Seroprevalence Study of Anti-HEV IgG among Different Adult Populations in Corsica, France, 2019

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
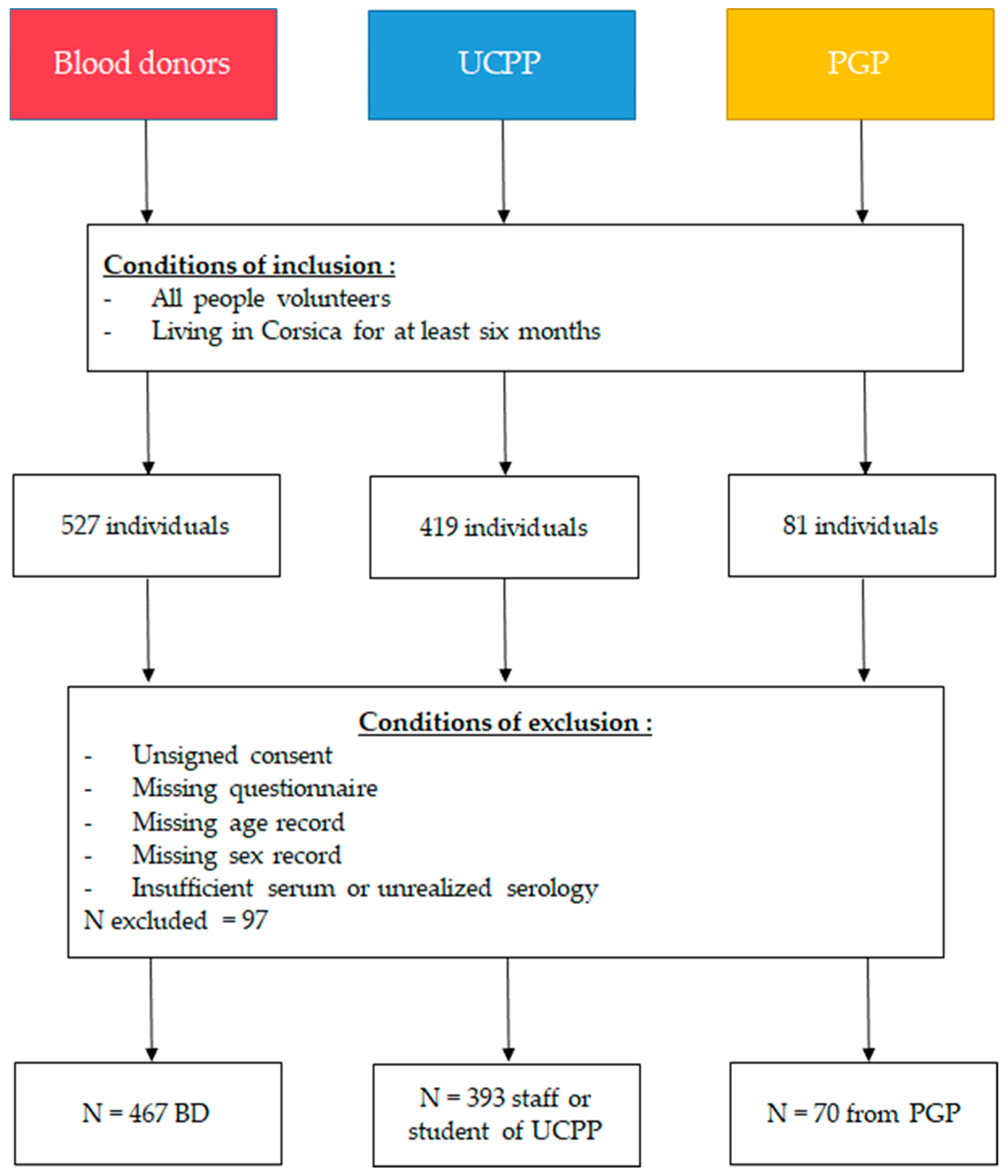
2.2. Study Populations
2.3. Questionnaire
2.4. Blood Samples and Laboratory Methods
2.4.1. Blood Samples
2.4.2. Anti-HEV IgG Detection
2.5. Statistical Analysis
2.5.1. Sample Size
2.5.2. Seroprevalence and Epidemiological Factors Analysis
3. Results
3.1. Anti-HEV IgG Seroprevalence
3.2. Risk Factors Associated with Anti-HEV IgG Seroprevalence
3.2.1. Univariate Analysis
3.2.2. Multivariate Analysis
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- -
- Age
- -
- Gender
- -
- Situation
- -
- Professional activity
- -
- Educational level
- -
- ZIP code
- -
- Type of residence
- -
- Water distribution
- -
- Sewage disposal
- -
- Contact with wastewater
- -
- Consumption water
- -
- Hunting
- -
- Breeding
- -
- Home at one kilometer of a farm or a breeding
- -
- Skinning or butchering activity
- -
- Contact with different animals
- -
- Eating habits and type of cooking
- -
- Clinical factors (presence of chronic diseases, transplantation, blood transfusion, immunosuppression, and a past HEV infection during the life of the individual) except for blood donors

{kind=link}
{kind=link}
| Blood Donors | Student and Personal of UCPP | Patient of General Practice | Overall | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | ||
| Gender | Men | 201 | 43.0 | 149 | 37.9 | 36 | 51.4 | 386 | 41.5 |
| Women | 266 | 57.0 | 244 | 62.1 | 34 | 48.6 | 544 | 58.5 | |
| Age groups | 18–27 | 126 | 27.0 | 242 | 61.6 | 6 | 8.6 | 374 | 40.2 |
| 28–37 | 101 | 21.6 | 67 | 17.0 | 5 | 7.1 | 173 | 18.6 | |
| 38–47 | 83 | 17.8 | 35 | 8.9 | 13 | 18.6 | 131 | 14.1 | |
| 48–57 | 84 | 18.0 | 34 | 8.7 | 19 | 27.1 | 137 | 14.7 | |
| 58–70 | 73 | 15.6 | 11 | 2.8 | 13 | 18.6 | 97 | 10.4 | |
| 70 | 4 | 1.0 | 14 | 20.0 | 18 | 1.9 | |||
| Graduate studies level | Pre bac | 87 | 18.6 | 30 | 7.6 | 42 | 60.0 | 159 | 17.1 |
| Bac | 145 | 31.0 | 180 | 45.8 | 8 | 11.4 | 333 | 35.8 | |
| Post bac | 232 | 49.7 | 179 | 45.5 | 20 | 28.6 | 431 | 46.3 | |
| Professional activity | No | 64 | 13.7 | 112 | 28.5 | 1 | 1.4 | 177 | 19.0 |
| Yes | 403 | 86.3 | 281 | 71.5 | 69 | 98.6 | 753 | 81.0 | |
| Kind of habitation | Apartment | 179 | 38.3 | 182 | 46.3 | 23 | 32.9 | 384 | 41.3 |
| Individual House | 284 | 60.8 | 204 | 51.9 | 47 | 67.1 | 535 | 57.5 | |
| Farm | 4 | 0.9 | 6 | 1.5 | 0 | 0.0 | 4 | 0.4 | |
| Hunters | No | 447 | 95.7 | 350 | 89.1 | 64 | 91.4 | 861 | 92.6 |
| Yes | 20 | 4.3 | 43 | 10.9 | 6 | 8.6 | 69 | 7.4 | |
| Breeders | No | 442 | 94.6 | 366 | 93.1 | 65 | 92.9 | 873 | 93.9 |
| Yes | 25 | 5.4 | 27 | 6.9 | 5 | 7.1 | 57 | 6.1 | |
| Skinning and butchering | No | 449 | 96.1 | 354 | 90.1 | 61 | 87.1 | 864 | 92.9 |
| Yes | 18 | 3.9 | 39 | 9.9 | 9 | 12.9 | 66 | 7.1 | |
| Contact with wastewater | No | 450 | 96.4 | 383 | 97.5 | 67 | 95.7 | 900 | 96.8 |
| Yes | 17 | 3.6 | 10 | 2.5 | 3 | 4.3 | 30 | 3.2 | |
| Housing water | Private | 22 | 4.7 | 19 | 4.1 | 2 | 0.4 | 43 | 9.2 |
| Collective | 429 | 91.9 | 360 | 91.6 | 69 | 98.6 | 858 | 92.3 | |
| Total | 467 | 50.2 | 393 | 42.3 | 70 | 7.5 | 930 | 100.0 | |
| Food Products | Cooking | OR [95% CI] | p-Value |
|---|---|---|---|
| Little wild game | Well-cooked | Reference | 0.45337 |
| Raw | INF | ||
| Rare/Medium | 0.85 [0.51;1.4] | ||
| Big wild game | Well-cooked | Reference | 0.23411 |
| Raw | INF | ||
| Rare/Medium | 0.75 [0.5;1.15] | ||
| Pork | Well-cooked | Reference | 0.2255 |
| Raw | 0.99 [0.4;2.49] | ||
| Rare/Medium | 0.69 [0.46;1.05] | ||
| Sausages and pâtés | Well-cooked | Reference | 0.81779 |
| Raw | 0.87 [0.53;1.45] | ||
| Rare/Medium | 0.9 [0.56;1.44] | ||
| Liver | Well-cooked | Reference | 0.18698 |
| Raw | INF | ||
| Rare/Medium | 0.71 [0.38;1.34] | ||
| Figatellu | Well-cooked | Reference | 0.86939 |
| Raw | 1.18 [0.62;2.32] | ||
| Rare/Medium | 1.05 [0.67;1.64] | ||
| Offal | Well-cooked | Reference | 0.17264 |
| Rare/Medium | 0.65 [0.35;1.21] | ||
| Beef | Well-cooked | Reference | 0.60331 |
| Raw | 1.29 [0.77;2.2] | ||
| Rare/Medium | 1.01 [0.75;1.36] | ||
| Poultry | Well-cooked | Reference | 0.51125 |
| Raw | INF | ||
| Rare/Medium | 0.97 [0.66;1.41] | ||
| Shellfish | Well-cooked | Reference | 0.40387 |
| Raw | 1.24 [0.86;1.8] | ||
| Rare/Medium | 1.3 [0.79;2.14] | ||
| Fish | Well-cooked | Reference | 0.7241 |
| Raw | 1.07 [0.73;1.58] | ||
| Rare/Medium | 1.16 [0.8;1.69] |
References
- Kamar, N.; Bendall, R.; Legrand-Abravanel, F.; Xia, N.S.; Ijaz, S.; Izopet, J.; Dalton, H.R. Hepatitis E. Lancet 2012, 379, 2477–2488. [Google Scholar] [CrossRef]
- Tam, A.W.; Smith, M.M.; Guerra, M.E.; Huang, C.C.; Bradley, D.W.; Fry, K.E.; Reyes, G.R. Hepatitis E virus (HEV): molecular cloning and sequencing of the full-length viral genome. Virology 1991, 185, 120–131. [Google Scholar] [CrossRef]
- International Committee on Taxonomy of viruses Hepeviridae. Available online: https://talk.ictvonline.org/ictv-reports/ictv_online_report/positive-sense-rna-viruses/w/hepeviridae (accessed on 11 March 2019).
- Doceul, V.; Bagdassarian, E.; Demange, A.; Pavio, N. Zoonotic hepatitis E virus: Classi fi cation, animal reservoirs and transmission routes. Viruses 2016, 8, 270. [Google Scholar] [CrossRef]
- Pavio, N.; Meng, X.J.; Renou, C. Zoonotic hepatitis E: animal reservoirs and emerging risks. Vet. Res. 2010, 41, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geng, Y.; Wang, Y. Epidemiology of hepatitis E. Adv. Exp. Med. Biol. 2016, 948, 39–59. [Google Scholar] [PubMed]
- Adlhoch, C.; Avellon, A.; Baylis, S.A.; Ciccaglione, A.R.; Couturier, E.; de Sousa, R.; Epstein, J.; Ethelberg, S.; Faber, M.; Feher, A.; et al. Hepatitis E virus: Assessment of the epidemiological situation in humans in Europe, 2014/15. J. Clin. Virol. 2016, 82, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Capai, L.; Falchi, A.; Charrel, R. Meta-analysis of human IgG anti-HEV seroprevalence in industrialized countries and a review of literature. Viruses 2019, 11, 84. [Google Scholar] [CrossRef]
- Mansuy, J.M.; Gallian, P.; Dimeglio, C.; Saune, K.; Arnaud, C.; Pelletier, B.; Morel, P.; Legrand, D.; Tiberghien, P.; Izopet, J. A nationwide survey of hepatitis E viral infection in French blood donors. Hepatology 2016, 63, 1145–1154. [Google Scholar] [CrossRef] [Green Version]
- Couturier, E.; Abravanel, F.; Figoni, J.; Van Cauteren, D.; Septfons, A.; Lhomme, S.; Durand, J.; Izopet, J.; De Valk, H. Hepatitis E surveillance in France 2002–2016. 2018, 28, 566–574. Bull. Epidémiol. Hebd. 2018, 28, 566–574. [Google Scholar]
- Pavio, N.; Laval, M.; Maestrini, O.; Casabianca, F.; Charrier, F.; Jori, F. Possible foodborne transmission of hepatitis E virus from domestic pigs and wild boars from corsica. Emerg. Infect Dis. 2016, 22, 2197–2199. [Google Scholar] [CrossRef]
- Renou, C.; Roque-Afonso, A.M.; Pavio, N. Foodborne transmission of hepatitis E virus from raw pork liver sausage, France. Emerg. Infect Dis. 2014, 20, 1945–1947. [Google Scholar] [CrossRef] [PubMed]
- Lapa, D.; Capobianchi, M.R.; Garbuglia, A.R. Epidemiology of hepatitis E virus in european countries. Int. J Mol Sci 2015, 16, 25711–25743. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, B.; Waddell, L.; Greig, J.; Young, I. Systematic review and meta-analysis of the seroprevalence of hepatitis E virus in the general population across non-endemic countries. PLoS ONE 2019, 14, e0216826. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Ge, S.X.; Huang, G.Y.; Li, S.W.; He, Z.Q.; Wang, Y.B.; Zheng, Y.J.; Gu, Y.; Ng, M.H.; Xia, N.S. Evaluation of antibody-based and nucleic acid-based assays for diagnosis of hepatitis E virus infection in a rhesus monkey model. J. Med. Virol. 2003, 71, 518–526. [Google Scholar] [CrossRef]
- Avellon, A.; Morago, L.; Garcia-Galera del Carmen, M.; Munoz, M.; Echevarria, J.M. Comparative sensitivity of commercial tests for hepatitis E genotype 3 virus antibody detection. J. Med. Virol. 2015, 87, 1934–1939. [Google Scholar] [CrossRef]
- Arya, R.; Antonisamy, B.; Kumar, S. Sample size estimation in prevalence studies. Indian J. Pediatr. 2012, 79, 1482–1488. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing, 2015. R Foundation for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 10 February 2015).
- Izopet, J.; Labrique, A.B.; Basnyat, B.; Dalton, H.R.; Kmush, B.; Heaney, C.D.; Nelson, K.E.; Ahmed, Z.B.; Zaman, K.; Mansuy, J.M.; et al. Hepatitis E virus seroprevalence in three hyperendemic areas: Nepal, Bangladesh and southwest France. J. Clin. Virol. 2015, 70, 39–42. [Google Scholar] [CrossRef]
- Mansuy, J.M.; Saune, K.; Rech, H.; Abravanel, F.; Mengelle, C.; L Homme, S.; Destruel, F.; Kamar, N.; Izopet, J. Seroprevalence in blood donors reveals widespread, multi-source exposure to hepatitis E virus, southern France, October 2011. Eurosurveillance 2015, 20, 27–34. [Google Scholar] [CrossRef]
- Christensen, P.B.; Engle, R.E.; Hjort, C.; Homburg, K.M.; Vach, W.; Georgsen, J.; Purcell, R.H. Time trend of the prevalence of hepatitis E antibodies among farmers and blood donors: a potential zoonosis in Denmark. Clin. Infect Dis. 2008, 47, 1026–1031. [Google Scholar] [CrossRef]
- Slot, E.; Hogema, B.M.; Riezebos-Brilman, A.; Kok, T.M.; Molier, M.; Zaaijer, H.L. Silent hepatitis E virus infection in Dutch blood donors, 2011 to 2012. Eurosurveillance 2013, 18. [Google Scholar] [CrossRef]
- Olsoy, I.B.; Henriksen, S.; Weissbach, F.H.; Larsen, M.; Borgen, K.; Abravanel, F.; Kamar, N.; Paulssen, E.J.; Hirsch, H.H.; Rinaldo, C.H. Seroprevalence of hepatitis E virus (HEV) in a general adult population in Northern Norway: the Tromso study. Med. Microbiol. Immunol. 2019. [Google Scholar]
- Zhou, Y. Immunobiology and host response to HEV. Adv. Exp. Med. Biol. 2016, 948, 113–141. [Google Scholar] [PubMed]
- Mansuy, J.M.; Bendall, R.; Legrand-Abravanel, F.; Saune, K.; Miedouge, M.; Ellis, V.; Rech, H.; Destruel, F.; Kamar, N.; Dalton, H.R.; et al. Hepatitis E virus antibodies in blood donors, France. Emerging Infect. Dis. 2011, 17, 2309–2312. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, T.; Lupulovic, D.; Jimenez de Oya, N.; Vojvodic, S.; Blazquez, A.B.; Escribano-Romero, E.; Martin-Acebes, M.A.; Potkonjak, A.; Milosevic, V.; Lazic, S.; et al. Prevalence of hepatitis E virus (HEV) antibodies in Serbian blood donors. J. Infect Dev. Ctries. 2014, 8, 1322–1327. [Google Scholar] [CrossRef]
- Pittaras, T.; Valsami, S.; Mavrouli, M.; Kapsimali, V.; Tsakris, A.; Politou, M. Seroprevalence of hepatitis E virus in blood donors in Greece. Vox sanguinis 2014, 106, 387. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL clinical practice guidelines on hepatitis E virus infection. J. Hepatol. 2018, 68, 1256–1271. [Google Scholar] [CrossRef]
- De Keukeleire, S.; Reynders, M. Hepatitis E: An underdiagnosed, emerging infection in nonendemic regions. J. Clin. Transl. Hepatol. 2015, 3, 288–291. [Google Scholar]
- Xin, S.; Xiao, L. Clinical manifestations of hepatitis E. Adv. Exp. Med. Biol. 2016, 948, 175–189. [Google Scholar]
- Teixeira, J.; Mesquita, J.R.; Pereira, S.S.; Oliveira, R.M.; Abreu-Silva, J.; Rodrigues, A.; Myrmel, M.; Stene-Johansen, K.; Overbo, J.; Goncalves, G.; et al. Prevalence of hepatitis E virus antibodies in workers occupationally exposed to swine in Portugal. Med. Microbiol. Immunol. 2017, 206, 77–81. [Google Scholar] [CrossRef]
- Jori, F.; Laval, M.; Maestrini, O.; Casabianca, F.; Charrier, F.; Pavio, N. Assessment of domestic pigs, wild boars and feral hybrid pigs as reservoirs of hepatitis E virus in Corsica, France. Viruses 2016, 8, 236. [Google Scholar] [CrossRef]
- Capai, L.F.C.; Maestrini, O.; Villechenaud, N.; Masse, S.; Bosseur, F.; De Lamballerie, X.; Charrel, R.; Falchi, A. Drastic decline of hepatitis E virus detection in domestic pigs after the age of 6 months, Corsica, France. Transbound. Emerg. Dis. 2019. [Google Scholar] [CrossRef] [PubMed]
- Schielke, A.; Ibrahim, V.; Czogiel, I.; Faber, M.; Schrader, C.; Dremsek, P.; Ulrich, R.G.; Johne, R. Hepatitis E virus antibody prevalence in hunters from a district in Central Germany, 2013: a cross-sectional study providing evidence for the benefit of protective gloves during disembowelling of wild boars. BMC Infect. Dis. 2015, 15, 440. [Google Scholar] [CrossRef] [PubMed]
- Berto, A.; Grierson, S.; Hakze-van der Honing, R.; Martelli, F.; Johne, R.; Reetz, J.; Ulrich, R.G.; Pavio, N.; Van der Poel, W.H.; Banks, M. Hepatitis E virus in pork liver sausage, France. Emerg. Infect. Dis. 2013, 19, 264–266. [Google Scholar] [CrossRef] [PubMed]
- Colson, P.; Borentain, P.; Queyriaux, B.; Kaba, M.; Moal, V.; Gallian, P.; Heyries, L.; Raoult, D.; Gerolami, R. Pig liver sausage as a source of hepatitis E virus transmission to humans. J. Infect. Dis. 2010, 202, 825–834. [Google Scholar] [CrossRef]
- Pavio, N.; Merbah, T.; Thebault, A. Frequent hepatitis E virus contamination in food containing raw pork liver, France. Emerg. Infect. Dis. 2014, 20, 1925–1927. [Google Scholar] [CrossRef]
- Mooij, S.H.; Hogema, B.M.; Tulen, A.D.; van Pelt, W.; Franz, E.; Zaaijer, H.L.; Molier, M.; Hofhuis, A. Risk factors for hepatitis E virus seropositivity in Dutch blood donors. BMC Infect. Dis. 2018, 18, 173. [Google Scholar] [CrossRef]
- Van Gageldonk-Lafeber, A.B.; van der Hoek, W.; Borlee, F.; Heederik, D.J.; Mooi, S.H.; Maassen, C.B.; Yzermans, C.J.; Rockx, B.; Smit, L.A.; Reimerink, J.H. Hepatitis E virus seroprevalence among the general population in a livestock-dense area in the Netherlands: a cross-sectional population-based serological survey. BMC Infect. Dis. 2017, 17, 21. [Google Scholar] [CrossRef]
- Barnaud, E.; Rogee, S.; Garry, P.; Rose, N.; Pavio, N. Thermal inactivation of infectious hepatitis E virus in experimentally contaminated food. Appl. Environ. Microbiol. 2012, 78, 5153–5159. [Google Scholar] [CrossRef]
- Emerson, S.U.; Arankalle, V.A.; Purcell, R.H. Thermal stability of hepatitis E virus. J. Infect. Dis. 2005, 192, 930–933. [Google Scholar] [CrossRef]
- Yugo, D.M.; Meng, X.J. Hepatitis E virus: foodborne, waterborne and zoonotic transmission. Int. J. Environ. Res. Public Health 2013, 10, 4507–4533. [Google Scholar] [CrossRef]
- Wichmann, O.; Schimanski, S.; Koch, J.; Kohler, M.; Rothe, C.; Plentz, A.; Jilg, W.; Stark, K. Phylogenetic and case-control study on hepatitis E virus infection in Germany. J. Infect Dis. 2008, 198, 1732–1741. [Google Scholar] [CrossRef] [PubMed]
- Bouwknegt, M.; Lodder-Verschoor, F.; van der Poel, W.H.; Rutjes, S.A.; de Roda Husman, A.M. Hepatitis E virus RNA in commercial porcine livers in The Netherlands. J. Food Prot. 2007, 70, 2889–2895. [Google Scholar] [CrossRef] [PubMed]
- Szabo, K.; Trojnar, E.; Anheyer-Behmenburg, H.; Binder, A.; Schotte, U.; Ellerbroek, L.; Klein, G.; Johne, R. Detection of hepatitis E virus RNA in raw sausages and liver sausages from retail in Germany using an optimized method. Int. J. Food Microbiol. 2015, 215, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Giannini, P.; Jermini, M.; Leggeri, L.; Nuesch-Inderbinen, M.; Stephan, R. Detection of hepatitis E virus RNA in raw cured sausages and raw cured sausages containing pig liver at retail stores in Switzerland. J. Food Prot. 2018, 81, 43–45. [Google Scholar] [CrossRef]
- Cossaboom, C.M.; Heffron, C.L.; Cao, D.; Yugo, D.M.; Houk-Miles, A.E.; Lindsay, D.S.; Zajac, A.M.; Bertke, A.S.; Elvinger, F.; Meng, X.J. Risk factors and sources of foodborne hepatitis E virus infection in the United States. J. Med. Virol. 2016, 88, 1641–1645. [Google Scholar] [CrossRef]
- Alfonsi, V.; Romano, L.; Ciccaglione, A.R.; La Rosa, G.; Bruni, R.; Zanetti, A.; Della Libera, S.; Iaconelli, M.; Bagnarelli, P.; Capobianchi, M.R.; et al. Hepatitis E in Italy: 5 years of national epidemiological, virological and environmental surveillance, 2012 to 2016. Euro. Surveill. 2018, 23. [Google Scholar] [CrossRef]
- Agence de l’eau Rhône Méditerranée Corse. RAPPORT d’activité 2017. Available online: https://www.eaurmc.fr/jcms/pro_73733/fr/rapport-d-activite-2017 (accessed on 31 December 2017).
- Iaconelli, M.; Purpari, G.; Della Libera, S.; Petricca, S.; Guercio, A.; Ciccaglione, A.R.; Bruni, R.; Taffon, S.; Equestre, M.; Fratini, M.; et al. Hepatitis A and E viruses in wastewaters, in river waters, and in bivalve molluscs in Italy. Food Environ. Virol. 2015, 7, 316–324. [Google Scholar] [CrossRef]
- Kokkinos, P.; Kozyra, I.; Lazic, S.; Soderberg, K.; Vasickova, P.; Bouwknegt, M.; Rutjes, S.; Willems, K.; Moloney, R.; de Roda Husman, A.M.; et al. Virological quality of irrigation water in leafy green vegetables and berry fruits production chains. Food Environ. Virol. 2017, 9, 72–78. [Google Scholar] [CrossRef]
- Maunula, L.; Kaupke, A.; Vasickova, P.; Soderberg, K.; Kozyra, I.; Lazic, S.; van der Poel, W.H.; Bouwknegt, M.; Rutjes, S.; Willems, K.A.; et al. Tracing enteric viruses in the European berry fruit supply chain. Int. J. Food Microbiol. 2013, 167, 177–185. [Google Scholar] [CrossRef]
- Brassard, J.; Gagne, M.J.; Genereux, M.; Cote, C. Detection of human food-borne and zoonotic viruses on irrigated, field-grown strawberries. Appl. Environ. Microbiol. 2012, 78, 3763–3766. [Google Scholar] [CrossRef]
- Kokkinos, P.; Kozyra, I.; Lazic, S.; Bouwknegt, M.; Rutjes, S.; Willems, K.; Moloney, R.; de Roda Husman, A.M.; Kaupke, A.; Legaki, E.; et al. Harmonised investigation of the occurrence of human enteric viruses in the leafy green vegetable supply chain in three European countries. Food Environ. Virol. 2012, 4, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Ceylan, A.; Ertem, M.; Ilcin, E.; Ozekinci, T. A special risk group for hepatitis E infection: Turkish agricultural workers who use untreated waste water for irrigation. Epidemiol. Infect. 2003, 131, 753–756. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, Z.; Crossan, C.; Craft, J.; Scobie, L. First report of the presence of hepatitis E virus in scottish-harvested shellfish purchased at retail level. Food Environ. Virol. 2018, 10, 217–221. [Google Scholar]
- Crossan, C.; Baker, P.J.; Craft, J.; Takeuchi, Y.; Dalton, H.R.; Scobie, L. Hepatitis E virus genotype 3 in shellfish, United Kingdom. Emerging Infect. Dis. 2012, 18, 2085–2087. [Google Scholar] [CrossRef] [PubMed]
- Li, T.C.; Miyamura, T.; Takeda, N. Detection of hepatitis E virus RNA from the bivalve Yamato-Shijimi (Corbicula japonica) in Japan. Am. J. Trop. Med. Hyg. 2007, 76, 170–172. [Google Scholar] [CrossRef] [PubMed]
- Rivadulla, E.; Varela, M.F.; Mesquita, J.R.; Nascimento, M.S.J.; Romalde, J.L. Detection of hepatitis E virus in shellfish harvesting areas from Galicia (Northwestern Spain). Viruses 2019, 11, 618. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, R.; Mesquita, J.R.; Pereira, S.; Abreu-Silva, J.; Teixeira, J.; Nascimento, M.S.J. Seroprevalence of hepatitis E virus antibodies in Portuguese children. Pediatr. Infect. Dis. J. 2017, 36, 623–626. [Google Scholar] [CrossRef]


| INF: Infinite | BD | UCPP | |||||||||
| NA: Missing Values | n | Anti-HEV IgG Positive | OR [95% CI] | p-Value | n | Anti-HEV IgG Positive | OR [95% CI] | p-Value | |||
| Parameters | Variables | n | % | n | % | ||||||
| Gender | Female | 266 | 128 | 48.1 | Reference | 0.00169 * | 244 | 107 | 43.9 | Reference | 0.05807 |
| Male | 201 | 126 | 62.7 | 1.81 [1.25–2.64] | 149 | 80 | 53.7 | 1.48 [0.99–2.24] | |||
| Age groups | 18–27 | 126 | 55 | 43.7 | Reference | 0.00633 * | 242 | 102 | 42.1 | Reference | 0.07139 |
| 28–37 | 101 | 58 | 57.4 | 1.74 [1.03–2.97] | 67 | 35 | 52.2 | 1.5 [0.87–2.59] | |||
| 38–47 | 83 | 40 | 48.2 | 1.2 [0.69–2.1] | 35 | 21 | 60.0 | 2.06 [1.01–4.32] | |||
| 48–57 | 84 | 52 | 61.9 | 2.1 [1.2–3.71] | 34 | 18 | 52.9 | 1.54 [0.75–3.2] | |||
| 58–70 | 73 | 49 | 67.1 | 2.64 [1.46–4.87] | 11 | 8 | 72.7 | 3.66 [1.03–17.02] | |||
| 70 | NA | 4 | 3 | 75.0 | 4.12 [0.52–83.9] | ||||||
| Hunting | No | 447 | 240 | 53.7 | 2.01 [0.79–5.77] | 0.14486 | 350 | 159 | 45.4 | 2.24 [1.17–4.45] | 0.01428 * |
| Yes | 20 | 14 | 70.0 | 43 | 28 | 65.1 | |||||
| Breeding | No | 442 | 235 | 53.2 | 2.79 [1.15–7.78] | 0.02165 * | 366 | 173 | 47.3 | 1.2 [0.55–2.66] | 0.64555 |
| Yes | 25 | 19 | 76.0 | 27 | 14 | 51.9 | |||||
| Skinning and butchering | No | 449 | 240 | 53.5 | 3.05 [1.07–10.88] | 0.03549 * | 354 | 160 | 45.2 | 2.73 [1.37–5.75] | 0.00403 * |
| Yes | 18 | 14 | 77.8 | 39 | 27 | 69.2 | |||||
| Contact with wastewater | No | 450 | 243 | 54.0 | 1.56 [0.58–4.6] | 0.37978 | 383 | 181 | 47.3 | 1.67 [0.47–6.64] | 0.42524 |
| Yes | 17 | 11 | 64.7 | 10 | 6 | 60.0 | |||||
| Tap water | No | 41 | 23 | 56.1 | 0.92 [0.47–1.74] | 0.78775 | 25 | 11 | 44.0 | 1.16 [0.52–2.69] | 0.71415 |
| Yes | 410 | 221 | 53.9 | 360 | 172 | 47.8 | |||||
| Bottled water | No | 15 | 10 | 66.7 | 0.57 [0.17–1.63] | 0.29725 | 10 | 5 | 50.0 | 0.88 [0.24–3.19] | 0.835 |
| Yes | 440 | 234 | 53.2 | 375 | 175 | 46.7 | |||||
| Water fountains in the villages | No | 213 | 102 | 47.9 | 1.58 [1.08–2.33] | 0.01895 * | 168 | 69 | 41.1 | 1.51 [1–2.29] | 0.05103 |
| Yes | 211 | 125 | 59.2 | 199 | 102 | 51.3 | |||||
| Mountain spring waters | No | 207 | 96 | 46.4 | 1.76 [1.2–2.6] | 0.00401 * | 182 | 86 | 47.3 | 0.96 [0.64–1.45] | 0.83939 |
| Yes | 212 | 128 | 60.4 | 184 | 85 | 46.2 | |||||
| Little wild game | No | 295 | 150 | 50.8 | 1.45 [0.97–2.18] | 0.06953 | 227 | 100 | 44.1 | 1.34 [0.89–2.02] | 0.16436 |
| Yes | 145 | 87 | 60.0 | 154 | 79 | 51.3 | |||||
| Big wild game | No | 175 | 79 | 45.1 | 1.8 [1.23–2.65] | 0.00264 * | 123 | 45 | 36.6 | 1.84 [1.19–2.88] | 0.00591 * |
| Yes | 268 | 160 | 59.7 | 260 | 134 | 51.5 | |||||
| Pork | No | 30 | 9 | 30.0 | 2.95 [1.36–6.92] | 0.00579 * | 26 | 6 | 23.1 | 3.26 [1.35–9.09] | 0.0075 * |
| Yes | 421 | 235 | 55.8 | 356 | 176 | 49.4 | |||||
| Sausages and pâtés | No | 52 | 18 | 34.6 | 2.47 [1.37–4.62] | 0.00263 * | 26 | 7 | 26.9 | 2.6 [1.11–6.78] | 0.027 * |
| Yes | 388 | 220 | 56.7 | 358 | 175 | 48.9 | |||||
| Liver | No | 301 | 147 | 48.8 | 1.82 [1.2–2.77] | 0.00463 * | 255 | 110 | 43.1 | 1.56 [1.01–2.42] | 0.04589 * |
| Yes | 134 | 85 | 63.4 | 120 | 65 | 54.2 | |||||
| Figatellu | No | 69 | 18 | 26.1 | 4.14 [2.37–7.53] | 2.46 × 10−8 * | 65 | 18 | 27.7 | 2.71 [1.53–4.98] | 0.00049 * |
| Yes | 374 | 222 | 59.4 | 322 | 164 | 50.9 | |||||
| Fittonu | No | 218 | 94 | 43.1 | 2.6 [1.76–3.86] | 1.82 × 10−6 * | 175 | 64 | 36.6 | 2.24 [1.47–3.42] | 0.00015 * |
| Yes | 211 | 140 | 66.4 | 190 | 107 | 56.3 | |||||
| Offal | No | 281 | 136 | 48.4 | 1.86 [1.25–2.78] | 0.00213 * | 247 | 103 | 41.7 | 1.78 [1.15–2.76] | 0.009 * |
| Yes | 159 | 101 | 63.5 | 125 | 70 | 56.0 | |||||
| Beef | No | 16 | 8 | 50.0 | 1.18 [0.43–3.27] | 0.74187 | 15 | 9 | 60.0 | 0.58 [0.19–1.64] | 0.3031 |
| Yes | 430 | 233 | 54.2 | 368 | 171 | 46.5 | |||||
| Poultry | No | 16 | 8 | 50.0 | 1.18 [0.43–3.28] | 0.73897 | 19 | 9 | 47.4 | 0.99 [0.39–2.56] | 0.99112 |
| Yes | 437 | 237 | 54.2 | 362 | 171 | 47.2 | |||||
| Shellfish | No | 76 | 38 | 50.0 | 1.2 [0.73–1.97] | 0.47138 | 71 | 24 | 33.8 | 1.98 [1.17–3.45] | 0.01107 * |
| Yes | 376 | 205 | 54.5 | 314 | 158 | 50.3 | |||||
| Fish | No | 22 | 10 | 45.5 | 1 [0.41–2.36] | 0.99845 | 31 | 10 | 32.3 | 1.98 [0.93–4.51] | 0.07726 |
| Yes | 431 | 235 | 54.5 | 352 | 171 | 48.6 | |||||
| Organic fruits and vegetables | No | 62 | 27 | 43.5 | 1.64 [0.96–2.84] | 0.07122 | 30 | 12 | 40.0 | 1.4 [0.66–3.07] | 0.38191 |
| Yes | 383 | 214 | 55.9 | 348 | 168 | 48.3 | |||||
| Wild berries | No | 234 | 115 | 49.1 | 1.57 [1.07–2.31] | 0.02001 * | 194 | 84 | 43.3 | 1.32 [0.88–1.99] | 0.17687 |
| Yes | 199 | 120 | 60.3 | 179 | 90 | 50.3 | |||||
| Total | 467 | 254 | 54.4 | 393 | 187 | 47.6 | |||||
| PGP | Overall | ||||||||||
| n | Anti-HEV IgG Positive | OR [95% CI] | p-Value | n | Anti-HEV IgG Positive | OR [95% CI] | p-Value | ||||
| Parameters | Variables | n | % | n | % | ||||||
| Gender | Female | 34 | 20 | 58.8 | Reference | 0.35362 | 544 | 255 | 46.9 | Reference | 0.00009 * |
| Male | 36 | 25 | 69.4 | 1.59 [0.6–4.33] | 386 | 231 | 59.8 | 1.69 [1.3–2.2] | |||
| Age groups | 18-27 | 6 | 3 | 50.0 | Reference | 0.40753 | 374 | 160 | 42.8 | Reference | 0.00001 * |
| 28-37 | 5 | 3 | 60.0 | 1.5 [0.13–19.11] | 173 | 96 | 55.5 | 1.67 [1.16–2.4] | |||
| 38-47 | 13 | 10 | 76.9 | 3.33 [0.43–29.22] | 131 | 71 | 54.2 | 1.58 [1.06–2.37] | |||
| 48-57 | 19 | 9 | 47.4 | 0.9 [0.13–5.99] | 137 | 79 | 57.7 | 1.82 [1.23–2.71] | |||
| 58-70 | 13 | 10 | 76.9 | 3.33 [0.43–29.22] | 97 | 67 | 69.1 | 2.99 [1.87–4.87] | |||
| 70 | 14 | 10 | 71.4 | 2.5 [0.34–19.67] | 18 | 13 | 72.2 | 3.48 [1.28–11.02] | |||
| Hunting | No | 64 | 39 | 60.9 | INF | 0.01785 * | 861 | 438 | 50.9 | 2.21 [1.32–3.82] | 0.0024 * |
| Yes | 6 | 6 | 100.0 | 69 | 48 | 69.6 | |||||
| Breeding | No | 65 | 41 | 63.1 | 2.34 [0.32–47.23] | 0.42697 | 873 | 449 | 51.4 | 1.75 [1.01–3.11] | 0.04641 * |
| Yes | 5 | 4 | 80.0 | 57 | 37 | 64.9 | |||||
| Skinning and butchering | No | 61 | 36 | 59.0 | INF | 0.00322 * | 864 | 436 | 50.5 | 3.07 [1.76–5.64] | 0.00005 * |
| Yes | 9 | 9 | 100.0 | 66 | 50 | 75.8 | |||||
| Contact with wastewater | No | 67 | 42 | 62.7 | INF | 0.09878 | 900 | 466 | 51.8 | 1.86 [0.88–4.19] | 0.1043 |
| Yes | 3 | 3 | 100.0 | 30 | 20 | 66.7 | |||||
| Tap water | No | 15 | 6 | 40.0 | 3.66 [1.14–12.58] | 0.02965 * | 81 | 40 | 49.4 | 1.13 [0.71–1.78] | 0.60849 |
| Yes | 55 | 39 | 70.9 | 825 | 432 | 52.4 | |||||
| Bottled water | No | 2 | 2 | 100.0 | INF | 0.17973 | 27 | 17 | 63.0 | 0.62 [0.27–1.34] | 0.22479 |
| Yes | 68 | 43 | 63.2 | 883 | 452 | 51.2 | |||||
| Water fountains in the villages | No | 35 | 21 | 60.0 | 1.39 [0.52–3.8] | 0.50842 | 416 | 192 | 46.2 | 1.5 [1.15–1.97] | 0.00289 * |
| Yes | 34 | 23 | 67.6 | 444 | 250 | 56.3 | |||||
| Mountain spring waters | No | 42 | 23 | 54.8 | 2.89 [1.01–9.21] | 0.04808 * | 431 | 205 | 47.6 | 1.36 [1.04–1.79] | 0.02331 * |
| Yes | 27 | 21 | 77.8 | 423 | 234 | 55.3 | |||||
| Little wild game | No | 46 | 27 | 58.7 | 1.99 [0.69–6.38] | 0.20866 | 568 | 277 | 48.8 | 1.38 [1.05–1.82] | 0.02055 * |
| Yes | 23 | 17 | 73.9 | 322 | 183 | 56.8 | |||||
| Big wild game | No | 22 | 10 | 45.5 | 3.14 [1.1–9.25] | 0.03188 | 320 | 134 | 41.9 | 1.84 [1.4–2.43] | 0.00001 * |
| Yes | 47 | 34 | 72.3 | 575 | 328 | 57.0 | |||||
| Pork | No | 1 | 0 | 0.0 | INF | 0.14871 | 57 | 15 | 26.3 | 3.27 [1.83–6.18] | 0.00004 * |
| Yes | 69 | 45 | 65.2 | 846 | 456 | 53.9 | |||||
| Sausages and pâtés | No | 5 | 2 | 40.0 | 2.93 [0.45–23.52] | 0.25158 | 83 | 27 | 32.5 | 2.44 [1.52–3.99] | 0.00017 * |
| Yes | 65 | 43 | 66.2 | 811 | 438 | 54.0 | |||||
| Liver | No | 48 | 28 | 58.3 | 2.29 [0.75–7.92] | 0.1474 | 604 | 285 | 47.2 | 1.7 [1.28–2.28] | 0.00028 * |
| Yes | 21 | 16 | 76.2 | 275 | 166 | 60.4 | |||||
| Figatellu | No | 6 | 2 | 33.3 | 4.1 [0.74–31.28] | 0.1066 | 140 | 38 | 27.1 | 3.48 [2.35–5.24] | 1.88 × 10−10 |
| Yes | 64 | 43 | 67.2 | 760 | 429 | 56.4 | |||||
| Fittonu | No | 35 | 17 | 48.6 | 4.08 [1.46–12.47] | 0.00694 * | 428 | 175 | 40.9 | 2.46 [1.87–3.24] | 8.41 × 10−11 |
| Yes | 34 | 27 | 79.4 | 435 | 274 | 63.0 | |||||
| Offal | No | 39 | 26 | 66.7 | 0.75 [0.28–2.02] | 0.56837 | 567 | 265 | 46.7 | 1.72 [1.3–2.28] | 0.00012 * |
| Yes | 30 | 18 | 60.0 | 314 | 189 | 60.2 | |||||
| Beef | No | 5 | 1 | 20.0 | 8.38 [1.15–169.46] | 0.0349 * | 36 | 18 | 50.0 | 1.08 [0.55–2.11] | 0.82208 |
| Yes | 65 | 44 | 67.7 | 863 | 448 | 51.9 | |||||
| Poultry | No | 2 | 1 | 50.0 | 1.83 [0.07–47.76] | 0.67522 | 37 | 18 | 48.6 | 1.15 [0.59–2.24] | 0.67789 |
| Yes | 68 | 44 | 64.7 | 867 | 452 | 52.1 | |||||
| Shellfish | No | 15 | 7 | 46.7 | 2.49 [0.77–8.21] | 0.12501 | 162 | 69 | 42.6 | 1.57 [1.11–2.21] | 0.00988 * |
| Yes | 54 | 37 | 68.5 | 744 | 400 | 53.8 | |||||
| Fish | No | 3 | 1 | 33.3 | 3.83 [0.35–84.93] | 0.26558 | 56 | 21 | 37.5 | 1.61 [0.94–2.83] | 0.08474 |
| Yes | 67 | 44 | 65.7 | 850 | 450 | 52.9 | |||||
| Organic fruits and vegetables or personal vegetable garden | No | 11 | 8 | 72.7 | 0.61 [0.12–2.38] | 0.49248 | 103 | 47 | 45.6 | 1.34 [0.89–2.03] | 0.1605 |
| Yes | 58 | 36 | 62.1 | 789 | 418 | 53.0 | |||||
| Wild berries | No | 37 | 19 | 51.4 | 3.38 [1.21–10.26] | 0.01937 * | 465 | 218 | 46.9 | 1.52 [1.17–1.99] | 0.00203 * |
| Yes | 32 | 25 | 78.1 | 410 | 235 | 57.3 | |||||
| Total | 70 | 45 | 64.3 | 930 | 486 | 52.3 | |||||
| BD | UCPP | PGP | Overall Glm | Overall Lmer Fixed Subpopulations | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Parameters | Variables | aOR [95% CI] | p-Value | aOR [95% CI] | p-Value | aOR [95% CI] | p-Value | aOR [95% CI] | p-Value | aOR [95% CI] | p-Value |
| Gender | Male | 1.58 [1.05–2.39] | 0.02973 | NS | NS | NS | NS | ||||
| Figatellu | 2.82 [1.54–5.34] | 0.00065 | 2.22 [1.45–3.45] | 0.00023 | 1.77 [1.04–3.01] | 0.035 | |||||
| Fittonu | 1.97 [1.29–3.03] | 0.00183 | 2.14 [1.4–3.28] | 0.00039 | 4.35 [1.48–13.92] | 0.00696 | 1.95 [1.45–2.64] | 0.00001 | 1.95 [1.38–2.74] | 0.00013 | |
| Skinning and butchering | 3.52 [1.09–15.83] | 0.03451 | 2.43 [1.16–5.38] | 0.01764 | 7.88 e6 [0–INF] | 0.00294 | 2.76 [1.51–5.37] | 0.00077 | 3.45 [1.37–8.71] | 0.0087 | |
| Age groups | 18–27 | NS | NS | NS | Reference | 0.00272 | NS | ||||
| 28–37 | 1.61 [1.09–2.38] | ||||||||||
| 38–47 | 1.52 [0.98–2.37] | ||||||||||
| 48–57 | 1.54 [1–2.38] | ||||||||||
| 58–70 | 2.44 [1.45–4.19] | ||||||||||
| 70 | 3.46 [1.17–12.65] | ||||||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capai, L.; Masse, S.; Gallian, P.; Souty, C.; Isnard, C.; Blanchon, T.; Peres, B.; de Lamballerie, X.; Charrel, R.; Falchi, A. Seroprevalence Study of Anti-HEV IgG among Different Adult Populations in Corsica, France, 2019. Microorganisms 2019, 7, 460. https://doi.org/10.3390/microorganisms7100460
Capai L, Masse S, Gallian P, Souty C, Isnard C, Blanchon T, Peres B, de Lamballerie X, Charrel R, Falchi A. Seroprevalence Study of Anti-HEV IgG among Different Adult Populations in Corsica, France, 2019. Microorganisms. 2019; 7(10):460. https://doi.org/10.3390/microorganisms7100460
Chicago/Turabian StyleCapai, Lisandru, Shirley Masse, Pierre Gallian, Cécile Souty, Christine Isnard, Thierry Blanchon, Brigitte Peres, Xavier de Lamballerie, Rémi Charrel, and Alessandra Falchi. 2019. "Seroprevalence Study of Anti-HEV IgG among Different Adult Populations in Corsica, France, 2019" Microorganisms 7, no. 10: 460. https://doi.org/10.3390/microorganisms7100460