
Osteoarticular Infections in Children: Accurately Distinguishing between MSSA and Kingella kingae
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Microbiological Methods
2.2. Statistical Analysis
3. Results
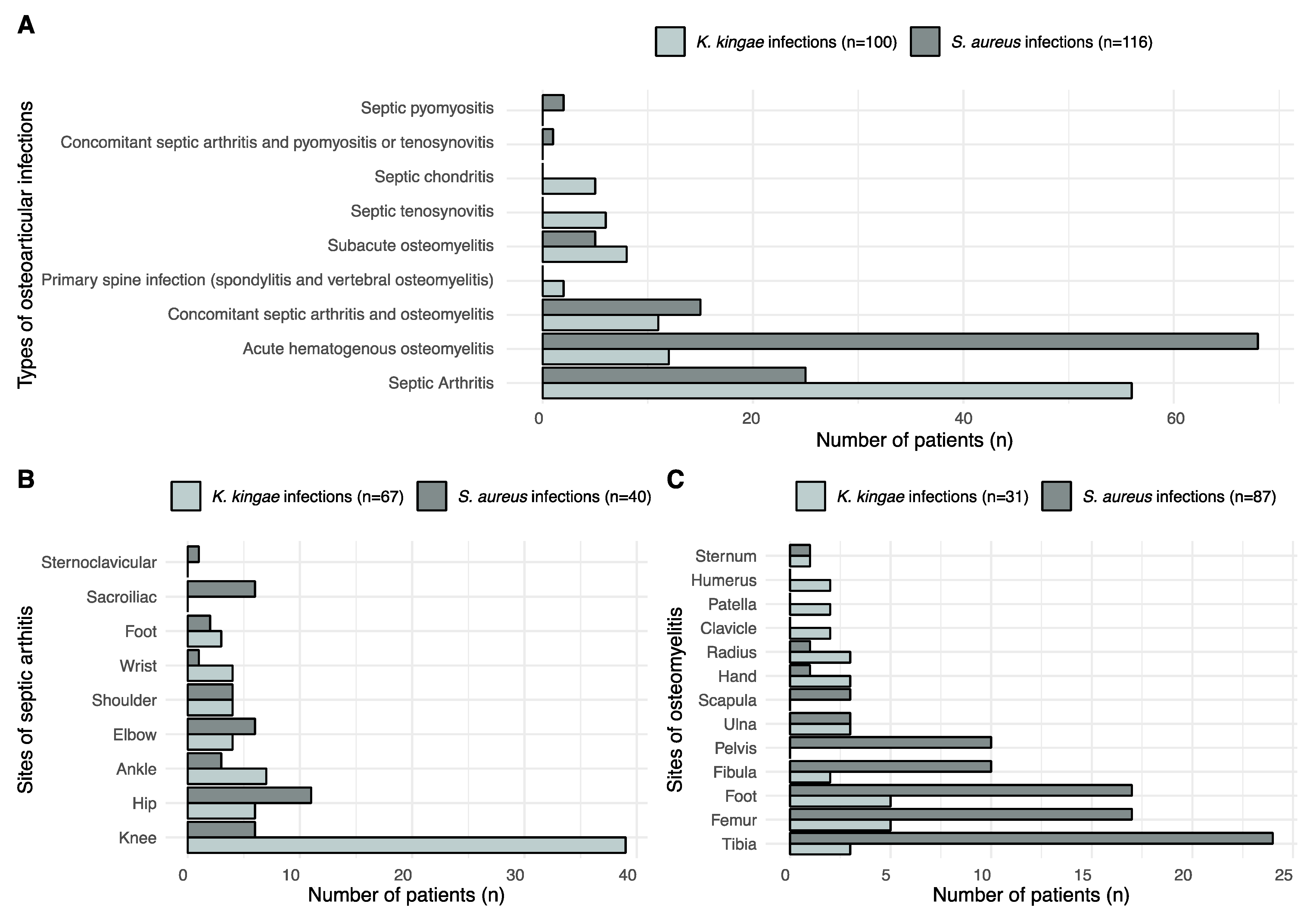
3.1. OAI Due to K. kingae
3.2. OAIs Due to S. aureus
3.3. Comparison of Demographic Characteristics and Clinical and Biological Features between OAIs Caused by MSSA and K. kingae
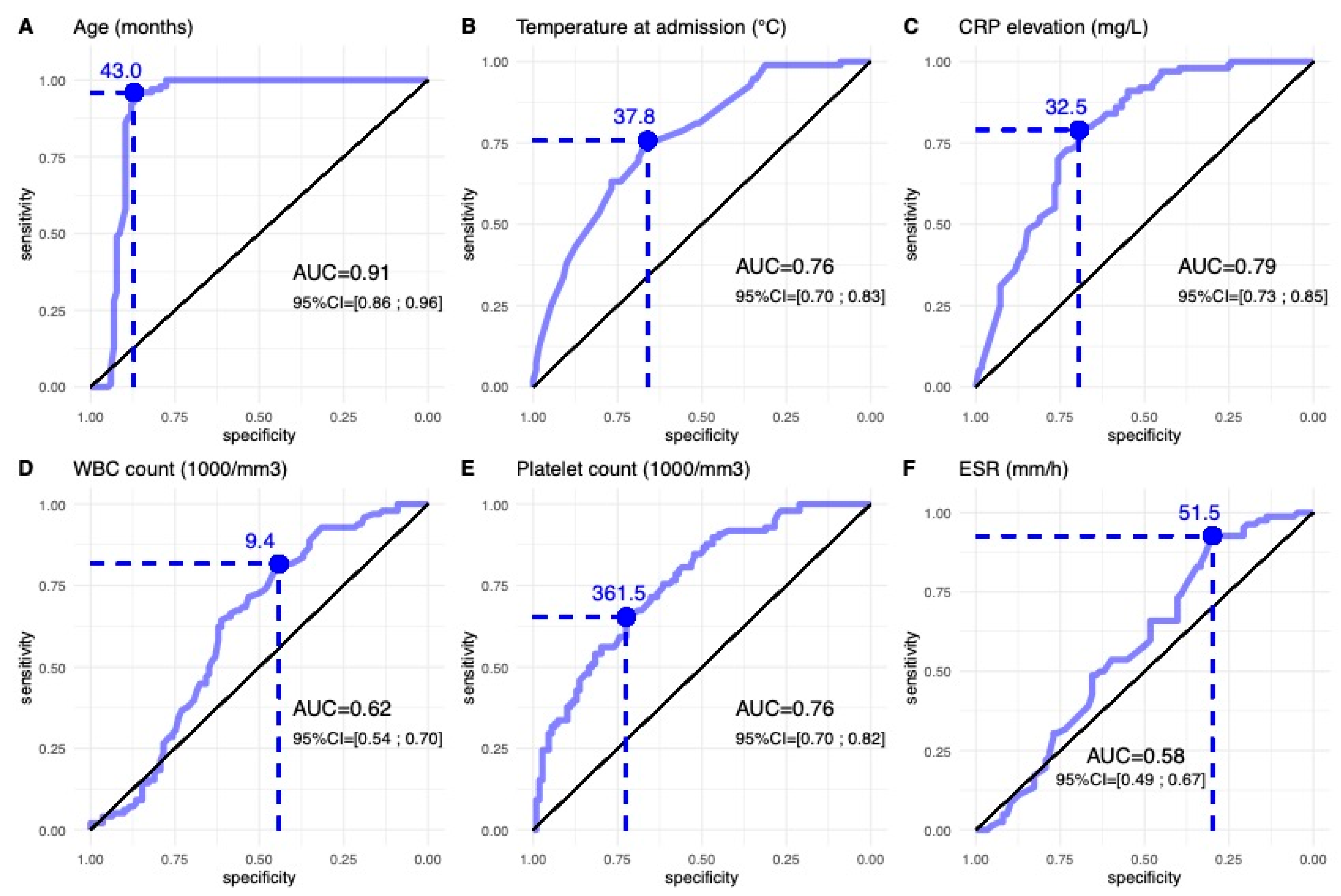
3.4. Prediction of OAIs Caused by K. kingae with Clinical and Biological Features in Children Less Than 4 Years Old
4. Discussion
5. Conclusions
6. Clinical Relevance
Author Contributions
Funding
Conflicts of Interest
References
- Gutierrez, K. Bone and joint infections in children. Pediatr. Clin. N. Am. 2005, 52, 779–794. [Google Scholar] [CrossRef] [PubMed]
- Luhmann, J.D.; Luhmann, S.J. Etiology of septic arthritis in children: An update for the 1990s. Pediatr. Emerg. Care 1999, 15, 40–42. [Google Scholar] [CrossRef] [PubMed]
- Dodwell, E.R. Osteomyelitis and septic arthritis in children: Current concepts. Curr. Opin. Pediatr. 2013, 25, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.-L.; Chang, W.-N.; Chen, Y.-S.; Hsieh, K.-S.; Chen, C.K.-H.; Peng, N.-J.; Wu, K.-S.; Cheng, M.-F. Acute Community-acquired Osteoarticular Infections in Children: High Incidence of Concomitant Bone and Joint Involvement. J. Microbiol. Immunol. Infect. 2010, 43, 332–338. [Google Scholar] [CrossRef] [Green Version]
- Juchler, C.; Spyropoulou, V.; Wagner, N.; Merlini, L.; Dhouib, A.; Manzano, S.; Tabard-Fougère, A.; Samara, E.; Ceroni, D. The Contemporary Bacteriologic Epidemiology of Osteoarticular Infections in Children in Switzerland. J. Pediatr. 2018, 194, 190–196.e1. [Google Scholar] [CrossRef]
- Samara, E.; Spyropoulou, V.; Tabard-Fougère, A.; Merlini, L.; Valaikaite, R.; Dhouib, A.; Manzano, S.; Juchler, C.; Dayeret, R.; Ceroni, D. Kingella kingae and Osteoarticular Infections. Pediatrics 2019, 144, e20191509. [Google Scholar] [CrossRef] [PubMed]
- Stähelin, J.; Goldenberger, D.; Gnehm, H.E.; Altwegg, M. Polymerase Chain Reaction Diagnosis of Kingella kingae Arthritis in a Young Child. Clin. Infect. Dis. 1998, 27, 1328–1329. [Google Scholar] [CrossRef] [Green Version]
- Verdier, I.; Gayet-Ageron, A.; Ploton, C.; Taylor, P.; Benito, Y.; Freydiere, A.-M.; Chotel, F.; Bérard, J.; Vanhems, P.; Vandenesch, F. Contribution of a broad range polymerase chain reaction to the diagnosis of osteoarticular infections caused by Kingella kingae: Description of twenty-four recent pediatric diagnoses. Pediatr. Infect. Dis. J. 2005, 24, 692–696. [Google Scholar] [CrossRef]
- Ceroni, D.; Cherkaoui, A.; Ferey, S.; Kaelin, A.; Schrenzel, J. Kingella kingae osteoarticular infections in young children: Clinical features and contribution of a new specific real-time PCR assay to the diagnosis. J. Pediatr. Orthop. 2010, 30, 301–304. [Google Scholar] [CrossRef]
- Dubnov-Raz, G.; Scheuerman, O.; Chodick, G.; Finkelstein, Y.; Samra, Z.; Garty, B.-Z. Invasive Kingella kingae infections in children: Clinical and laboratory characteristics. Pediatrics 2008, 122, 1305–1309. [Google Scholar] [CrossRef]
- Dubnov-Raz, G.; Ephros, M.; Garty, B.-Z.; Schlesinger, Y.; Maayan-Metzger, A.; Hasson, J.; Kassis, I.; Schwartz-Harari, O.; Yagupsky, P. Invasive pediatric Kingella kingae Infections: A nationwide collaborative study. Pediatr. Infect. Dis. J. 2010, 29, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Ilharreborde, B.; Bidet, P.; Lorrot, M.; Even, J.; Mariani-Kurkdjian, P.; Liguori, S.; Vitoux, C.; Lefevre, Y.; Doit, C.; Fitoussi, F.; et al. New real-time PCR-based method for Kingella kingae DNA detection: Application to samples collected from 89 children with acute arthritis. J. Clin. Microbiol. 2009, 47, 1837–1841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basmaci, R.; Lorrot, M.; Bidet, P.; Doit, C.; Vitoux, C.; Penneçot, G.; Mazda, K.; Bingen, E.; Ilharreborde, B.; Bonacorsi, S. Comparison of Clinical and Biologic Features of Kingella kingae and Staphylococcus aureus Arthritis at Initial Evaluation. Pediatr. Infect. Dis. J. 2011, 30, 902–904. [Google Scholar] [CrossRef] [PubMed]
- Lundy, D.; Kehl, D. Increasing Prevalence of Kingella kingae in Osteoarticular Infections in Young Children. J. Pediatr. Orthop. 1998, 18, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Yagupsky, P. Kingella kingae: From medical rarity to an emerging paediatric pathogen. Lancet Infect. Dis. 2004, 4, 358–367. [Google Scholar] [CrossRef]
- Yagupsky, P.; Porsch, E.; Geme, J.W.S. Kingella kingae: An Emerging Pathogen in Young Children. Pediatrics 2011, 127, 557–565. [Google Scholar] [CrossRef]
- Dormans, J.; Drummond, D. Pediatric Hematogenous Osteomyelitis: New Trends in Presentation, Diagnosis, and Treatment. J. Am. Acad. Orthop. Surg. 1994, 2, 333–341. [Google Scholar] [CrossRef] [Green Version]
- Scott, R.J.; Christofersen, M.R.; Robertson, W.W.J.; Davidson, R.S.; Rankin, L.; Drummond, D.S. Acute Osteomyelitis in Children: A Review of 116 Cases. J. Pediatr. Orthop. 1990, 10, 649–652. [Google Scholar] [CrossRef]
- Morrey, B.F.; Bianco, A.J.; Rhodes, K.H. Septic arthritis in children. Orthop. Clin. N. Am. 1975, 6, 923–934. [Google Scholar] [CrossRef]
- Morrey, B.F.; Bianco, A.J.; Rhodes, K.H. Suppurative arthritis of the hip in children. J. Bone Jt. Surg. Am. 1976, 58, 388–392. [Google Scholar] [CrossRef]
- Morrey, B.F.; Peterson, H.A. Hematogenous pyogenic osteomyelitis in children. Orthop. Clin. N. Am. 1975, 6, 935–951. [Google Scholar] [CrossRef]
- Morrissey, R.T. Bone and Joint Infections. In Lovell and Winter’s: Pediatric Orthopedics; Morrissy, R.T., Ed.; J.B. Lippincott: Philadelphia, PA, USA, 1996; pp. 579–624. [Google Scholar]
- Morrison, W.B.; Schweitzer, M.E.; Bock, G.W.; Mitchell, D.G.; Hume, E.L.; Pathria, M.N.; Resnick, D. Diagnosis of osteomyelitis: Utility of fat-suppressed contrast-enhanced MR imaging. Radiology 1993, 189, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Cherkaoui, A.; Ceroni, D.; Emonet, S.; Lefevre, Y.; Schrenzel, J. Molecular diagnosis of Kingella kingae osteoarticular infections by specific real-time PCR assay. J. Med. Microbiol. 2009, 58 Pt 1, 65–68. [Google Scholar] [CrossRef]
- Ceroni, D.; Dubois-Ferriere, V.; Cherkaoui, A.; Gesuele, R.; Combescure, C.; Lamah, L.; Manzano, S.; Hibbs, J.; Schrenzel, J. Detection of Kingella kingae osteoarticular infections in children by oropharyngeal swab PCR. Pediatrics 2013, 131, e230–e235. [Google Scholar] [CrossRef] [Green Version]
- Ceroni, D.; Cherkaoui, A.; Combescure, C.; François, P.; Kaelin, A.; Schrenzel, J. Differentiating osteoarticular infections caused by Kingella kingae from those due to typical pathogens in young children. Pediatr. Infect. Dis. J. 2011, 30, 906–909. [Google Scholar] [CrossRef] [PubMed]
- Chometon, S.; Benito, Y.; Chaker, M.; Boisset, S.; Ploton, C.; Bérard, J.; Vandenesch, F.; Freydiere, A. Specific real-time polymerase chain reaction places Kingella kingae as the most common cause of osteoarticular infections in young children. Pediatr. Infect. Dis. J. 2007, 26, 377–381. [Google Scholar] [CrossRef]
- Pääkkönen, M.; Kallio, M.J.T.; Kallio, P.E.; Peltola, H. Sensitivity of Erythrocyte Sedimentation Rate and C-reactive Protein in Childhood Bone and Joint Infections. Clin. Orthop. Relat. Res. 2010, 468, 861–866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorrot, M.; Fitoussi, F.; Faye, A.; Mariani, P.; Job-Deslandre, C.; Penneçot, G.-F.; Bingen, E.; Bourrillon, A. Marqueurs de l’inflammation et infection ostéoarticulaire. Arch. Pédiatr. 2007, 14, S86–S90. [Google Scholar] [CrossRef]
- Rose, S.R.; Petersen, N.J.; Gardner, T.J.; Hamill, R.J.; Trautner, B.W. Etiology of Thrombocytosis in a General Medicine Population: Analysis of 801 Cases with Emphasis on Infectious Causes. J. Clin. Med. Res. 2012, 4, 415–423. [Google Scholar] [CrossRef] [Green Version]
- Gouveia, C.; Subtil, A.; Norte, S.; Arcangelo, J.; Santos, M.A.; Corte-Real, R.; Simões, M.J.; Canhão, H.; Tavares, D. Distinguishing Kingella kingae from Pyogenic Acute Septic Arthritis in Young Portuguese Children. Microorganisms 2022, 10, 1233. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 216) | K. kingae (n = 100) | S. aureus (n = 116) | Student t-Test | |||
|---|---|---|---|---|---|---|
| p | ES | 95% CI | ||||
| Age, mean (SD) | 68.0 (58.9) | 19.9 (12.7) | 109.5 (51.0) | <0.001 * | 2.347 | −99.4 to −79.9 |
| Temperature, mean (SD) | 37.8 (1.1) | 37.3 (0.8) | 38.2 (1.0) | <0.001 * | 1.022 | −1.2 to −0.7 |
| CRP elevation, mean (SD) | 54.3 (62.7) | 24.0 (23.0) | 81.6 (73.7) | <0.001 * | 1.029 | −72.2 to −43.0 |
| WBC count, mean (SD) | 11.582 (4.189) | 12.300 (3.500) | 11.000 (4.600) | 0.021 * | 0.318 | 0.2 to 2.4 |
| Platelet count, mean (SD) | 360.7 (133.2) | 416.100 (115.500) | 310.900 (128.700) | <0.001 * | 0.860 | 71.7 to 138.6 |
| ESR, mean (SD) | 38.8 (29.0) | 32.9 (17.5) | 44.2 (35.9) | 0.010 * | 0.391 | −19.9 to −2.7 |
| GERMS | Sens./Spec./PPV/NVP (95% CI) | |||
|---|---|---|---|---|
| KK | MSSA | |||
| Age | <43 months | 96 | 15 | Sens = 96% (90%; 99%); PPV = 86% (79%; 92%) |
| ≥43 months | 4 | 101 | Spec = 87% (80%; 93%); NPV = 96% (91%; 99%) | |
| Temperature | <37.85 °C | 72 | 38 | Sens = 72% (62%; 81%); PPV = 65% (56%; 74%) |
| ≥37.85 °C | 28 | 78 | Spec = 67% (58%; 76%); NPV = 74% (64%; 82%) | |
| CRP elevation | <32.5 mg/L | 79 | 34 | Sens = 79% (70%; 87%); PPV = 70% (61%; 78%) |
| ≥32.5 mg/L | 21 | 82 | Spec = 71% (62%; 79%); NPV = 80% (71%; 87%) | |
| WBC count | <9350/mm3 | 82 | 67 | Sens = 82% (73%; 89%); PPV = 55% (47%; 63%) |
| ≥9350/mm3 | 18 | 49 | Spec = 42% (33%; 52%); NPV = 73% (61%; 83%) | |
| Platelet count | <361,500/mm3 | 66 | 37 | Sens = 66% (56%; 75%); PPV = 64% (54%; 73%) |
| ≥361,500/mm3 | 34 | 79 | Spec = 68% (59%; 76%); NPV = 70% (61%; 78%) | |
| ESR | <51.5 mm/h | 76 | 61 | Sens = 76% (66%; 84%); PPV = 55% (47%; 64%) |
| ≥51.5 mm/h | 34 | 41 | Spec = 47% (38%; 57%); NPV = 70% (58%; 79%) | |
| Predictors | Contrast | Univariate Logistic Regression | Multivariate Logistic Regression | ||
|---|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | ||
| CRP | 1 mg/L increase | 0.995 (0.993–0.996) | <0.001 | 0.996 (0.994–0.998) | <0.001 |
| ESR | 1 mm/h increase | 0.997 (0.993–1.000) | 0.048 | 0.998 (0.995–1.000) | 0.189 |
| WBC count | 1000/mm3 increase | 0.981 (0.963–0.999) | 0.041 | 0.982 (0.964–1.000) | 0.075 |
| Platelet count | 1000/mm increase | 1.000(0.999–1.000) | 0.590 | 1.000 (1.000–1.000) | 0.145 |
| T. admission | 1 °C increase | 0.876 (0.812–0.946) | 0.001 | 0.962 (0.885–1.040) | 0.360 |
| Intercept | - | - | - | 12.8 (0.6–279.0) | 0.109 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coulin, B.; DeMarco, G.; Vazquez, O.; Spyropoulou, V.; Gavira, N.; Vendeuvre, T.; Tabard-Fougère, A.; Dayer, R.; Steiger, C.; Ceroni, D. Osteoarticular Infections in Children: Accurately Distinguishing between MSSA and Kingella kingae. Microorganisms 2023, 11, 11. https://doi.org/10.3390/microorganisms11010011
Coulin B, DeMarco G, Vazquez O, Spyropoulou V, Gavira N, Vendeuvre T, Tabard-Fougère A, Dayer R, Steiger C, Ceroni D. Osteoarticular Infections in Children: Accurately Distinguishing between MSSA and Kingella kingae. Microorganisms. 2023; 11(1):11. https://doi.org/10.3390/microorganisms11010011
Chicago/Turabian StyleCoulin, Benoit, Giacomo DeMarco, Oscar Vazquez, Vasiliki Spyropoulou, Nathaly Gavira, Tanguy Vendeuvre, Anne Tabard-Fougère, Romain Dayer, Christina Steiger, and Dimitri Ceroni. 2023. "Osteoarticular Infections in Children: Accurately Distinguishing between MSSA and Kingella kingae" Microorganisms 11, no. 1: 11. https://doi.org/10.3390/microorganisms11010011