
Antimicrobial Resistance Is Prevalent in E. coli and Other Enterobacterales Isolated from Public and Private Drinking Water Supplies in the Republic of Ireland

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
{kind=link}
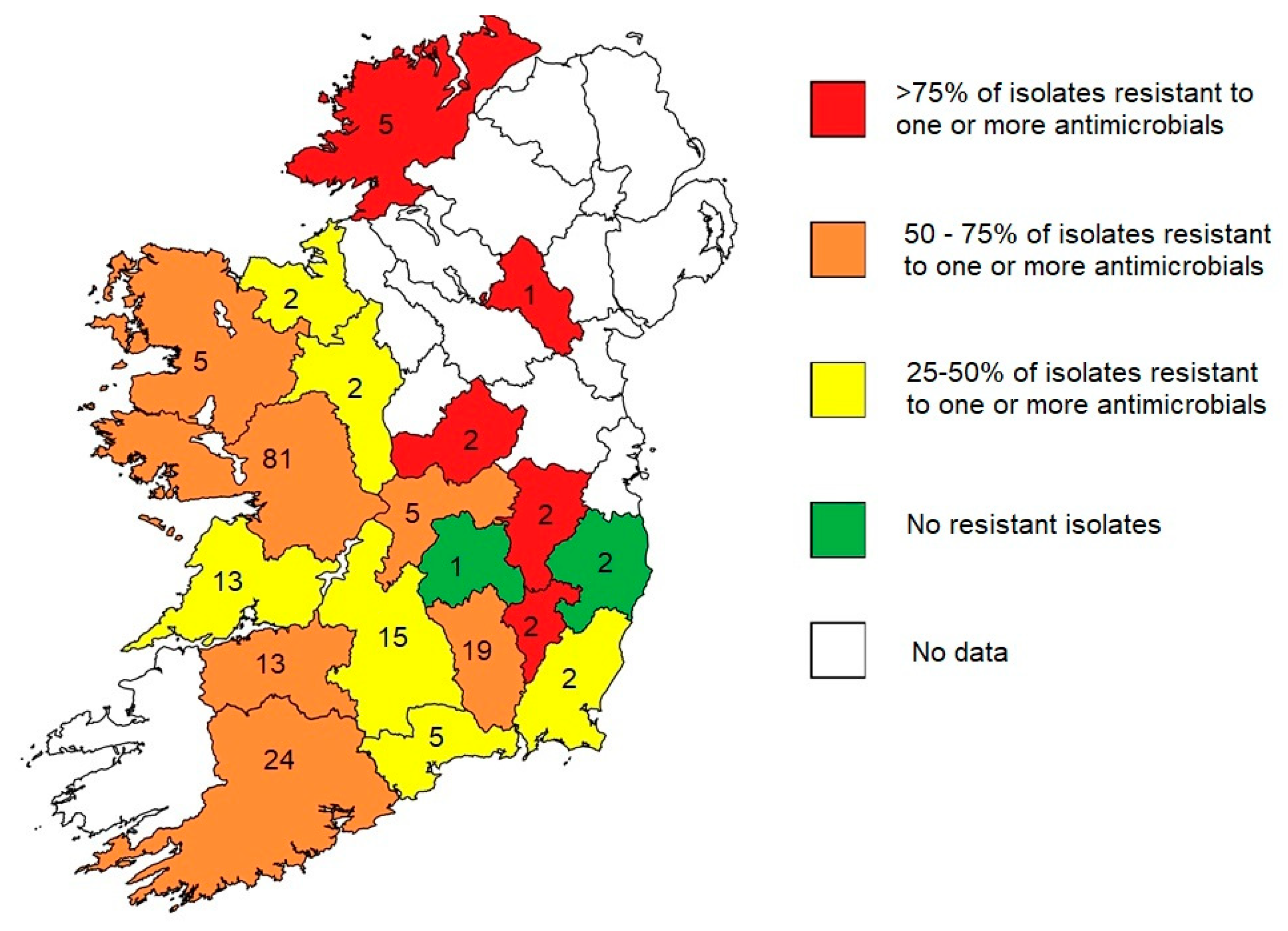
| GWS | Private | Public | Total | AMX | AMC | ATM | CHL | CIP | GEN | CRO | SXT | No Resistance | Resistance (Any) | Total | % Resistance (Any) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Carlow | 2 | 2 | 2 | 2 | 2 | 2 | 100% | |||||||||
| Kildare | 2 | 2 | 2 | 1 | 2 | 2 | 100% | |||||||||
| Monaghan | 1 | 1 | 1 | 1 | 1 | 100% | ||||||||||
| Westmeath | 2 | 2 | 2 | 1 | 1 | 2 | 2 | 100% | ||||||||
| Donegal | 5 | 5 | 4 | 1 | 1 | 1 | 4 | 5 | 80% | |||||||
| Kilkenny | 4 | 15 | 19 | 12 | 4 | 1 | 2 | 7 | 12 | 19 | 63% | |||||
| Cork | 24 | 24 | 15 | 7 | 1 | 1 | 1 | 1 | 1 | 9 | 15 | 24 | 63% | |||
| Limerick | 12 | 1 | 13 | 8 | 2 | 2 | 1 | 5 | 8 | 13 | 62% | |||||
| Mayo | 5 | 5 | 3 | 2 | 3 | 5 | 60% | |||||||||
| Offaly | 5 | 5 | 3 | 1 | 1 | 2 | 3 | 5 | 60% | |||||||
| Galway | 1 | 80 | 81 | 44 | 21 | 2 | 1 | 1 | 3 | 3 | 37 | 44 | 81 | 54% | ||
| Roscommon | 1 | 1 | 2 | 1 | 1 | 1 | 1 | 2 | 50% | |||||||
| Sligo | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 50% | |||||||
| Wexford | 2 | 2 | 1 | 1 | 1 | 1 | 2 | 50% | ||||||||
| Tipperary | 1 | 14 | 15 | 7 | 4 | 1 | 2 | 8 | 7 | 15 | 47% | |||||
| Waterford | 5 | 5 | 1 | 1 | 3 | 2 | 5 | 40% | ||||||||
| Clare | 13 | 13 | 4 | 1 | 1 | 9 | 4 | 13 | 31% | |||||||
| Laois | 1 | 1 | 1 | 0 | 1 | 0% | ||||||||||
| Wicklow | 2 | 2 | 2 | 0 | 2 | 0% | ||||||||||
| Total | 2 | 182 | 17 | 201 | 111 | 43 | 4 | 4 | 2 | 2 | 17 | 6 | 89 | 112 | 201 | 56% |
References
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Antimicrobial Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 13 April 2022).
- World Health Organisation. Global Antimicrobial Resistance and Use Surveillance System (GLASS). Available online: https://www.who.int/initiatives/glass (accessed on 18 March 2023).
- European Medicines Agency. Sales of Veterinary Antimicrobial Agents in 31 European Countries in 2021. Available online: https://www.ema.europa.eu/en/documents/report/sales-veterinary-antimicrobial-agents-31-european-countries-2021-trends-2010-2021-twelfth-esvac_en.pdf (accessed on 20 March 2023).
- Eurostat. Agricultural Production—Livestock and Meat. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Agricultural_production_-_livestock_and_meat#Meat_production (accessed on 20 March 2023).
- Niegowska, M.; Sanseverino, I.; Navarro, A.; Lettieri, T. Knowledge gaps in the assessment of antimicrobial resistance in surface waters. FEMS Microbiol. Ecol. 2021, 97, fiab140. [Google Scholar] [CrossRef]
- Gaze, W.; Depledge, M. Chapter 1. Antimicrobial Resistance: Investigating the Environmental Dimension—Frontiers 2017: Emerging Issues of Environmental Concern. Available online: https://wedocs.unep.org/20.500.11822/22263 (accessed on 13 April 2022).
- Chique, C.; Cullinan, J.; Hooban, B.; Morris, D. Mapping and Analysing Potential Sources and Transmission Routes of Antimicrobial Resistant Organisms in the Environment using Geographic Information Systems-An Exploratory Study. Antibiotics 2019, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Berendonk, T.U.; Manaia, C.M.; Merlin, C.; Fatta-Kassinos, D.; Cytryn, E.; Walsh, F.; Bürgmann, H.; Sørum, H.; Norström, M.; Pons, M.N.; et al. Tackling antibiotic resistance: The environmental framework. Nat. Rev. Microbiol. 2015, 13, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.; Jackson, C.R.; Frye, J.G. Freshwater environment as a reservoir of extended-spectrum β-lactamase-producing Enterobacteriaceae. J. Appl. Microbiol. 2023, 134, lxad034. [Google Scholar] [CrossRef] [PubMed]
- Alawi, M.; Torrijos, T.V.; Walsh, F. Plasmid-mediated antimicrobial resistance in drinking water. Environ. Adv. 2022, 8, 100191. [Google Scholar] [CrossRef]
- Department of Health. Ireland’s National Action Plan on Antimicrobial Resistance. Available online: https://assets.gov.ie/204952/75635d71-abf8-4f07-88f7-9465c8da7e6e.pdf (accessed on 13 April 2022).
- Department of Health & Department of Agriculture Food and Marine. Ireland’s second One Health Action Plan on Antimicrobial Resistance 2021–2025 (iNAP2). Available online: https://assets.gov.ie/215951/3a18768d-69dc-40fd-bfe5-ec4b31767d30.pdf (accessed on 22 November 2022).
- World Health Organisation. Technical Brief on Water, Sanitation, Hygiene (WASH) and Wastewater Management to Prevent Infections and Reduce the Spread of Antimicrobial Resistance (AMR). Available online: https://apps.who.int/iris/rest/bitstreams/1279113/retrieve (accessed on 13 April 2022).
- Cahill, N.; O’Connor, L.; Mahon, B.; Varley, Á.; McGrath, E.; Ryan, P.; Cormican, M.; Brehony, C.; Jolley, K.A.; Maiden, M.C.; et al. Hospital effluent: A reservoir for carbapenemase-producing Enterobacterales? Sci. Total Environ. 2019, 672, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Coleman, B.L.; Salvadori, M.I.; McGeer, A.J.; Sibley, K.A.; Neumann, N.F.; Bondy, S.J.; Gutmanis, I.A.; McEwen, S.A.; Lavoie, M.; Strong, D.; et al. The role of drinking water in the transmission of antimicrobial-resistant E. coli. Epidemiol. Infect. 2012, 140, 633–642. [Google Scholar] [CrossRef]
- Coleman, B.L.; Louie, M.; Salvadori, M.I.; McEwen, S.A.; Neumann, N.; Sibley, K.; Irwin, R.J.; Jamieson, F.B.; Daignault, D.; Majury, A.; et al. Contamination of Canadian private drinking water sources with antimicrobial resistant Escherichia coli. Water Res. 2013, 47, 3026–3036. [Google Scholar] [CrossRef]
- Tanner, W.D.; VanDerslice, J.A.; Goel, R.K.; Leecaster, M.K.; Fisher, M.A.; Olstadt, J.; Gurley, C.M.; Morris, A.G.; Seely, K.A.; Chapman, L.; et al. Multi-state study of Enterobacteriaceae harboring extended-spectrum beta-lactamase and carbapenemase genes in U.S. drinking water. Sci. Rep. 2019, 9, 3938. [Google Scholar] [CrossRef]
- Gibbons, J.F.; Boland, F.; Egan, J.; Fanning, S.; Markey, B.K.; Leonard, F.C. Antimicrobial Resistance of Faecal Escherichia coli Isolates from Pig Farms with Different Durations of In-feed Antimicrobial Use. Zoonoses Public Health 2016, 63, 241–250. [Google Scholar] [CrossRef]
- Prendergast, D.M.; O’Doherty, Á.; Burgess, C.M.; Howe, N.; McMahon, F.; Murphy, D.; Leonard, F.; Morris, D.; Harrington, C.; Carty, A.; et al. Critically important antimicrobial resistant Enterobacteriaceae in Irish farm effluent and their removal in integrated constructed wetlands. Sci. Total Environ. 2022, 806, 151269. [Google Scholar] [CrossRef] [PubMed]
- Hooban, B.; Fitzhenry, K.; Cahill, N.; Joyce, A.; O’Connor, L.; Bray, J.E.; Brisse, S.; Passet, V.; Abbas Syed, R.; Cormican, M.; et al. A Point Prevalence Survey of Antibiotic Resistance in the Irish Environment, 2018–2019. Environ. Int. 2021, 152, 106466. [Google Scholar] [CrossRef] [PubMed]
- Hooban, B.; Fitzhenry, K.; O’Connor, L.; Miliotis, G.; Joyce, A.; Chueiri, A.; Farrell, M.L.; DeLappe, N.; Tuohy, A.; Cormican, M.; et al. A Longitudinal Survey of Antibiotic-Resistant Enterobacterales in the Irish Environment, 2019–2020. Sci. Total Environ. 2022, 828, 154488. [Google Scholar] [CrossRef]
- Voigt, A.M.; Ciorba, P.; Döhla, M.; Exner, M.; Felder, C.; Lenz-Plet, F.; Sib, E.; Skutlarek, D.; Schmithausen, R.M.; Faerber, H.A. The investigation of antibiotic residues, antibiotic resistance genes and antibiotic-resistant organisms in a drinking water reservoir system in Germany. Int. J. Hyg. Environ. Health 2020, 224, 113449. [Google Scholar] [CrossRef]
- Environmental Protection Agency. Types of Drinking Water Supplies. Available online: https://www.epa.ie/our-services/compliance--enforcement/drinking-water/supply-types/ (accessed on 13 April 2022).
- O’Connor, C.; Cormican, M.; Boo, T.W.; McGrath, E.; Slevin, B.; O’Gorman, A.; Commane, M.; Mahony, S.; O’Donovan, E.; Powell, J.; et al. An Irish outbreak of New Delhi metallo-β-lactamase (NDM)-1 carbapenemase-producing Enterobacteriaceae: Increasing but unrecognized prevalence. J. Hosp. Infect. 2016, 94, 351–357. [Google Scholar] [CrossRef]
- O’Connor, C.; Powell, J.; Finnegan, C.; O’Gorman, A.; Barrett, S.; Hopkins, K.L.; Pichon, B.; Hill, R.; Power, L.; Woodford, N.; et al. Incidence, management and outcomes of the first cfr-mediated linezolid-resistant Staphylococcus epidermidis outbreak in a tertiary referral centre in the Republic of Ireland. J. Hosp. Infect. 2015, 90, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Neylon, O.; O’Connell, N.H.; Slevin, B.; Powell, J.; Monahan, R.; Boyle, L.; Whyte, D.; Mannix, M.; McElligott, F.; Kearns, A.M.; et al. Neonatal staphylococcal scalded skin syndrome: Clinical and outbreak containment review. Eur. J. Pediatr. 2010, 169, 1503–1509. [Google Scholar] [CrossRef]
- O’Connor, C.; Philip, R.K.; Kelleher, J.; Powell, J.; O’Gorman, A.; Slevin, B.; Woodford, N.; Turton, J.F.; McGrath, E.; Finnegan, C.; et al. The first occurrence of a CTX-M ESBL-producing Escherichia coli outbreak mediated by mother to neonate transmission in an Irish neonatal intensive care unit. BMC Infect. Dis. 2017, 17, 16. [Google Scholar] [CrossRef]
- O’Connor, C.; Fitzgibbon, M.; Powell, J.; Barron, D.; O’Mahony, J.; Power, L.; O’Connell, N.H.; Dunne, C. A commentary on the role of molecular technology and automation in clinical diagnostics. Bioengineered 2014, 5, 155–160. [Google Scholar] [CrossRef]
- Teoh, T.; McNamara, R.; Powell, J.; O’Connell, N.H.; Dunne, C.P. A retrospective observational study of the impact of 16s and 18s ribosomal RNA PCR on antimicrobial treatment over seven years: A tertiary hospital experience. PLoS ONE 2021, 16, e0258552. [Google Scholar] [CrossRef] [PubMed]
- Mostyn, A.; Lenihan, M.; O’Sullivan, D.; Woods, S.; O’Hara, M.; Powell, J.; Power, L.; O’Connell, N.H.; Dunne, C.P. Assessment of the FilmArray® multiplex PCR system and associated meningitis/encephalitis panel in the diagnostic service of a tertiary hospital. Infect. Prev. Pract. 2020, 2, 100042. [Google Scholar] [CrossRef] [PubMed]
- Powell, J.; Porter, E.; Rafferty, S.; Field, S.; O’Connell, N.H.; Dunne, C.P. Dermatology mycology diagnostics in Ireland: National deficits identified in 2022 that are relevant internationally. Mycoses 2023, 66, 249–257. [Google Scholar] [CrossRef]
- O’Connell, N.H.; Mulchrone, C.; Lynskey, M.; Heffernan, S.C.; O’Brien, B.; Powell, J.; Dunne, C.P. Off-label novel application of diagnostic multiplex molecular platforms for environmental detection of carbapenemase-producing Enterobacterales. J. Hosp. Infect. 2023, 133, 103–104. [Google Scholar] [CrossRef] [PubMed]
- Teoh, T.K.; Powell, J.; Kelly, J.; McDonnell, C.; Whelan, R.; O’Connell, N.H.; Dunne, C.P. Outcomes of point-of-care testing for influenza in the emergency department of a tertiary referral hospital in Ireland. J. Hosp. Infect. 2021, 110, 45–51. [Google Scholar] [CrossRef]
- O’Connor, C.; Philip, R.K.; Powell, J.; Slevin, B.; Quinn, C.; Power, L.; O’Connell, N.H.; Dunne, C.P. Combined education and skin antisepsis intervention for persistently high blood-culture contamination rates in neonatal intensive care. J. Hosp. Infect. 2016, 93, 105–107. [Google Scholar] [CrossRef]
- Dunne, C.P.; Ryan, P.; Connolly, R.; Dunne, S.S.; Kaballo, M.A.; Powell, J.; Woulfe, B.; O’Connell, N.H.; Gupta, R.K. Management of Staphylococcus aureus bacteraemia (SAB) in the oncology patient: Further evidence supports prompt removal of central venous catheters and shorter duration of intravenous antimicrobial therapy. Infect. Prev. Pract. 2020, 2, 100037. [Google Scholar] [CrossRef]
- Truong, W.R.; Hidayat, L.; Bolaris, M.A.; Nguyen, L.; Yamaki, J. The antibiogram: Key considerations for its development and utilization. JAC-Antimicrobal. Resist. 2021, 3, dlab060. [Google Scholar] [CrossRef]
- Andrade, L.; Chique, C.; Hynds, P.; Weatherill, J.; O’Dwyer, J. The antimicrobial resistance profiles of Escherichia coli and Pseudomonas aeruginosa isolated from private groundwater wells in the Republic of Ireland. Environ. Pollut. 2023, 317, 120817. [Google Scholar] [CrossRef]
- O’Dwyer, J.; Hynds, P.; Pot, M.; Adley, C.C.; Ryan, M.P. Evaluation of levels of antibiotic resistance in groundwater-derived E. coli isolates in the Midwest of Ireland and elucidation of potential predictors of resistance. Hydrogeol. J. 2017, 25, 939–951. [Google Scholar] [CrossRef]
- Larson, A.J.; Haver, S.; Hattendorf, J.; Salmon-Mulanovich, G.; Riveros, M.; Verastegui, H.; Mäusezahl, D.; Hartinger, S.M. Household-level risk factors for water contamination and antimicrobial resistance in drinking water among households with children under 5 in rural San Marcos, Cajamarca, Peru. One Health 2023, 16, 100482. [Google Scholar] [CrossRef] [PubMed]
- Odonkor, S.T.; Simpson, S.V.; Morales Medina, W.R.; Fahrenfeld, N.L. Antibiotic-Resistant Bacteria and Resistance Genes in Isolates from Ghanaian Drinking Water Sources. J. Environ. Public Health 2022, 2022, 2850165. [Google Scholar] [CrossRef]
- Papandreou, S.; Pagonopoulou, O.; Vantarakis, A.; Papapetropoulou, M. Multiantibiotic resistance of gram-negative bacteria isolated from drinking water samples in southwest Greece. J. Chemother. 2000, 12, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Rayasam, S.D.G.; Ray, I.; Smith, K.R.; Riley, L.W. Extraintestinal Pathogenic Escherichia coli and Antimicrobial Drug Resistance in a Maharashtrian Drinking Water System. Am. J. Trop. Med. Hyg. 2019, 100, 1101–1104. [Google Scholar] [CrossRef] [PubMed]
- Swedan, S.; Abu Alrub, H. Antimicrobial Resistance, Virulence Factors, and Pathotypes of Escherichia coli Isolated from Drinking Water Sources in Jordan. Pathogens 2019, 8, 86. [Google Scholar] [CrossRef]
- Bijay, S.; Craswell, E. Fertilizers and nitrate pollution of surface and ground water: An increasingly pervasive global problem. SN Appl. Sci. 2021, 3, 518. [Google Scholar] [CrossRef]
- Martin, H.; Manzanilla, E.G.; More, S.J.; O’Neill, L.; Bradford, L.; Carty, C.I.; Collins, Á.B.; McAloon, C.G. Current antimicrobial use in farm animals in the Republic of Ireland. Ir. Vet. J. 2020, 73, 11. [Google Scholar] [CrossRef]
- Health Protection Surveillance Centre. Point Prevalence Survey of Hospital-Acquired Infections & Antimicrobial Use in European Acute Care Hospitals: May 2017. Available online: https://www.hpsc.ie/a-z/microbiologyantimicrobialresistance/infectioncontrolandhai/surveillance/hospitalpointprevalencesurveys/2017/nationalppsreports/PPS%202017%20National%20Report_FINAL_191218.pdf (accessed on 21 April 2023).
- Health Protection and Surveillance Centre. Summary of EARS-Net Data by Pathogen and Year. Available online: https://www.hpsc.ie/az/microbiologyantimicrobialresistance/europeanantimicrobialresistancesurveillancesystemearss/ears-netdataandreports/EARS-Net%20National%20Summary_2016-2020_20220325.pdf (accessed on 13 April 2022).
- Fàbrega, A.; Vila, J. Yersinia enterocolitica: Pathogenesis, virulence and antimicrobial resistance. Enferm. Infecc. Microbiol. Clínica 2012, 30, 24–32. [Google Scholar] [CrossRef]
- Strydom, H.; Wang, J.; Paine, S.; Dyet, K.; Cullen, K.; Wright, J. Evaluating sub-typing methods for pathogenic Yersinia enterocolitica to support outbreak investigations in New Zealand. Epidemiol. Infect. 2019, 147, e186. [Google Scholar] [CrossRef]
- Health Policy Watch. “No Time to Wait”—AMR Could Cause 10 Million Deaths Annually By 2050, Warns UN Report. Available online: https://healthpolicy-watch.news/no-time-to-wait-amr-could-cause-10-million-deaths-annually-by-2050-warns-un-report/ (accessed on 19 March 2023).
- Department of Health. One Health Report on Antimicrobial Use and Antimicrobial Resistance. 2019. Available online: https://www.gov.ie/en/publication/d72f1-joint-action-on-antimicrobial-resistance/ (accessed on 19 March 2023).



| Date ¥ | Total Orgs | E. coli | AMX | CIP | GEN | SXT | ||
|---|---|---|---|---|---|---|---|---|
| our results | Ireland | 2023 | 201 | 53 | 25% | 4% | 4% | 9% |
| Andrade et al. [38] | Ireland | 2023 | 66 | 54 | 13% | 6% | 0% | 2% |
| O’Dwyer et al. [39] | Ireland | 2017 | 42 | 42 | 14% | 5% | ||
| Coleman et al. [17] | Canada | 2012 | U/K | 7063 | 4% * | 0% | 4% | |
| Larson et al. [40] | Peru | 2023 | U/K | 117 | 28% | 18% | ||
| Odonkor et al. [41] | Ghana | 2022 | 83 | 23 | 22% | 0% | 0% | |
| Papandreou et al. [42] | Greece | 2000 | 239 | 10 | 30% | 0% | ||
| Rayasam et al. [43] | India | 2019 | U/K | 104 | 100% | 16% | 2% | 35% |
| Swedan et al. [44] | Jordan | 2019 | U/K | 109 | 94% | 16% | 41% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daly, M.; Powell, J.; O’Connell, N.H.; Murphy, L.; Dunne, C.P. Antimicrobial Resistance Is Prevalent in E. coli and Other Enterobacterales Isolated from Public and Private Drinking Water Supplies in the Republic of Ireland. Microorganisms 2023, 11, 1224. https://doi.org/10.3390/microorganisms11051224
Daly M, Powell J, O’Connell NH, Murphy L, Dunne CP. Antimicrobial Resistance Is Prevalent in E. coli and Other Enterobacterales Isolated from Public and Private Drinking Water Supplies in the Republic of Ireland. Microorganisms. 2023; 11(5):1224. https://doi.org/10.3390/microorganisms11051224
Chicago/Turabian StyleDaly, Maureen, James Powell, Nuala H. O’Connell, Liz Murphy, and Colum P. Dunne. 2023. "Antimicrobial Resistance Is Prevalent in E. coli and Other Enterobacterales Isolated from Public and Private Drinking Water Supplies in the Republic of Ireland" Microorganisms 11, no. 5: 1224. https://doi.org/10.3390/microorganisms11051224