
TGF Beta as a Prognostic Biomarker of COVID-19 Severity in Patients with NAFLD—A Prospective Case–Control Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Laboratory and Clinical Data
2.3. TGF-β1 Measurments
2.4. Statistical Analysis
3. Results
3.1. Baseline Patients’ Characteristics
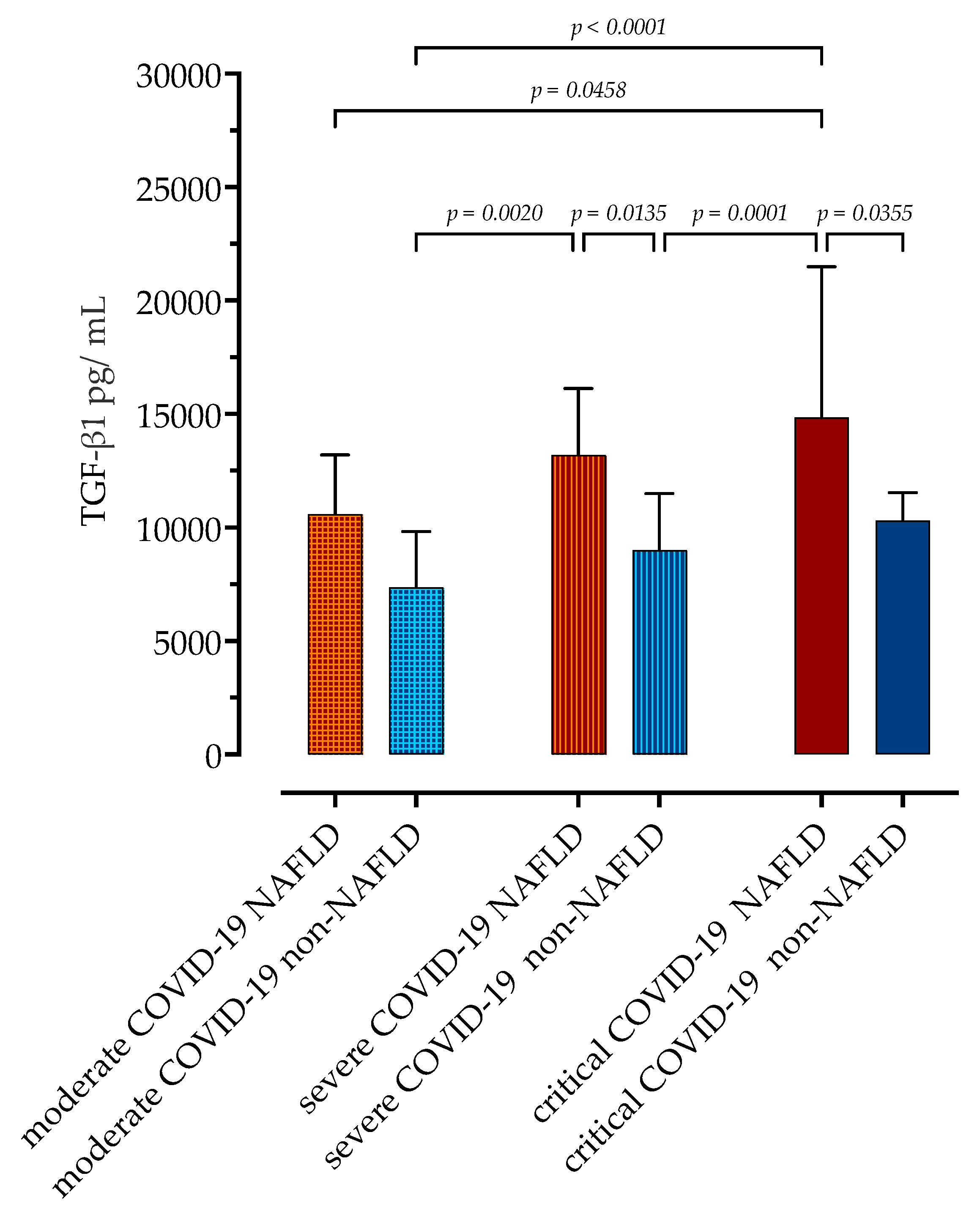
3.2. Association of Serum Concentrations of TGF-β1 with COVID-19 Severity in Patients with and without NAFLD
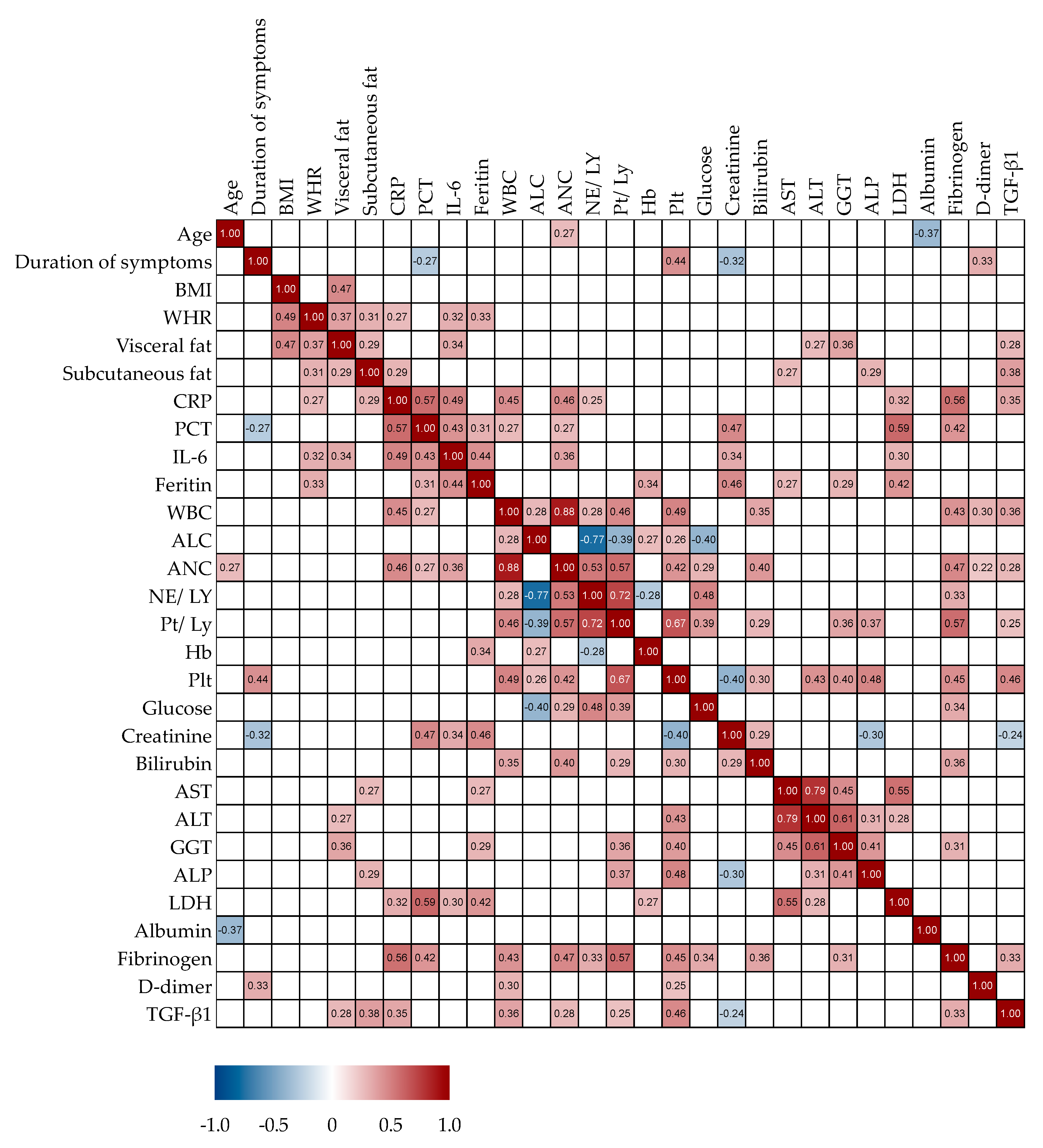
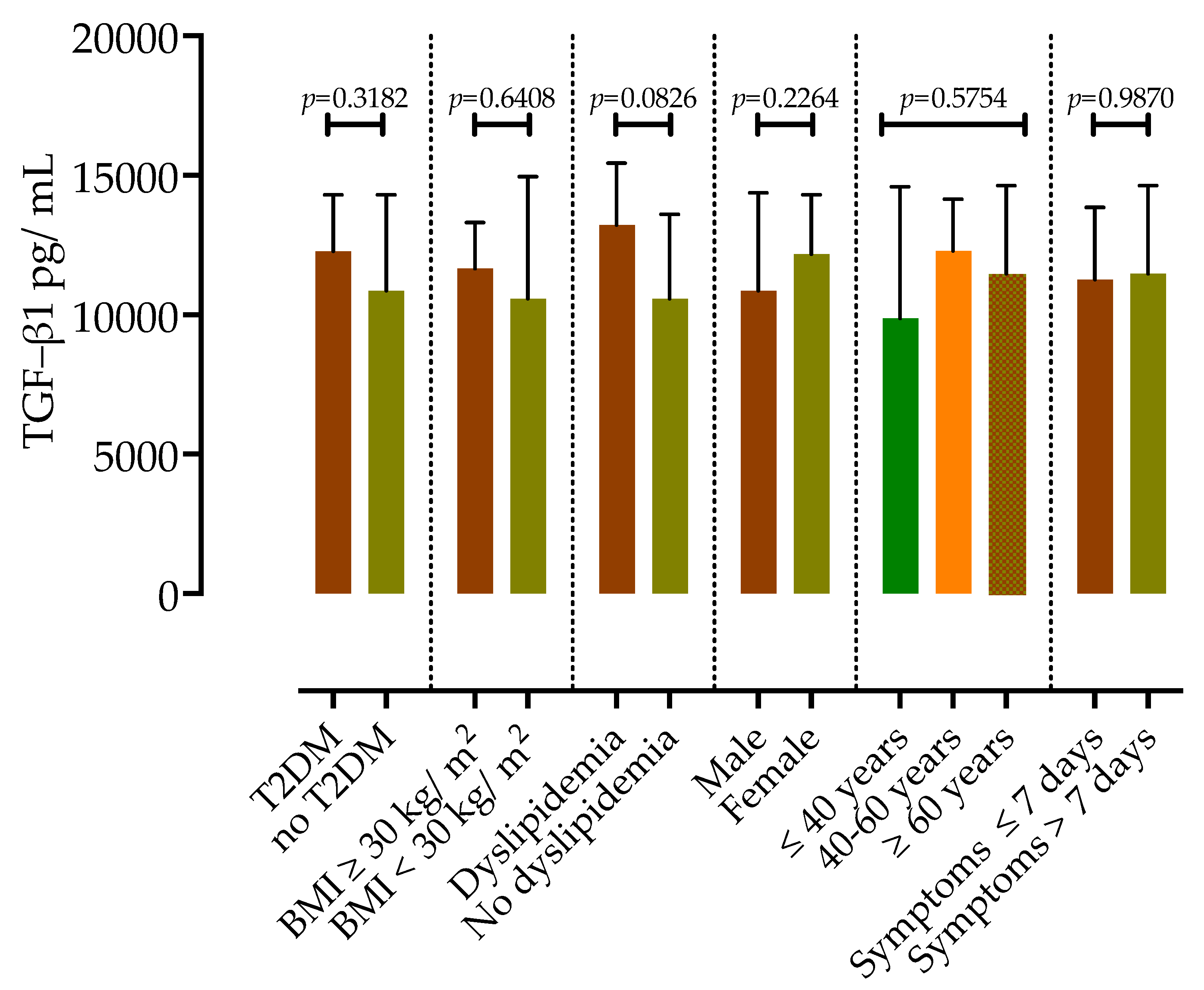
3.3. Correlation Analysis of Serum TGF-β1 Concentrations in Patients with COVID-19
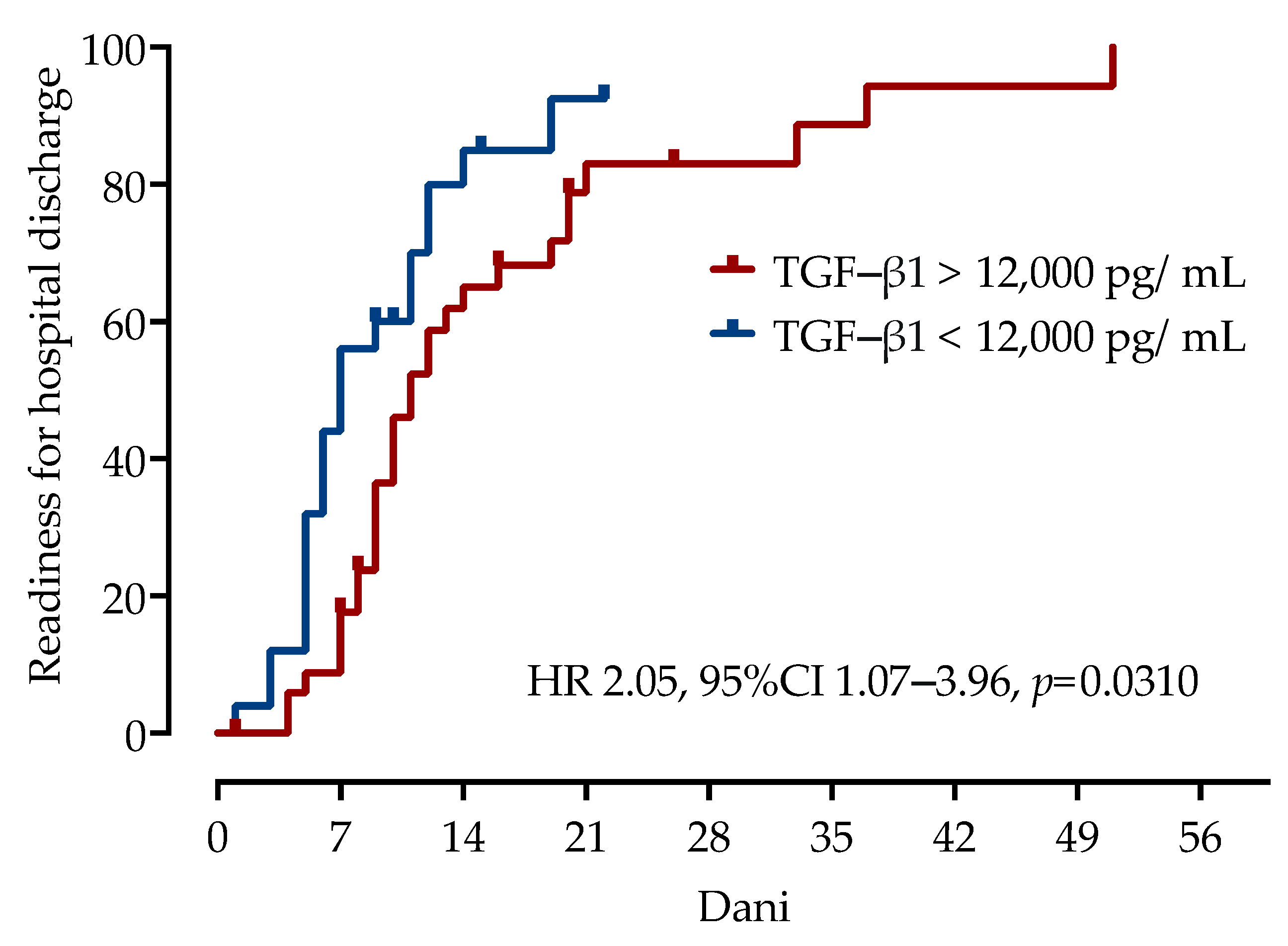
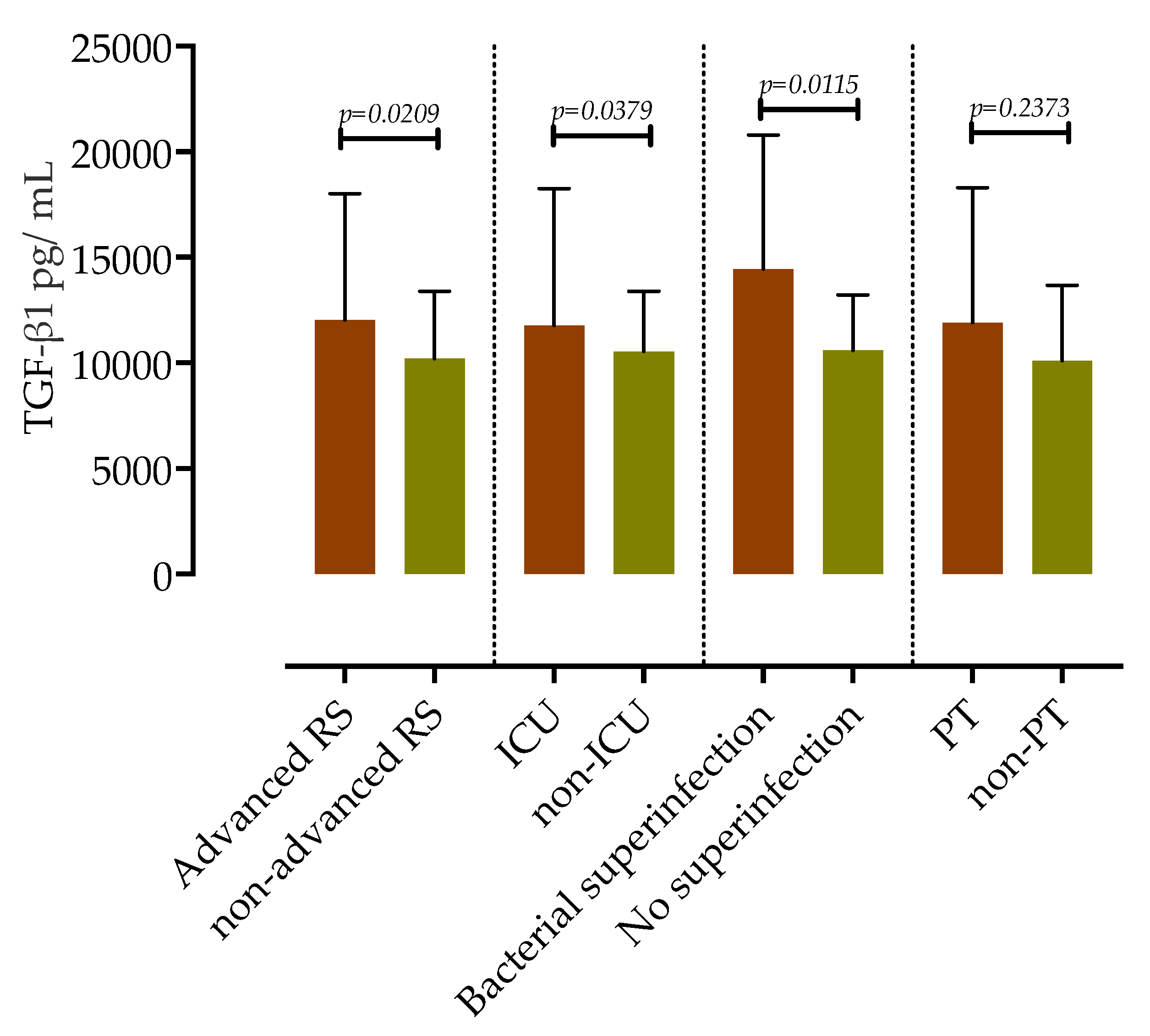
3.4. Association of Serum TGF-β1 Concentrations with COVID-19 Clinical Outcomes and Complications
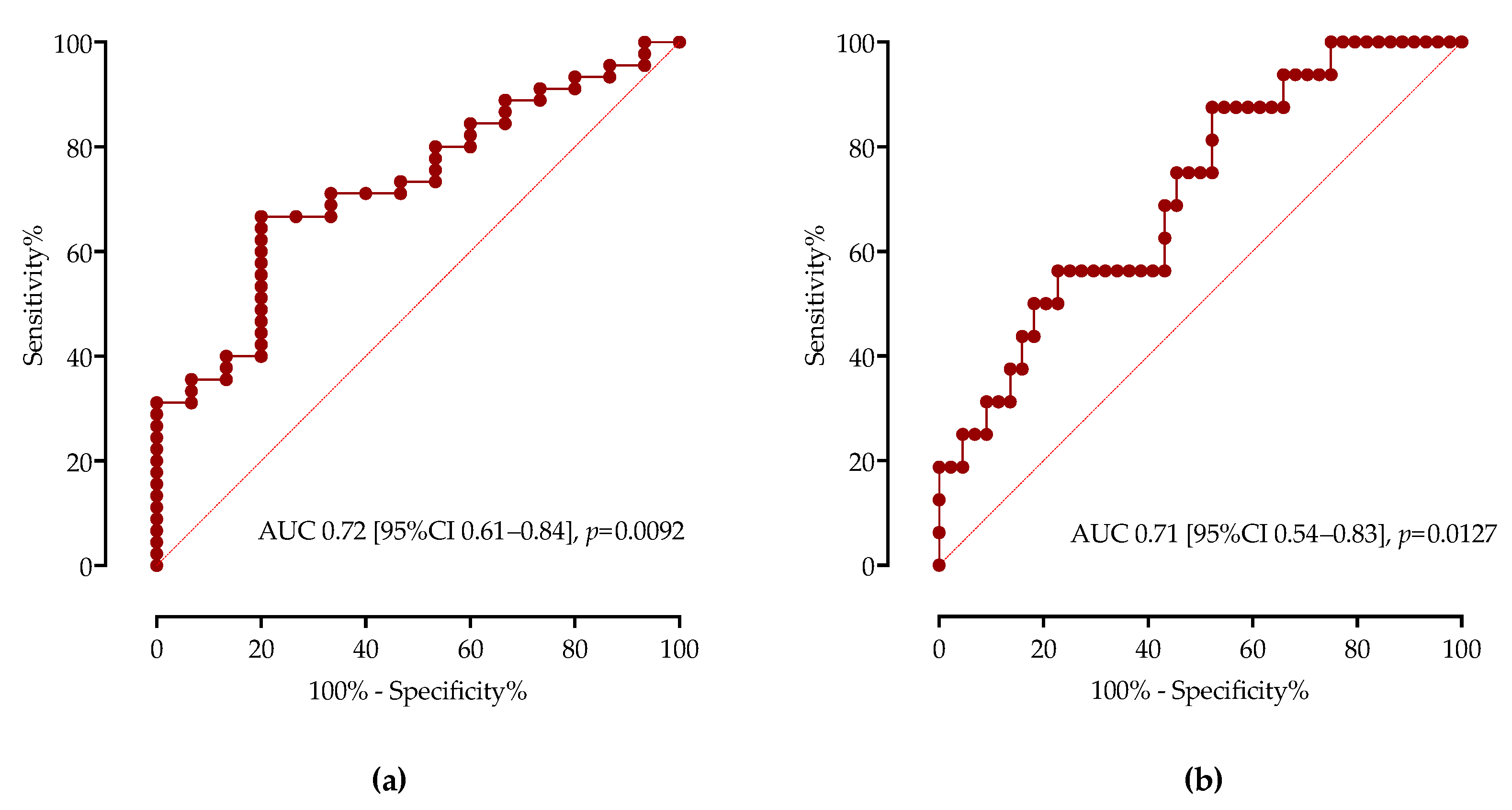
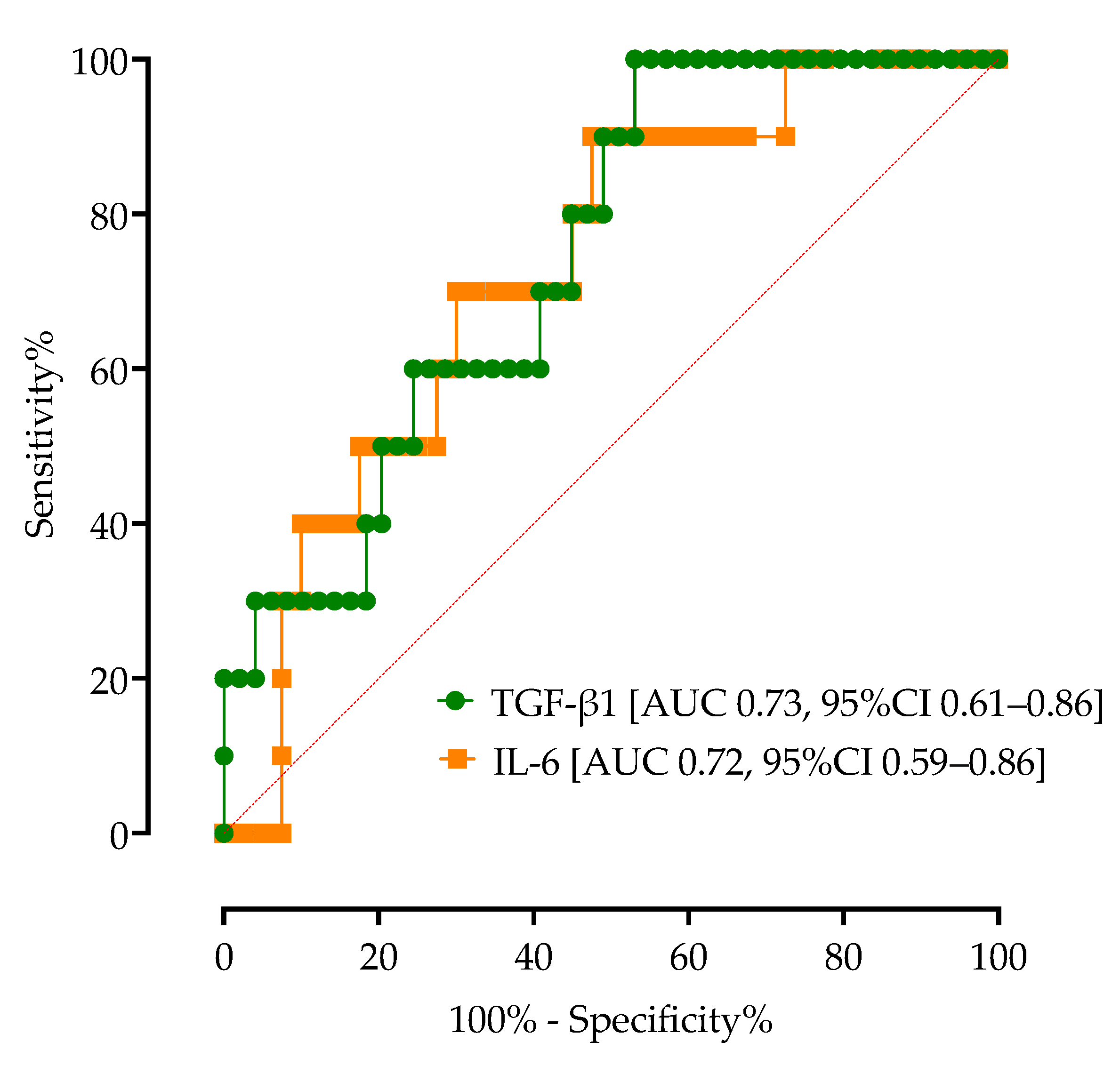
3.5. Association of Serum TGF-β1 Concentrations with COVID-19 Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Foroughi, M.; Maghsoudi, Z.; Khayyatzadeh, S.; Ghiasvand, R.; Askari, G.; Iraj, B. Relationship between non-alcoholic fatty liver disease and inflammation in patients with non-alcoholic fatty liver. Adv. Biomed. Res. 2016, 5, 28. [Google Scholar] [CrossRef]
- Byrne, C.D.; Targher, G. NAFLD: A multisystem disease. J. Hepatol. 2015, 62, S47–S64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomeno, W.; Imajo, K.; Takayanagi, T.; Ebisawa, Y.; Seita, K.; Takimoto, T.; Honda, K.; Kobayashi, T.; Nogami, A.; Kato, T.; et al. Complications of Non-Alcoholic Fatty Liver Disease in Extrahepatic Organs. Diagnostics 2020, 10, 912. [Google Scholar] [CrossRef] [PubMed]
- Krznaric, J.; Vince, A. The Role of Non-Alcoholic Fatty Liver Disease in Infections. Life 2022, 12, 2052. [Google Scholar] [CrossRef] [PubMed]
- Gjurasin, B.; Jelicic, M.; Kutlesa, M.; Papic, N. The Impact of Nonalcoholic Fatty Liver Disease on Severe Community-Acquired Pneumonia Outcomes. Life 2022, 13, 36. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.W.; Jin, H.Y.; Yon, D.K.; Effenberger, M.; Shin, Y.H.; Kim, S.Y.; Yang, J.M.; Kim, M.S.; Koyanagi, A.; Jacob, L.; et al. Non-alcoholic Fatty Liver Disease and COVID-19 Susceptibility and Outcomes: A Korean Nationwide Cohort. J. Korean Med. Sci. 2021, 36, e291. [Google Scholar] [CrossRef]
- Singh, A.; Hussain, S.; Antony, B. Non-alcoholic fatty liver disease and clinical outcomes in patients with COVID-19: A comprehensive systematic review and meta-analysis. Diabetes Metab. Syndr. 2021, 15, 813–822. [Google Scholar] [CrossRef]
- Hegyi, P.J.; Vancsa, S.; Ocskay, K.; Dembrovszky, F.; Kiss, S.; Farkas, N.; Eross, B.; Szakacs, Z.; Hegyi, P.; Par, G. Metabolic Associated Fatty Liver Disease Is Associated With an Increased Risk of Severe COVID-19: A Systematic Review With Meta-Analysis. Front. Med. 2021, 8, 626425. [Google Scholar] [CrossRef]
- Pan, L.; Huang, P.; Xie, X.; Xu, J.; Guo, D.; Jiang, Y. Metabolic associated fatty liver disease increases the severity of COVID-19: A meta-analysis. Dig. Liver Dis. 2021, 53, 153–157. [Google Scholar] [CrossRef]
- Vrsaljko, N.; Samadan, L.; Viskovic, K.; Mehmedovic, A.; Budimir, J.; Vince, A.; Papic, N. Association of Nonalcoholic Fatty Liver Disease with COVID-19 Severity and Pulmonary Thrombosis: CovidFAT, a Prospective, Observational Cohort Study. Open. Forum Infect. Dis. 2022, 9, ofac073. [Google Scholar] [CrossRef]
- Forlano, R.; Mullish, B.H.; Mukherjee, S.K.; Nathwani, R.; Harlow, C.; Crook, P.; Judge, R.; Soubieres, A.; Middleton, P.; Daunt, A.; et al. In-hospital mortality is associated with inflammatory response in NAFLD patients admitted for COVID-19. PLoS ONE 2020, 15, e0240400. [Google Scholar] [CrossRef]
- Mather, M.W.; Jardine, L.; Talks, B.; Gardner, L.; Haniffa, M. Complexity of immune responses in COVID-19. Semin. Immunol. 2021, 55, 101545. [Google Scholar] [CrossRef] [PubMed]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.H.; Beckmann, N.D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.H.; Madduri, D.; Stock, A.; et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef] [PubMed]
- Halim, C.; Mirza, A.F.; Sari, M.I. The Association between TNF-alpha, IL-6, and Vitamin D Levels and COVID-19 Severity and Mortality: A Systematic Review and Meta-Analysis. Pathogens 2022, 11, 195. [Google Scholar] [CrossRef] [PubMed]
- Papic, N.; Samadan, L.; Vrsaljko, N.; Radmanic, L.; Jelicic, K.; Simicic, P.; Svoboda, P.; Lepej, S.Z.; Vince, A. Distinct Cytokine Profiles in Severe COVID-19 and Non-Alcoholic Fatty Liver Disease. Life 2022, 12, 795. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Zheng, K.I.; Yan, H.D.; Sun, Q.F.; Pan, K.H.; Wang, T.Y.; Chen, Y.P.; Targher, G.; Byrne, C.D.; George, J.; et al. Association and Interaction Between Serum Interleukin-6 Levels and Metabolic Dysfunction-Associated Fatty Liver Disease in Patients With Severe Coronavirus Disease 2019. Front. Endocrinol. 2021, 12, 604100. [Google Scholar] [CrossRef] [PubMed]
- Nolte, M.; Margadant, C. Controlling Immunity and Inflammation through Integrin-Dependent Regulation of TGF-beta. Trends Cell. Biol. 2020, 30, 49–59. [Google Scholar] [CrossRef]
- Mantel, P.Y.; Schmidt-Weber, C.B. Transforming growth factor-beta: Recent advances on its role in immune tolerance. Methods Mol. Biol. 2011, 677, 303–338. [Google Scholar] [CrossRef]
- Fabregat, I.; Moreno-Caceres, J.; Sanchez, A.; Dooley, S.; Dewidar, B.; Giannelli, G.; Ten Dijke, P.; Consortium, I.-L. TGF-beta signalling and liver disease. FEBS J. 2016, 283, 2219–2232. [Google Scholar] [CrossRef] [Green Version]
- Brianso-Llort, L.; Fuertes-Rioja, L.; Ramos-Perez, L.; Salcedo-Allende, M.T.; Hernandez, C.; Simo, R.; Selva, D.M. Transforming growth factor-beta 1: A new factor reducing hepatic SHBG production in liver fibrosis. J. Cell. Physiol. 2022, 237, 3598–3613. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, H.; Umar, M.I.; Imran, S.; Javaid, F.; Syed, S.K.; Riaz, R.; Hassan, W. TGF-beta1 signaling can worsen NAFLD with liver fibrosis backdrop. Exp. Mol. Pathol. 2022, 124, 104733. [Google Scholar] [CrossRef] [PubMed]
- Nair, B.; Nath, L.R. Inevitable role of TGF-beta1 in progression of nonalcoholic fatty liver disease. J. Recept. Signal. Transduct. Res. 2020, 40, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Vaz de Paula, C.B.; Nagashima, S.; Liberalesso, V.; Collete, M.; da Silva, F.P.G.; Oricil, A.G.G.; Barbosa, G.S.; da Silva, G.V.C.; Wiedmer, D.B.; da Silva Deziderio, F.; et al. COVID-19: Immunohistochemical Analysis of TGF-beta Signaling Pathways in Pulmonary Fibrosis. Int. J. Mol. Sci. 2021, 23, 168. [Google Scholar] [CrossRef]
- Wang, E.Y.; Chen, H.; Sun, B.Q.; Wang, H.; Qu, H.Q.; Liu, Y.; Sun, X.Z.; Qu, J.; Fang, Z.F.; Tian, L.; et al. Serum levels of the IgA isotype switch factor TGF-beta1 are elevated in patients with COVID-19. FEBS Lett. 2021, 595, 1819–1824. [Google Scholar] [CrossRef]
- Ferreira-Gomes, M.; Kruglov, A.; Durek, P.; Heinrich, F.; Tizian, C.; Heinz, G.A.; Pascual-Reguant, A.; Du, W.; Mothes, R.; Fan, C.; et al. SARS-CoV-2 in severe COVID-19 induces a TGF-beta-dominated chronic immune response that does not target itself. Nat. Commun. 2021, 12, 1961. [Google Scholar] [CrossRef]
- Karadeniz, H.; Avanoglu Guler, A.; Ozger, H.S.; Yildiz, P.A.; Erbas, G.; Bozdayi, G.; Deveci Bulut, T.; Gulbahar, O.; Yapar, D.; Kucuk, H.; et al. The Prognostic Value of Lung Injury and Fibrosis Markers, KL-6, TGF-beta1, FGF-2 in COVID-19 Patients. Biomark. Insights 2022, 17, 11772719221135443. [Google Scholar] [CrossRef]
- Rubina, K.; Shmakova, A.; Shabanov, A.; Andreev, Y.; Borovkova, N.; Kulabukhov, V.; Evseev, A.; Popugaev, K.; Petrikov, S.; Semina, E. Novel prognostic determinants of COVID-19-related mortality: A pilot study on severely-ill patients in Russia. PLoS ONE 2022, 17, e0264072. [Google Scholar] [CrossRef]
- National Institutes of Health. COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 19 May 2023).
- Ferraioli, G.; Soares Monteiro, L.B. Ultrasound-based techniques for the diagnosis of liver steatosis. World J. Gastroenterol. 2019, 25, 6053–6062. [Google Scholar] [CrossRef]
- Rinella, M.E.; Neuschwander-Tetri, B.A.; Siddiqui, M.S.; Abdelmalek, M.F.; Caldwell, S.; Barb, D.; Kleiner, D.E.; Loomba, R. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 2023, 77, 1797–1835. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver; European Association for the Study of Diabetes; European Association for the Study of Obesity. EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, S.; Aoki, K.; Hasegawa, O.; Numata, K.; Tanaka, K.; Shibata, N.; Shimada, S.; Okamura, A.; Terauchi, Y. Sonographic evaluation of visceral fat by measuring para- and perirenal fat. J. Clin. Ultrasound 2008, 36, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Kubiczkova, L.; Sedlarikova, L.; Hajek, R.; Sevcikova, S. TGF-beta—An excellent servant but a bad master. J. Transl. Med. 2012, 10, 183. [Google Scholar] [CrossRef] [Green Version]
- Lodyga, M.; Hinz, B. TGF-beta1—A truly transforming growth factor in fibrosis and immunity. Semin. Cell. Dev. Biol. 2020, 101, 123–139. [Google Scholar] [CrossRef]
- Rendon-Ramirez, E.J.; Ortiz-Stern, A.; Martinez-Mejia, C.; Salinas-Carmona, M.C.; Rendon, A.; Mata-Tijerina, V.L.; Rosas-Taraco, A.G. TGF-beta Blood Levels Distinguish Between Influenza A (H1N1)pdm09 Virus Sepsis and Sepsis due to Other Forms of Community-Acquired Pneumonia. Viral Immunol. 2015, 28, 248–254. [Google Scholar] [CrossRef] [Green Version]
- Denney, L.; Branchett, W.; Gregory, L.G.; Oliver, R.A.; Lloyd, C.M. Epithelial-derived TGF-beta1 acts as a pro-viral factor in the lung during influenza A infection. Mucosal Immunol. 2018, 11, 523–535. [Google Scholar] [CrossRef] [Green Version]
- Li, N.; Ren, A.; Wang, X.; Fan, X.; Zhao, Y.; Gao, G.F.; Cleary, P.; Wang, B. Influenza viral neuraminidase primes bacterial coinfection through TGF-beta-mediated expression of host cell receptors. Proc. Natl. Acad. Sci. USA 2015, 112, 238–243. [Google Scholar] [CrossRef] [Green Version]
- Beijing Group of National Research Project for SARS. Dynamic changes in blood cytokine levels as clinical indicators in severe acute respiratory syndrome. Chin. Med. J. 2003, 116, 1283–1287. [Google Scholar]
- Lee, C.H.; Chen, R.F.; Liu, J.W.; Yeh, W.T.; Chang, J.C.; Liu, P.M.; Eng, H.L.; Lin, M.C.; Yang, K.D. Altered p38 mitogen-activated protein kinase expression in different leukocytes with increment of immunosuppressive mediators in patients with severe acute respiratory syndrome. J. Immunol. 2004, 172, 7841–7847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghazavi, A.; Ganji, A.; Keshavarzian, N.; Rabiemajd, S.; Mosayebi, G. Cytokine profile and disease severity in patients with COVID-19. Cytokine 2021, 137, 155323. [Google Scholar] [CrossRef] [PubMed]
- Laloglu, E.; Alay, H. Role of transforming growth factor-beta 1 and connective tissue growth factor levels in coronavirus disease-2019-related lung Injury: A prospective, observational, cohort study. Rev. Soc. Bras. Med. Trop. 2022, 55, e06152021. [Google Scholar] [CrossRef]
- Zivancevic-Simonovic, S.; Minic, R.; Cupurdija, V.; Stanojevic-Pirkovic, M.; Milosevic-Djordjevic, O.; Jakovljevic, V.; Mihaljevic, O. Transforming growth factor beta 1 (TGF-beta1) in COVID-19 patients: Relation to platelets and association with the disease outcome. Mol. Cell. Biochem. 2023, 1–11. [Google Scholar] [CrossRef]
- Colarusso, C.; Maglio, A.; Terlizzi, M.; Vitale, C.; Molino, A.; Pinto, A.; Vatrella, A.; Sorrentino, R. Post-COVID-19 Patients Who Develop Lung Fibrotic-like Changes Have Lower Circulating Levels of IFN-beta but Higher Levels of IL-1alpha and TGF-beta. Biomedicines 2021, 9, 1931. [Google Scholar] [CrossRef] [PubMed]
- Lin, E.; Kuo, P.H.; Liu, Y.L.; Yang, A.C.; Tsai, S.J. Transforming growth factor-beta signaling pathway-associated genes SMAD2 and TGFBR2 are implicated in metabolic syndrome in a Taiwanese population. Sci. Rep. 2017, 7, 13589. [Google Scholar] [CrossRef] [Green Version]
- Nasr El-Din, A.; Ata, K.A.E.; Abdel-Gawad, A.R.; Fahmy, N.F. Impact of High Serum Levels of MMP-7, MMP-9, TGF-beta and PDGF Macrophage Activation Markers on Severity of COVID-19 in Obese-Diabetic Patients. Infect. Drug. Resist. 2021, 14, 4015–4025. [Google Scholar] [CrossRef]
- Guo, S.A.; Bowyer, G.S.; Ferdinand, J.R.; Maes, M.; Tuong, Z.K.; Gillman, E.; Liao, M.; Lindeboom, R.G.H.; Yoshida, M.; Worlock, K.; et al. Obesity Is Associated with Attenuated Tissue Immunity in COVID-19. Am. J. Respir. Crit. Care Med. 2023, 207, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Witkowski, M.; Tizian, C.; Ferreira-Gomes, M.; Niemeyer, D.; Jones, T.C.; Heinrich, F.; Frischbutter, S.; Angermair, S.; Hohnstein, T.; Mattiola, I.; et al. Untimely TGFbeta responses in COVID-19 limit antiviral functions of NK cells. Nature 2021, 600, 295–301. [Google Scholar] [CrossRef]
- Peters, D.M.; Vadasz, I.; Wujak, L.; Wygrecka, M.; Olschewski, A.; Becker, C.; Herold, S.; Papp, R.; Mayer, K.; Rummel, S.; et al. TGF-beta directs trafficking of the epithelial sodium channel ENaC which has implications for ion and fluid transport in acute lung injury. Proc. Natl. Acad. Sci. USA 2014, 111, E374–E383. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Duan, Q.; Wu, R.; Harris, E.N.; Su, Q. Pathophysiological communication between hepatocytes and non-parenchymal cells in liver injury from NAFLD to liver fibrosis. Adv. Drug. Deliv. Rev. 2021, 176, 113869. [Google Scholar] [CrossRef]
- Nasiri-Ansari, N.; Androutsakos, T.; Flessa, C.M.; Kyrou, I.; Siasos, G.; Randeva, H.S.; Kassi, E.; Papavassiliou, A.G. Endothelial Cell Dysfunction and Nonalcoholic Fatty Liver Disease (NAFLD): A Concise Review. Cells 2022, 11, 2511. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NAFLD (n = 30) | Non-NAFLD (n = 30) | p-Value a | |
|---|---|---|---|
| Age, median (IQR) | 56 (36–65) | 64 (36–70) | 0.297 |
| Male, No. (%) | 16 (53.33%) | 20 (66.67%) | 0.429 |
| Comorbidities | |||
| Diabetes Mellitus | 6 (20.00%) | 6 (20.00%) | 1.000 |
| Arterial Hypertension | 16 (53.33%) | 17 (56.67%) | 1.000 |
| Obesity | 16 (53.33%) | 10 (33.33%) | 0.192 |
| Gastritis/GERD | 3 (10.00%) | 1 (3.33%) | 0.612 |
| Cardiovascular disease | 3 (10.00%) | 2 (6.67%) | 1.000 |
| Clinical findings on admission | |||
| Peripheral oxygen saturation (SpO2), % | 93 (88–96) | 93 (90–95) | 0.828 |
| Respiratory rate,/min | 24 (22–31) | 24 (18–28) | 0.141 |
| Heart rate,/min | 93 (83–103) | 95 (81–100) | 0.828 |
| Body temperature, °C | 38 (37–39) | 38 (37–38) | 0.076 |
| Anthropometric and ultrasound measurements | |||
| BMI, kg/m2 | 31 (26–34) | 28 (24–31) | 0.015 |
| Waist-hip ratio (WHR) | 1.0 (0.96–1.1) | 0.98 (0.83–1.1) | 0.030 |
| Subcutaneous fat, mm | 24 (17–28) | 18 (13–21) | 0.005 |
| Visceral fat, mm | 12 (8–14) | 6.5 (5–8) | <0.0001 |
| NAFLD (n = 30) | Non-NAFLD (n = 30) | p-Value a | |
|---|---|---|---|
| Leukocyte count, 109/L, median (IQR) b | 7.4 (5.6–10) | 5.7 (4.8–7.1) | 0.028 |
| Lymphocyte count, 109/L | 0.73 (0.51–1.1) | 0.63 (0.44–0.81) | 0.248 |
| Neutrophil count, 109/L | 5.9 (4.1–8.8) | 4.6 (4.1–5.9) | 0.097 |
| Neutrophils/lymphocytes ratio | 8 (4–14) | 7 (5.3–10) | 0.889 |
| Hemoglobin, g/L | 138 (129–146) | 134 (124–148) | 0.447 |
| Platelet count, 109/L | 219 (160–270) | 176 (121–236) | 0.011 |
| Platelets/lymphocytes ratio (PTR) | 16 (13–37) | 15 (10–22) | 0.197 |
| Urea, mmol/L | 5.7 (4.4–7.2) | 5.7 (4.3–9.5) | 0.689 |
| Creatinine, μmol/L | 72 (63–94) | 79 (63–99) | 0.511 |
| AST, IU/L | 47 (35–79) | 46 (35–85) | 0.738 |
| ALT, IU/L | 39 (27–86) | 38 (21–58) | 0.154 |
| GGT, IU/L | 61 (42–131) | 38 (24–62) | 0.018 |
| ALP, IU/L | 59 (52–86) | 55 (44–76) | 0.293 |
| LDH, IU/L | 401 (275–560) | 415 (283–510) | 0.933 |
| Bilirubin, μmol/L | 12 (8.8–14) | 11 (9–14) | 0.997 |
| Prothrombin time | 1.2 (1.1–1.3) | 1.2 (1–1.3) | 0.892 |
| Fibrinogen, g/L | 6.0 (5.4–6.9) | 5.7 (5.1–6.6) | 0.425 |
| D-dimers, mg/L | 1.1 (0.54–2) | 0.93 (0.58–1.2) | 0.425 |
| CRP, mg/L | 140 (71–221) | 90 (39–139) | 0.032 |
| Procalcitonin μg/L | 0.18 (0.077–0.41) | 0.14 (0.069–0.32) | 0.539 |
| IL-6, pg/L | 87 (15–150) | 41 (14–62) | 0.035 |
| Ferritin, μg/L | 1111 (706–1797) | 711 (505–1564) | 0.207 |
| APRI score | 0.72 (0.51–1.3) | 0.60 (0.34–0.91) | 0.119 |
| FIB-4 score | 3.3 (1.7–4.4) | 2.0 (1.2–2.7) | 0.009 |
| Deceased (n = 10) | Survived (n = 50) | p-Value a | |
|---|---|---|---|
| TGF-β1, pg/mL, median (IQR) b | 13,352 (11,090–19,250) | 10,572 (8731–20,794) | 0.0192 |
| IL-6, pg/L | 95 (49–164) | 41 (6.9–90) | 0.0262 |
| Ferritin, μg/L | 948 (679–1797) | 743 (553–1591) | 0.6015 |
| CRP, mg/L | 129 (80–162) | 103 (56–188) | 0.7324 |
| LDH, IU/L | 436 (330–614) | 399 (273–512) | 0.3604 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Susak, F.; Vrsaljko, N.; Vince, A.; Papic, N. TGF Beta as a Prognostic Biomarker of COVID-19 Severity in Patients with NAFLD—A Prospective Case–Control Study. Microorganisms 2023, 11, 1571. https://doi.org/10.3390/microorganisms11061571
Susak F, Vrsaljko N, Vince A, Papic N. TGF Beta as a Prognostic Biomarker of COVID-19 Severity in Patients with NAFLD—A Prospective Case–Control Study. Microorganisms. 2023; 11(6):1571. https://doi.org/10.3390/microorganisms11061571
Chicago/Turabian StyleSusak, Frano, Nina Vrsaljko, Adriana Vince, and Neven Papic. 2023. "TGF Beta as a Prognostic Biomarker of COVID-19 Severity in Patients with NAFLD—A Prospective Case–Control Study" Microorganisms 11, no. 6: 1571. https://doi.org/10.3390/microorganisms11061571