Efficacy Evaluation of an Intradermally Delivered Enterotoxigenic Escherichia coli CF Antigen I Fimbrial Tip Adhesin Vaccine Coadministered with Heat-Labile Enterotoxin with LT(R192G) against Experimental Challenge with Enterotoxigenic E. coli H10407 in Healthy Adult Volunteers

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Clinical Trial Design
2.2. Study Population and Enrollment Criteria
2.3. Immunization Procedures
2.4. Manufacture and Analysis of cGMP dscCfaE and LTR192G Vaccine Components
2.5. Bacterial Challenge Strain Preparation
2.6. Challenge Procedures
2.7. Antigen-Specific ELISA
2.8. Antibody in Lymphocyte Supernatant (ALS)
2.9. Primary (and Secondary) Study Endpoints and Definitions
2.10. Outcome Adjudication
3. Data Analysis and Statistical Considerations
4. Results
4.1. Subjects
4.2. Vaccine Safety
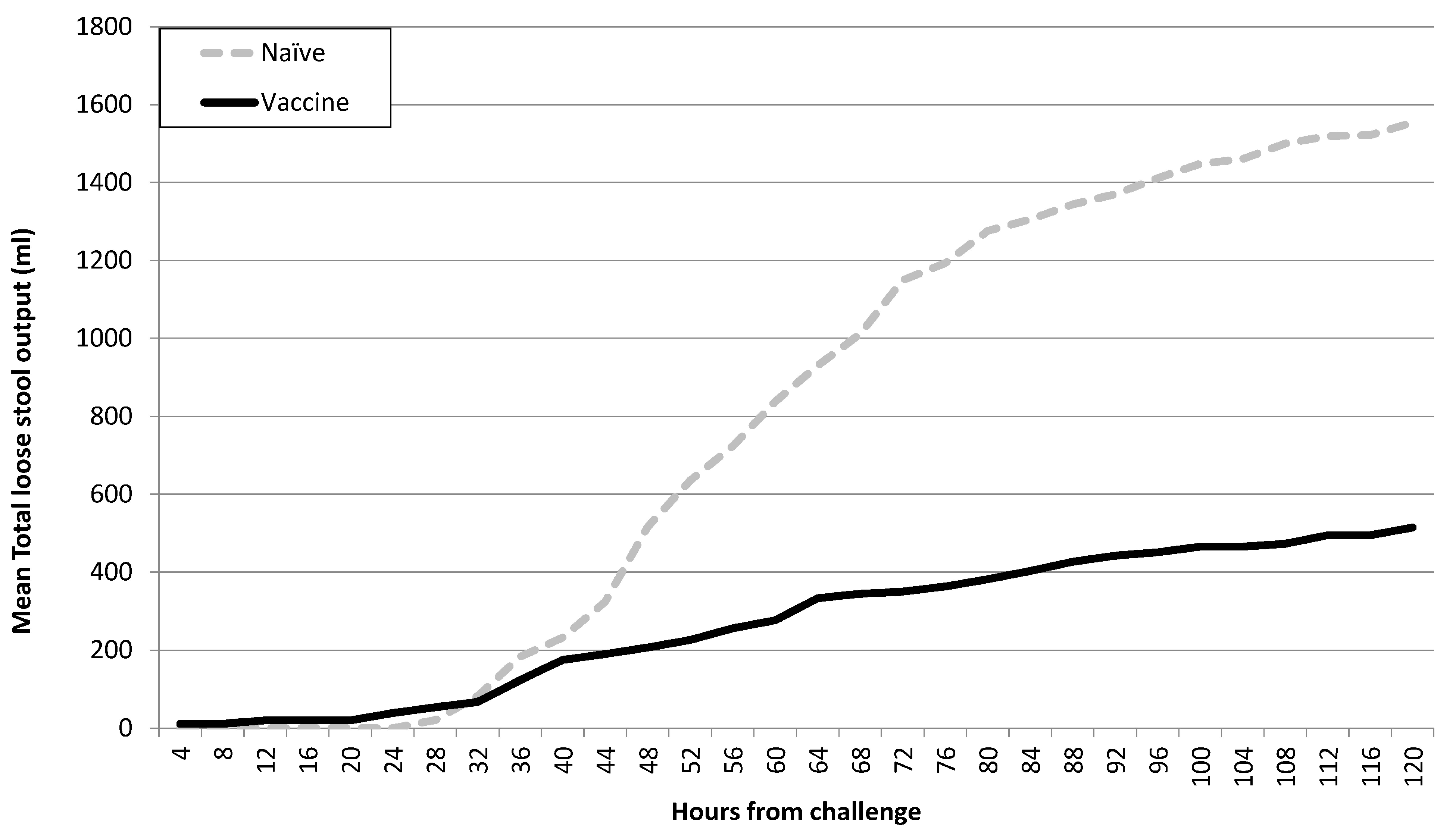
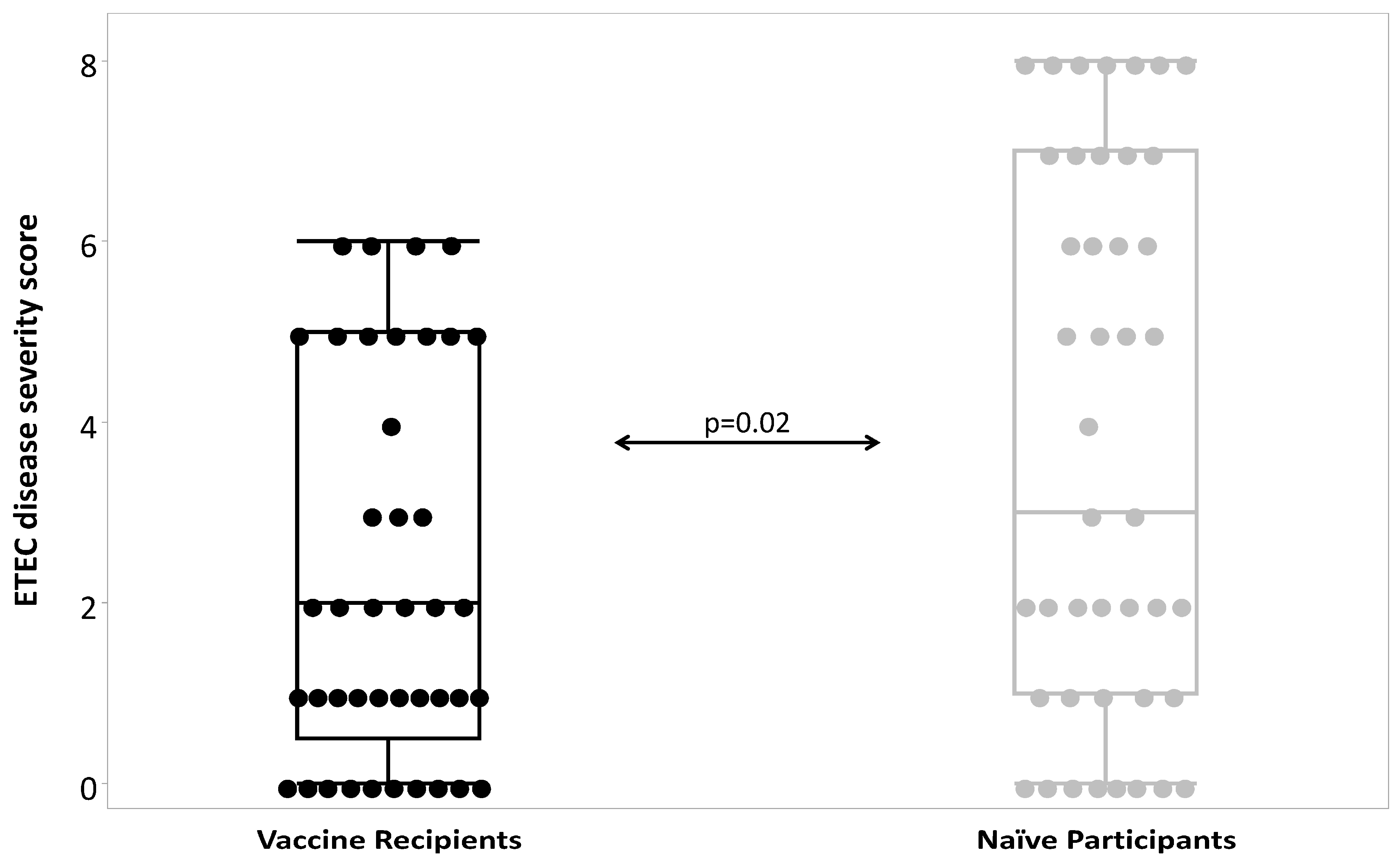
4.3. Vaccine Efficacy
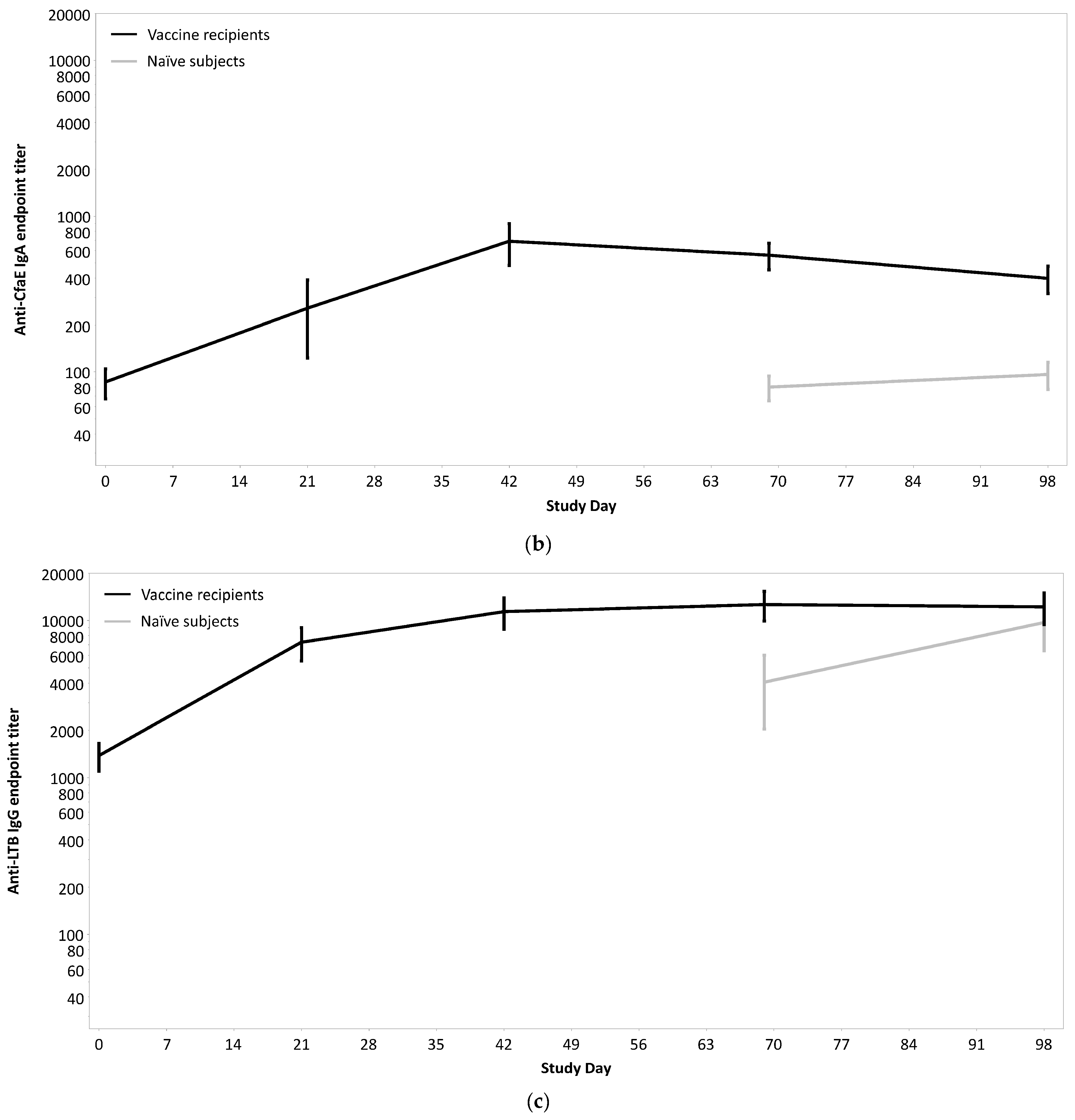
4.4. Immune Responses
5. Discussion
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
Human Volunteers Protection
Copyright Statement
References
- Croxen, M.A.; Law, R.J.; Scholz, R.; Keeney, K.M.; Wlodarska, M.; Finlay, B.B. Recent Advances in Understanding Enteric Pathogenic Escherichia coli. Clin. Microbiol. Rev. 2013, 26, 822–980. [Google Scholar] [CrossRef] [PubMed]
- Nataro, J.P.; Guerrant, R.L. Chronic consequences on human health induced by microbial pathogens: Growth faltering among children in developing countries. Vaccine 2017, 35, 6807–6812. [Google Scholar] [CrossRef] [PubMed]
- Okhuysen, P.C.; Jiang, Z.D.; Carlin, L.; Forbes, C.; DuPont, H.L. Post-diarrhea chronic intestinal symptoms and irritable bowel syndrome in North American travelers to Mexico. Am. J. Gastroenterol. 2004, 99, 1774–1778. [Google Scholar] [CrossRef] [PubMed]
- Porter, C.K.; Kowalcyk, B.; Riddle, M.S. Chronic Health Consequences of Acute Enteric Infections in the Developed World. Am. J. Gastroenterol. Supp. 2016, 3, 12–23. [Google Scholar] [CrossRef]
- Porter, C.K.; Thura, N.; Riddle, M.S. Quantifying the Incidence and Burden of Postinfectious Enteric Sequelae. Mil. Med. 2013, 178, 452–469. [Google Scholar] [CrossRef]
- Hasso-Agopsowicz, M.; Lopman, B.A.; Lanata, C.F.; Rogawski McQuade, E.T.; Kang, G.; Prudden, H.J.; Khalil, I.; Platts-Mills, J.A.; Kotloff, K.; Jit, M.; et al. World Health Organization Expert Working Group: Recommendations for assessing morbidity associated with enteric pathogens. Vaccine 2021, 39, 7521–7525. [Google Scholar] [CrossRef]
- Wellcome Trust. Vaccines to Tackle Drug Resistant Infections. In An Evaluation of R & D Opportunities; Wellcome Trust: London, UK, 2018; pp. 1–175. Available online: https://vaccinesforamr.org/wp-content/uploads/2018/09/Vaccines_for_AMR.pdf (accessed on 12 January 2024).
- Khalil, I.; Walker, R.; Porter, C.K.; Muhib, F.; Chilengi, R.; Cravioto, A.; Guerrant, R.; Svennerholm, A.M.; Qadri, F.; Baqar, S.; et al. Enterotoxigenic Escherichia coli (ETEC) vaccines: Priority activities to enable product development, licensure, and global access. Vaccine 2021, 39, 4266–4277. [Google Scholar] [CrossRef] [PubMed]
- Isidean, S.D.; Riddle, M.S.; Savarino, S.J.; Porter, C.K. A systematic review of ETEC epidemiology focusing on colonization factor and toxin expression. Vaccine 2011, 29, 6167–6178. [Google Scholar] [CrossRef]
- Poole, S.T.; McVeigh, A.L.; Anantha, R.P.; Lee, L.H.; Akay, Y.M.; Pontzer, E.A.; Scott, D.A.; Bullitt, E.; Savarino, S.J. Donor strand complementation governs intersubunit interaction of fimbriae of the alternate chaperone pathway. Mol. Microbiol. 2007, 63, 1372–1384. [Google Scholar] [CrossRef]
- Baker, K.K.; Levine, M.M.; Morison, J.; Phillips, A.; Barry, E.M. CfaE tip mutations in enterotoxigenic Escherichia coli CFA/I fimbriae define critical human intestinal binding sites. Cell. Microbiol. 2009, 11, 742–754. [Google Scholar] [CrossRef]
- Amcheslavsky, A.; Wallace, A.L.; Ejemel, M.; Li, Q.; McMahon, C.T.; Stoppato, M.; Giuntini, S.; Schiller, Z.A.; Pondish, J.R.; Toomey, J.R.; et al. Anti-CfaE nanobodies provide broad cross-protection against major pathogenic enterotoxigenic Escherichia coli strains, with implications for vaccine design. Sci. Rep. 2021, 11, 2751. [Google Scholar] [CrossRef]
- Sincock, S.A.; Hall, E.R.; Woods, C.M.; O’Dowd, A.; Poole, S.T.; McVeigh, A.L.; Nunez, G.; Espinoza, N.; Miller, M.; Savarino, S.J. Immunogenicity of a prototype enterotoxigenic Escherichia coli adhesin vaccine in mice and nonhuman primates. Vaccine 2016, 34, 284–291. [Google Scholar] [CrossRef]
- Maciel, M., Jr.; Bauer, D.; Baudier, R.L.; Bitoun, J.; Clements, J.D.; Poole, S.T.; Smith, M.A.; Kaminski, R.W.; Savarino, S.J.; Norton, E.B. Intradermal or Sublingual Delivery and Heat-Labile Enterotoxin Proteins Shape Immunologic Responses to a CFA/I Fimbria-Derived Subunit Antigen Vaccine against Enterotoxigenic Escherichia coli. Infect. Immun. 2019, 87, 10–1128. [Google Scholar] [CrossRef]
- Rollenhagen, J.E.; Woods, C.M.; O’Dowd, A.; Poole, S.T.; Tian, J.H.; Guebre-Xabier, M.; Ellingsworth, L.; Prouty, M.G.; Glenn, G.; Savarino, S.J. Evaluation of transcutaneous immunization as a delivery route for an enterotoxigenic E. coli adhesin-based vaccine with CfaE, the colonization factor antigen 1 (CFA/I) tip adhesin. Vaccine 2019, 37, 6134–6138. [Google Scholar] [CrossRef]
- Rollenhagen, J.E.; Jones, F.; Hall, E.; Maves, R.; Nunez, G.; Espinoza, N.; O’Dowd, A.; Prouty, M.G.; Savarino, S.J. Establishment, Validation, and Application of a New World Primate Model of Enterotoxigenic Escherichia coli Disease for Vaccine Development. Infect. Immun. 2019, 87, 10–1128. [Google Scholar] [CrossRef] [PubMed]
- Luiz, W.B.; Rodrigues, J.F.; Crabb, J.H.; Savarino, S.J.; Ferreira, L.C. Maternal vaccination with a fimbrial tip adhesin and passive protection of neonatal mice against lethal human enterotoxigenic Escherichia coli challenge. Infect. Immun. 2015, 83, 4555–4564. [Google Scholar] [CrossRef] [PubMed]
- Savarino, S.J.; McKenzie, R.; Tribble, D.R.; Porter, C.K.; O’Dowd, A.; Cantrell, J.A.; Sincock, S.A.; Poole, S.T.; DeNearing, B.; Woods, C.M.; et al. Prophylactic Efficacy of Hyperimmune Bovine Colostral Antiadhesin Antibodies against Enterotoxigenic Escherichia coli Diarrhea: A Randomized, Double-Blind, Placebo-Controlled, Phase 1 Trial. J. Infect. Dis. 2017, 216, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, R.L.; Riddle, M.S.; Porter, C.K.; Maciel, M., Jr.; Poole, S.T.; Laird, R.M.; Lane, M.; Turiansky, G.W.; Jarell, A.; Savarino, S.J. A First in Human Clinical Trial Assessing the Safety and Immunogenicity of Two Intradermally Delivered Enterotoxigenic Escherichia coli CFA/I Fimbrial Tip Adhesin Antigens with and without Heat-Labile Enterotoxin with Mutation LT(R192G). Microorganisms 2023, 11, 2689. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, R.L.; Porter, C.K.; Jarell, A.; Alcala, A.; Riddle, M.S.; Turiansky, G.W. A grading system for local skin reactions developed for clinical trials of an intradermal and transcutaneous ETEC vaccine. Vaccine 2020, 38, 3773–3779. [Google Scholar] [CrossRef]
- Porter, C.K.; Riddle, M.S.; Tribble, D.R.; Louis Bougeois, A.; McKenzie, R.; Isidean, S.D.; Sebeny, P.; Savarino, S.J. A systematic review of experimental infections with enterotoxigenic Escherichia coli (ETEC). Vaccine 2011, 29, 5869–5885. [Google Scholar] [CrossRef] [PubMed]
- Hanevik, K.; Chen, W.H.; Talaat, K.R.; Porter, C.; Bourgeois, L. The way forward for ETEC controlled human infection models (CHIMs). Vaccine 2019, 37, 4794–4799. [Google Scholar] [CrossRef] [PubMed]
- Porter, C.K.; Talaat, K.R.; Isidean, S.D.; Kardinaal, A.; Chakraborty, S.; Gutierrez, R.L.; Sack, D.A.; Bourgeois, A.L. The Controlled Human Infection Model for Enterotoxigenic Escherichia coli. Curr. Top. Microbiol. Immunol. 2021. [Google Scholar] [CrossRef]
- Harro, C.; Chakraborty, S.; Feller, A.; DeNearing, B.; Cage, A.; Ram, M.; Lundgren, A.; Svennerholm, A.M.; Bourgeois, A.L.; Walker, R.I.; et al. Refinement of a human challenge model for evaluation of enterotoxigenic Escherichia coli vaccines. Clin. Vaccine Immunol. 2011, 18, 1719–1727. [Google Scholar] [CrossRef] [PubMed]
- Porter, C.K.; Riddle, M.S.; Alcala, A.N.; Sack, D.A.; Harro, C.; Chakraborty, S.; Gutierrez, R.L.; Savarino, S.J.; Darsley, M.; McKenzie, R.; et al. An Evidenced-Based Scale of Disease Severity following Human Challenge with Enteroxigenic Escherichia coli. PLoS ONE 2016, 11, e0149358. [Google Scholar] [CrossRef]
- Talaat, K.R.; Bourgeois, A.L.; Frenck, R.W.; Chen, W.H.; MacLennan, C.A.; Riddle, M.S.; Suvarnapunya, A.E.; Brubaker, J.L.; Kotloff, K.L.; Porter, C.K. Consensus Report on Shigella Controlled Human Infection Model: Conduct of Studies. Clin. Infect. Dis. 2019, 69 (Suppl. S8), S580–S590. [Google Scholar] [CrossRef]
- Pocock, S. Group sequential methods in the design and analysis of clinical trials. Biometrika 1977, 64, 191–199. [Google Scholar] [CrossRef]
- Mantel, N.; Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar] [PubMed]
- Greenland, S.; Robins, J.M. Estimation of a common effect parameter from sparse follow-up data. Biometrics 1985, 41, 55–68. [Google Scholar] [CrossRef]
- Breslow, N.E.; Day, N.E. Statistical methods in cancer research. Volume I—The analysis of case-control studies. IARC Sci. Publ. 1980, 32, 5–338. [Google Scholar]
- Talaat, K.R.; Alaimo, C.; Martin, P.; Bourgeois, A.L.; Dreyer, A.M.; Kaminski, R.W.; Porter, C.K.; Chakraborty, S.; Clarkson, K.A.; Brubaker, J.; et al. Human challenge study with a Shigella bioconjugate vaccine: Analyses of clinical efficacy and correlate of protection. EBioMedicine 2021, 66, 103310. [Google Scholar] [CrossRef]
- McArthur, M.A.; Chen, W.H.; Magder, L.; Levine, M.M.; Sztein, M.B. Impact of CD4+ T Cell Responses on Clinical Outcome following Oral Administration of Wild-Type Enterotoxigenic Escherichia coli in Humans. PLoS Negl. Trop. Dis. 2017, 11, e0005291. [Google Scholar] [CrossRef] [PubMed]
- Frenck, R.W., Jr.; Dickey, M.; Suvarnapunya, A.E.; Chandrasekaran, L.; Kaminski, R.W.; Clarkson, K.A.; McNeal, M.; Lynen, A.; Parker, S.; Hoeper, A.; et al. Establishment of a Controlled Human Infection Model with a Lyophilized Strain of Shigella sonnei 53G. mSphere 2020, 5, 10–1128. [Google Scholar] [CrossRef]
- Frenck, R.W., Jr.; Conti, V.; Ferruzzi, P.; Ndiaye, A.G.W.; Parker, S.; McNeal, M.M.; Dickey, M.; Granada, J.P.; Cilio, G.L.; De Ryck, I.; et al. Efficacy, safety, and immunogenicity of the Shigella sonnei 1790GAHB GMMA candidate vaccine: Results from a phase 2b randomized, placebo-controlled challenge study in adults. EClinicalMedicine 2021, 39, 101076. [Google Scholar] [CrossRef]
- Poncet, D.; Hessler, C.; Liang, H.; Gautheron, S.; Sergent, M.; Rintala, N.D.; Seydoux, E.; Huang, P.D.; Argilla, D.; Ruiz, S.; et al. Preclinical optimization of an enterotoxigenic Escherichia coli adjuvanted subunit vaccine using response surface design of experiments. npj Vaccines 2020, 5, 83. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Shahabudin, S.; Farid, S.; Lee, L.H.; McVeigh, A.L.; Maciel, M., Jr.; Poole, S.T.; Broadman, M.; Prouty, M.G.; Savarino, S.J. Cross-Reactivity, Epitope Mapping, and Potency of Monoclonal Antibodies to Class 5 Fimbrial Tip Adhesins of Enterotoxigenic Escherichia coli. Infect. Immun. 2020, 88, 10–1128. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Poncet, D.; Seydoux, E.; Rintala, N.D.; Maciel, M., Jr.; Ruiz, S.; Orr, M.T. The TLR4 agonist adjuvant SLA-SE promotes functional mucosal antibodies against a parenterally delivered ETEC vaccine. npj Vaccines 2019, 4, 19. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Maciel, M., Jr.; O’Dowd, A.; Poole, S.T.; Rollenhagen, J.E.; Etobayeva, I.V.; Savarino, S.J. Development and Comparison of a Panel of Modified CS17 Fimbrial Tip Adhesin Proteins as Components for an Adhesin-Based Vaccine against Enterotoxigenic Escherichia coli. Microorganisms 2021, 9, 1646. [Google Scholar] [CrossRef]
- Li, S.; Seo, H.; Upadhyay, I.; Zhang, W. A Polyvalent Adhesin-Toxoid Multiepitope-Fusion-Antigen-Induced Functional Antibodies against Five Enterotoxigenic Escherichia coli Adhesins (CS7, CS12, CS14, CS17, and CS21) but Not Enterotoxins (LT and STa). Microorganisms 2023, 11, 2473. [Google Scholar] [CrossRef]
- Lee, T.; Gutierrez, R.L.; Maciel, M.; Poole, S.; Testa, K.J.; Trop, S.; Duplessis, C.; Lane, A.; Riddle, M.S.; Hamer, M.; et al. Safety and immunogenicity of intramuscularly administered CS6 subunit vaccine with a modified heat-labile enterotoxin from enterotoxigenic Escherichia coli. Vaccine 2021, 39, 5548–5556. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort 1 | Cohort 2 | Cohort 3 | All Cohorts | |||||
|---|---|---|---|---|---|---|---|---|
| Vaccine (n = 19) | Naïve (n = 11) | Vaccine (n = 9) | Naïve (n = 17) | Vaccine (n = 13) | Naïve (n = 15) | Vaccine (n = 41) | Naïve (n = 43) | |
| Mean Age (SD) | 34.0 (8.2) | 32.6 (9.0) | 39.0 (8.4) | 36.0 (9.7) | 32.5 (8.8) | 33.1 (7.1) | 34.6 (8.6) | 34.1 (8.6) |
| Sex; n (%) | ||||||||
| Male | 13 (68.4) | 8 (72.7) | 7 (77.8) | 12 (70.6) | 8 (61.5) | 6 (40.0) | 28 (68.3) | 26 (60.5) |
| Female | 6 (31.6) | 3 (27.3) | 2 (22.2) | 5 (29.4) | 5 (38.5) | 9 (60.0) | 13 (31.7) | 17 (39.5) |
| Race; n (%) | ||||||||
| Caucasian | 1 (5.3) | 1 (9.1) | 0 (0.0) | 1 (5.9) | 1 (7.7) | 2 (14.3) | 2 (4.9) | 4 (9.5) |
| Black | 18 (94.7) | 10 (90.9) | 8 (88.9) | 16 (94.2) | 12 (92.3) | 9 (64.3) | 38 (92.7) | 35 (83.3) |
| Asian | 0 (0.0) | 0 (0.0) | 1 (11.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (2.4) | 0 (0.0) |
| Multi-Race | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 3 (21.4) | 0 (0.0) | 3 (7.1) |
| Ethnicity; n (%) | ||||||||
| Hispanic/Latino | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (5.9) | 2 (15.4) | 2 (13.3) | 2 (4.9) | 3 (7.0) |
| Non-Hispanic/Latino | 19 (100) | 11 (100) | 9 (100) | 16 (94.1) | 11 (84.6) | 13 (86.7) | 39 (95.1) | 40 (93.0) |
| Adverse Event | Cohort 1 (N = 23) | Cohort 2 (N = 14) | Cohort 3 (N = 19) | Total (N = 56) |
|---|---|---|---|---|
| Decreased Absolute Lymphocytes | 1 (4.3) | 0 (0.0) | 0 (0.0) | 1 (1.8) |
| Elevated ALT | 1 (4.3) | 0 (0.0) | 0 (0.0) | 1 (1.8) |
| Chills | 2 (8.7) | 1 (7.1) | 0 (0.0) | 3 (5.4) |
| Fever | 1 (4.3) | 0 (0.00) | 0 (0.0) | 1 (1.8) |
| Arthralgia | 2 (8.7) | 2 (14.3) | 0 (0.0) | 4 (7.1) |
| Myalgia | 2 (8.7) | 2 (14.3) | 0 (0.0) | 4 (7.1) |
| Lightheadedness | 1 (4.3) | 0 (0.0) | 1 (5.3) | 2 (3.6) |
| Malaise | 2 (8.7) | 2 (14.3) | 0 (0.0) | 4 (7.1) |
| Fatigue | 0 (0.0) | 0 (0.0) | 1 (5.3) | 1 (1.8) |
| Headache | 3 (13.0) | 4 (28.6) | 1 (5.3) | 8 (14.3) |
| Abdominal Pain | 1 (4.3) | 0 (0.0) | 0 (0.0) | 1 (1.8) |
| Nausea | 2 (8.7) | 0 (0.0) | 0 (0.0) | 2 (3.6) |
| Muscle Twitch Right Arm | 0 (0.0) | 1 (7.1) | 0 (0.0) | 1 (1.8) |
| Right Deltoid Pain | 0 (0.0) | 1 (7.1) | 0 (0.0) | 1 (1.8) |
| Left Deltoid Pain | 0 (0.0) | 1 (7.1) | 0 (0.0) | 1 (1.8) |
| Vaccine Site Pain | 5 (21.7) | 5 (35.7) | 1 (5.3) | 11 (19.6) |
| Vaccine Site Pruritus | 21 (91.3) | 10 (71.4) | 18 (94.7) | 49 (87.5) |
| Vaccine Site Reaction | 23 (100) | 14 (100) | 19 (100) | 56 (100) |
| Vaccine Site Swelling | 1 (4.3) | 0 (0.0) | 7 (36.8) | 8 (12.5) |
| Vaccine Site Tenderness | 14 (60.9) | 6 (42.9) | 12 (63.2) | 32 (57.1) |
| Dose 1 (n = 56) | Dose 2 (n = 55) | Dose 3 (n = 52) | |
|---|---|---|---|
| Erythema (any) | 56 (100%) | 37 (67%) | 36 (69%) |
| Score 1 | 15 (27%) | 16 (29%) | 15 (29%) |
| Score 2 | 27 (48%) | 13 (24%) | 11 (21%) |
| Score 3 | 14 (25%) | 8 (15%) | 10 (19%) |
| Score 4 | 0 (0%) | 0 (0%) | 0 (0%) |
| Score 5 | 0 (0%) | 0 (0%) | 0 (0%) |
| Induration (any) | 56 (100%) | 54 (98%) | 52 (100%) |
| Score 1 | 0 (0%) | 0 (0%) | 2 (4%) |
| Score 2 | 16 (29%) | 30 (55%) | 35 (67%) |
| Score 3 | 29 (52%) | 16 (29%) | 15 (29%) |
| Score 4 | 8 (14%) | 5 (9%) | 0 (0%) |
| Score 5 | 3 (5%) | 3 (5%) | 0 (0%) |
| Hyperpigmentation (any) | 56 (100%) | 55 (100%) | 50 (96%) |
| Score 1 | 2 (4%) | 6 (11%) | 11 (21%) |
| Score 2 | 9 (16%) | 25 (45%) | 21 (40%) |
| Score 3 | 28 (50%) | 16 (29%) | 16 (31%) |
| Score 4 | 17 (30%) | 8 (15%) | 2 (4%) |
| Score 5 | 0 (0%) | 0 (0%) | 0 (0%) |
| Hypopigmentation (any) | 1 (2%) | 9 (16%) | 3 (6%) |
| Score 1 | 0 (0%) | 4 (7%) | 1 (2%) |
| Score 2 | 1 (2%) | 3 (5%) | 1 (2%) |
| Score 3 | 0 (0%) | 2 (4%) | 1 (2%) |
| Score 4 | 0 (0%) | 0 (0%) | 0 (0%) |
| Score 5 | 0 (0%) | 0 (0%) | 0 (0%) |
| Edema (any) | 11 (20%) | 0 (0%) | 0 (0%) |
| Score 1 | 0 (0%) | 0 (0%) | 0 (0%) |
| Score 2 | 8 (14%) | 0 (0%) | 0 (0%) |
| Score 3 | 3 (5%) | 0 (0%) | 0 (0%) |
| Score 4 | 0 (0%) | 0 (0%) | 0 (0%) |
| Score 5 | 0 (0%) | 0 (0%) | 0 (0%) |
| Cohort | Challenge Dose (cfu) | Naïve n/N (%) | Vaccinee n/N (%) | Efficacy Estimate 95% CI (%) |
|---|---|---|---|---|
| 1 | 1.0 × 107 | 5/11 (45.5%) | 9/19 (47.4%) | −3.6 (−106.2–47.9) |
| 2 | 1.2 × 107 | 11/17 (64.7%) | 1/9 (11.1%) | 60.3 (21.3–80.0) |
| 3 | 1.9 × 107 | 8/15 (53.3%) | 6/13 (46.2%) | 13.3 (−81.5–58.6) |
| All | -- | 24/43 (55.8%) | 16/41 (39.0%) | * 27.8 (−7.5–51.6) |
| Adverse Event | Naïve | Vaccine | ||||
|---|---|---|---|---|---|---|
| Mild | Mod-Sev | Any | Mild | Mod-Sev | Any | |
| Abdominal Cramps | 8 (18.6) | 20 (46.5) | 28 (65.1) | 11 (26.8) | 6 (14.6) | 17 (41.5) |
| Abdominal Pain | 0 (0.0) | 15 (34.9) | 15 (34.9) | 3 (7.3) | 4 (9.8) | 7 (17.1) |
| Anorexia | 4 (9.3) | 19 (44.2) | 23 (53.5) | 6 (14.6) | 6 (14.6) | 12 (29.3) |
| Headache | 7 (16.3) | 10 (23.3) | 17 (39.5) | 5 (12.2) | 8 (19.5) | 13 (31.7) |
| Lightheadedness | 5 (11.6) | 3 (7.0) | 8 (18.6) | 3 (7.3) | 1 (2.4) | 4 (9.8) |
| Malaise | 4 (9.3) | 17 (39.5) | 21 (48.8) | 7 (17.1) | 6 (14.6) | 13 (31.7) |
| Vomiting | 4 (9.3) | 8 (18.6) | 12 (27.9) | 2 (4.9) | 1 (2.4) | 3 (7.3) |
| Nausea | 11 (25.6) | 8 (18.6) | 19 (44.2) | 6 (14.6) | 4 (9.8) | 10 (24.4) |
| Serum IgG | Serum IgA | ALS IgA | |
|---|---|---|---|
| anti-CfaE | 41 (100) | 25 (61.0) | 40 (97.6) |
| anti-LT | 36 (87.8) | 26 (63.4) | 28 (68.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez, R.L.; Porter, C.K.; Harro, C.; Talaat, K.; Riddle, M.S.; DeNearing, B.; Brubaker, J.; Maciel, M., Jr.; Laird, R.M.; Poole, S.; et al. Efficacy Evaluation of an Intradermally Delivered Enterotoxigenic Escherichia coli CF Antigen I Fimbrial Tip Adhesin Vaccine Coadministered with Heat-Labile Enterotoxin with LT(R192G) against Experimental Challenge with Enterotoxigenic E. coli H10407 in Healthy Adult Volunteers. Microorganisms 2024, 12, 288. https://doi.org/10.3390/microorganisms12020288
Gutiérrez RL, Porter CK, Harro C, Talaat K, Riddle MS, DeNearing B, Brubaker J, Maciel M Jr., Laird RM, Poole S, et al. Efficacy Evaluation of an Intradermally Delivered Enterotoxigenic Escherichia coli CF Antigen I Fimbrial Tip Adhesin Vaccine Coadministered with Heat-Labile Enterotoxin with LT(R192G) against Experimental Challenge with Enterotoxigenic E. coli H10407 in Healthy Adult Volunteers. Microorganisms. 2024; 12(2):288. https://doi.org/10.3390/microorganisms12020288
Chicago/Turabian StyleGutiérrez, Ramiro L., Chad K. Porter, Clayton Harro, Kawsar Talaat, Mark S. Riddle, Barbara DeNearing, Jessica Brubaker, Milton Maciel, Jr., Renee M. Laird, Steven Poole, and et al. 2024. "Efficacy Evaluation of an Intradermally Delivered Enterotoxigenic Escherichia coli CF Antigen I Fimbrial Tip Adhesin Vaccine Coadministered with Heat-Labile Enterotoxin with LT(R192G) against Experimental Challenge with Enterotoxigenic E. coli H10407 in Healthy Adult Volunteers" Microorganisms 12, no. 2: 288. https://doi.org/10.3390/microorganisms12020288