E virus in patients with chronic hepatitis C virus infection. J. Clin. Virol. 2017, 88, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Vilibic-Cavlek, T.; Vilibic, M.; Kolaric, B.; Jemersic, L.; Kucinar, J.; Barbic, L.; Bagaric, A.; Stevanovic, V.; Tabain, I.; Sviben, M.; et al. Seroepidemiology of Hepatitis E in Selected Population Groups in Croatia: A Prospective Pilot Study. Zoonoses Public Health 2016, 63, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, R.; Collier, M.G.; Kamili, S.; Drobeniuc, J.; Cuevas-Mota, J.; Garfein, R.S.; Teshale, E. Hepatitis E virus among persons who inject drugs, San Diego, California, USA, 2009–2010. Emerg. Infect. Dis. 2013, 19, 1664–1666. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.L.; Yarbough, P.O.; Vlahov, D.; Tsarev, S.A.; Nelson, K.E.; Saah, A.J.; Purcell, R.H. Seroreactivity to hepatitis E virus in areas where the disease is not endemic. J. Clin. Microbiol. 1997, 35, 1244–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sylvan, S.P. The high rate of antibodies to hepatitis E virus in young, intravenous drug-abusers with acute hepatitis B-virus infection in a Swedish community: A study of hepatitis markers in individuals with intravenously or sexually acquired hepatitis B-virus infection. Scand. J. Infect. Dis. 1998, 30, 429–430. [Google Scholar] [CrossRef]
- Gessoni, G.; Manoni, F. Hepatitis E virus infection in north-east Italy: Serological study in the open population and groups at risk. J. Viral Hepat. 1996, 3, 197–202. [Google Scholar] [CrossRef]
- Christensen, P.B.; Engle, R.E.; Jacobsen, S.E.; Krarup, H.B.; Georgsen, J.; Purcell, R.H. High prevalence of hepatitis E antibodies among Danish prisoners and drug users. J. Med. Virol. 2002, 66, 49–55. [Google Scholar] [CrossRef]
- Fainboim, H.; Gonzalez, J.; Fassio, E.; Martinez, A.; Otegui, L.; Eposto, M.; Cahn, P.; Marino, R.; Landeira, G.; Suaya, G.; et al. Prevalence of hepatitis viruses in an anti-human immunodeficiency virus-positive population from Argentina. A multicentre study. J. Viral Hepat. 1999, 6, 53–57. [Google Scholar] [CrossRef]
- Balayan, M.S.; Fedorova, O.E.; Mikhailov, M.I.; Rytick, P.G.; Eremin, V.F.; Danilova, T.I.; Shevelev, B.I.; Gorbacheva, E.C.; Pankova, G.Y. Antibody to hepatitis E virus in HIV-infected individuals and AIDS patients. J. Viral Hepat. 1997, 4, 279–283. [Google Scholar] [CrossRef]
- Kaba, M.; Brouqui, P.; Richet, H.; Badiaga, S.; Gallian, P.; Raoult, D.; Colson, P. Hepatitis E virus infection in sheltered homeless persons, France. Emerg. Infect. Dis. 2010, 16, 1761–1763. [Google Scholar] [CrossRef] [PubMed]
- Trinta, K.S.; Liberto, M.I.; de Paula, V.S.; Yoshida, C.F.; Gaspar, A.M. Hepatitis E virus infection in selected Brazilian populations. Mem. Inst. Oswaldo Cruz 2001, 96, 25–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsoi, W.C.; Zhu, X.; To, A.P.; Holmberg, J. Hepatitis E virus infection in Hong Kong blood donors. Vox Sang. 2020, 115, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.C.W.; Kwok, K.; Hung, T.N.; Chan, P.K.S. Molecular Epidemiology and Strain Comparison between Hepatitis E Viruses in Human Sera and Pig Livers during 2014 to 2016 in Hong Kong. J. Clin. Microbiol. 2017, 55, 1408–1415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, B.; Cai, G.F.F.; Lv, H.K.K.; Xu, S.F.F.; Wang, Z.T.T.; Jiang, Z.G.G.; Hu, C.G.G.; Chen, Y.D.D. Factors Correlating to the Development of Hepatitis C Virus Infection among Drug Users-Findings from a Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2345. [Google Scholar] [CrossRef] [Green Version]
- Aitken, C.K.; Agius, P.A.; Higgs, P.G.; Stoove, M.A.; Bowden, D.S.; Dietze, P.M. The effects of needle-sharing and opioid substitution therapy on incidence of hepatitis C virus infection and reinfection in people who inject drugs. Epidemiol. Infect. 2017, 145, 796–801. [Google Scholar] [CrossRef] [Green Version]
- Abravanel, F.; Lhomme, S.; Chapuy-Regaud, S.; Mansuy, J.M.; Muscari, F.; Sallusto, F.; Rostaing, L.; Kamar, N.; Izopet, J. Hepatitis E virus reinfections in solid-organ-transplant recipients can evolve into chronic infections. J. Infect. Dis. 2014, 209, 1900–1906. [Google Scholar] [CrossRef]
- Liu, K.S.H.; Seto, W.K.; Lau, E.H.Y.; Wong, D.K.; Lam, Y.F.; Cheung, K.S.; Mak, L.Y.; Ko, K.L.; To, W.P.; Law, M.W.K.; et al. A Territorywide Prevalence Study on Blood-Borne and Enteric Viral Hepatitis in Hong Kong. J. Infect. Dis. 2019, 219, 1924–1933. [Google Scholar] [CrossRef]
- Chiu, D.M.; Chan, M.C.; Yeung, A.C.; Ngai, K.L.; Chan, P.K. Seroprevalence of hepatitis E virus in Hong Kong, 2008–2009. J. Med. Virol. 2013, 85, 459–461. [Google Scholar] [CrossRef]
- Rivero-Juarez, A.; Frias, M.; Lopez-Lopez, P.; de Los Angeles Risalde, M.; Brieva, T.; Machuca, I.; Camacho, A.; Martinez-Peinado, A.; Gomez-Villamandos, J.C.; Rivero, A. Hepatitis E Virus (HEV) Infection in Anti-HEV Immunoglobulin G-Carrying Patients After Successful Hepatitis C Virus Treatment: Reactivation or Reinfection? Clin. Infect. Dis. 2017, 64, 964–966. [Google Scholar] [CrossRef] [PubMed]
- Panning, M.; Basho, K.; Fahrner, A.; Neumann-Haefelin, C. Chronic hepatitis E after kidney transplantation with an antibody response suggestive of reinfection: A case report. BMC Infect. Dis. 2019, 19, 675. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Zhang, X.; Skinner, B. Analysis of IgG Anti-HEV Antibody Protective Levels During Hepatitis E Virus Reinfection in Experimentally Infected Rhesus Macaques. J. Infect. Dis. 2019, 219, 916–924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riveiro-Barciela, M.; Rando-Segura, A.; Barreira-Diaz, A.; Bes, M.; Ruzo, S.P.; Piron, M.; Quer, J.; Sauleda, S.; Rodriguez-Frias, F.; Esteban, R.; et al. Unexpected long-lasting anti-HEV IgM positivity: Is HEV antigen a better serological marker for hepatitis E infection diagnosis? J. Viral Hepat. 2020. [Google Scholar] [CrossRef]
- Solomon, S.S.; Srikrishnan, A.K.; McFall, A.M.; Kumar, M.S.; Saravanan, S.; Balakrishnan, P.; Solomon, S.; Thomas, D.L.; Sulkowski, M.S.; Mehta, S.H. Burden of Liver Disease among Community-Based People Who Inject Drugs (PWID) in Chennai, India. PLoS ONE 2016, 11, e0147879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, J.C.; Wong, G.L.; Yip, T.C.; Tse, Y.K.; Lam, K.L.; Lui, G.C.; Chan, H.L.; Wong, V.W. Chronic Hepatitis B Increases Liver-Related Mortality of Patients With Acute Hepatitis E: A Territorywide Cohort Study From 2000 to 2016. Clin. Infect. Dis. 2018, 67, 1278–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bricks, G.; Senise, J.F.; Pott-Jr, H.; Grandi, G.; Carnauba-Jr, D.; de Moraes, H.A.B.; Granato, C.F.H.; Castelo, A. Previous hepatitis E virus infection, cirrhosis and insulin resistance in patients with chronic hepatitis C. Braz. J. Infect. Dis. 2019, 23, 45–52. [Google Scholar] [CrossRef]
- Neukam, K.; Barreiro, P.; Macias, J.; Avellon, A.; Cifuentes, C.; Martin-Carbonero, L.; Echevarria, J.M.; Vargas, J.; Soriano, V.; Pineda, J.A. Chronic hepatitis E in HIV patients: Rapid progression to cirrhosis and response to oral ribavirin. Clin. Infect. Dis. 2013, 57, 465–468. [Google Scholar] [CrossRef] [Green Version]
- Peak, C.M.; Stous, S.S.; Healy, J.M.; Hofmeister, M.G.; Lin, Y.; Ramachandran, S.; Foster, M.; Kao, A.; McDonald, E.C. Homelessness and Hepatitis A—San Diego County, 2016–2018. Clin. Infect. Dis. 2019. [Google Scholar] [CrossRef]
- Social Indicators of Hong Kong. Homeless Persons Per 100,000 Population. Available online: https://www.socialindicators.org.hk/en/indicators/housing/8.10 (accessed on 25 March 2020).
- Pas, S.D.; Streefkerk, R.H.; Pronk, M.; de Man, R.A.; Beersma, M.F.; Osterhaus, A.D.; van der Eijk, A.A. Diagnostic performance of selected commercial HEV IgM and IgG ELISAs for immunocompromised and immunocompetent patients. J. Clin. Virol. 2013, 58, 629–634. [Google Scholar] [CrossRef]
- Cattoir, L.; Van Hoecke, F.; Van Maerken, T.; Nys, E.; Ryckaert, I.; De Boulle, M.; Geerts, A.; Verhelst, X.; Colle, I.; Hutse, V.; et al. Hepatitis E virus serology and PCR: Does the methodology matter? Arch. Virol. 2017, 162, 2625–2632. [Google Scholar] [CrossRef] [PubMed]
- Erbelding, E.J.; Vlahov, D.; Nelson, K.E.; Rompalo, A.M.; Cohn, S.; Sanchez, P.; Quinn, T.C.; Brathwaite, W.; Thomas, D.L. Syphilis serology in human immunodeficiency virus infection: Evidence for false-negative fluorescent treponemal testing. J. Infect. Dis. 1997, 176, 1397–1400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnegg, A.; Burgisser, P.; Andre, C.; Kenfak-Foguena, A.; Canellini, G.; Moradpour, D.; Abravanel, F.; Izopet, J.; Cavassini, M.; Darling, K.E. An analysis of the benefit of using HEV genotype 3 antigens in detecting anti-HEV IgG in a European population. PLoS ONE 2013, 8, e62980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Zhang, X.F.; Huang, S.J.; Wu, T.; Hu, Y.M.; Wang, Z.Z.; Wang, H.; Jiang, H.M.; Wang, Y.J.; Yan, Q.; et al. Long-term efficacy of a hepatitis E vaccine. N. Engl. J. Med. 2015, 372, 914–922. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Bivariable Analysis | Multiple Regression | ||||
|---|---|---|---|---|---|
| Variable | HEV IgG Positive /No. Tested (%) | Odds Ratio 2 | p-Value | Odds Ratio 2 | p-Value |
| Age (y) | 1.06 (1.02–1.09) 1 | <0.005 | 1.07 (1.03–1.10) 1 | <0.005 | |
| <35 | 1/11 (9) | 0.18 (0.02–1.44) | 0.106 | ||
| 35–44 | 17/66 (25.8) | 0.55 (0.28–1.07) | 0.076 | ||
| 45–54 | 16/57 (28.1) | 0.67 (0.34–1.33) | 0.251 | ||
| 55–64 | 19/32 (59.3) | 3.64 (1.65–8.01) | <0.005 | ||
| >65 | 9/16 (56.3) | 2.74 (0.97–7.78) | 0.057 | ||
| Sex | |||||
| Male | 52/150 (34.7) | 1.17 (0.51–2.65) | 0.711 | NA | NA |
| Female | 10/32 (31.3) | Ref | |||
| PWID | 42/91 (46.2) | 3.04 (1.59–5.79) | <0.005 | 3.43 (1.72–6.81) 1 | <0.005 |
| Donor | 20/91 (22) | Ref | |||
| Reference | Country; HEV IgG Assay | PWID HEV IgG Positive/No. Tested (%) | Control Group | Control Group HEV-IgG Positive/No. Tested (%) | Significant Difference between PWID and Control Groups? |
|---|---|---|---|---|---|
| [13] | France; Wantai | 22/52 (42.3%) | Blood donors; age- and sex-matched | 43/99 (43.4%) | No p = 0.890 |
| [14] | Sweden; Diapro | (26%) | HCV patients, but HCV acquired via blood transfusion; not age- and sex-matched | (48%) | Yes, but higher in transfusion-acquired group p < 0.020 |
| [15] | Croatia; Euroimmun | 3/49 (6.1%) | Healthcare professionals | 12/214 (5.6%) | No (p > 0.050) |
| [17] | USA; In-house assay | 68/295 (23%) | Blood donors; not age- and sex-matched | 64/300 (21.3%) | No (p = 0.614) |
| [18] | Sweden; Abbott | 21/34 (62%) | HBV carriers; older control group/ sex-matched | 9/36 (25%) | Yes p < 0.005 |
| [19] | Italy; Abbott | 15/279 (5.4%) | General population; not age- and sex-matched | 50/1889 (2.6%) | Yes p < 0.050 |
| [20] | Denmark; Abbott | 36/137 (26.3%) | Non-drug-using prisoners; not age- and sex-matched | N/A | No (p value not shown) |
| [24] | Brazil; Abbott | 12/102 (11.8%) | Blood donor; not age- and sex-matched | 4/93 (4.3%) | No (p = 0.070) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sridhar, S.; Chew, N.F.-S.; Situ, J.; Wu, S.; Chui, E.S.-H.; Lam, A.H.-Y.; Cai, J.-P.; Cheng, V.C.-C.; Yuen, K.-Y. Risk of Hepatitis E among Persons Who Inject Drugs in Hong Kong: A Qualitative and Quantitative Serological Analysis. Microorganisms 2020, 8, 675. https://doi.org/10.3390/microorganisms8050675
Sridhar S, Chew NF-S, Situ J, Wu S, Chui ES-H, Lam AH-Y, Cai J-P, Cheng VC-C, Yuen K-Y. Risk of Hepatitis E among Persons Who Inject Drugs in Hong Kong: A Qualitative and Quantitative Serological Analysis. Microorganisms. 2020; 8(5):675. https://doi.org/10.3390/microorganisms8050675
Chicago/Turabian StyleSridhar, Siddharth, Nicholas Foo-Siong Chew, Jianwen Situ, Shusheng Wu, Ernest Sing-Hong Chui, Athene Hoi-Ying Lam, Jian-Piao Cai, Vincent Chi-Chung Cheng, and Kwok-Yung Yuen. 2020. "Risk of Hepatitis E among Persons Who Inject Drugs in Hong Kong: A Qualitative and Quantitative Serological Analysis" Microorganisms 8, no. 5: 675. https://doi.org/10.3390/microorganisms8050675