
Effectiveness and Efficacy of Thermoformed and 3D Printed Aligners in Correcting Malocclusion (Spacing) and Its Impact on Periodontal Oral Health and Oral Microbiome: A Double-Blinded Parallel Randomized Controlled Multicenter Clinical Trial

 , and
, and 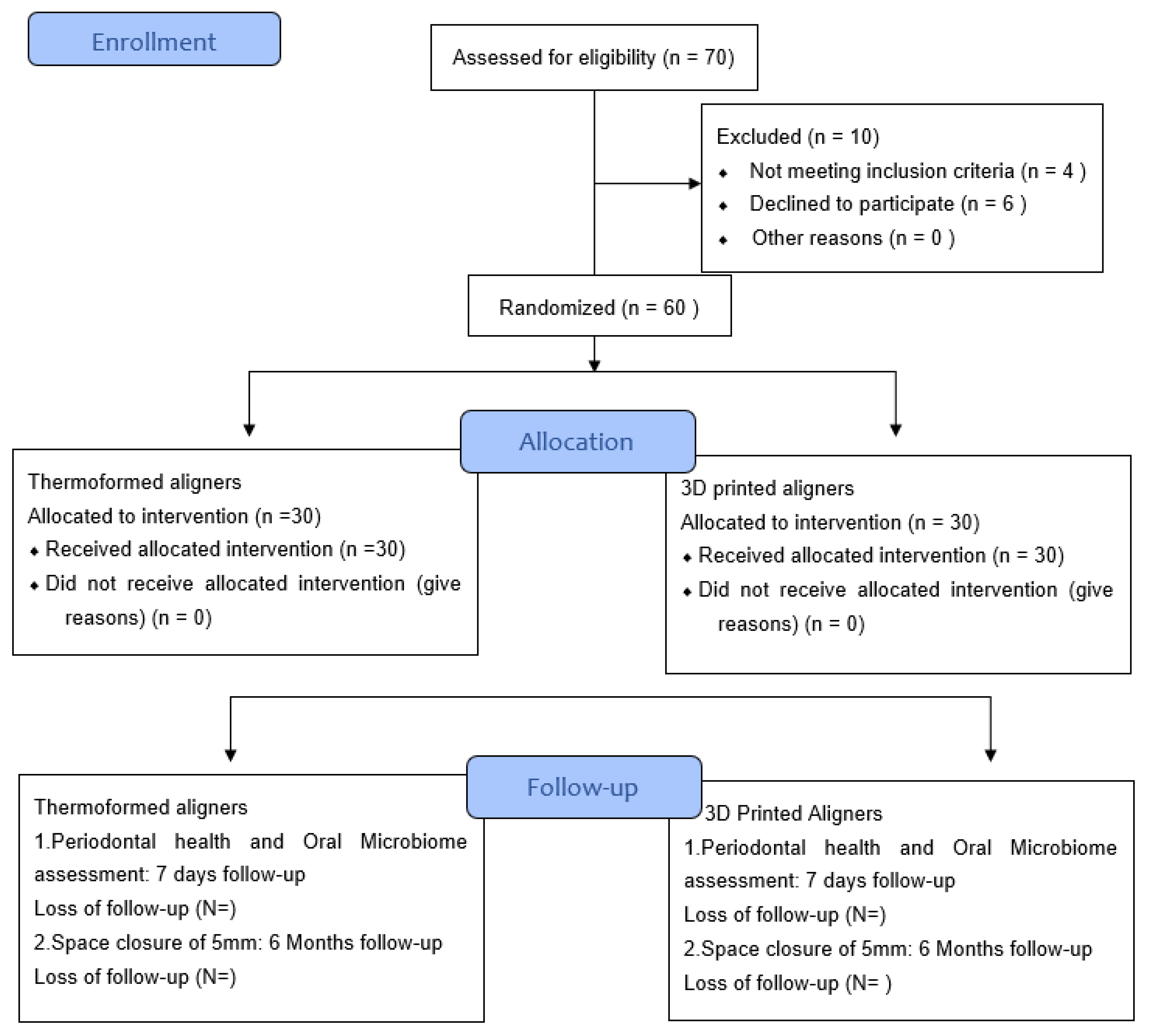{kind=link}
Abstract
:1. Introduction
1.1. Aim 1: Effectiveness and Efficacy of Clear Aligners (Invisalign) in Correcting Malocclusions
1.2. Aim 2: Periodontal Health Status and Oral Microbiome
2. Study Design
2.1. Preliminary Studies
2.2. Trial Design
2.3. Primary End Point
- Five-millimeter space closure: To determine the successful outcome of the 3D and thermoformed aligners, a 5 mm of space closure is considered a successful outcome.
- Debris Index: (The buccal scores) + (The lingual scores)/(Total number of examined buccal and lingual surfaces).
- Calculus Index: Calculus Index = (The buccal scores) + (The lingual scores)/(Total number of examined buccal and lingual surfaces).
- Oral Hygiene Index simplified (OHIS): OHIS estimates the extent and amount of debris and calculus present on the tooth in each quadrant of the mouth. It demonstrates the oral hygiene status of the mouth. It is estimated using the debris index and calculus index provided by Greene and vermillion (1964).
- Plaque Index: The plaque index estimates the amount of plaque on the tooth surface in each quadrant. 0—Absence of plaque, stain or debris; 1—plaque covering no more than 1/3rd of tooth surface; 2—subtle plaque more than 1/3rd but not more than 2/3rd; 3. Plaque cover more than 2/3rd of the tooth surface.
- Bleeding Index: A modified Sulcus Bleeding Index (mSBI) will be used to record the bleeding from the sulcus and to determine the inflammation, as it is the early indicator of inflammation (clinically).
- Basic periodontal examination index (BPE): Periodontal status will be determined using the BPE scoring.
- Root Resorption: Basic periodontal examination such as hard tissues will be conducted using a combination of bitewing and peri-apical radiographs following selection criteria for dental radiography guidelines.
- Biofilm/Saliva: Saliva (Protease activity in saliva) to determine the immune-inflammatory processes by ELISA and biofilm (protease activity) by polymerase chain reaction (PCR).
- Oral microbiome: A standard estimation of the oral microbiome will be carried out using 16S ribosomal RNA gene sequencing analysis.
2.4. Secondary End Point
3. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bresnahan, B.W.; Kiyak, H.A.; Masters, S.H.; McGorray, S.P.; Lincoln, A.; King, G. Quality of life and economic burdens of malocclusion in US patients enrolled in Medicaid. J. Am. Dent. Assoc. 2010, 141, 1202–1212. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.; Wright, J.; Conboy, F. Early treatment for Class II Division 1 malocclusion with the Twin-block appliance: A multi-center, randomized, controlled trial. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Deans, J.; Playle, R.; Durning, P.; Richmond, S. An exploratory study of the cost-effectiveness of orthodontic care in seven European countries. Eur. J. Orthod. 2009, 31, 90–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2014, 85, 881–889. [Google Scholar] [CrossRef] [Green Version]
- Zheng, M.; Liu, R.; Ni, Z.; Yu, Z. Efficiency, effectiveness and treatment stability of clear aligners: A systematic review and meta-analysis. Orthod. Craniofacial Res. 2017, 20, 127–133. [Google Scholar] [CrossRef]
- Djeu, G.; Shelton, C.; Maganzini, A. Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 292–298. [Google Scholar] [CrossRef]
- Koenig, N.; Choi, J.Y.; McCray, J.; Hayes, A.; Schneider, P.; Kim, K.B. Comparison of dimensional accuracy between direct-printed and thermoformed aligners.Korean. J. Orthod. 2022. [Google Scholar] [CrossRef]
- Lee, S.Y.; Kim, H.; Kim, H.J.; Chung, C.J.; Choi, Y.J.; Kim, S.; Cha, J.Y. Thermo-mechanical properties of 3D printed photocurable shape memory resin for clear aligners. Sci. Rep. 2022, 12, 6246. [Google Scholar] [CrossRef]
- Jia, L.; Wang, C.; Wang, C.; Song, J.; Fan, Y. Efficacy of various multi-layers of orthodontic clear aligners: A simulated study. Comput. Methods Biomech. Biomed. Engin. 2022, 21, 1–12. [Google Scholar] [CrossRef]
- Valeri, C.; Aloisio, A.; Mummolo, S.; Quinzi, V. Performance of Rigid and Soft Transfer Templates Using Viscous and Fluid Resin-Based Composites in the Attachment Bonding Process of Clear Aligners. Int. J. Dent. 2022, 2022, 1637594. [Google Scholar] [CrossRef]
- Yu, X.; Li, G.; Zheng, Y.; Gao, J.; Fu, Y.; Wang, Q.; Huang, L.; Pan, X.; Ding, J. ‘Invisible’ orthodontics by polymeric ‘clear’ aligners molded on 3D-printed personalized dental models. Regen. Biomater. 2022, 4, 9. [Google Scholar] [CrossRef] [PubMed]
- Ould-Slimane, M.; Luc, F.; Chastan, N.; Dujardin, F.; Michelin, P.; Tavolacci, M.P.; Gillibert, A.; Gauthé, R. Static and dynamic stabilometric force platform study of spinopelvic anterior sagittal imbalance. Orthop. Traumatol. Surg. Res. 2021, 23, 103195. [Google Scholar] [CrossRef] [PubMed]
- Daniele, V.; Macera, L.; Taglieri, G.; Spera, L.; Marzo, G.; Quinzi, V. Color Stability, Chemico-Physical and Optical Features of the Most Common PETG and PU Based Orthodontic Aligners for Clear Aligner Therapy. Polymers 2021, 14, 14. [Google Scholar] [CrossRef] [PubMed]
- Behyar, M.; Ratzmann, A.; Shojaei Khatouni, S.; Quasthoff, M.; Pink, C.; Ladisch, J.; Krey, K.F. Modular 3D printable orthodontic measuring apparatus for force and torque measurements of thermoplastic/removable appliances. Biomed. Tech. 2021, 26, 593–601. [Google Scholar] [CrossRef]
- Golkhani, B.; Weber, A.; Keilig, L.; Reimann, S.; Bourauel, C. Variation of the modulus of elasticity of aligner foil sheet materials due to thermoforming. J. Orofac. Orthop. 2021. [Google Scholar] [CrossRef]
- Dalaie, K.; Fatemi, S.M.; Ghaffari, S. Dynamic mechanical and thermal properties of clear aligners after thermoforming and aging. Prog. Orthod. 2021, 28, 22. [Google Scholar] [CrossRef]
- Tartaglia, G.M.; Mapelli, A.; Maspero, C.; Santaniello, T.; Serafin, M.; Farronato, M.; Caprioglio, A. Direct 3D Printing of Clear Orthodontic Aligners: Current State and Future Possibilities. Materials 2021, 5, 1799. [Google Scholar] [CrossRef]
- Palone, M.; Longo, M.; Arveda, N.; Nacucchi, M.; Pascalis, F.; Spedicato, G.A.; Siciliani, G.; Lombardo, L. Micro-computed tomography evaluation of general trends in aligner thickness and gap width after thermoforming procedures involving six commercial clear aligners: An in vitro study. Korean J. Orthod. 2021, 25, 135–141. [Google Scholar] [CrossRef]
- Elshazly, T.M.; Keilig, L.; Alkabani, Y.; Ghoneima, A.; Abuzayda, M.; Talaat, S.; Bourauel, C.P. Primary Evaluation of Shape Recovery of Orthodontic Aligners Fabricated from Shape Memory Polymer (A Typodont Study). Dent. J. 2021, 10, 31. [Google Scholar] [CrossRef]
- Sabouni, W.; Lacroix, M.; Leclercq, P.; Des Georges, O. Orthognathic treatment and aligners, which protocol? Orthod. Fr. 2021, 1, 95–113. [Google Scholar] [CrossRef]
- Maspero, C.; Tartaglia, G.M. 3D Printing of Clear Orthodontic Aligners: Where We Are and Where We Are Going. Materials 2020, 13, 5204. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khijmatgar, S.; Tumedei, M.; Del Fabbro, M.; Tartaglia, G.M. Effectiveness and Efficacy of Thermoformed and 3D Printed Aligners in Correcting Malocclusion (Spacing) and Its Impact on Periodontal Oral Health and Oral Microbiome: A Double-Blinded Parallel Randomized Controlled Multicenter Clinical Trial. Microorganisms 2022, 10, 1452. https://doi.org/10.3390/microorganisms10071452
Khijmatgar S, Tumedei M, Del Fabbro M, Tartaglia GM. Effectiveness and Efficacy of Thermoformed and 3D Printed Aligners in Correcting Malocclusion (Spacing) and Its Impact on Periodontal Oral Health and Oral Microbiome: A Double-Blinded Parallel Randomized Controlled Multicenter Clinical Trial. Microorganisms. 2022; 10(7):1452. https://doi.org/10.3390/microorganisms10071452
Chicago/Turabian StyleKhijmatgar, Shahnawaz, Margherita Tumedei, Massimo Del Fabbro, and Gianluca Martino Tartaglia. 2022. "Effectiveness and Efficacy of Thermoformed and 3D Printed Aligners in Correcting Malocclusion (Spacing) and Its Impact on Periodontal Oral Health and Oral Microbiome: A Double-Blinded Parallel Randomized Controlled Multicenter Clinical Trial" Microorganisms 10, no. 7: 1452. https://doi.org/10.3390/microorganisms10071452