
Prevalence and Clinical Characteristics of Bacterial Pneumonia in Neurosurgical Emergency Center Patients: A Retrospective Study Spanning 13 Years at a Tertiary Center
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Bacterial Isolates and Susceptibility Testing
2.3. Statistical Analysis
3. Results
3.1. Demographics and Epidemiology
3.2. Trends in Bacterial Isolates
3.3. AMR Patterns of Top Four Bacteria
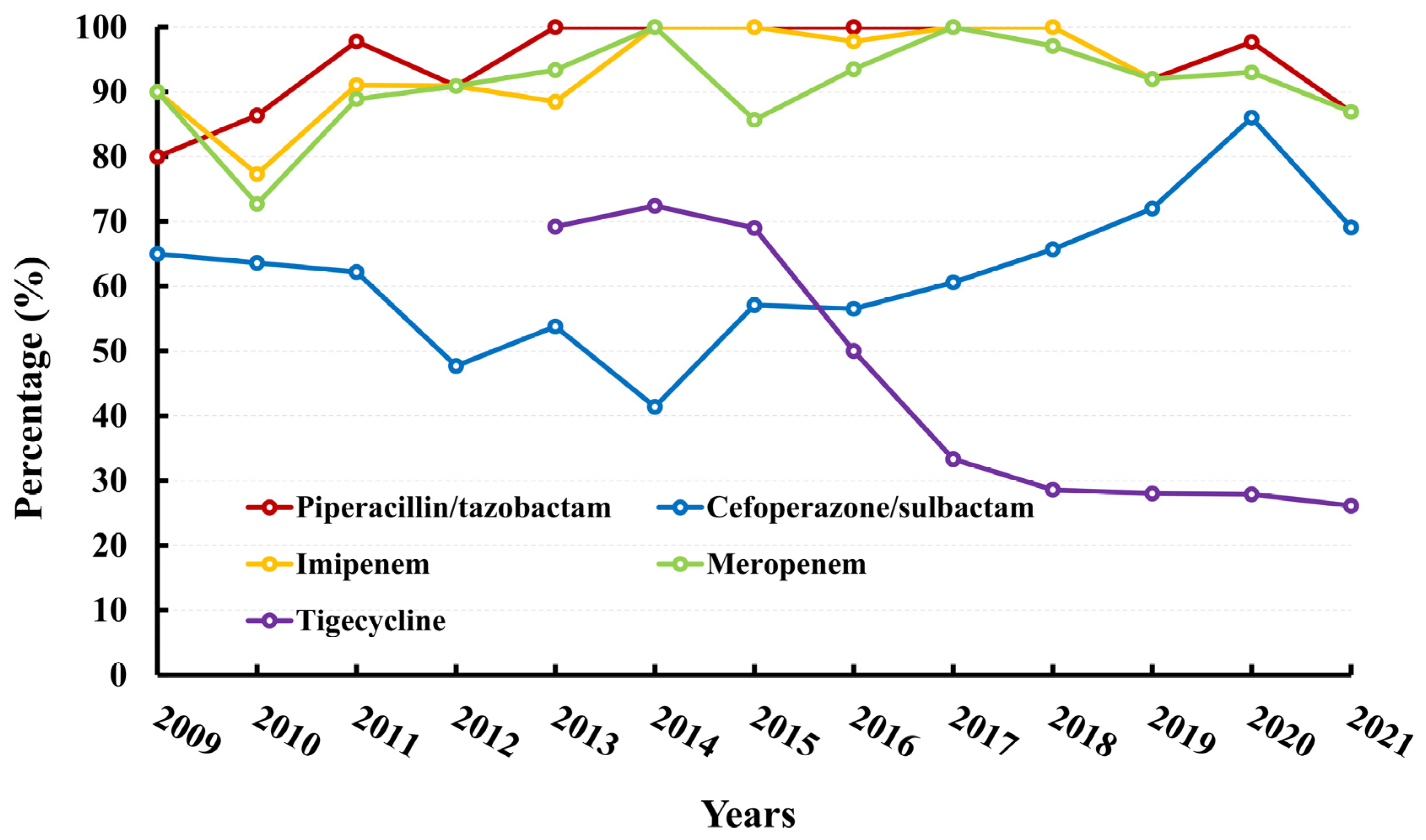
3.3.1. Klebsiella pneumoniae
3.3.2. Acinetobacter baumanni
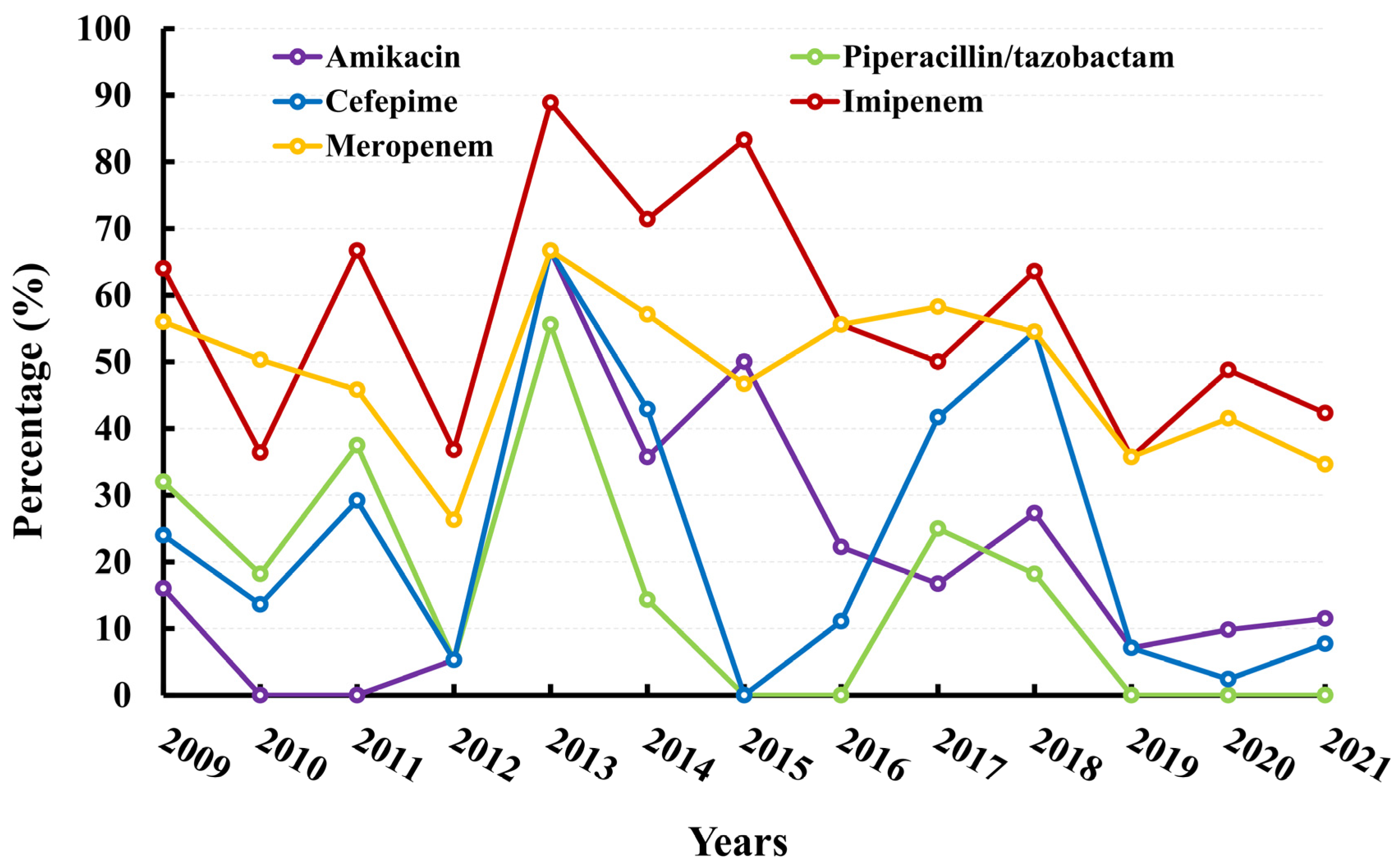
3.3.3. Pseudomonas aeruginosa
3.3.4. Staphylococcus aureus
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Erfani, Z.; Mamaghani, H.J.; Rawling, J.A.; Eajazi, A.; Deever, D.; Mirmoeeni, S.; Jafari, A.A.; Seifi, A. Pneumonia in Nervous System Injuries: An Analytic Review of Literature and Recommendations. Cureus 2022, 14, e25616. [Google Scholar] [CrossRef]
- Caceres, E.; Olivella, J.C.; Yanez, M.; Viñan, E.; Estupiñan, L.; Boada, N.; Martin-Loeches, I.; Reyes, L.F. Risk factors and outcomes of lower respiratory tract infections after traumatic brain injury: A retrospective observational study. Front. Med. 2023, 10, 1077371. [Google Scholar] [CrossRef]
- Roquilly, A.; Feuillet, F.; Seguin, P.; Lasocki, S.; Cinotti, R.; Launey, Y.; Thioliere, L.; Le Floch, R.; Mahe, P.J.; Nesseler, N.; et al. Empiric antimicrobial therapy for ventilator-associated pneumonia after brain injury. Eur. Respir. J. 2016, 47, 1219–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tacconelli, E.; Sifakis, F.; Harbarth, S.; Schrijver, R.; van Mourik, M.; Voss, A.; Sharland, M.; Rajendran, N.B.; Rodríguez-Baño, J.; Bielicki, J.; et al. Surveillance for control of antimicrobial resistance. Lancet Infect. Dis. 2018, 18, e99–e106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marutescu, L.G. Current and Future Flow Cytometry Applications Contributing to Antimicrobial Resistance Control. Microorganisms 2023, 11, 1300. [Google Scholar] [CrossRef] [PubMed]
- Chaibi, K.; Pean, D.P.G.; Dortet, L.; Zahar, J.R.; Pilmis, B. Empiric Treatment in HAP/VAP: “Don’t You Want to Take a Leap of Faith?”. Antibiotics 2022, 11, 359. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, J.S.; Albarrak, M.; Alhasawi, A.; Al-Musawi, T.; Alraddadi, B.M.; Wali, W.A.; Elhoufi, A.; Habashy, N.; Hassanien, A.M.; Kurdi, A. Narrative Review of the Epidemiology of Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia in Gulf Cooperation Council Countries. Infect. Dis. Ther. 2023, 12, 1741–1773. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratala, J.; et al. Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef] [Green Version]
- Hu, F.; Zhu, D.; Wang, F.; Wang, M. Current Status and Trends of Antibacterial Resistance in China. Clin. Infect. Dis. 2018, 67, S128–S134. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Mao, Y.; Zhu, J.H.; Zhou, L.F. The Department of Neurosurgery at Shanghai Huashan Hospital. Neurosurgery 2008, 62, 947–953. [Google Scholar] [CrossRef]
- Fernando, S.M.; Tran, A.; Cheng, W.; Klompas, M.; Kyeremanteng, K.; Mehta, S.; English, S.; Muscedere, J.; Cook, D.J.; Torres, A.; et al. Diagnosis of ventilator-associated pneumonia in critically ill adult patients-a systematic review and meta-analysis. Intensive Care Med. 2020, 46, 1170–1179. [Google Scholar] [CrossRef]
- Jitmuang, A.; Puttinad, S.; Hemvimol, S.; Pansasiri, S.; Horthongkham, N. A multiplex pneumonia panel for diagnosis of hospital-acquired and ventilator-associated pneumonia in the era of emerging antimicrobial resistance. Front. Cell. Infect. Microbiol. 2022, 12, 977320. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.; Guo, Y.; Yang, Y.; Zheng, Y.; Wu, S.; Jiang, X.; Zhu, D.; Wang, F. Resistance reported from China antimicrobial surveillance network (CHINET) in 2018. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 2275–2281. [Google Scholar] [CrossRef] [PubMed]
- Georgakopoulou, V.E.; Gkoufa, A.; Aravantinou-Fatorou, A.; Trakas, I.; Trakas, N.; Faropoulos, K.; Paterakis, K.; Fotakopoulos, G. Lower respiratory tract infections due to multi-drug resistant pathogens in central nervous system injuries (Review). Biomed. Rep. 2023, 18, 30. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Bassi, G.L.; Luna, C.M.; Martin-Loeches, I.; et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociacion Latinoamericana del Torax (ALAT). Eur. Respir. J. 2017, 50, 1700582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healthcare-Associated Infections Acquired in Intensive Care Units—Annual Epidemiological Report for 2019. Available online: https://www.ecdc.europa.eu/en/publications-data/healthcare-associated-infections-intensive-care-units-2019 (accessed on 25 July 2023).
- Aldali, H.J.; Khan, A.; Alshehri, A.A.; Aldali, J.A.; Meo, S.A.; Hindi, A.; Elsokkary, E.M. Hospital-Acquired Infections Caused by Carbapenem-Resistant Enterobacteriaceae: An Observational Study. Microorganisms 2023, 11, 1595. [Google Scholar] [CrossRef]
- Hu, Y.; Liu, C.; Shen, Z.; Zhou, H.; Cao, J.; Chen, S.; Lv, H.; Zhou, M.; Wang, Q.; Sun, L.; et al. Prevalence, risk factors and molecular epidemiology of carbapenem-resistant Klebsiella pneumoniae in patients from Zhejiang, China, 2008–2018. Emerg. Microbes Infect. 2020, 9, 1771–1779. [Google Scholar] [CrossRef]
- Antimicrobial Resistance in the EU/EEA (EARS-Net)—Annual Epidemio-Logical Report for 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2021 (accessed on 25 July 2023).
- Coque, T.M.; Canton, R.; Perez-Cobas, A.E.; Fernández-De-Bobadilla, M.D.; Baquero, F. Antimicrobial Resistance in the Global Health Network: Known Unknowns and Challenges for Efficient Responses in the 21st Century. Microorganisms 2023, 11, 1050. [Google Scholar] [CrossRef]
- Collineau, L.; Bourely, C.; Rousset, L.; Berger-Carbonne, A.; Ploy, M.-C.; Pulcini, C.; Colomb-Cotinat, M. Towards One Health surveillance of antibiotic resistance: Characterisation and mapping of existing programmes in humans, animals, food and the environment in France, 2021. Eurosurveillance 2023, 28, 2200804. [Google Scholar] [CrossRef]
- Iera, J.; Seghieri, C.; Tavoschi, L.; Isonne, C.; Baccolini, V.; Petrone, D.; Agodi, A.; Barchitta, M.; Arnoldo, L.; Creti, R.; et al. Early Warning Systems for Emerging Profiles of Antimicrobial Resistance in Italy: A National Survey. Int. J. Environ. Res. Public Health 2023, 20, 5623. [Google Scholar] [CrossRef]
- Shadan, A.; Pathak, A.; Ma, Y.; Pathania, R.; Singh, R.P. Deciphering the virulence factors, regulation, and immune response to Acinetobacter baumannii infection. Front. Cell. Infect. Microbiol. 2023, 13, 1053968. [Google Scholar] [CrossRef]
- Zeng, M.; Xia, J.; Zong, Z.; Shi, Y.; Ni, Y.; Hu, F.; Chen, Y.; Zhuo, C.; Hu, B.; Lv, X.; et al. Guidelines for the diagnosis, treatment, prevention and control of infections caused by carbapenem-resistant gram-negative bacilli. J. Microbiol. Immunol. Infect. 2023; ahead of print. [Google Scholar] [CrossRef]
- Lee, Y.L.; Ko, W.C.; Hsueh, P.R. Geographic patterns of Acinetobacter baumannii and carbapenem resistance in the Asia-Pacific Region: Results from the Antimicrobial Testing Leadership and Surveillance (ATLAS) program, 2012–2019. Int. J. Infect. Dis. 2023, 127, 48–55. [Google Scholar] [CrossRef]
- Zhou, H.; Sun, X.; Lyu, S.; Yu, X.; Li, R.; Wang, H.; An, Z. Evaluation of Tigecycline Utilization and Trends in Antibacterial Resistance from 2018 to 2021 in a Comprehensive Teaching Hospital in China. Infect. Drug Resist. 2023, 16, 879–889. [Google Scholar] [CrossRef] [PubMed]
- Hafiz, T.A.; Alghamdi, S.S.; Mubaraki, M.A.; Alghamdi, S.S.; Alothaybi, A.; Aldawood, E.; Alotaibi, F. A two-year retrospective study of multidrug-resistant Acinetobacter baumannii respiratory infections in critically Ill patients: Clinical and microbiological findings. J. Infect. Public Health 2023, 16, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Losito, A.R.; Raffaelli, F.; Del, G.P.; Tumbarello, M. New Drugs for the Treatment of Pseudomonas aeruginosa Infections with Limited Treatment Options: A Narrative Review. Antibiotics 2022, 11, 579. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Xiao, W.; Zhou, C.; Pu, Q.; Deng, X.; Lan, L.; Liang, H.; Song, X.; Wu, M. Pseudomonas aeruginosa: Pathogenesis, virulence factors, antibiotic resistance, interaction with host, technology advances and emerging therapeutics. Signal Transduct. Target. Ther. 2022, 7, 199. [Google Scholar] [CrossRef]
- Hu, Y.-Y.; Cao, J.-M.; Yang, Q.; Chen, S.; Lv, H.-Y.; Zhou, H.-W.; Wu, Z.; Zhang, R. Risk Factors for Carbapenem-Resistant Pseudomonas aeruginosa, Zhejiang Province, China. Emerg. Infect. Dis. 2019, 25, 1861–1867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popovich, K.J.; Aureden, K.; Ham, D.C.; Harris, A.D.; Hessels, A.J.; Huang, S.S.; Maragakis, L.L.; Milstone, A.M.; Moody, J.; Yokoe, D.; et al. SHEA/IDSA/APIC Practice Recommendation: Strategies to prevent methicillin-resistant Staphylococcus aureus transmission and infection in acute-care hospitals: 2022 Update. Infect. Control Hosp. Epidemiol. 2023, 44, 1039–1067. [Google Scholar] [CrossRef]
- Wang, H. Current and Future Landscape of the Antimicrobial Resistance of Nosocomial Infections in China. China CDC Wkly. 2022, 4, 1101–1104. [Google Scholar] [CrossRef]
- Yao, Z.; Wu, Y.; Xu, H.; Lei, Y.; Long, W.; Li, M.; Gu, Y.; Jiang, Z.; Cao, C. Prevalence and clinical characteristics of methicillin-resistant Staphylococcus aureus infections among dermatology inpatients: A 7-year retrospective study at a tertiary care center in southwest China. Front. Public Health 2023, 11, 1124930. [Google Scholar] [CrossRef]
- Hu, F.; Yuan, L.; Yang, Y.; Xu, Y.; Huang, Y.; Hu, Y.; Ai, X.; Zhuo, C.; Su, D.; Shan, B.; et al. A multicenter investigation of 2,773 cases of bloodstream infections based on China antimicrobial surveillance network (CHINET). Front. Cell. Infect. Microbiol. 2022, 12, 1075185. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Zhang, R.; Hu, Y.; Zhou, H.; Cao, J.; Lv, H.; Chen, S.; Ding, S.; Chen, G. Epidemiology and risk factors of methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci infections in Zhejiang China from 2015 to 2017. Antimicrob. Resist. Infect. Control 2019, 8, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Total | TBI | ICH | p |
|---|---|---|---|---|
| Cases | 739 | 479 | 260 | - |
| Age | 50.4 ± 13.3 | 48.9 ± 13.6 | 53.1 ± 12.4 | <0.0001 |
| Sex, male:female | 592:147 | 390:89 | 202:58 | 0.2 |
| GCS | 8.2 ± 3.3 | 8.3 ± 3.3 | 8.2 ± 3.3 | 0.7 |
| Interval days | 6.8 ± 4.4 | 6.9 ± 4.3 | 6.6 ± 4.7 | 0.3 |
| Days in hospital | 22.8 ± 12.2 | 22.3 ± 10.8 | 23.8 ± 14.4 | 0.1 |
| Death | 27 (3.6%) | 17 (3.5%) | 10 (3.8%) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, W.; Yao, H.; Xi, C.; Ye, X.; Chen, Q.; Zhang, J.; Yu, J.; Hu, J. Prevalence and Clinical Characteristics of Bacterial Pneumonia in Neurosurgical Emergency Center Patients: A Retrospective Study Spanning 13 Years at a Tertiary Center. Microorganisms 2023, 11, 1992. https://doi.org/10.3390/microorganisms11081992
Yang W, Yao H, Xi C, Ye X, Chen Q, Zhang J, Yu J, Hu J. Prevalence and Clinical Characteristics of Bacterial Pneumonia in Neurosurgical Emergency Center Patients: A Retrospective Study Spanning 13 Years at a Tertiary Center. Microorganisms. 2023; 11(8):1992. https://doi.org/10.3390/microorganisms11081992
Chicago/Turabian StyleYang, Weijian, Haijun Yao, Caihua Xi, Xiangru Ye, Qifang Chen, Jun Zhang, Jian Yu, and Jin Hu. 2023. "Prevalence and Clinical Characteristics of Bacterial Pneumonia in Neurosurgical Emergency Center Patients: A Retrospective Study Spanning 13 Years at a Tertiary Center" Microorganisms 11, no. 8: 1992. https://doi.org/10.3390/microorganisms11081992