Human Immunodeficiency Virus Infected Patients are Not at Higher Risk for Hepatitis E Virus Infection: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategies and Selection Criteria
2.2. Selection of Studies
2.3. Data Extraction and Analysis
2.4. Assessment Quality of Studies
2.5. Statistical Analysis
3. Results
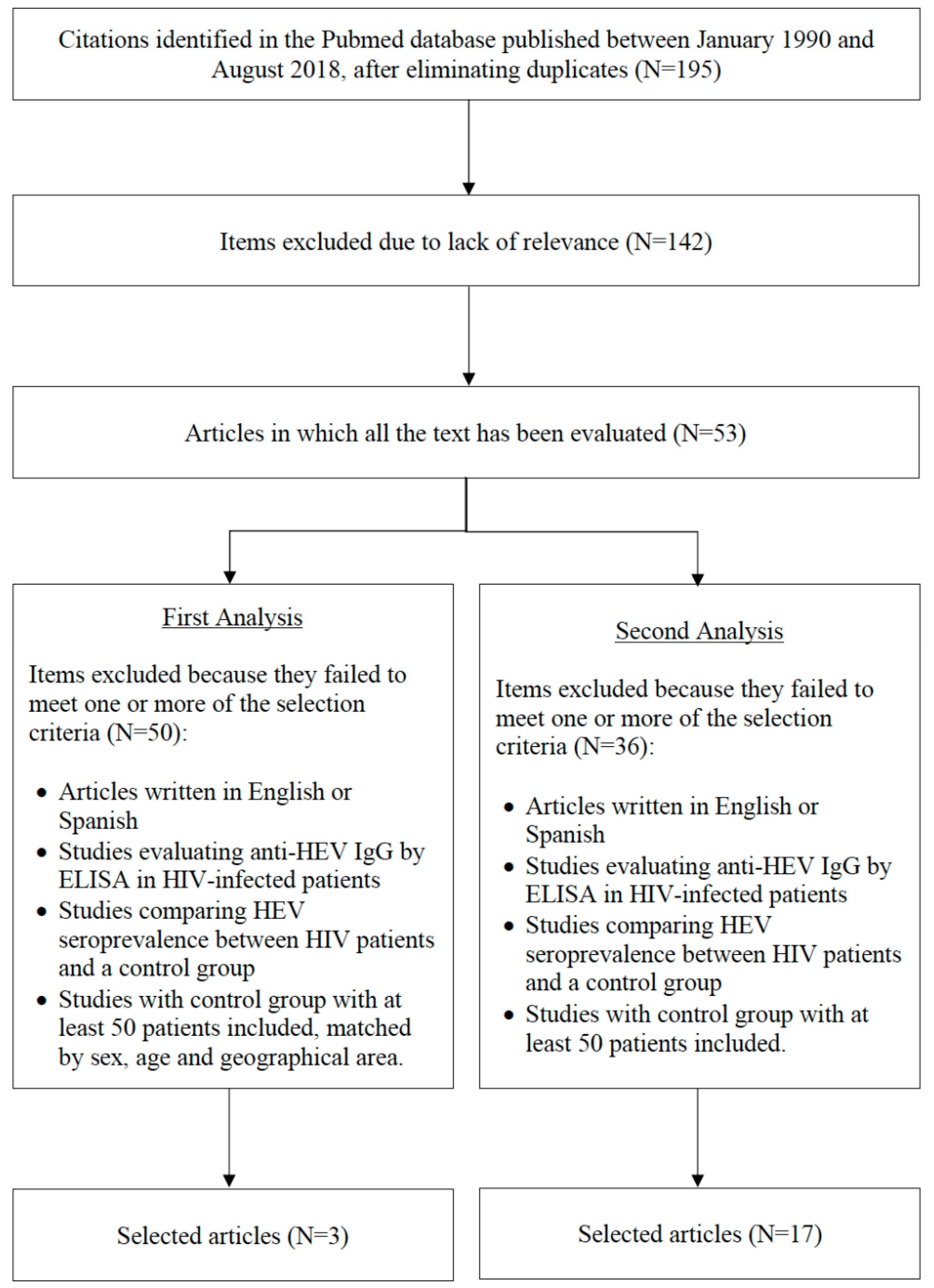
3.1. Data Recovery and Study Selection
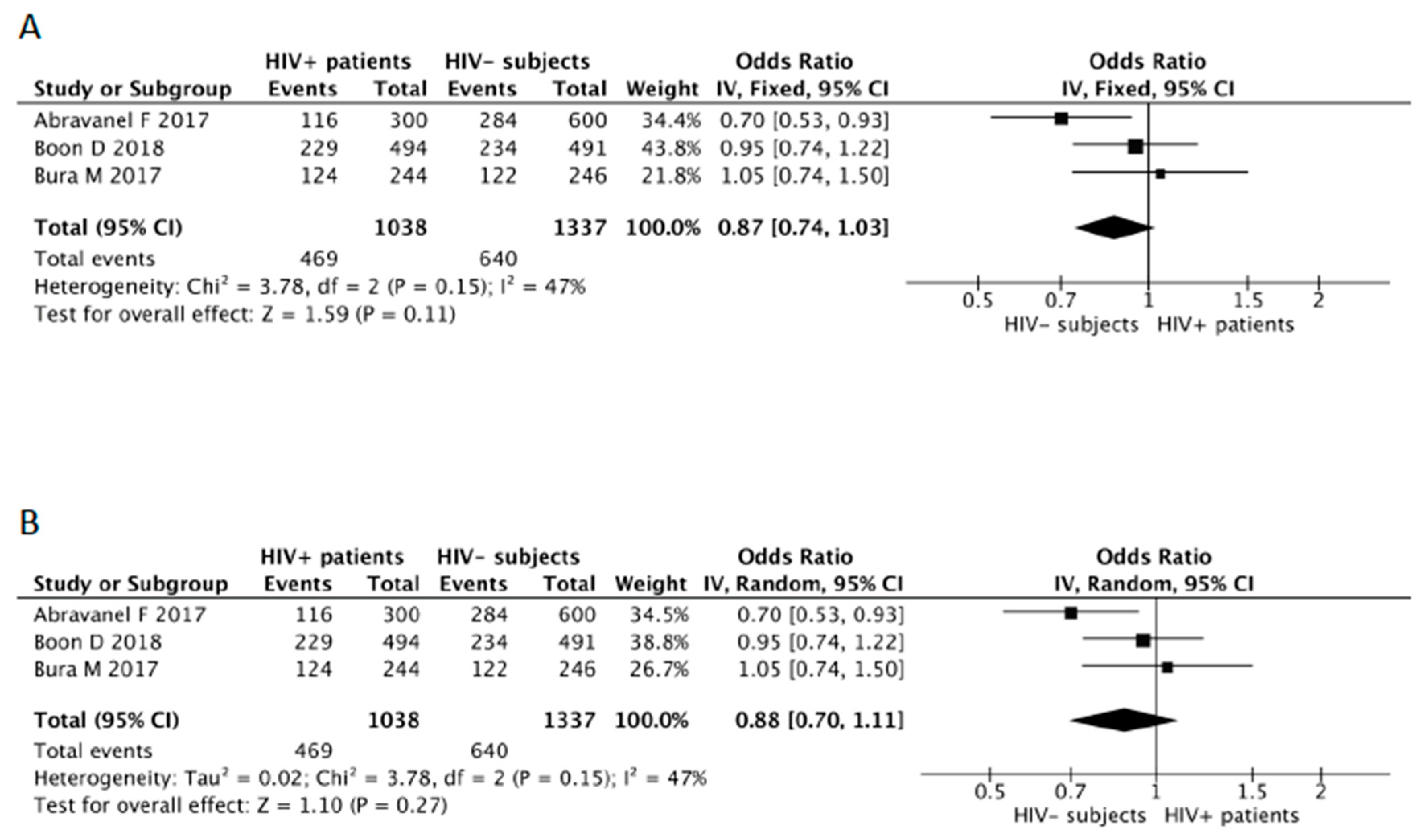
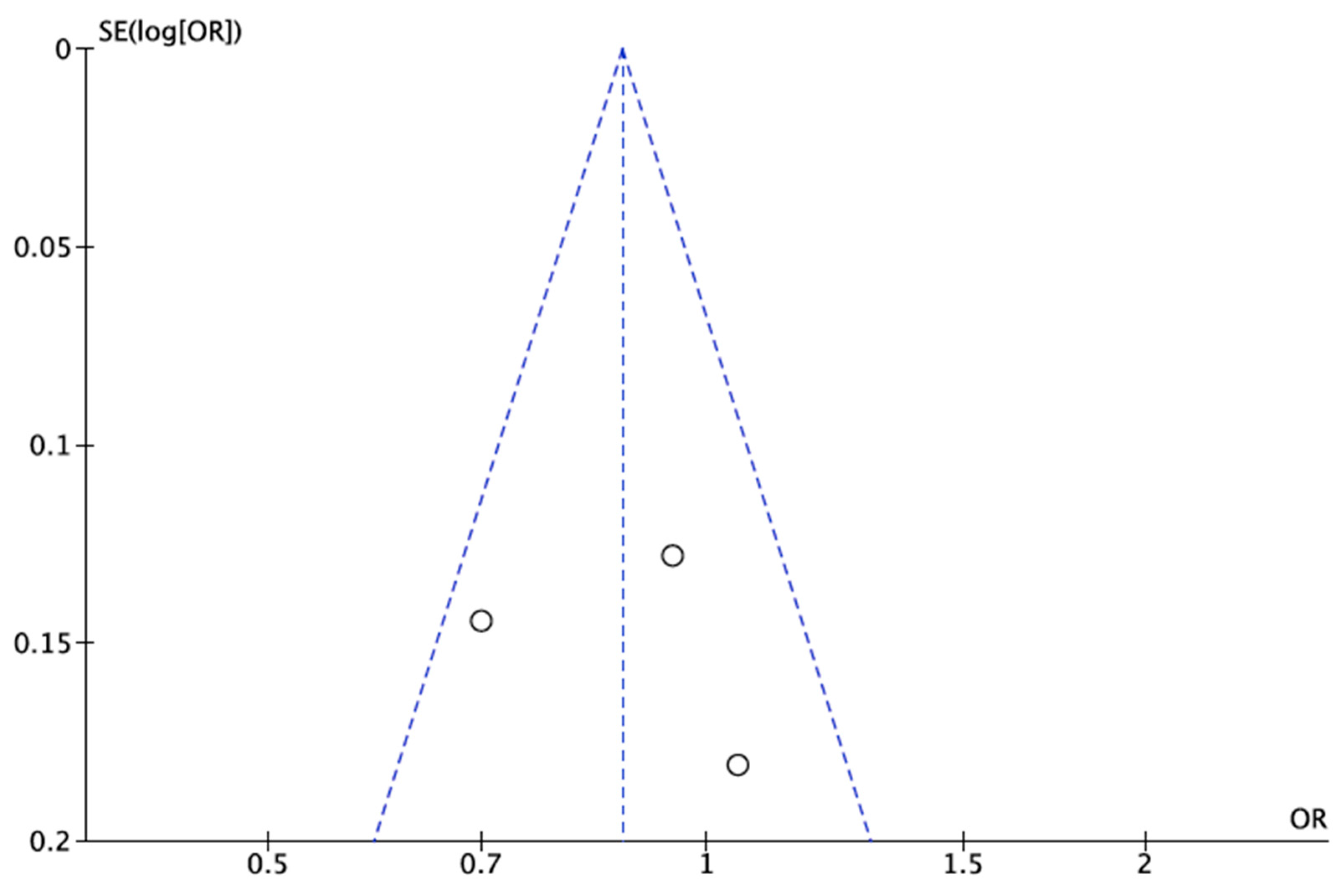
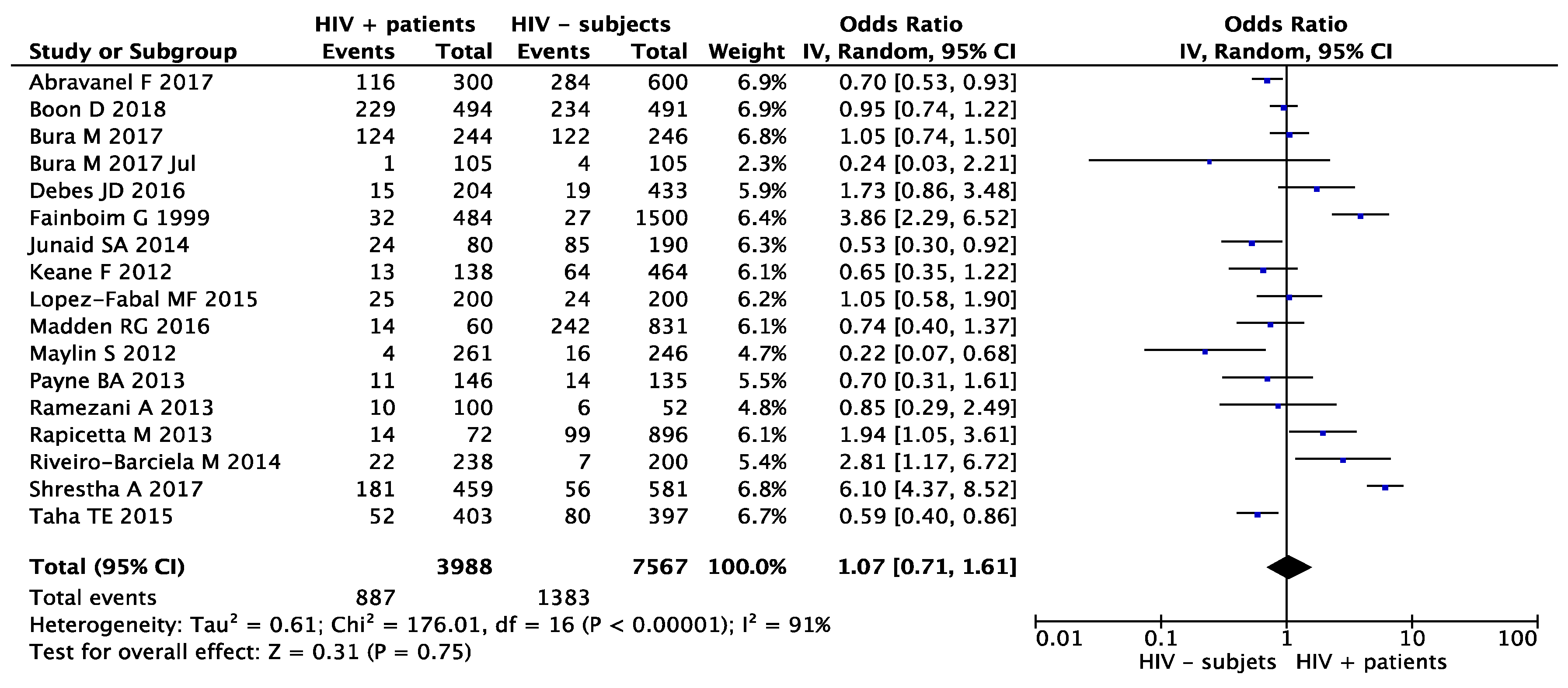
3.2. Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kamar, N.; Dalton, H.R.; Abravanel, F.; Izopet, J. Hepatitis E Virus Infection. Clin. Microbiol. Rev. 2014, 27, 116–138. [Google Scholar] [CrossRef] [PubMed]
- Forni, D.; Cagliani, R.; Clerici, M.; Sironi, M. Origin and dispersal of Hepatitis E virus. Emerg. Microbes Infect. 2018, 7, 11–13. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Teng, J.L.L.; Lau, S.K.P.; Sridhar, S.; Fu, H.; Gong, W.; Li, M.; Xu, Q.; He, Y.; Zhuang, H.; et al. Transmission of a Novel Genotype of Hepatitis E Virus from Bactrian Camels to Cynomolgus Macaques. J. Virol. 2019, 93. [Google Scholar] [CrossRef] [PubMed]
- Hoofnagle, J.H.; Nelson, K.E.; Purcell, R.H. Hepatitis E. N. Engl. J. Med. 2012, 367, 1237–1244. [Google Scholar]
- Krain, L.J.; Nelson, K.E.; Labrique, A.B. Host Inmune Status and Response to Hepatitis E Virus Infection. Clin. Microbiol. Rev. 2014, 27, 139–165. [Google Scholar] [CrossRef] [PubMed]
- Frias, M.; López-López, P.; Rivero, A.; Rivero-Juarez, A. Role of Hepatitis E Virus Infection in Acute-On-Chronic Liver Failure. BioMed Res. Int. 2018, 2018, 9098535. [Google Scholar] [CrossRef]
- Neukam, K.; Barreiro, P.; Macías, J.; Avellón, A.; Cifuentes, C.; Martín-Carbonero, L.; Echevarría, J.M.; Vargas, J.; Soriano, V.; Pineda, J.A. Chronic hepatitis E in HIV patients: Rapid progression to cirrhosis and response to oral ribavirin. Clin. Infect. Dis. 2013, 57, 465–468. [Google Scholar] [CrossRef]
- Shrestha, A.; Adhikari, A.; Bhattarai, M.; Rauniyar, R.; Debes, J.D.; Boonstra, A.; Lama, T.K.; Al Mahtab, M.; Butt, A.S.; Akbar, S.M.F.; et al. Prevalence and risk of hepatitis E virus infection in the HIV population of Nepal. Virol. J. 2017, 14, 228. [Google Scholar] [CrossRef]
- Riveiro-Barciela, M.; Buti, M.; Homs, M.; Campos-Varela, I.; Cantarell, C.; Crespo, M.; Castells, L.; Tabernero, D.; Quer, J.; Esteban, R.; et al. Cirrhosis, liver transplantation and HIV infection are risk factors associated with hepatitis E virus infection. PLoS ONE 2014, 9, e103028. [Google Scholar] [CrossRef]
- Rapicetta, M.; Monarca, R.; Kondili, L.A.; Chionne, P.; Madonna, E.; Madeddu, G.; Soddu, A.; Candido, A.; Carbonara, S.; Mura, M.S.; et al. Hepatitis E virus and hepatitis A virus exposure in an apparently healthy high-risk population in Italy. Infection 2013, 41, 69–76. [Google Scholar] [CrossRef]
- Fainboim, H.; González, J.; Fassio, E.; Martinez, A.; Otegui, L.; Eposto, M.; Cahn, P.; Marino, R.; Landeira, G.; Suaya, G.; et al. Prevalence of hepatitis viruses in an anti-human immunodeficiency virus-positive population from Argentina. A multicentre study. J. Viral Hepat. 1999, 6, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Madden, R.G.; Wallace, S.; Sonderup, M.; Korsman, S.; Chivese, T.; Gavine, B.; Edem, A.; Govender, R.; English, N.; Kaiyamo, C.; et al. Hepatitis E virus: Western Cape, South Africa. World J. Gastroenterol. 2016, 22, 9853–9859. [Google Scholar] [CrossRef] [PubMed]
- Taha, T.E.; Rusie, L.K.; Labrique, A.; Nyirenda, M.; Soko, D.; Kamanga, M.; Kumwenda, J.; Farazadegan, H.; Nelson, K.; Kumwenda, N. Seroprevalence for Hepatitis E and Other Viral Hepatitides among Diverse Populations, Malawi. Emerg. Infect. Dis. 2015, 21, 1174–1182. [Google Scholar] [CrossRef] [PubMed]
- Junaid, S.A.; Agina, S.E.; Abubakar, K.A. Epidemiology and associated risk factors of hepatitis e virus infection in plateau state, Nigeria. Virology 2014, 5, 15–26. [Google Scholar] [CrossRef]
- Payne, B.A.; Medhi, M.; Ijaz, S.; Valappil, M.; Savage, E.J.; Gill, O.N.; Tedder, R.; Schwab, U. Hepatitis E virus seroprevalence among men who have sex with men, United Kingdom. Emerg. Infect. Dis. 2013, 19, 333–335. [Google Scholar] [CrossRef]
- Keane, F.; Gompels, M.; Bendall, R.; Drayton, R.; Jennings, L.; Black, J.; Baragwanath, G.; Lin, N.; Henley, W.; Ngui, S.L.; et al. virus coinfection in patients with HIV infection. HIV Med. 2012, 13, 83–88. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P.; Ga, S.W.; Zello, G.A.; Petersen, J.; et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2013. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 November 2019).
- Abravanel, F.; Lhomme, S.; Fougère, M.; Saune, K.; Alvarez, M.; Péron, J.-M.; Delobel, P.; Izopet, J. HEV infection in French HIV-infected patients. J. Infect. 2017, 74, 310–313. [Google Scholar] [CrossRef]
- Boon, D.; Redd, A.D.; Laeyendecker, O.; Engle, R.E.; Nguyen, H.; Ocama, P.; Boaz, I.; Ndyanabo, A.; Kiggundu, V.; Reynolds, S.J.; et al. Hepatitis E Virus Seroprevalence and Correlates of Anti-HEV IgG Antibodies in the Rakai District, Uganda. J. Infect. Dis 2018, 217, 785–789. [Google Scholar] [CrossRef]
- Bura, M.; Lagiedo, M.; Michalak, M.; Sikora, J.; Mozer-Lisewska, I. Hepatitis E Virus IgG seroprevalence in HIV patients and blood donors, west-central Poland. Int. J. Infect. Dis. 2017, 61, 20–22. [Google Scholar] [CrossRef]
- Zeng, H.; Wang, L.; Liao, L.; Shao, Y.; Liu, P. Seroprevalence of hepatitis E virus in HIV-infected patients in China. AIDS 2017, 31, 2019–2021. [Google Scholar] [CrossRef] [PubMed]
- Pineda, J.A.; Cifuentes, C.; Parra, M.; Merchante, N.; Pérez-Navarro, E.; Rivero-Juárez, A.; Monje, P.; Rivero, A.; Macías, J.; Real, L.M. Incidence and natural history of hepatitis E virus coinfection among HIV-infected patients. AIDS 2014, 28, 1931–1937. [Google Scholar] [CrossRef] [PubMed]
- Christensen, P.B.; Engle, R.E.; Hjort, C.; Homburg, K.M.; Vach, W.; Georgsen, J.; Purcell, R.H. Time trend of the prevalence of hepatitis E antibodies among farmers and blood donors: A potential zoonosis in Denmark. Clin. Infect. Dis. 2018, 47, 1026–1031. [Google Scholar] [CrossRef]
- Rivero-Juarez, A.; Martinez-Dueñas, L.; Martínez-Peinado, A.; Camacho, A.; Cifuentes, C.; Gordon, A.; Frias, M.; Torre-Cisneros, J.; Pineda, J.A.; Rivero, A. High hepatitis E virus seroprevalence with absence of chronic infection in HIV-infected patients. J. Infect. 2015, 70, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Rivero-Juarez, A.; Cuenca-Lopez, F.; Martinez-Peinado, A.; Camacho, A.; Real, L.M.; Frías, M.; Gordon, A.; Cantisán, S.; Torre-Cisneros, J.; Pineda, J.A.; et al. Rural habitat as risk factor for hepatitis E virus seroconversion in HIV-infected patients: A prospective longitudinal study. Zoonoses Public Health 2017, 64, e60–e64. [Google Scholar] [CrossRef] [PubMed]
- Mansuy, J.M.; Gallian, P.; DiMeglio, C.; Sauné, K.; Arnaud, C.; Pelletier, B.; Morel, P.; Legrand, D.; Tiberghien, P.; Izopet, J. A nationwide survey of hepatitis E viral infection in French blood donors. Hepatology 2016, 63, 1145–1154. [Google Scholar] [CrossRef] [PubMed]
- Cleland, A.; Smith, L.; Crossan, C.; Blatchford, O.; Dalton, H.R.; Scobie, L.; Petrik, J. Hepatitis E virus in Scottish blood donors. Vox Sang. 2013, 105, 283–289. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Included Studies | NOS for Assessing the Quality of Studies* | Extracted Data | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Year | Place of Study | Tittle | Selection | Comparability | Exposure | Total Score | HIV-Positive Patients | HIV-Negative Subjects | OR (95% CI) | p Value | ||||
| Total Patients Included | HEV + Patients | % | Total Subjects Included | HEV + Patients | % | ||||||||||
| Abravanel et al. [19] | 2017 | France (Europe) | HEV infection in French HIV-infected patients | **** | ** | ** | 8 | 300 | 116 | 38.7 | 600 | 284 | 41.3 | 0.70 (0.53–0.93) | 0.0138 |
| Boon et al. [20] | 2018 | Uganda (Africa) | Hepatitis E Virus Seroprevalence and Correlates of Anti-HEV IgG Antibodies in the Rakai District, Uganda | **** | ** | ** | 8 | 494 | 229 | 46.4 | 491 | 234 | 47.7 | 0.95 (0.74–1.22) | 0.6824 |
| Bura et al. [21] | 2017 | Poland (Europe) | Hepatitis E virus IgG seroprevalence in HIV patients and blood donors, west-central Poland | **** | ** | ** | 8 | 244 | 124 | 50.8 | 246 | 122 | 49.6 | 1.05 (0.74–1.50) | 0.7861 |
| TOTAL | 1038 | 469 | 45.2 | 1337 | 640 | 47.9 | - | - | |||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopez-Lopez, P.; Frias, M.; Camacho, A.; Rivero, A.; Rivero-Juarez, A. Human Immunodeficiency Virus Infected Patients are Not at Higher Risk for Hepatitis E Virus Infection: A Systematic Review and Meta-Analysis. Microorganisms 2019, 7, 618. https://doi.org/10.3390/microorganisms7120618
Lopez-Lopez P, Frias M, Camacho A, Rivero A, Rivero-Juarez A. Human Immunodeficiency Virus Infected Patients are Not at Higher Risk for Hepatitis E Virus Infection: A Systematic Review and Meta-Analysis. Microorganisms. 2019; 7(12):618. https://doi.org/10.3390/microorganisms7120618
Chicago/Turabian StyleLopez-Lopez, Pedro, Mario Frias, Angela Camacho, Antonio Rivero, and Antonio Rivero-Juarez. 2019. "Human Immunodeficiency Virus Infected Patients are Not at Higher Risk for Hepatitis E Virus Infection: A Systematic Review and Meta-Analysis" Microorganisms 7, no. 12: 618. https://doi.org/10.3390/microorganisms7120618