
Bartonella- and Borrelia-Related Disease Presenting as a Neurological Condition Revealing the Need for Better Diagnostics

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. DNA Extraction from Blood
2.3. PCR Primers and Positive Controls
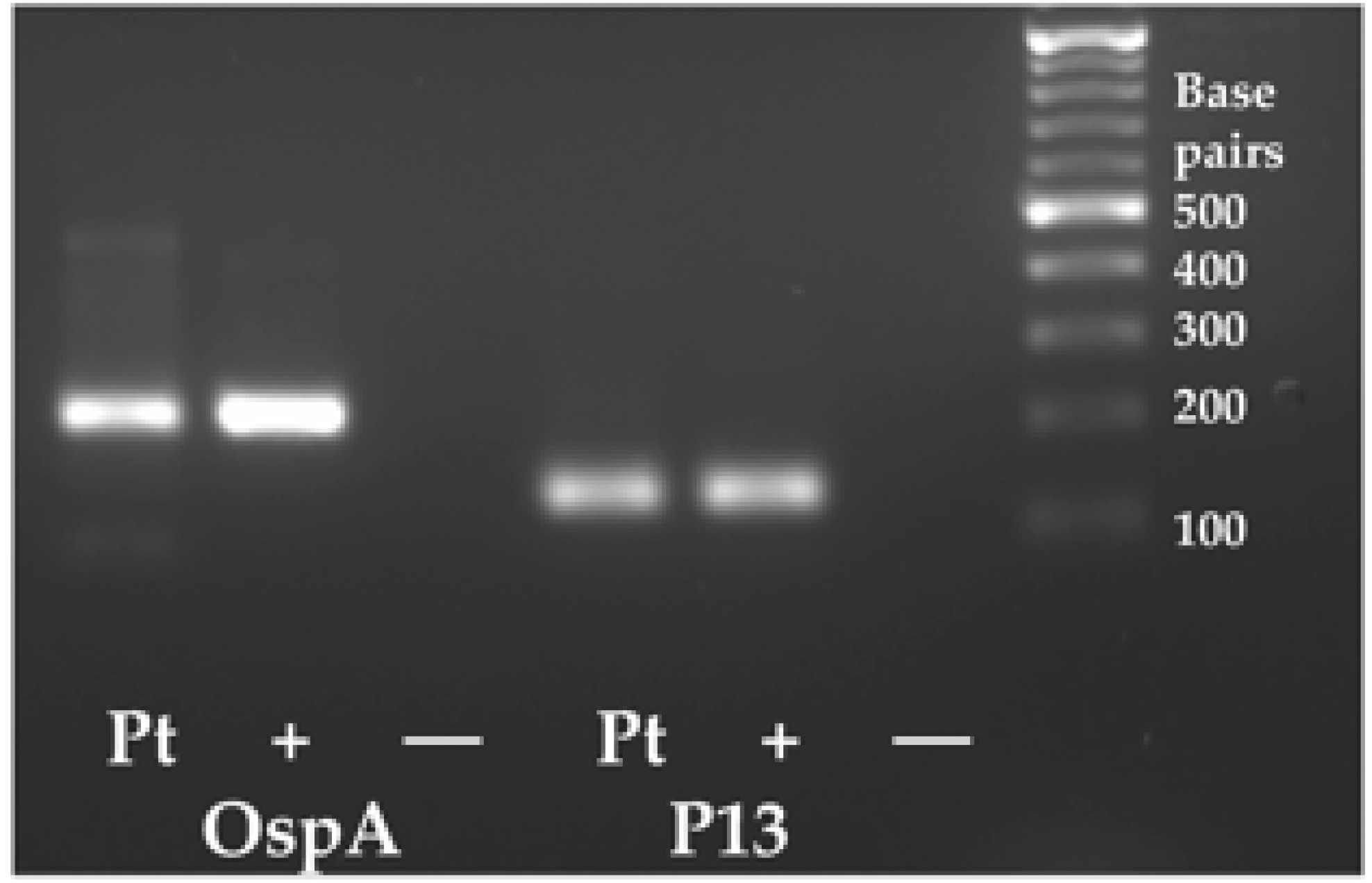
2.4. PCR Methods and Direct Sequencing
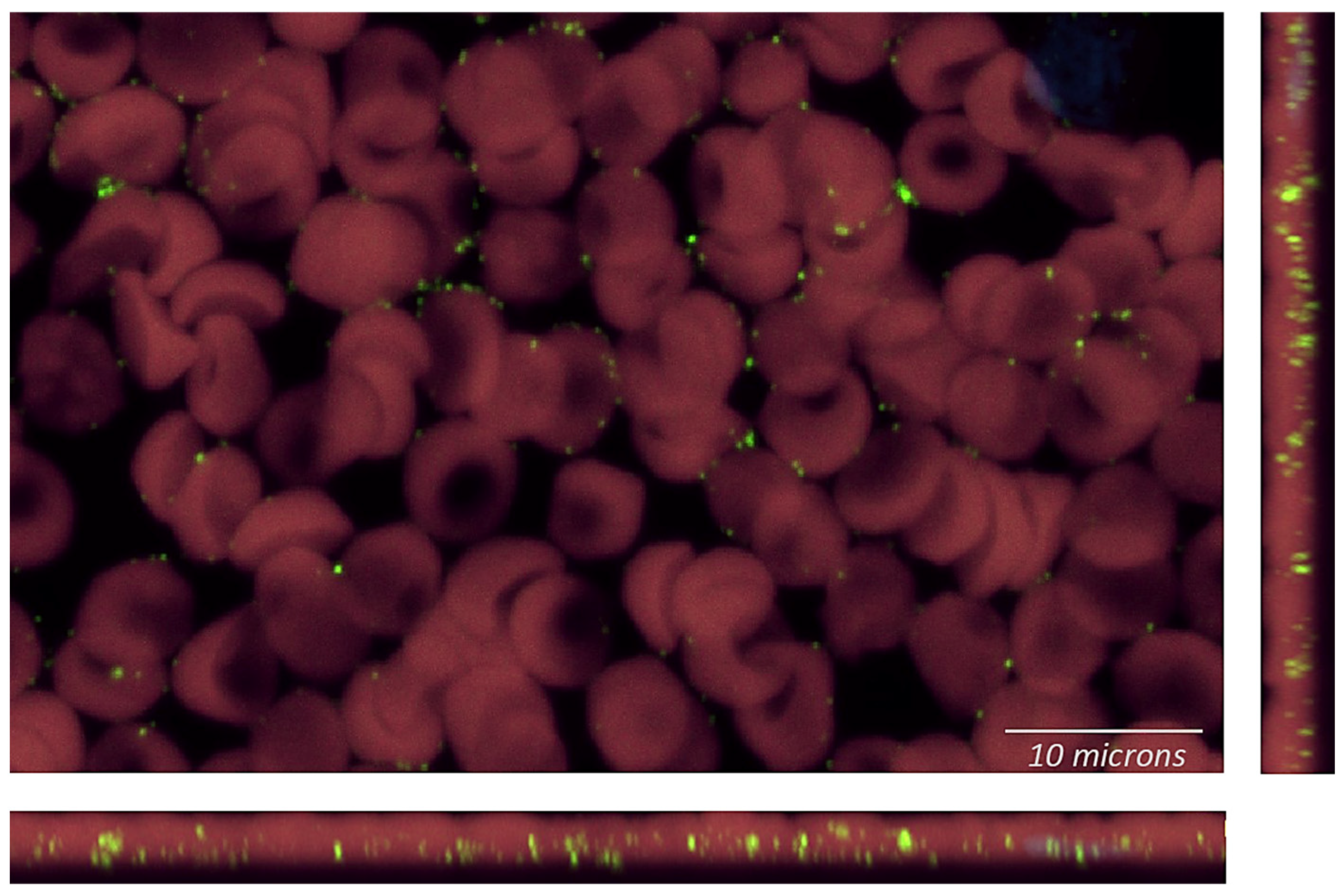
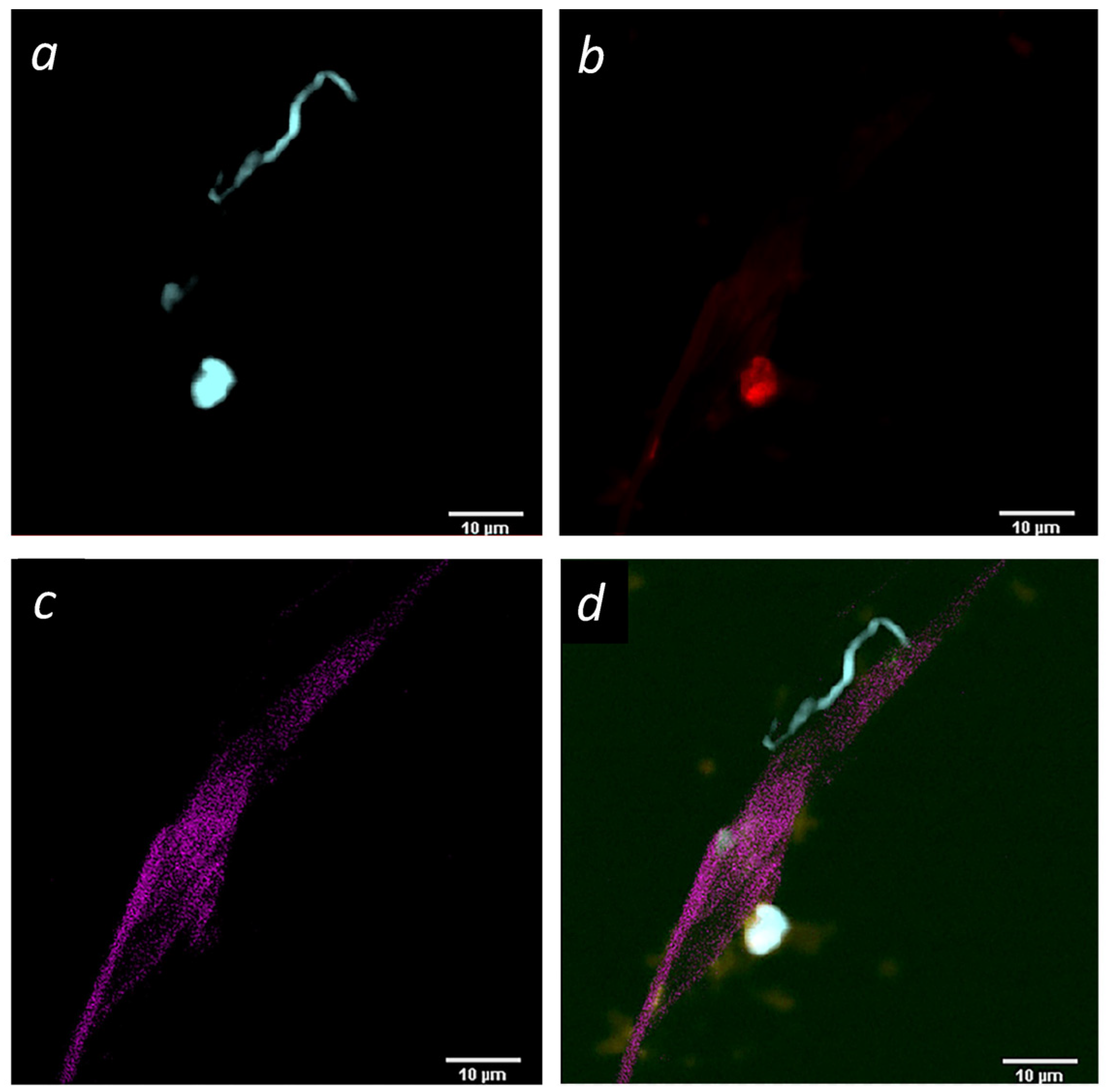
2.5. Imaging of Blood Smears and Buffy Coat Smears Following rRNA Fluorescent In Situ Hybridization (FISH)
3. Case Presentation
4. Discussion
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ben-Tekaya, H.; Gorvel, J.P.; Dehio, C. Bartonella and Brucella--weapons and strategies for stealth attack. Cold Spring Harb. Perspect. Med. 2013, 3, a010231. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.R.; Dos Santos, L.S.; de Almeida, A.R.; Lins, K.A.; Barjas-Castro, M.L.; Diniz, P.P.V.P.; Velho, P.E.N.F. Comparison of molecular methods for Bartonella henselae detection in blood donors. PLoS Negl. Trop. Dis. 2023, 17, e0011336. [Google Scholar] [CrossRef] [PubMed]
- Okaro, U.; Addisu, A.; Casanas, B.; Anderson, B. Bartonella Species, an Emerging Cause of Blood-Culture-Negative Endocarditis. Clin. Microbiol. Rev. 2017, 30, 709–746. [Google Scholar] [CrossRef] [PubMed]
- García-Álvarez, L.; García-García, C.; Muñoz, P.; Fariñas-Álvarez, M.D.C.; Cuadra, M.G.; Fernández-Hidalgo, N.; García-Vázquez, E.; Moral-Escudero, E.; Alonso-Socas, M.D.M.; García-Rosado, D.; et al. On Behalf Of Grupo de Apoyo Al Manejo de la Endocarditis Infecciosa En España Games. Bartonella Endocarditis in Spain: Case Reports of 21 Cases. Pathogens 2022, 11, 561. [Google Scholar] [CrossRef] [PubMed]
- Berghoff, W. Chronic Lyme Disease and Co-infections: Differential Diagnosis. Open Neurol. J. 2012, 6, 158–178. [Google Scholar] [CrossRef] [PubMed]
- Maggi, R.G.; Mozayeni, B.R.; Pultorak, E.L.; Hegarty, B.C.; Bradley, J.M.; Correa, M.; Breitschwerdt, E.B. Bartonella spp. bacteremia and rheumatic symptoms in patients from Lyme disease-endemic region. Emerg. Infect. Dis. 2012, 18, 783–791. [Google Scholar] [CrossRef]
- Koutantou, M.; Kambas, K.; Makka, S.; Fournier, P.E.; Raoult, D.; Angelakis, E. Limitations of Serological Diagnosis of Typical Cat Scratch Disease and Recommendations for the Diagnostic Procedure. Can. J. Infect. Dis. Med. Microbiol. 2023, 2023, 4222511. [Google Scholar] [CrossRef] [PubMed]
- Hegarty, B.C.; Bradley, J.M.; Lappin, M.R.; Balakrishnan, N.; Mascarelli, P.E.; Breitschwerdt, E.B. Analysis of seroreactivity against cell culture-derived Bartonella spp. antigens in dogs. J. Vet. Intern. Med. 2014, 28, 38–41. [Google Scholar] [CrossRef]
- Allizond, V.; Costa, C.; Sidoti, F.; Scutera, S.; Bianco, G.; Sparti, R.; Banche, G.; Dalmasso, P.; Cuffini, A.M.; Cavallo, R.; et al. Serological and molecular detection of Bartonella henselae in specimens from patients with suspected cat scratch disease in Italy: A comparative study. PLoS ONE 2019, 14, e0211945. [Google Scholar] [CrossRef]
- McCormick, D.W.; Rassoulian-Barrett, S.L.; Hoogestraat, D.R.; Salipante, S.J.; SenGupta, D.; Dietrich, E.A.; Cookson, B.T.; Marx, G.E.; Lieberman, J.A. Bartonella spp. Infections Identified by Molecular Methods, United States. Emerg. Infect. Dis. 2023, 29, 467–476. [Google Scholar] [CrossRef]
- Ericson, M.E.; Breitschwerdt, E.B.; Reicherter, P.; Maxwel, C.; Maggi, R.G.; Melvin, R.G.; Maluki, A.H.; Bradley, J.M.; Miller, J.C.; Simmons, G.E.; et al. Bartonella henselae Detected in Malignant Melanoma, a Preliminary Study. Pathogens 2021, 10, 326. [Google Scholar] [CrossRef] [PubMed]
- Jacomo, V.; Kelly, P.J.; Raoult, D. Natural history of Bartonella infections (an exception to Koch’s postulate). Clin. Diagn. Lab. Immunol. 2002, 9, 8–18. [Google Scholar] [CrossRef]
- Scott, J.D. Presentation of Acrodermatitis Chronica Atrophicans Rashes on Lyme Disease Patients in Canada. Healthcare 2020, 8, 157. [Google Scholar] [CrossRef] [PubMed]
- Kinderlehrer, D.A. Anorexia Nervosa Caused by Polymicrobial Tick-Borne Infections: A Case Study. Int. Med. Case Rep. J. 2021, 14, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Lashnits, E.; Maggi, R.; Jarskog, F.; Bradley, J.; Breitschwerdt, E.; Frohlich, F. Schizophrenia and Bartonella spp. Infection: A Pilot Case-Control Study. Vector Borne Zoonotic Dis. 2021, 21, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Breitschwerdt, E.B.; Bradley, J.M.; Maggi, R.G.; Lashnits, E.; Reicherter, P. Bartonella Associated Cutaneous Lesions (BACL) in People with Neuropsychiatric Symptoms. Pathogens 2020, 9, 1023. [Google Scholar] [CrossRef] [PubMed]
- Breitschwerdt, E.B. Bartonellosis, One Health and all creatures great and small. Vet. Dermatol. 2017, 28, 96-e21. [Google Scholar] [CrossRef]
- Gutiérrez, R.; Vayssier-Taussat, M.; Buffet, J.P.; Harrus, S. Guidelines for the Isolation, Molecular Detection, and Characterization of Bartonella Species. Vector Borne Zoonotic Dis. 2017, 17, 42–50. [Google Scholar] [CrossRef]
- CDC Website. Available online: https://www.cdc.gov/bartonella/faq.html (accessed on 29 October 2023).
- Osterhoudt, K.C.; Zaoutis, T.; Zorc, J.J. Lyme disease masquerading as brown recluse spider bite. Ann. Emerg. Med. 2002, 39, 558–561. [Google Scholar] [CrossRef]
- Mascarelli, P.E.; Maggi, R.G.; Hopkins, S.; Mozayeni, B.R.; Trull, C.L.; Bradley, J.M.; Hegarty, B.C.; Breitschwerdt, E.B. Bartonella henselae infection in a family experiencing neurological and neurocognitive abnormalities after woodlouse hunter spider bites. Parasit. Vectors 2013, 15, 98. [Google Scholar] [CrossRef]
- Eskow, E.; Rao, R.S.; Mordechai, E. Concurrent Infection of the Central Nervous System by Borrelia burgdorferi and Bartonella henselae: Evidence for a Novel Tick-borne Disease Complex. Arch. Neurol. 2001, 58, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Podsiadły, E.; Chmielewski, T.; Tylewska-Wierzbanowska, S. Bartonella henselae and Borrelia burgdorferi infections of the central nervous system. Ann. N. Y Acad. Sci. 2003, 990, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Ericson, M.; Balakrishnan, N.; Mozayeni, B.R.; Woods, C.W.; Dencklau, J.; Kelly, S.; Breitschwerdt, E.B. Culture, PCR, DNA sequencing, and second harmonic generation (SHG) visualization of Bartonella henselae from a surgically excised human femoral head. Clin. Rheumatol. 2017, 36, 1669–1675. [Google Scholar] [CrossRef] [PubMed]
- Szymczak, Z.; Płusa, T.; Baranowski, P.; Krawczyk, J. Hip arthoplasty in a forester after numerous tick bites. Int. J. Occup. Med. Environ. Health 2021, 34, 693–699. [Google Scholar] [CrossRef]
- CDC Website. Available online: https://www.cdc.gov/lyme/diagnosistesting/index.html (accessed on 14 January 2024).
- Stricker, R.B.; Johnson, L. Lyme disease diagnosis and treatment: Lessons from the AIDS epidemic. Minerva Med. 2010, 101, 419–425. [Google Scholar]
- CDC Website. Available online: https://wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/bartonella-infections#diagnosis (accessed on 14 January 2024).
- Marques, A.R. Laboratory diagnosis of Lyme disease: Advances and challenges. Infect. Dis. Clin. North Am. 2015, 29, 295–307. [Google Scholar] [CrossRef]
- Godfrey, R.; Curtis, S.; Schilling, W.H.; James, P.R. Blood culture negative endocarditis in the modern era of 16S rRNA sequencing. Clin. Med. 2020, 20, 412–416. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Diagnostic Test | Months after Bite | |
|---|---|---|
| 5 Months * | 12 Months * | |
| Bartonella henselae IgG Ab | Negative | |
| Bartonella henselae IgM Ab | Negative | |
| Bartonella quintana IgG Ab | Negative | |
| Bartonella quintana IgM Ab | Negative | |
| Parvovirus B19 PCR | Negative | |
| Lyme disease was not suspected due to the absence of a tick bite | Not tested | |
| Bartonella henselae IgG/IgM by (ELISA) | Negative | |
| Bartonella henselae PCR | Negative | |
| Bartonella clarridgeiae PCR | Negative | |
| Bartonella bacilloformis PCR | Negative | |
| Bartonella elizabethae PCR | Negative | |
| Bartonella quintana PCR | Negative | |
| Lyme disease Western blot (Borrelia burgdorferi) IgG/IgM By CDC or alternative criteria | Negative | |
| Borrelia miyamotoi PCR | Negative | |
| Borrelia turicatae PCR | Negative | |
| Borrelia mayonii PCR | Negative | |
| Borrelia hermsii PCR | Negative | |
| Borrelia parkeri PCR | Negative | |
| Babesia microti IgG/IgM by IFA | Negative | |
| Babesia microti IgG/IgM | Negative | |
| Babesia microti PCR | Negative | |
| Babesia duncani PCR | Negative | |
| Pathogen and Novel Diagnostic Test | Months after Bite | ||
|---|---|---|---|
| 5 Months | 36 Months | 60 Months | |
| Bartonella henselae PCR | Positive (16S intergenic) | Positive (BRT1) | Positive (BRT1) |
| Bartonella vinsonii PCR | Positive (16S intergenic) | ||
| Borrelia burgdorferi PCR | Positive (OspA) | Positive (OspA) | |
| Babesia microti PCR | Negative (18S) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ericson, M.E.; Mozayeni, B.R.; Radovsky, L.; Bemis, L.T. Bartonella- and Borrelia-Related Disease Presenting as a Neurological Condition Revealing the Need for Better Diagnostics. Microorganisms 2024, 12, 209. https://doi.org/10.3390/microorganisms12010209
Ericson ME, Mozayeni BR, Radovsky L, Bemis LT. Bartonella- and Borrelia-Related Disease Presenting as a Neurological Condition Revealing the Need for Better Diagnostics. Microorganisms. 2024; 12(1):209. https://doi.org/10.3390/microorganisms12010209
Chicago/Turabian StyleEricson, Marna E., B. Robert Mozayeni, Laurie Radovsky, and Lynne T. Bemis. 2024. "Bartonella- and Borrelia-Related Disease Presenting as a Neurological Condition Revealing the Need for Better Diagnostics" Microorganisms 12, no. 1: 209. https://doi.org/10.3390/microorganisms12010209