Comparison of Four Commercial Screening Assays for the Detection of blaKPC, blaNDM, blaIMP, blaVIM, and blaOXA48 in Rectal Secretion Collected by Swabs

Abstract
:1. Introduction
2. Materials and Methods
2.1. Culture Based and Molecular Routine Methods for the Identification of CRE
2.2. Molecular Tests
2.2.1. Allplex™ Entero-DR Assay (Seegene Inc., Seoul, Korea)
2.2.2. Amplidiag® CARBAR+MCR (Mobidiag, Espoo, Finland)
2.2.3. AusDiagnostics MT CRE EU Assay (AusDiagnostics, Mascot NSW, Australia)
2.2.4. EasyScreen™ ESBL/CPO Detection Kit (Genetic Signatures, Newtown NSW, Australia)
3. Results
4. Discussion
Supplementary Files
Supplementary File 1Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Antimicrobial Resistance: Global Report on Surveillance 2014; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. Essential Medicines and Health Products. Prioritization of Pathogens to Guide Discovery, Research and Development of New Antibiotics for drug-Resistant Bacterial Infections, Including Tuberculosis; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Sheu, C.C.; Chang, Y.T.; Lin, S.Y.; Chen, Y.H.; Hsueh, P.R. Infections Caused by Carbapenem-Resistant Enterobacteriaceae: An Update on Therapeutic Options. Front. Microbiol. 2019, 10, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, H.; Qu, F.; Shan, B.; Huang, B.; Jia, W.; Chen, C.; Li, A.; Miao, M.; Zhang, X.; Bao, C.; et al. Detection of the mcr-1 Colistin Resistance Gene in Carbapenem-Resistant Enterobacteriaceae from Different Hospitals in China. Antimicrob. Agents Chemother. 2016, 82, 5033–5035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mediavilla, J.R.; Patrawalla, A.; Chen, L.; Chavda, K.D.; Mathema, B.; Vinnard, C.; Dever, L.L.; Kreiswirth, B.N. Colistin- and Carbapenem-Resistant Escherichia coli Harboring mcr-1 and blaNDM-5, Causing a Complicated Urinary Tract Infection in a Patient from the United States. MBio 2016, 7, e1191-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Q.; Zhang, P.; Zhao, D.; Jiang, Y.; Zhao, F.; Wang, Y.; Li, X.; Du, X.; Yu, Y. Emergence of tigecycline resistance in Escherichia coli co-producing MCR-1 and NDM-5 during tigecycline salvage treatment. Infect. Drug Resist. 2018, 11, 2241–2248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Queenan, A.M.; Bush, K. Carbapenemases: The versatile beta-lactamases. Clin. Microbiol. Rev. 2007, 20, 440–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livermore, D.M. Defining an extended-spectrum beta-lactamase. Clin. Microbiol. Infect. 2008, 14, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Poirel, L.; Pitout, J.D.; Nordmann, P. Carbapenemases: Molecular diversity and clinical consequences. Future Microbiol. 2007, 2, 501–512. [Google Scholar] [CrossRef]
- Walsh, T.R. Emerging carbapenemases: A global perspective. Int. J. Antimicrob. Agents 2010, 36, S8–S14. [Google Scholar] [CrossRef]
- Yang, Y.J.; Wu, P.J.; Livermore, D.M. Biochemical characterization of a β-lactamase that hydrolyzes penems and carbapenems from two Serratia marcescens isolates. Antimicrob. Agents Chemother. 1990, 34, 755–758. [Google Scholar] [CrossRef] [Green Version]
- Nordmann, P.; Mariotte, S.; Naas, T.; Labia, R.; Nicolas, M.H. Biochemical properties of a carbapenem-hydrolyzing β-lactamase for Enterobacter cloacae and cloning of the gene into Escherichia coli. Antimicrob. Agents Chemother. 1993, 37, 939–946. [Google Scholar] [CrossRef] [Green Version]
- Rasmussen, B.A.; Bush, K.; Keeney, D.; Yang, Y.; Hare, R.; O’Gara, C.; Medeiros, A.A. Characterization of IMI-1 β-lactamase, a class A carbapenem-hydrolyzing enzyme from Enterobacter cloacae. Antimicrob. Agents Chemother. 1996, 40, 2080–2086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambler, R.P. The structure of β-lactamases. Philos. Trans. R. Soc. Lond. B Biol. Sci. 1980, 289, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Nordmann, P.; Cuzon, G.; Naas, T. The real threat of Klebsiella pneumoniae carbapenemase-producing bacteria. Lancet Infect. Dis. 2009, 9, 228–236. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Surveillance of Antimicrobial Resistance in Europe—Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net) 2017; ECDC: Stockholm, Sweden, 2018.
- Peirano, G.; Lascols, C.; Hackel, M.; Hoban, D.J.; Pitout, J.D. Molecular epidemiology of Enterobacteriaceae that produce VIMs and IMPs from the SMART surveillance program. Diagn. Microbiol. Infect. Dis. 2014, 78, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, Y.; Peirano, G.; Motyl, M.R.; Adams, M.D.; Chen, L.; Kreiswirth, B.; DeVinney, R.; Pitout, J.D. Global Molecular Epidemiology of IMP-Producing Enterobacteriaceae. Antimicrob. Agents Chemother. 2017, 61, e02729-16. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.U.; Maryam, L.; Zarrilli, R. Structure, Genetics and Worldwide Spread of New Delhi Metallo-β-lactamase (NDM): A threat to public health. BMC Microbiol. 2017, 17, 101. [Google Scholar] [CrossRef] [Green Version]
- Poirel, L.; Héritier, C.; Tolün, V.; Nordmann, P. Emergence of oxacillinase-mediated resistance to imipenem in Klebsiella pneumoniae. Antimicrob. Agents Chemother. 2004, 48, 15–22. [Google Scholar] [CrossRef] [Green Version]
- Poirel, L.; Potron, A.; Nordmann, P. OXA-48-like carbapenemases: The phantom menace. J. Antimicrob. Chemother. 2012, 67, 1597–1606. [Google Scholar] [CrossRef] [Green Version]
- Pitout, J.D.; Laupland, K.B. Extended-spectrum β-lactamase-producing Enterobacteriaceae: An emerging public-health concern. Lancet Infect. Dis. 2008, 8, 159–166. [Google Scholar] [CrossRef]
- Baughman, R.P. The use of carbapenems in the treatment of serious infections. J. Intensive Care Med. 2009, 24, 230–241. [Google Scholar] [CrossRef]
- Deleo, F.R.; Chen, L.; Porcella, S.F.; Martens, C.A.; Kobayashi, S.D.; Porter, A.R.; Chavda, K.D.; Jacobs, M.R.; Mathema, B.; Olsen, R.J.; et al. Molecular dissection of the evolution of carbapenem-resistant multilocus sequence type 258 Klebsiella pneumoniae. Proc. Natl. Acad. Sci. USA 2014, 111, 4988–4993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carattoli, A. Resistance plasmid families in Enterobacteriaceae. Antimicrob. Agents Chemother. 2009, 53, 2227–2238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poirel, L.; Bonnin, R.A.; Nordmann, P. Genetic features of the widespread plasmid coding for the carbapenemase OXA-48. Antimicrob. Agents Chemother. 2012, 56, 559–562. [Google Scholar] [CrossRef] [Green Version]
- Mathers, A.J.; Peirano, G.; Pitout, J.D. The role of epidemic resistance plasmids and international high-risk clones in the spread of multidrug-resistant Enterobacteriaceae. Clin. Microbiol. Rev. 2015, 28, 565–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tada, T.; Miyoshi-Akiyama, T.; Dahal, R.K.; Mishra, S.K.; Ohara, H.; Shimada, K.; Kirikae, T.; Pokhrel, B.M. Dissemination of multidrug-resistant Klebsiella pneumoniae clinical isolates with various combinations of carbapenemases (NDM-1 and OXA-72) and 16S rRNA methylases (ArmA, RmtC and RmtF) in Nepal. Int. J. Antimicrob. Agents 2013, 42, 372–374. [Google Scholar] [CrossRef] [PubMed]
- Seiffert, S.N.; Marschall, J.; Perreten, V.; Carattoli, A.; Furrer, H.; Endimiani, A. Emergence of Klebsiella pneumoniae co-producing NDM-1, OXA-48, CTX-M-15, CMY-16, QnrA and ArmA in Switzerland. Int. J. Antimicrob. Agents 2014, 44, 260–262. [Google Scholar] [CrossRef] [PubMed]
- Kelly, A.M.; Mathema, B.; Larson, E.L. Carbapenem-resistant Enterobacteriaceae in the community: A scoping review. Int. J. Antimicrob. Agents 2017, 50, 127–134. [Google Scholar] [CrossRef]
- Agenzia Sanitaria e Sociale Regionale (ASSR) Emilia-Romagna. Indicazioni Pratiche e Protocolli Operativi per la Diagnosi, la Sorveglianza e il Controllo Degli Enterobatteri Produttori di Carbapenemasi Nelle Strutture Sanitarie e Socio-Sanitarie; ASSR: Bologna, Italy, 2017. [Google Scholar]
- Parker, V.A.; Logan, C.K.; Currie, B. Carbapenem-Resistant Enterobacteriaceae (CRE) Control and Prevention Toolkit; AHRQ Publication No. 14-0028; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2014.
- Gagliotti, C.; Ciccarese, V.; Sarti, M.; Giordani, S.; Barozzi, A.; Braglia, C.; Gallerani, C.; Gargiulo, R.; Lenzotti, G.; Manzi, O.; et al. Active surveillance for asymptomatic carriers of carbapenemase-producing Klebsiella pneumoniae in a hospital setting. J. Hosp. Infect. 2013, 83, 330–332. [Google Scholar] [CrossRef]
- Danial, J.; Noel, M.; Templeton, K.E.; Cameron, F.; Mathewson, F.; Smith, M.; Cepeda, J.A. Real-time evaluation of an optimized real-time PCR assay versus Brilliance chromogenic MRSA agar for the detection of meticillin-resistant Staphylococcus aureus from clinical specimens. J. Med. Microbiol. 2011, 60, 323–328. [Google Scholar] [CrossRef]
- Singh, K.; Mangold, K.A.; Wyant, K.; Schora, D.M.; Voss, B.; Kaul, K.L.; Hayden, M.K.; Chundi, V.; Peterson, L.R. Rectal screening for Klebsiella pneumoniae carbapenemases: Comparison of real-time PCR and culture using two selective screening agar plates. J. Clin. Microbiol. 2012, 50, 2596–2600. [Google Scholar] [CrossRef] [Green Version]
- Bakthavatchalam, Y.D.; Anandan, S.; Veeraraghavan, B. Laboratory Detection and Clinical Implication of Oxacillinase-48 like Carbapenemase: The Hidden Threat. J. Glob. Infect. Dis. 2016, 8, 41–50. [Google Scholar] [PubMed]
- Potron, A.; Poirel, L.; Rondinaud, E.; Nordmann, P. Intercontinental spread of OXA-48 beta-lactamase-producing Enterobacteriaceae over a 11-year period, 2001 to 2011. Eurosurveillance 2013, 18, e20549. [Google Scholar] [CrossRef] [PubMed]
- Del Bianco, F.; Morotti, M.; Pedna, M.F.; Farabegoli, P.; Sambri, V. Microbiological surveillance of plasmid mediated colistin resistance in human Enterobacteriaceae isolates in Romagna (Northern Italy): August 2016–July 2017. Int. J. Infect Dis. 2018, 69, 96–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaper, J.B.; Nataro, J.P.; Mobley, H.L. Pathogenic Escherichia coli. Nat. Rev. Microbiol. 2004, 2, 123–140. [Google Scholar] [CrossRef]
- Allocati, N.; Masulli, M.; Alexeyev, M.F.; Di Ilio, C. Escherichia coli in Europe: An overview. Int. J. Environ. Res. Public Health 2013, 10, 6235–6254. [Google Scholar] [CrossRef]
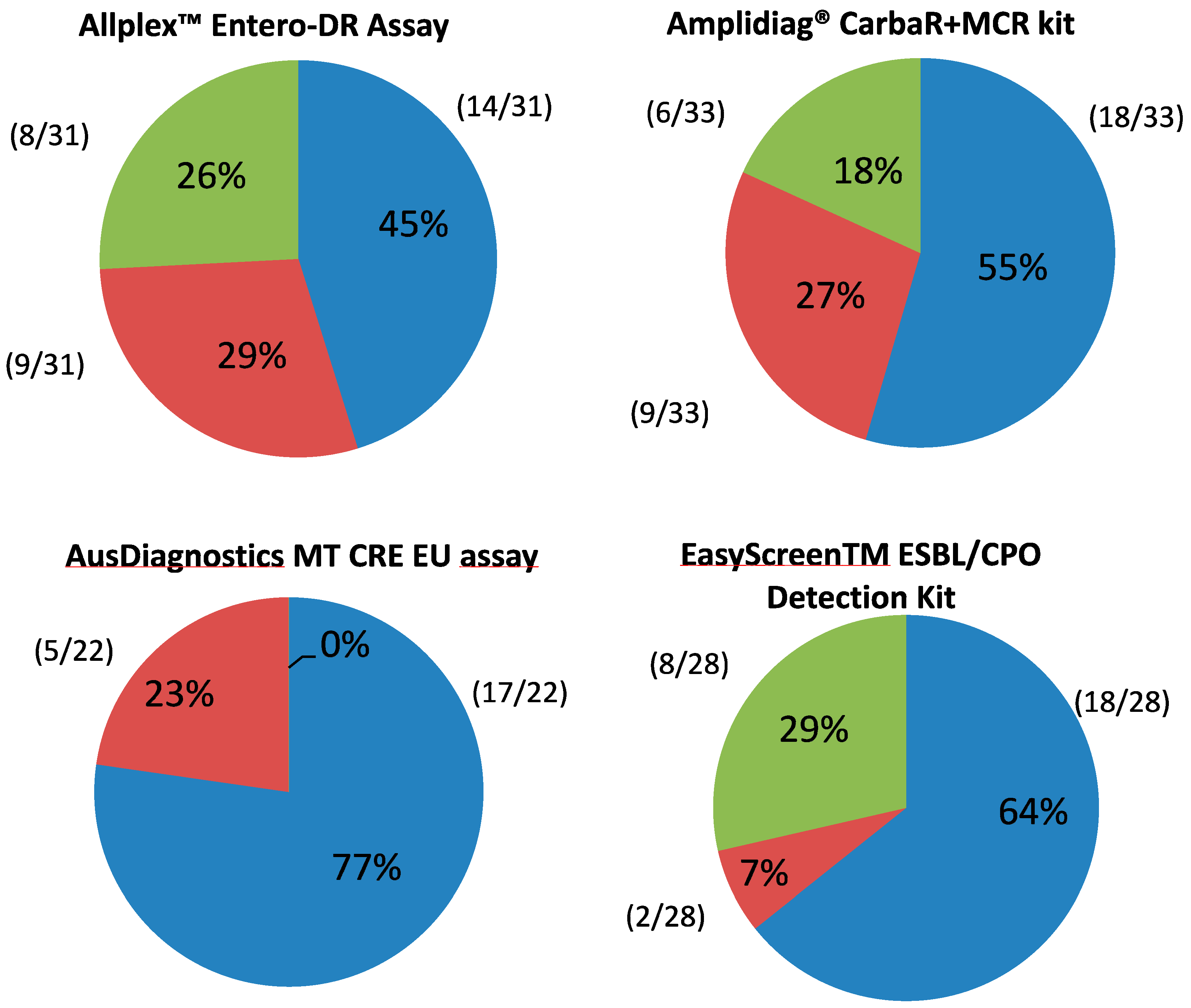
 Target concordant with routine screening but not in agreement with at least one other molecular test.
Target concordant with routine screening but not in agreement with at least one other molecular test.  Target not in agreement with routine screening but concordant with at least one other molecular test.
Target not in agreement with routine screening but concordant with at least one other molecular test.  Target not in agreement with either routine screening or any other test.
Target concordant with routine screening but not in agreement with at least one other molecular test. Target not in agreement with routine screening but concordant with at least one other molecular test. Target not in agreement with either routine screening or any other test.
Target not in agreement with either routine screening or any other test.
Target concordant with routine screening but not in agreement with at least one other molecular test. Target not in agreement with routine screening but concordant with at least one other molecular test. Target not in agreement with either routine screening or any other test.

{kind=link}
| Assay | Routine Screening Tests | |||
|---|---|---|---|---|
| Assay Results | Positive | Negative | Total | |
| Allplex Entero-DR assay | Positive | 25 | 17 | 42 |
| Negative | 0 | 940 | 940 | |
| Total | 25 | 957 | 982 | |
| Amplidiag CarbaR + MCR kit | Positive | 20 | 11 a | 31 a |
| Negative | 4 | 949 | 953 | |
| Total | 24 | 959 | 983 | |
| AusDiagnostics MT CRE EU assay | Positive | 19 | 5 | 24 |
| Negative | 0 | 810 | 810 | |
| Total | 19 | 815 | 834 | |
| EasyScreen ESBL/CPO Detection Kit | Positive | 22 | 5 | 27 |
| Negative | 0 | 751 | 751 | |
| Total | 22 | 756 | 778 | |
| Assay | Sensitivity | Specificity | PPV | NPV | Overall % Agreement | Kappa Statistic |
|---|---|---|---|---|---|---|
| (%[95%CI]) | (%[95%CI]) | (%[95%CI]) | (%[95%CI]) | (%[95%CI]) | ||
| Allplex | 100 | 98.22 | 59.52 | 100 | 98,27 | 0.74 |
| Entero-DR assay | (86.28–100) | (97.17–98.96) | (47.86–70.20) | (97.24–98.99) | ||
| Amplidiag | 83.33 | 98.85 | 64.52 | 99.58 | 98.48 | 0.72 |
| CARBAR + MCR kit | (62.62–95.26) | (97.96–99.43) | (49.59–77.07) | (98.98–99.83) | (97.50–99.14) | |
| AusDiagnostics | 100 | 99.39 | 79.17 | 100 | 99.4 | 0.88 |
| MT CRE EU assay | (82.35–100) | (98.57–99.80) | (61.33–90.10) | (98.61–99.81) | ||
| EasyScreen | 100 | 99.34 | 81.48 | 100 | 99.36 (98.51–99.79) | 0.89 |
| ESBL/CPO Detection Kit | (84.56–100) | (98.46–99.78) | (64.75–91.33) |
| Allplex Entero-DR Assay | Amplidiag CarbaR + MCR Kit | Ausdiagnostics MT CRE EU Assay | EasyScreen ESBL/CPO Detection Kit | |
|---|---|---|---|---|
| Sample throughput | up to 94 tests/batch | up to 64 tests/batch | 24 up to 64 tests/batch | up to 80 tests/batch |
| Hands on time | 45 min | 1 h | 20 min a | 3 h |
| Assay run time | 4 h | 5 h | 2 h a | 6 h |
| Extraction control | yes | yes | yes | yes |
| PCR control | yes | yes | yes | yes |
| intrinsic control | yes | no | yes | yes |
| Other targets | vanA; vanB; CTX-M | AcOXA; MCR 1/2; Guiana extended-spectrum (GES)-CPO; | SME; OXA-23,51,58-like; CTX-M group 1 and group 9; GES | TEM; DHA; CTX-M; CMY SHV; OXA 23; 51-like |
| Traceability | yes | yes | Depending on DNA extraction system | no |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Del Bianco, F.; Morotti, M.; Zannoli, S.; Dirani, G.; Fantini, M.; Pedna, M.F.; Farabegoli, P.; Sambri, V. Comparison of Four Commercial Screening Assays for the Detection of blaKPC, blaNDM, blaIMP, blaVIM, and blaOXA48 in Rectal Secretion Collected by Swabs. Microorganisms 2019, 7, 704. https://doi.org/10.3390/microorganisms7120704
Del Bianco F, Morotti M, Zannoli S, Dirani G, Fantini M, Pedna MF, Farabegoli P, Sambri V. Comparison of Four Commercial Screening Assays for the Detection of blaKPC, blaNDM, blaIMP, blaVIM, and blaOXA48 in Rectal Secretion Collected by Swabs. Microorganisms. 2019; 7(12):704. https://doi.org/10.3390/microorganisms7120704
Chicago/Turabian StyleDel Bianco, Francesca, Manuela Morotti, Silvia Zannoli, Giorgio Dirani, Michela Fantini, Maria Federica Pedna, Patrizia Farabegoli, and Vittorio Sambri. 2019. "Comparison of Four Commercial Screening Assays for the Detection of blaKPC, blaNDM, blaIMP, blaVIM, and blaOXA48 in Rectal Secretion Collected by Swabs" Microorganisms 7, no. 12: 704. https://doi.org/10.3390/microorganisms7120704